")
Back to Journals » OncoTargets and Therapy » Volume 13
Primary Pulmonary Diffuse Large B Cell Lymphoma Mimicking Metastasis: A Case Report and Literature Review
Authors Liu B, Liu H, Guo L, Ma Y, Guan M, Liu M
Received 26 February 2020
Accepted for publication 22 May 2020
Published 19 June 2020 Volume 2020:13 Pages 5837—5843
DOI https://doi.org/10.2147/OTT.S251344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Bailong Liu,1,* Hui Liu,1,* Liang Guo,2 Yunfei Ma,1 Meng Guan,3 Min Liu1
1Department of Radiation Oncology, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China; 2Department of Pathology, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China; 3Cancer Center, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Meng Guan; Min Liu Tel +86 158-0430-2751
Email [email protected]; [email protected]
Abstract: Primary pulmonary diffuse large B cell lymphoma (PPDLBCL) is extremely rare, with fewer than 40 cases reported to date and a lack of systemic analysis. Herein, we present a case of PPDLBCL mimicking metastasis in a heavily treated patient with breast cancer. To our knowledge, this is the first reported case of PPDLBCL in a patient with breast cancer. A 66-year-old Chinese female diagnosed with breast cancer 7.5 years previously and multiple bone metastases 31 months later presented with a new-onset subpleural nodule in the inferior lobe of left lung detected by routine follow-up in November 2017. A 18F-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography scan showed that the pulmonary nodule was hypermetabolic with a maximum standard uptake value of 14.9, consistent with lung metastasis in view of her history of breast cancer and multiple bone involvement. Surprisingly, pathologic investigation revealed primary lung DLBCL, staged IEA. Systemic chemotherapy with R-CDOP (rituximab, cyclophosphamide, vindesine, doxorubicin liposome, and prednisone) achieved complete remission with mild side effects. At the latest follow-up in August 2019, the patient had disease-free survival of 21 months. The findings from this case indicate that primary pulmonary lymphoma should be included in the differential diagnostic checklist of pulmonary occupancy, even in solid tumor patients treated with multiple modalities. When a newly developed lung nodule is identified in such patients, clinicians should not take for granted that it is lung metastasis. Pathology results are a prerequisite for making a correct diagnosis, choosing appropriate treatment, and improving patient prognosis.
Keywords: primary pulmonary lymphoma, diffuse large B cell, pathology, case report
Introduction
Primary pulmonary lymphoma (PPL) is an extremely rare entity of heterogenous group, and diffuse large B cell lymphoma (DLBCL) accounts for just 10% of PPL.1 With regard to the aggressive subset termed primary pulmonary diffuse large B cell lymphoma (PPDLBCL), we have little information about its biological characteristics, optimized therapeutic protocols, and outcomes since less than 40 cases have been reported.1–19 Here, we present an instructive PPDLBCL case mimicking lung metastasis in a heavily treated breast cancer patient. In view of the patient’s nonspecific discomfort, isolated subpleural nodule, and definite history of metastatic breast cancer, it could easily have been misdiagnosed as lung metastasis. Our case highlights that PPL should be included in the differential diagnosis of new-onset lung lesions even in solid tumor patients to avoid misdiagnosis and ensure timely and correct intervention.
Case Report
In September 2012, a 61-year-old Chinese woman presented with a 6-month history of a painless mass in her right breast. A firm 2×1-cm mass was palpated in the inner upper quadrant of the right breast. Following mastectomy, pathology demonstrated breast invasive lobular carcinoma with immunohistochemical results of estrogen receptor (90%+), progesterone receptor (10%+), human epidermal growth factor receptor 2 (-), Ki-67 (7%+). The postoperative stage was T1N0 (axillary lymph nodes: 0/7). The patient received adjuvant endocrine therapy with anastrozole.
