Back to Journals » Infection and Drug Resistance » Volume 14
Preventive Practice and Associated Factors Toward Coronavirus Disease 19 in Adigrat Town, Northern Ethiopia: Community-Based Cross-Sectional Study
Authors Gebremeskel III F, Teklay E, Gebrehaweria M
Received 4 November 2020
Accepted for publication 10 June 2021
Published 25 June 2021 Volume 2021:14 Pages 2379—2386
DOI https://doi.org/10.2147/IDR.S288941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Fre Gebremeskel III,1 Embeba Teklay,2 Menaseb Gebrehaweria1
1Department of Public Health, College of Medicine and Health Science, Adigrat University, Adigrat, Ethiopia; 2School of Public Health, College of Health sciences, Aksum University, Aksum, Ethiopia
Correspondence: Fre Gebremeskel
Department of Public Health, College of Medicine and Health Science, Adigrat University, P.O.Box:50, Adigrat, Ethiopia
Tel +251924862758
Email [email protected]
Purpose: The global coronavirus disease 19 pandemic is an unprecedented crisis, unlike any since the end of the Second World War. Yet no successful vaccine or treatment has been reported. Even though increasing the practice of the community is critical to prevent coronavirus disease 19 pandemic, there is limited study in Ethiopia particularly in the study area. Therefore, the study aimed to assess practice and associated factors toward coronavirus disease 19.
Objective: To assess the prevalence and associated factors with practice toward coronavirus disease 19 prevention in Adigrat residents, Northern Ethiopia, 2020.
Methods: A community-based cross-sectional study design was carried out among 421 Adigrat Town residents from September 10 to 20, 2020. Households were selected using systematic sampling technique. To identify determinant factors, binary logistic regression analyses were employed with confidence interval of 95%. To identify statistically significant factors, the adjusted odds ratio (AOR) was used. Statisticalsignificance was determined at P-value < 0.05.
Results: The prevalence of poor practice was 32.2% (95% CI (31.5– 38.5%)). Age of 20– 29 (AOR=2.1, 95% CI (1.9– 6.5)), occupational status of unemployed (AOR=1.5, CI 95% (1.4– 1.9)), marital status of unmarried (AOR=1.9, 95% CI (1.2– 12.5)), and educational status of cannot read and write (AOR=2.1, 95% CI (2.0– 9.3)) were statistically significant factors toward COVID-19 prevention.
Conclusion: The poor practice toward coronavirus disease 19 prevention was significantly high. Age, occupation, marital status, and educational status were significantly associated with the preventive practice toward the coronavirus disease 19. It would be helpful if the health professionals or other volunteers inform the community continuously by giving health educations regarding the preventive ways to increase the practice.
Keywords: COVID-19, practice, Ethiopia
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS –CoV-2). It was initially identified in December 2019 in Wuhan, the capital of China’s Hubei province, and has since spread globally, being the ongoing pandemic. World Health Organization announced it as a public health emergency of international concern on 30 January 2020 and pandemic on 11 March 2020.1
Incubation period of COVID-19 averagely varies from 2 to 14 days from infection. Common symptom includes fever, cough, shortness of breath, and fatigue. While majority cases result with mild symptom but it may progress to viral pneumonia, multi organ failure.2,3 The virus primarily transmitted between people during close contact, often via small droplet produced during coughing, sneezing, or talking, and people also get infected through touching contaminated surface and then touching their face.2,4
Sub-Saharan Africa (SSA), including Ethiopia, is unlikely to escape the direct and indirect impact of the pandemic.5 It has precipitated massive short-term economic contraction, shuttered many firms whether big or small, thrown tens of millions out of work, disrupted global supply chains, severely strained health services, fiscal capacity and safety nets, and eroded global solidarity and multilateralism just when they are needed the most. It has also triggered some social unrest, albeit contained at present, but the future in this regard is hard to predict.5 Its effects are already wide-ranging, and its longer-term repercussions will be profound.5
Studies showed that public health emergency due to COVID-19 may affect the safety, health and wellbeing of both the community and individual.6–12 These effects may translate in to arrange of emotional reactions (such as depression, anxiety, insomnia, and acute stress), unhealthy behavior, increase risk of suicide among the general population.6–9 People who contract the disease, risky group (elder, people with compromised immunity, people with preexisting medical, and psychiatric problem) are at increased risk of psychosocial outcome.7,11 The disease also increases the risk of suicide.6,13 Health professionals are also at increased risk of mental health consequence.13–15
Currently, more than 36,658,137 people were getting infected of coronavirus, and more than 1,064,560 coronavirus deaths were reported globally as of 8 October 2020. In Africa, more than 1,553,035 people got infected of coronavirus and more than 37,283 coronavirus deaths were reported as of 8 October 2020. Ethiopia is being the fourth most affected country in Africa with total coronavirus case of 81,797, total death of 902 as of 8 October 2020.16
Yet, there is no successful vaccine or medicine for COVID-19.17 But there are prevention methods such as hand washing, social distancing, avoiding social gathering, when coughing or sneezing cover mouth and nose with bent elbow or tissue, avoiding physical greeting, avoid touching nose, eye and mouth, clean surface in house, work or transport, and face covering.17 Therefore, applying the preventive measure to prevent it is the utmost critical intervention. Poor practice of the preventive method directly increases the infection.17
Research done in Ethiopia revealed that (83.0%) knew the main clinical symptoms of COVID-19. 72.0% knew that older people who have chronic illnesses are at high risk of developing a severe form of the disease.18 About 95.1% knew that the virus spreads via respiratory droplets of infected people, while 77 (31.2%) of the respondents knew about the possibility of asymptomatic transmission.18 Only 15 (6.1%) knew that children and young adults had to involve preventive measures. Overall, 41.3% of the visitors had high knowledge. Frequent hand washing (77.3%) and avoidance of shaking hands (53.8%) were the dominant practices. Knowledge status, self-efficacy (positively), older age, and unemployment (negatively) predicted hand washing and avoidance of handshaking.18
Consequently, knowing the preventive measure and factors associated with COVID-19 is very crucial. It helps to predict the behaviors of the community in order to take some interventions to prevent the disease. But there is limited study on the prevalence of the preventive measures and factors associated with COVID-19 particularly in the study area. Furthermore, most of the studies are health facility based in which community-based studies may be important for community interventions to prevent the disease. So, this study aimed to determine the prevalence and associated factors of the preventive measure towards COVID-19 among Adigrat residents. The result of this study in the pandemic time may help to guide the health professionals, and health system managers, and other concerned stakeholders for the prevention of the disease effectively.
Materials and Methods
Study Design, Area and Period
A community-based cross-sectional study design was carried out from Sept. 10–20, 2020, at Adigrat, Northern Ethiopia. Adigrat is located 900 km away from Addis Ababa, the capital city of Ethiopia.19 It has six kebelles, and regarding Health infrastructure it has one general hospital, and three health centers.
Source and Study Population
All residents of Adigrat Town were the source population, while all selected residents in Adigrat Town during the study period were the study population.
Inclusion and Exclusion Criteria
All residents who reside in Adigrat Town at least for the previous six months prior to the study were included in the study whereas residents who reside in Adigrat Town less than six-month, household head less than 18 ages, and household with severely ill household head without respondent were excluded from the study.
Sample Size and Sampling Procedure
The sample size was calculated using single population formula (n=Z2 p (1−p)/d2), where z is the normal standard distribution set at 1.96, with a confidence level specified at 95% and a tolerable margin of error (d) at 5%, considering 10% nonresponse rate and prevalence of poor practice toward COVID-19 (p) 47.3% taken from a previous similar study conducted in Ethiopia.20 Finally, the sample size yielded 421. The sample was proportionally allocated based on the number of households in each kebelle; finally, households were selected using systematic random sampling until the required sample was yielded.
Study Variables
Practice (Yes/No) was the outcome variable and socio demographic like age, sex, educational status, marital status, occupation, and religion were the independent variables in this study.
Data Collection Method
A pretested, structured, interviewer administered questionnaire adopted from the World Health Organization was used. The questionnaire includes socio demographic characteristics, practice towards COVID-19. The questionnaire addressing practice (15 questions) was responded based on yes/no and one was given for the correct answer and zero was given for an incorrect answer.