In April 2015, the patient complained of low back pain. Subsequent positron emission tomography-computed tomography (PET/CT) scanning in a tertiary hospital revealed hypermetabolic lesions consistent with bone metastases in T6, L2, and the sacrum. Local radiotherapy with a dose of 39Gy/13F and 30Gy/10F was applied to the sacrum and L2 metastases, respectively, which significantly relieved her pain. The endocrine therapy was switched to letrozole based on the local doctor’s advice, and zoledronic acid was given. Emission computed tomography in November 2016 demonstrated abnormal increased radioactive uptake in T6 and T7. Additional radiotherapy was given for T6 and T7 metastatic lesions.
In November 2017, the patient had routine follow-up visit and did not report cough, chest pain, fever, night sweats, or weight loss. No superficial enlarged lymph nodes were palpable on physical examination, but thoracic CT scan found a subpleural nodule measuring about 1.5 cm×1.5 cm located in the inferior lobe of the left lung and connected to adjacent pleura with a broad basal pattern (Figure 1A–C). A subsequent 18F-FDG PET/CT scan showed the pulmonary nodule was hypermetabolic with a maximum standard uptake value (SUVmax) of 14.9, and there was no clear boundary with adjacent pleura. Whole-body PET/CT also showed a FDG-avid lesion in T6 with a SUVmax of 9.9, and high-density foci in C6, L2, and the sacrum, indicating bone metastases. In view of her history of breast cancer and multiple bone involvement, lung metastasis was considered (Figure 2). Her past history was unremarkable except for hypertension for 10 years with regular treatment and good control, left shoulder joint synovial cystectomy for calcification in 2012, and cholecystectomy in 2017 for cholecystolithiasis and cholecystitis. Her Eastern Cooperative Oncology Group performance status was 1. Clinical laboratory tests showed normal serum lactate dehydrogenase, erythrocyte sedimentation rate, and slightly elevated β2-microglobulin of 1.84 mg/L (0.7–1.8 mg/L). The hepatitis B antigen and serum antibodies for hepatitis C, syphilis, and human immunodeficiency virus (HIV) were negative. Bone marrow aspiration tests showed no involvement. A percutaneous lung lesion biopsy revealed diffuse medium to large neoplastic cells with obvious nuclear atypia, obvious nucleoli, vacuolar chromatin, and invasion of small vessels (Figure 3A). Furthermore, no low-grade B-cell lymphoma components such as marginal zone lymphoma or follicular lymphoma were found around the tumor. This indicated that was de novo rather than transformed from marginal B cell lymphoma or follicular lymphoma. The neoplasm exhibited a high Ki-67 proliferation index of 80% (Figure 3B). Tumor cells were strongly immunoreactive to CD20 (Figure 3C), Bcl-2 (Figure 3D), Bcl-6 (Figure 3E), and MUM1 (Figure 3F) but negative for CD10 (Figure 3G) and cyclin D1 (Figure 3H). Tumor immunohistochemistry showed PAX-5 (+), CD5 (-) (Figure 3I), and c-Myc (30%+). B cell gene rearrangement was positive for immunoglobulin IGH and IGκ by polymerase chain reaction. Epstein-Barr virus encoded RNA in situ hybridization was negative (Figure 3J). The neoplastic cells of pleomorphic mantle cell lymphoma generally have unobvious nucleoli, rich chromatin, and scarce cytoplasm, and blastic mantle cell lymphoma is immunoreactive to cyclin D1. In our patient, the tumor cells were medium to large with obvious nuclear atypia, apparent nucleoli, and vacuolar chromatin, but negative for Cyclin D1. Based on morphology and immunohistochemistry, the diagnosis was DLBCL (non-germinal center subtype) staged as IEA with an International Prognostic Index score of 1.
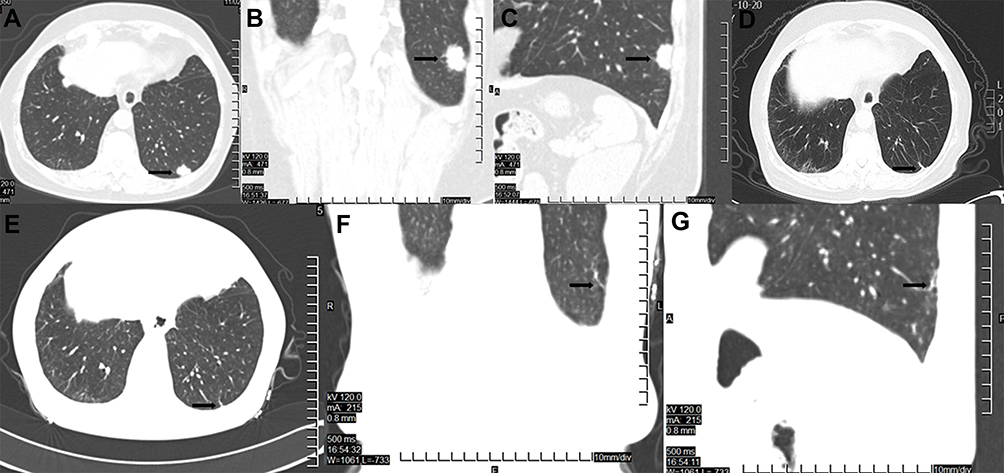 |
Figure 1 CT lung scan results. Notes: (A–C) Thoracic CT on November 2, 2017 revealed a new-onset nodule located in the LLL. (A) Transverse view; (B) coronal view; (C) sagittal view; (D) thoracic CT demonstrated CR after three cycles of chemotherapy with R-CDOP. (E–G) Lung CT in August 2019 still showed a CR status. (E) Transverse view; (F) coronal view; (G) sagittal view. Abbreviations: CT, computed tomography; LLL, left lower lobe of lung; CR, complete remission; R-CDOP, rituximab, cyclophosphamide, vindesine, doxorubicin liposome, and prednisone. |
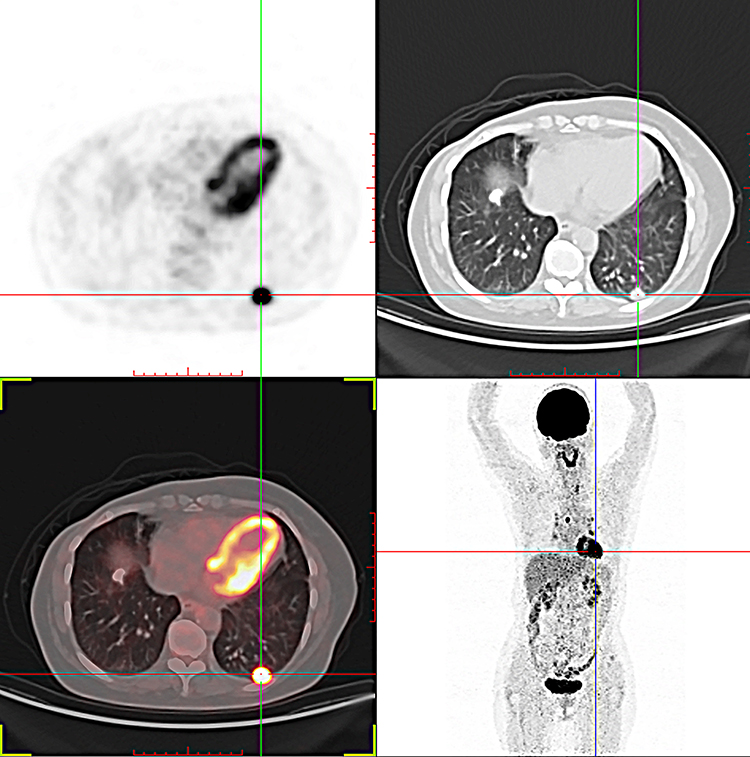 |
Figure 2 Whole-body PET/CT findings. Notes: PET/CT demonstrated a subpleural hypermetabolic nodule in the LLL measuring about 1.5cm×1.5cm with SUVmax of 14.9. This nodule had an unclear boundary with the adjacent pleura (A, PET images; B, CT images; C, fused PET/CT images of the FDG-avid lung lesion; D, coronal image of whole-body PET). Abbreviations: PET, positron emission tomography; CT, computed tomography; LLL, left lower lobe of lung; SUVmax, maximum of standard uptake value; FDG, fluorodeoxyglucose. |
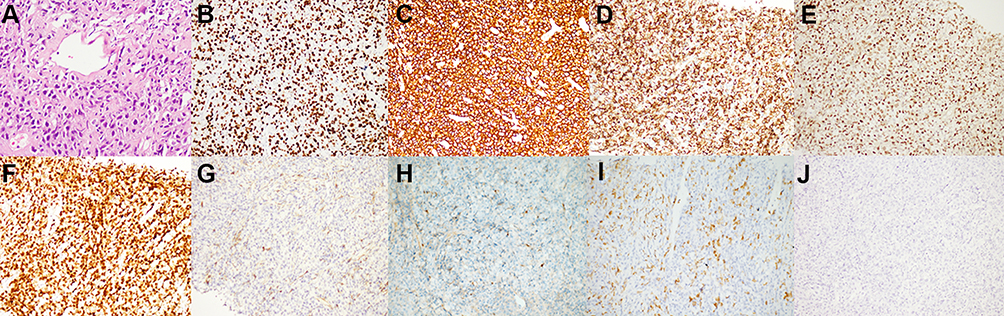 |