Data Quality Control
To secure data quality, the questionnaire was initially developed in English version then translated to the Tigrigna version (local language) then translated back to English by language expert. A pretest was conducted out of the study area in 5%21 of the sample for detection of any wording error and to set the appropriate time. Then, the necessary correction was made accordingly. Data collectors and supervisors were trained for two consecutive days. During the data collection process, the filled questionnaire was checked for its completeness every day by the principal investigator. After data collection, data were stored in a secured place to maintain confidentiality and back up of the data were stored in different areas not to lose the data. Finally, data were cleaned for missing data using a frequency table before entering into the analysis.
Data Processing and Analysis
The collected data were coded, entered using Epi info version 7.2.1.0 then exported to SPSS version 25 for the analysis purpose. Then, data were analyzed using appropriate descriptive statistics, and summarized by frequency, and percentage. Both multivariable and binary logistic regression analyses were employed to determine factors associated with preventive measures. The variables with p < 0.2 in the bivariable analysis were entered into multivariable logistic regression. The factors associated with practice were determined by calculating the adjusted odds ratio (AOR) and crude odds ratio (COR) with a confidence interval (CI) of 95%. Statistical significance was decided at P-value <0.05. Finally, tables, and text were used to present the analyzed data accordingly. The goodness of fit for the final logistic model was tested using Hosmer and lemeshow test at a value of >0.05.
Operational Definition
Bloom’s cut-off point was used to classify the overall practice score.
Good practice: Those who score between 80% and 100% (12–15 points) out of the COVID_19 preventive practice questions15 were classified as good; if the score was between 60% and 79% (9–11.9 points), it was classified as moderate practice.21
Poor practice: Those who score less than 60% (<9 points) out of the total COVID_19 preventive practice questions15 were classified as poor.21
Results
Socio Demographic and Clinical Characteristics of Study Participants
The response rate was 95% in which a total of 400 respondents were included in the study. Of these, 140 (35%) were in the age group of 30–39, and majority of the study participants were female 214 (50.9%). About 189 (47.2%) were married. Concerning occupation, 122 (30.5%) of the study participants were housewife while 100 (25%) were merchant. Three hundred sixty (90%) of the study participants were orthodox by religion. Concerning educational status, 186 (46.5%) of the study participants had an educational status of can read and write (Table 1).
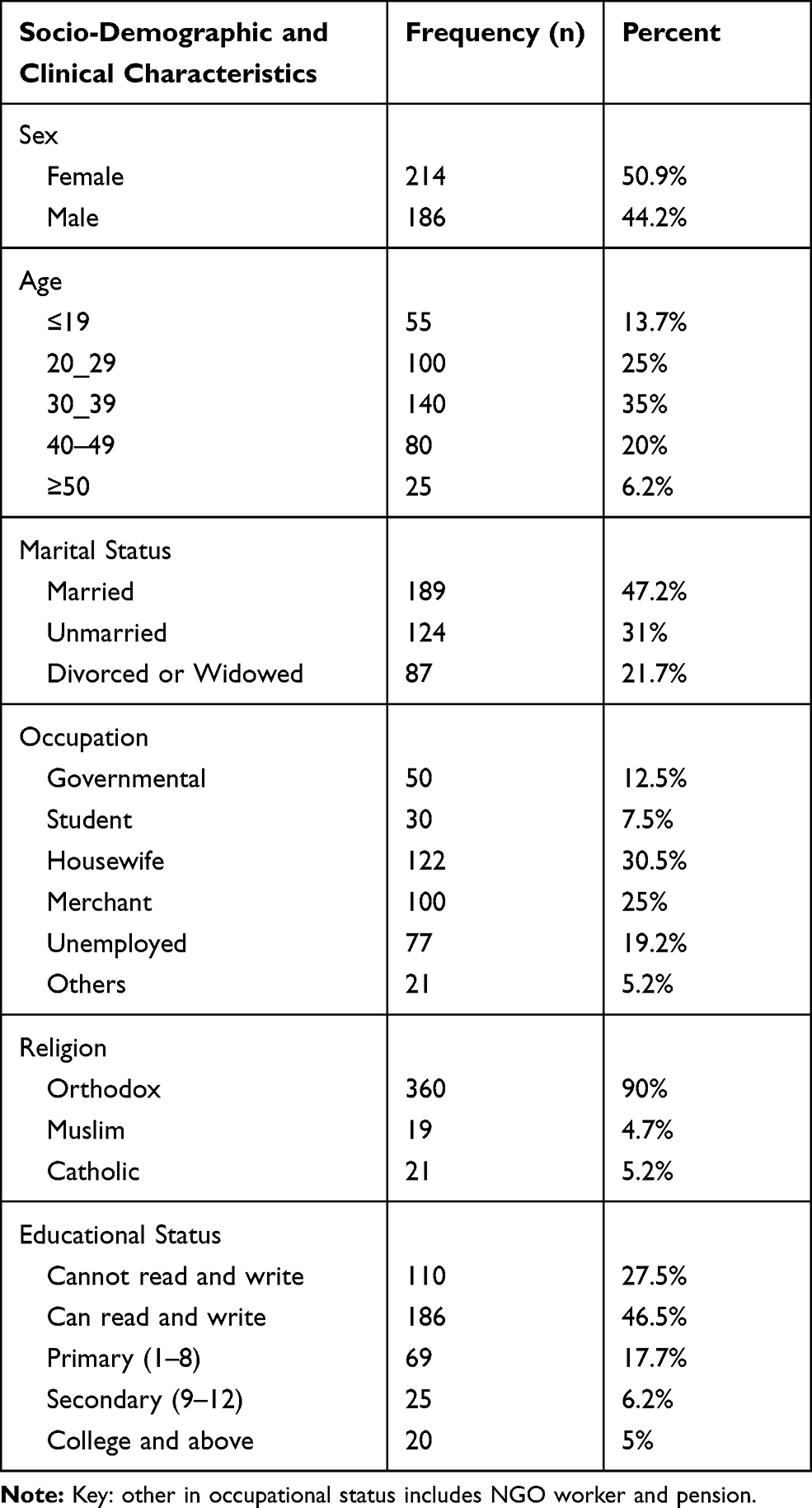 |