Figure 3 Pathological results of the pulmonary lesion biopsy. Notes: (A) HE staining showing infiltration of medium to large tumor cells with obvious nuclear atypia, nucleoli, vacuolar chromatin, and invasion of small vessels (original magnification, 400×). (B) The neoplasm exhibited a high Ki-67 proliferation index (80%, original magnification, 200×) and stained positive for CD20 (C, original magnification, 200×), Bcl-2 (D, original magnification, 200×), Bcl-6 (E, original magnification, 200×), and MUM1 (F, original magnification, 200×) but negative for CD10 (G, original magnification, 200×), cyclin D1 (H, original magnification, 200×) and CD5 (I, original magnification, 200×). (J) Epstein-Barr virus encoded RNA in situ hybridization was negative (original magnification, 200×). Abbreviations: HE, hematoxylin-eosin; CD, cluster of differentiation; RNA, ribonucleic acid. |
Systemic chemotherapy with R-CDOP (rituximab, cyclophosphamide, vindesine, doxorubicin liposome, and prednisone) was administered, and the PPDLBCL strongly responded. After three cycles, lung CT showed a complete remission (CR) response (Figure 1D). Whole-body PET-CT also confirmed CR after four cycles of R-CDOP (Figure 4). The patient then underwent two cycles of rituximab. The endocrine therapy was switched to fulvestrant for breast cancer, and treatment was well tolerated. At the patient’s most recent follow-up in August 2019, her quality of life was good, lung CT demonstrated CR status (Figure 1E–G), and her disease-free survival (DFS) had reached 21 months.