Table 1 Socio Demographic and Clinical Characteristics of Adigrat Town Residents, Tigray, Northern Ethiopia, 2020 (N=421) |
Practice Toward COVID-19 Prevention
Out of the total respondents, in the Adigrat resident’s poor practice was reported in 32.2% (95% CI (31.5–38.5%)) of them. About 380 (95%) reported that they had avoided hand shaking, and 344 (86%) stayed at home when they were sick due to common cold-like infection during the transmission period. About 339 (84.7%) of the household head listen and follow the direction of the state and local authorities. Three hundred and twenty (80%) of the household heads Practiced physical distancing to prevent COVID-19. Reuse of a mask 141 (35.2%), touch the front of the mask when taking it off 170 (42.5%), and wear a mask 200 (50%) were practiced less than the other preventive measures (Table 2).
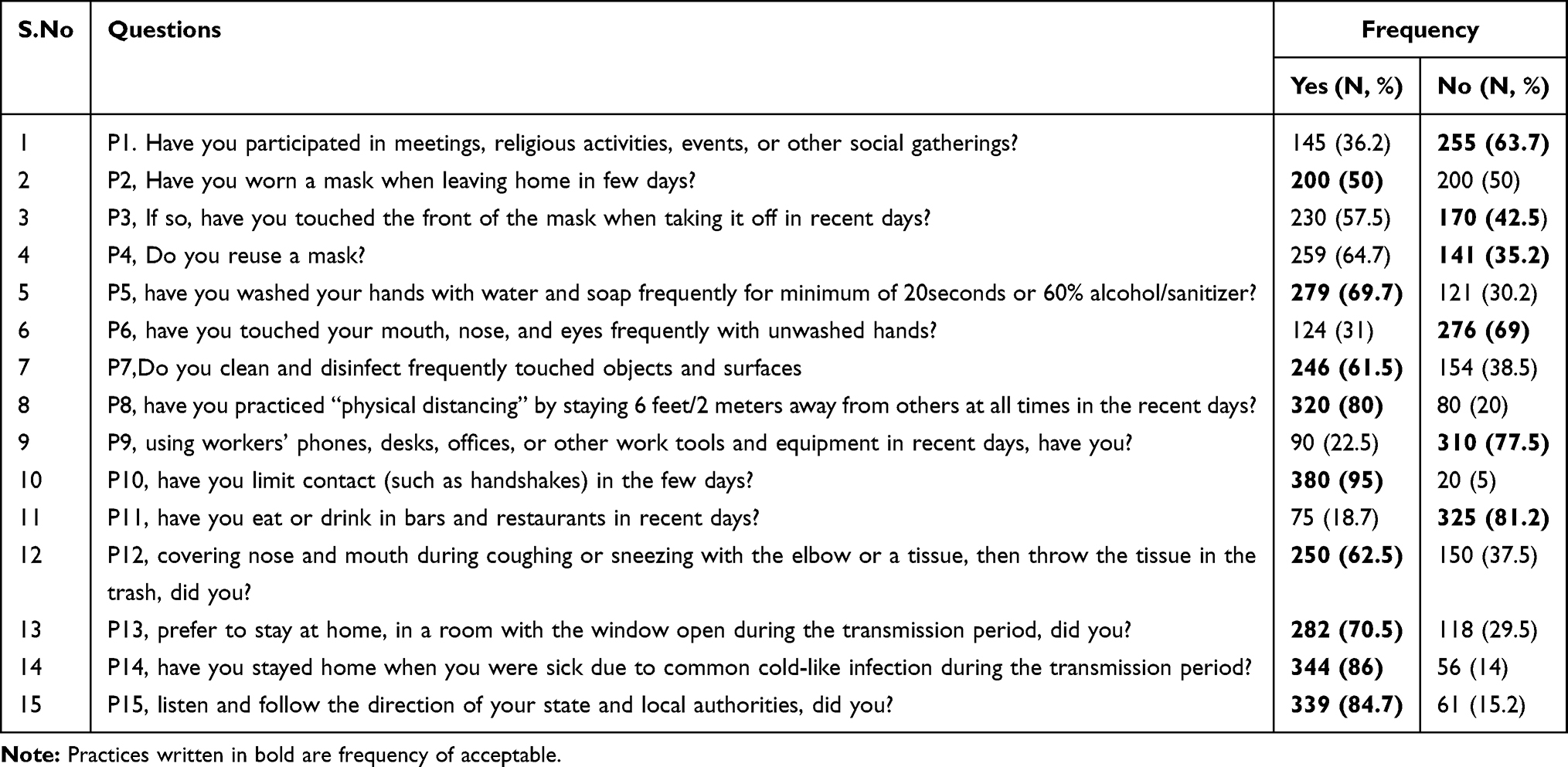 |
Table 2 Frequency of Response for Practice Questions Among Adigrat Residents, Tigray, Northern Ethiopia, 2020 (N=400) |
Preventive Practices Predictors Toward COVID-19
The multivariable analysis showed that, Age of 20–29 (AOR=2.1, 95% CI (1.9–6.5)), occupation of unemployed (AOR= 1.5, 95% CI (1.42–1.98)), marital status of unmarried (AOR=1.9, 95% CI (1.2–12.5)), and educational status of cannot read and write (AOR=2.1, 95% CI (2.08–9.34)) were factors associated with poor practice toward COVID-19. The Hosmer-Lemeshow goodness of fit test (p = 0.315) provides evidence of model fit with the predictor (Table 3).
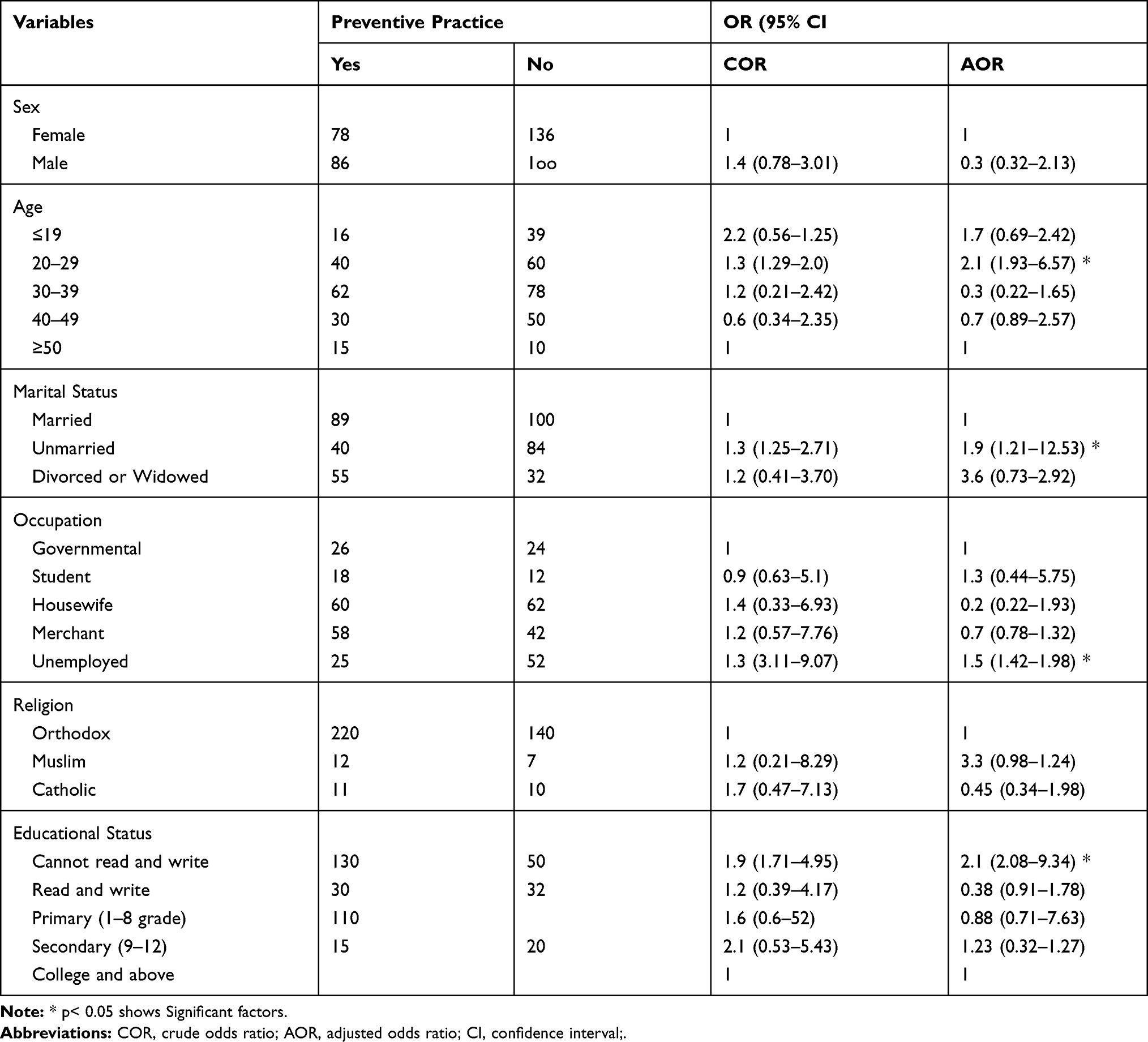 |
Table 3 COVID-19 Preventive Practices Predictors Among Adigrat Residents, Tigray, Ethiopia, October 2020 (n = 400) |
Discussion
The global COVID-19 pandemic is an unprecedented crisis, unlike any since the end of the Second World War.5 It is the most powerful sign to-date of what happens when uncontrolled expansion of human activity collides with the realities and boundaries of the planet.5 However, there is limited study on the preventive measure toward COVID-19 particularly in the study area. So, the study was carried out to assess the preventive practice to prevent COVID-19 and factors associated with it.