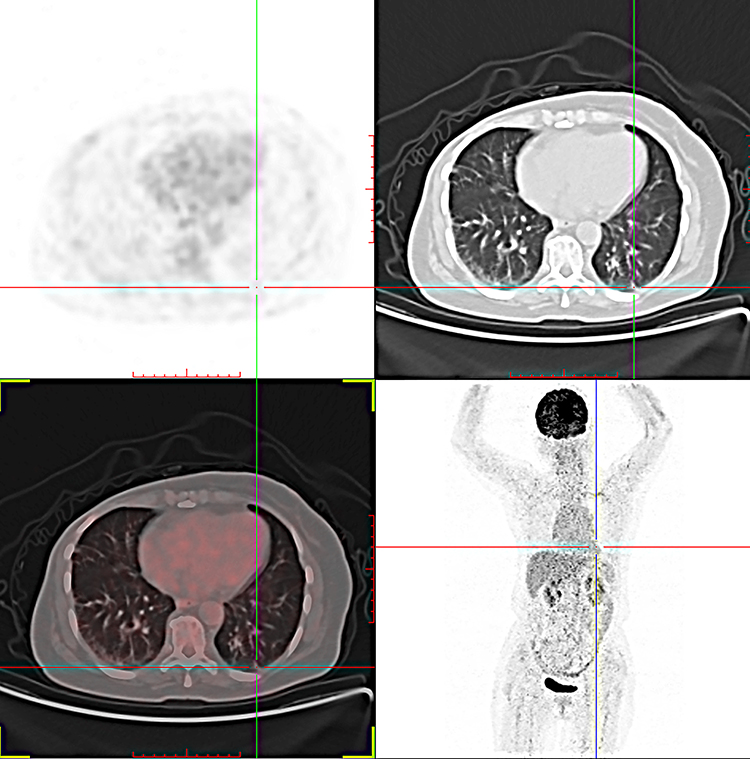 |
Figure 4 Whole-body PET/CT after four cycles of R-CDOP demonstrated CR. Notes: (A) PET images; (B) CT images; (C) fused PET/CT images; (D) coronal image of whole-body PET. Abbreviations: PET, positron emission tomography; CT, computed tomography; R-CDOP, rituximab, cyclophosphamide, vindesine, doxorubicin liposome, and prednisone; CR, complete remission. |
Discussion
PPL is exceedingly rare, accounting for just 0.5–1% of all the primary lung malignancies and 3–4% of extranodal non-Hodgkin lymphoma.4 The most common subset of PPL is mucosa-associated lymphoid tissue (MALT)-associated lymphoma, accounting for 70–80% of all PPL and showing an indolent clinical course. The 10-year overall survival rate of pulmonary MALT is about 90%.20 In contrast, DLBCL only constitutes ~10% of PPL.1 Given its rarity, there remains considerable uncertainty regarding the clinical and radiological features and best treatment strategy for PPDLBCL.
PPL is defined as malignant lymphoma that originates from the one or both pulmonary parenchyma or bronchi.21 The PPL diagnostic criteria proposed by Cordier et al state the following: 1) definite pathological results supporting PPL; 2) the lesions at diagnosis are limited in the thorax; and 3) within 3 months after diagnosis, there is no evidence of extrathoracic involvement of lymphoma. As shown in Table 1, PPL staging refers to the stage standard of extranodal lymphoma.22
 |
Table 1 PPL Staging System |
PPL diagnosis is challenging since the symptoms are generally non-specific. The chief complaints can be pulmonary such as cough (dry or productive), chest pain, shortness of breath, dyspnea, and hemoptysis and/or systemic such as fever, fatigue, night sweats, and unintentional weight loss. Occasionally, patients are asymptomatic as in the present case, but routine thoracic radiologic follow-up reveals the abnormality. Radiological manifestations are highly variable; the lesion can be single or multiple, mass or nodule-like, solid (including air bronchograms) or cavitated. Ground-glass opacities can be an uncommon radiological finding in PPL. Pleural involvement is infrequent, manifesting as pleural effusions, extensive areas of pleural calcification, or pleural plaques. Some studies analyzed imaging differences between PPL and secondary pulmonary lymphoma (SPL). Dong et al reported that large size (>3 cm), cavitation, consolidation, and peripheral location were suggestive of PPL while hilar and mediastinal lymph node enlargement were more common in SPL. In view of the insidious onset and lack of specificity in clinical symptoms and imaging findings, PPL is frequently misdiagnosed as refractory pneumonia, lung abscess, asthma, primary lung cancer, or lung metastasis.5,9,10,12
As a functional whole-body imaging modality, PET/CT plays an important role in the initial assessment and response evaluation of lymphoma. In individuals with symptoms suggestive of pulmonary lymphoma, if the first PET/CT reveals FDG-avid lesions in both the lung and extrathoracic sites, we cannot define it as PPL or SPL despite the radiological difference mentioned above. Our patient could easily have been misdiagnosed with lung metastasis of breast cancer based on the subpleural hypermetabolic nodule revealed by whole-body PET/CT, no symptoms, typical radiological features (eg, oval shape with regularity), and definite history of metastatic breast cancer. CT-guided or transbronchial needle biopsy is frequently inconclusive. Generally, excisional biopsy or surgery leads to the final diagnosis. Our patient was heavily treated and had definite multiple bone metastases of breast cancer. Furthermore, the new oval nodule was located in the subpleural region and an unclear boundary with the adjacent pleura, mimicking lung metastasis. In refractory or metastatic settings, patients often refuse rebiopsy due to poor physical tolerance. Our case highlights that clinicians should keep the possibility of a second primary tumor in mind and encourage patients to undergo biopsy to allow pathology studies.