The finding showed that the prevalence of poor practice toward COVID-19 was 32.2% (95% CI (31.5–38.5%)); 95% had avoided hand shaking, 86% stayed at home when they were sick due to common cold-like infection during the transmission period, and 84.7% of the household head listen and follow the direction of the state and local authorities. Reuse of a mask (35.2%), touch the front of the mask when taking it off (42.5%), and wearing a mask were less practiced preventive methods. This may directly increase the risk of infection to coronavirus. This result is higher than study conducted in Iran (30%),22 and China (10%).23 On the contrary, it is lower than studies done in Cameron (40%),24 and in Ethiopia (47.3%).20 The difference could be due to discrepancy in the study area, difference for media exposure, sources of information difference, frequency of media exposure, knowledge, difference in information searching action, and difference in the source populations concern related to the pandemic which lead to the variant actions in the use of suggested preventive measures toward COVID-19. The measure employed by the government to contain the disease may bring a significant difference in which during our study there was no regional and national emergency state as result the community preventive practice may be decreased. Moreover, the study population religion, beliefs and culture may affect the practice in which in our study 90% of the study participants were orthodox where people can gather for religious ceremonies at the church.
The odds of poor practice among the age of 20–29 participants were 2.1 times higher than the age group of ≥50. This might be due to the misconception about the disease in which young people believe that COVID-19 is the disease of people with chronic disease and older age, and younger people engaged in risky behaviors as result it can decrease the practice. This is in line with study done in Iran,22 and China.23 But it is inconsistent with the study done in Ethiopia.
Study participant with the occupational status of unemployed were 1.5 times higher to practice poorly than those of governmental employer. This may be due to unemployed individuals may not afford the cost of mask, and soap, and they may not stay at home in order to search work. Moreover, people who are food insecure due to unemployment are more likely to participate in social gathering like wedding in order to get food. This is similar with study done in Ethiopia,18 Iran,22 and China.23
Study participants with marital status of unmarried were 1.9 times higher than married. Explanation for this could be the married one may think that they have the responsibility to take precaution for the sake of others, may be influenced by their partner, their partner may also remind them to practice the preventive measures, while those of without partner may not have someone to bother and as a result take actions less to prevent the disease. In addition, when individuals have partner, she/he will bother about infecting her/his partner because of his/her inappropriate action to prevent the disease. So, they choose to practice the preventive measures appropriately.
The odds of poor practice among participants with educational status of ”cannot read and write” were 2.1 times higher than study participants with educational status of “college and above”. This result was in line with a finding from Iran,22 and in Ethiopia20 in which poor practice was reported to be higher among study participant with lower level of education. The reason could be education is one of the controlling factors that affect healthy actions. There might be challenge in seeking information to be informed about the preventive methods and may not practice appropriately people those with low educational status. As one is not educated, there will be difficulty of acquiring information to understand the preventive measures toward COVID-19 and may not practice appropriately. Alongside, when someone is unable to read and write she/he may not have a better way of searching the right information as a result they may practice the preventive practice in wrong way, and the potential to apply the suggested preventive measure will decrease. Furthermore, education results in stronger information gathering custom and guide to appropriate use the preventive measures toward COVID-19.
Conclusions
This study showed that prevalence of poor practice was 32.2% among Adigrat town residents which were significantly low to prevent the pandemic disease. Reuse of a mask, touch the front of the mask when taking it off, and wearing a mask were practiced less frequently. Being age of 20–29, being unemployed, being unmarried and educational status of cannot read and write were statistically significant factors to prevent COVID-19. It would be helpful if the health professionals or other volunteers inform the community continuously by giving health educations regarding the preventive ways to increase the practice.
Limitation of the Study
In this study only the socio demographic factors were assessed, but there might be other factors which can affect the preventive measures toward COVID-19 prevention. The study was done using cross-sectional design; it might not show the temporal relationship between the dependent and independent variable.
Abbreviations
AOR, adjusted odds ratio; SARS-CoV-2, severe acute respiratory syndrome corona-2; ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; WHO, World Health Organization; CI, confidence interval.
Data Sharing Statement
The datasets used and/or analyzed during the current study are accessible from the principal author (Fre Gebremeskel Ftwi) on reasonable request.
Ethical Approval and Consent to Participate
Prior to the data collection study ethical approval was obtained from the Research and Ethical Committee of Tigray Health Research institute on 04|01×2013 E.C. Besides, written informed consent was obtained from the respondents before data collection. The respondents’ privacy, right to anonymity, right to refuse, confidentiality was respected all the time. Moreover, those respondents were also briefed about the aim and benefit of the study. The interviewers wore protective face masks. Appropriate physical distance was practiced between the interviewer and interviewee during data collection. Appropriate hand washing and alcohol-based practice was also practiced during the data collection time. The potential risk was minimal at the time of the study. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to express our gratitude to the study participants for their kind and cooperative participation during the data collection.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Home - Johns Hopkins coronavirus resource center [Internet]. Available from: https://coronavirus.jhu.edu/.