Immunosuppression might be a risk factor for PPDLBCL development. The majority of acquired immune deficiency syndrome-associated PPL is high-grade B cell lymphoma including DLBCL. Additionally, methotrexate can be carcinogenic in a subset of patients.8,11,16 Ebeo et al described a patient with rheumatoid arthritis and Epstein-Barr virus infection in whom methotrexate induced PPDLBCL, even when given at a low dose. After the patient discontinued methotrexate, the lymphoma had not recurred 2 years later.16 Our patient had no HIV infection, methotrexate use, or toxic exposure. The immunocompromised state due to metastatic breast cancer might have contributed to the development of PPL.
The relationship between breast cancer and lymphoma is worthy of attention. There is increasing evidence that breast implants can induce the development of anaplastic large cell lymphoma (ALCL).23 Up to February 2018, 516 pathologically identified breast-implant-associated (BIA) ALCL cases were described globally.23,24 BIA-ALCL generally presents as a late-developing seroma after an average of 7–13 years after implant exposure.23 We should pay special attention to this issue given the cosmetic needs and use of prosthetic implants during breast cancer treatment. Additionally, males with a past history of lymphoma might have a higher than expected risk of primary breast cancer.25
The pathogenetic features of PPL have been explored. The identification of MALT-1 gene rearrangement by fluorescence in situ hybridization in bronchoalveolar fluid cells contributes to the definitive diagnosis of MALT PPL.26 Approximately 40–50% of MALT PPL harbors the typical translocation of t(11;18)(q21;q21), generating a fusion gene of API2-MALT1 and subsequent activation of nuclear factor-kB signaling. Other cytogenetic abnormalities such as t(1;14)(p22;q32)(IgH-BCL10) and trisomy 3 have also been documented.27 Additionally, MYC-inactivation was effective in sustained regression of lymphoma.28
The optimal treatment for PPDLBCL remains to be clarified. Surgery, followed by adjuvant chemotherapy or not or chemotherapy alone can be available.19 Hilar or mediastinal lymph node involvement is not a contraindication for resection.19 Any individual up to stage IIE with complete resection is surgical candidate.19 Whether adjuvant chemotherapy after R0 resection should be given remains controversial. Kawashima et al recommended complete resection plus regional lymph node dissection followed by adjuvant chemotherapy to achieve a satisfactory DFS. The two PPDLBCL cases in their report had DFS of 81 and 20 months. Wei et al described a large PPDLBCL in a 25-year-old female involving the superior vena cava (SVC). She underwent extensive resection and reconstruction of the pulmonary artery, SVC, and right bronchus followed by six cycles of R-CHOP (rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone) with long-term DFS.19 However, in another young female with PPDLBCL who presented with SVC syndrome, involved field radiotherapy was initiated to rapidly relieve symptoms, followed by R-CHOP chemotherapy.2 As an aggressive subtype, PPDLBCL has a poorer prognosis compared with lung MALT lymphoma, intensive chemotherapy is essential especially for those who refused surgery just like our patient.
Conclusion
Despite the rarity of PPL, clinicians should consider it when a new-onset lung lesion is identified, even in solid tumor patients. Due to the aggressive nature of PPDLBCL, early recognition is critical. Pathology is prerequisite for selecting appropriate treatment and improving prognosis. In the future, multi-center clinical trials should be performed to extend our understanding of the biological features of PPDLBL to guide treatment choices.
Ethics Approval
This is a case report, and institutional approval was not needed.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Tanriverdi E, Acat M, Ozgul G, et al. Primary pulmonary lymphoma: four different and unusual radiologic and clinical manifestations. Leuk Lymphoma. 2017;58(5):1231–1233. doi:10.1080/10428194.2016.1225210
2. Salhan D, Verma P, Naing TW, et al. Primary pulmonary lymphoma presenting with superior vena cava syndrome in a young female. Case Rep Pulmonol. 2017;2017:1937107.
3. Delgado Torralbo JA, Garcia Gomez LC, Sanchez Varilla JM. Unilateral lung infiltrate: a rare form of presentation of primary pulmonary lymphoma. Arch Bronconeumol. 2018;54(2):103–104. doi:10.1016/j.arbres.2017.06.004
4. Agarwal KK, Dhanapathi H, Nazar AH, Kumar R. Primary pulmonary lymphoma-role of fluoro-deoxy-glucose positron emission tomography-computed tomography in the initial staging and evaluating response to treatment – case reports and review of literature. Indian J Nucl Med. 2016;31(3):194–197. doi:10.4103/0972-3919.181529
5. Matsumoto T, Otsuka K, Funayama Y, Imai Y, Tomii K. Primary pulmonary lymphoma mimicking a refractory lung abscess: a case report. Oncol Lett. 2015;9(4):1575–1578. doi:10.3892/ol.2015.2929
6. Latif Moini A, Farbod Ara T, Fazeli Mosleh Abadi M. Primary pulmonary lymphoma and cutaneous metastasis: a case report. Iran J Radiol. 2014;11(3):e15574. doi:10.5812/iranjradiol.15574
7. Shahani L, McKenna M. Primary pulmonary lymphoma in a patient with advanced AIDS. BMJ Case Rep. 2014;2014:bcr2013203265. doi:10.1136/bcr-2013-203265
8. Shinoda K, Taki H, Tsuda T, Hayashi R, Nomoto K, Tobe K. Primary pulmonary lymphoma presenting with multiple lung nodules. Am J Respir Crit Care Med. 2014;190(9):e30–e31. doi:10.1164/rccm.201401-0086IM
9. Zhao Q, Wei S, Li X, Zhou Q, Chen J. [Primary pulmonary lymphoma: a case report]. Zhongguo Fei Ai Za Zhi. 2014;17(10):765–768. Chinese. doi:10.3779/j.issn.1009-3419.2014.10.10
10. Hadda V, Khilnani GC, Bhalla AS, Gupta R, Gupta SD, Goel A. Pulmonary lymphoma mimicking metastases: a case report. Cases J. 2009;2:7081. doi:10.1186/1757-1626-0002-0000007081
11. Suzuki M, Hirano S, Ito H, et al. Pulmonary lymphoma developed during long-term methotrexate therapy for psoriasis. Respirology. 2007;12(5):774–776. doi:10.1111/j.1440-1843.2007.01139.x
12. Sirmali M, Kalac N, Agackiran Y, Kaya S. Primary pulmonary lymphoma disguised as asthma. Acta Chir Belg. 2006;106(1):127–129. doi:10.1080/00015458.2006.11679855