2. Bizzoca ME, Campisi G, Lo Muzio L. Covid-19 pandemic: what changes for dentists and oral medicine experts? A narrative review and novel approaches to infection containment. Int J Environ Res Public Health. 2020;17(11). doi:10.3390/ijerph17113793
3. Hui DS, Azhar E I, Madani TA. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health - the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020;91:264–266. doi:10.1016/j.ijid.2020.01.009
4. Meselson M. Droplets and aerosols in the transmission of SARS-CoV-2. N Engl J Med. 2020;382(21):2063. doi:10.1056/NEJMc2009324
5. UN Socio-economic Assessment of COVID-19 in Ethiopia | United Nations in Ethiopia [Internet]; 2021. Available from: https://ethiopia.un.org/en/49388-un-socio-economic-assessment-covid-19-ethiopia.
6. Amerio A, Bianchi D, Santi F, et al. Covid-19 pandemic impact on mental health: a web-based cross-sectional survey on a sample of Italian general practitioners. Acta Biomed. 2020;91(2):83–88. doi:10.23750/abm.v91i2.9619
7. Holmes EA, O’Connor RC, Perry VH, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–560. doi:10.1016/S2215-0366(20)30168-1
8. Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. 2020;383(6):510–512. doi:10.1056/NEJMp2008017
9. Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: address mental health care to empower society. Lancet. 2020;395(10224):e37–8. doi:10.1016/S0140-6736(20)30309-3
10. Moreno C, Wykes T, Galderisi S, et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry. 2020;7(9):813–824. doi:10.1016/S2215-0366(20)30307-2
11. Shi L, Lu Z-A, Que J-Y, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in china during the coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3(7):e2014053. doi:10.1001/jamanetworkopen.2020.14053
12. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. 2020;89:531–542. doi:10.1016/j.bbi.2020.05.048
13. Kang L, Ma S, Chen M, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain Behav Immun. 2020;87:11–17. doi:10.1016/j.bbi.2020.03.028
14. Costanza A, Marco SD, Burroni M, et al. Meaning in life and demoralization: a mental-health reading perspective of suicidality in the time of COVID-19. Acta Biomed. 2020;91(4):e2020163–e2020163. doi:10.23750/abm.v91i4.10515
15. Gunnell D, Appleby L, Arensman E, et al. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry. 2020;7(6):468–471. doi:10.1016/S2215-0366(20)30171-1
16. [Internet]. Availablefrom: http://www.salute.gov.it/portale/uovocoronavirus/homeNuovoCoronavirus.jsp?.
17. Baloch S, Baloch MA, Zheng T, Pei X. The Coronavirus Disease 2019 (COVID-19) pandemic. Tohoku J Exp Med. 2020;250(4):271–278. doi:10.1620/tjem.250.271
18. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University medical center visitors, Southwest Ethiopia [Internet]. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0233744.
19. Adigrat. In: Wikipedia [Internet]; 2021. Available from: https://en.wikipedia.org/w/index.php?title=Adigrat&oldid=1021643925.
20. Knowledge, attitude and practice towards COVID-19 among chronic disease | IDR [Internet]; 2021. Available from: https://www.dovepress.com/knowledge-attitude-and-practice-towards-covid-19-among-chronic-disease-peer-reviewed-fulltext-article-IDR.
21. Seid M, Seid M. Knowledge and attitude towards antimicrobial resistance among final year undergraduate paramedical students at University of Gondar, Ethiopia. BMC Infect Dis. 2018;18. doi:10.1186/s12879-018-3199-1
22. Honarvar B, Lankarani KB, Kharmandar A, et al. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health. 2020;65(6):731–739. doi:10.1007/s00038-020-01406-2
23. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
24. Ngwewondo A, Nkengazong L, Ambe LA, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. 2020;14(9):e0008700. doi:10.1371/journal.pntd.0008700
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.