13. Dobrilovic N, Wright CB, Vester SR, Patel MA, Fannin EA. Unusual chest lesion: giant primary pulmonary lymphoma. Ann Thorac Surg. 2005;80(3):1134. doi:10.1016/j.athoracsur.2003.09.091
14. Storch I, Jorda M, Ribeiro A. EUS-guided biopsy in the diagnosis of pulmonary lymphoma in a patient with an esophagopulmonary fistula. Gastrointest Endosc. 2005;61(7):904–906. doi:10.1016/S0016-5107(05)00288-9
15. Varona JF, Guerra JM, Grande C, Villena V, Gonzalez-Lois C, Martinez MA. Primary pulmonary lymphoma: diagnosis and follow-up of 6 cases and review of an uncommon entity. Tumori J. 2005;91(1):24–29. doi:10.1177/030089160509100106
16. Ebeo CT, Girish MR, Byrd RP, Roy TM, Mehta JB. Methotrexate-induced pulmonary lymphoma. Chest. 2003;123(6):2150–2153. doi:10.1378/chest.123.6.2150
17. Miyahara N, Eda R, Umemori Y, et al. Pulmonary lymphoma of large B-cell type mimicking Wegener’s granulomatosis. Intern Med. 2001;40(8):786–790. doi:10.2169/internalmedicine.40.786
18. Matsuoka Y, Kenzaka T. Lung lymphoma with ground glass opacity CT image. QJM. 2017;110(5):327.
19. Wei S, Li X, Qiu X, et al. Primary lung lymphoma involving the superior vena cava. World J Surg Oncol. 2012;10:131. doi:10.1186/1477-7819-10-131
20. Nahorecki A, Chabowski M, Straszak E, et al. Primary pulmonary MALT lymphoma – case report and literature overview. Eur Rev Med Pharmacol Sci. 2016;20(10):2065–2069.
21. Dong Y, Zeng M, Zhang B, et al. Significance of imaging and clinical features in the differentiation between primary and secondary pulmonary lymphoma. Oncol Lett. 2017;14(5):6224–6230. doi:10.3892/ol.2017.6962
22. Ferraro P, Trastek VF, Adlakha H, Deschamps C, Allen MS, Pairolero PC. Primary non-Hodgkin’s lymphoma of the lung. Ann Thorac Surg. 2000;69(4):993–997. doi:10.1016/s0003-4975(99)01535-0
23. Kricheldorff J, Fallenberg EM, Solbach C, Gerber-Schäfer C, Rancsó C, Fritschen UV. Breast implant-associated lymphoma. Dtsch Arztebl Int. 2018;115(38):628–635. doi:10.3238/arztebl.2018.0628
24. Leberfinger AN, Behar BJ, Williams NC, et al. Breast implant-associated anaplastic large cell lymphoma: a systematic review. JAMA Surg. 2017;152(12):1161–1168. doi:10.1001/jamasurg.2017.4026
25. Farr DE, Thomas A, Khan SA, Schroeder MC. Male breast cancer as a second primary cancer: increased risk following lymphoma. Oncologist. 2017;22(8):895–900. doi:10.1634/theoncologist.2016-0460
26. Cardenas-Garcia J, Talwar A, Shah R, Fein A. Update in primary pulmonary lymphomas. Curr Opin Pulm Med. 2015;21(4):333–337. doi:10.1097/MCP.0000000000000180
27. Piña-Oviedo S, Weissferdt A, Kalhor N, Moran CA. Primary pulmonary lymphomas. Adv Anat Pathol. 2015;22(6):355–375. doi:10.1097/PAP.0000000000000090
28. Tran PT, Fan AC, Bendapudi PK, et al. Combined inactivation of MYC and K-Ras oncogenes reverses tumorigenesis in lung adenocarcinomas and lymphomas. PLoS One. 2008;3(5):e2125. doi:10.1371/journal.pone.0002125
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.