")
Back to Journals » International Journal of Women's Health » Volume 12
Prevalence, Risk Factors and Effects of Domestic Violence Before and During Pregnancy on Birth Outcomes: An Observational Study of Literate Omani Women
Authors Al Shidhani NA, Al Kendi AA, Al Kiyumi MH
Received 16 July 2020
Accepted for publication 12 October 2020
Published 28 October 2020 Volume 2020:12 Pages 911—925
DOI https://doi.org/10.2147/IJWH.S272419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Nuhour Ali Al Shidhani,1 Asma Ali Al Kendi,1 Maisa Hamed Al Kiyumi2
1Ministry of Health, Muscat, Oman; 2Department of Family Medicine and Public Health, Sultan Qaboos University Hospital, Muscat, Oman
Correspondence: Maisa Hamed Al Kiyumi
Sultan Qaboos University Hospital, P.O.Box 35, P.C.123, Al-Khod, Sultanate of Oman
Tel +0096824141127
Email [email protected]
Background: Domestic violence against women before and/or during pregnancy is a concerning public health issue. It has a deleterious impact on both the mother and the baby.
Aim: The aim of this study is to identify the prevalence and predictors of emotional and physical domestic violence during three periods (lifelong, one year before pregnancy and during pregnancy). Moreover, it evaluates the effects of domestic violence on the outcomes of pregnancy, including miscarriages, birth weight of the baby, gestational age at delivery, and mode of delivery.
Methodology: This is a prospective observational study of literate pregnant women, attending four primary health-care centers in Muscat, from 1st April 2019 to 31st March 2020. Subjects with twin pregnancies were excluded from the study. The validated Arabic NorVold Domestic Abuse Questionnaire (NORAQ) was used to determine the prevalence of emotional and physical domestic violence. The recruited subjects were re-evaluated for birth outcomes at 2– 4 weeks postpartum.
Results: A total of 960 women participated in the study, with the mean age of 30.3 ± 5.4 years. Overall, experiences of lifelong domestic violence were reported by 161 women (16.8%), and the prevalence rate declined substantially in the one-year period preceding pregnancy and during pregnancy, 2.7% and 1.6%, respectively. Women who reported any type of domestic violence one year before pregnancy were at a higher risk of experiencing it again during pregnancy. A multivariate analysis of the obtained data revealed a strong association between physical domestic violence one year before pregnancy and unplanned pregnancy. Subjects with lifelong domestic violence reported higher rates of depression, insomnia, and somatic symptoms. No significant association was found between domestic violence, across any periods, and birth outcomes.
Conclusion: The rates of domestic violence are relatively lower during pregnancy and one year before pregnancy compared to those of the lifelong period among Omani women. A significant association was found between domestic violence and depression, insomnia, somatic symptoms, and unplanned pregnancy. Screening for domestic violence during the perinatal period, using high-quality surveys, is of utmost importance.
Keywords: domestic violence, women, pregnancy, risk factors, birth outcomes, Oman
Introduction
Violence against women is a concerning and global public health issue with a worldwide prevalence rate of 35%.1 It is defined as any act of gender-based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life.2 Generally, there is a fragmented evidence of the prevalence of intimate partner violence (IPV) among Arab countries with a range of 6–59% for physical violence, and 5–91% for emotional violence.3 Domestic violence (DV), during pregnancy, has drawn a high level of scrutiny in recent years, given its potential negative impacts on both the mother and the baby. The WHO’s multi-country study showed that the prevalence of IPV during pregnancy is ranging from 1% to 28%.4 Few studies addressing IPV during pregnancy in Arab countries have been conducted, of which the highest prevalence was reported in Egypt followed by Saudi Arabia, with rates of 44.1%, and 21%, respectively.5,6
Although pregnancy is thought to cause the evolution of DV, no definite evidence exists on its role and influence.4 Besides, it is still debatable whether pregnancy is a risk or a protective factor for DV. A study corroborated a decrease in IPV during pregnancy while other studies underlined higher or unchanged prevalence rates.7–9 There are different patterns of violence against women around the time of pregnancy with some cases commence only during pregnancy while others may terminate at pregnancy. Another pattern has been identified in the literature, which may reveal the persistence of violence before and during pregnancy.7,10,11
Several risk factors for DV against women exist with inconclusive evidence. A history of IPV, lack of social support, lower educational level of the woman, and unplanned pregnancy were considered to be among the significant predictors of DV during pregnancy.11–14 A recent study of DV in Oman, which included all women regardless of their pregnancy status, revealed that alcohol consumption of the spouse was a significant risk factor.15 Interestingly, father, husband/ex-husband, and brother were the main perpetrators of DV against Omani women in that study.15
DV during pregnancy imposes risks for both the mother and the baby. Such risks might be fatal such as suicide and homicide. Notably, a systematic review substantiated that IPV was the main cause of about one-third of female homicide.16 Other adverse effects include physical and/or mental impairment of the mother such as sustaining pain, depression, and insomnia. Importantly, deleterious effects of DV on birth outcome may include miscarriages, low birth weight of the baby, preterm labor, and lack of attachment to the child.4,17
While there was no prior study addressing the DV among pregnant women in Oman, a recent study of antenatal depression revealed a significant association between antenatal depression and marital conflicts.18 Furthermore, a significant association between antenatal depression and delivery by cesarean section was observed.19 However, the exact meaning and the extent of marital conflicts were not adequately measured.18 Thus, there is a need to study DV in pregnant women and its effects on pregnancy outcome in a greater depth. The present study identifies the prevalence rate and predictors of emotional and physical DV among pregnant literate Omani women. Additionally, it determines the potential effects of DV on the outcomes of pregnancies, particularly miscarriage, birth weight of the baby, gestational age at delivery, and mode of delivery.
Methodology
This is a cross-sectional study, followed by a prospective cohort study at which the baseline assessment was utilized as a cross-sectional design to study the prevalence and risk factors of DV and the follow-up assessment was utilized for outcomes measurement. It included any pregnant Omani woman attending antenatal clinics in primary health-care centers (PHC) in Al Seeb Wilayat (province), which is the most populated Wilayat under the Muscat governorate. Four out of nine primary health-care centers were randomly selected, and a consecutive sampling was performed. All literate women (able to read and write) at any gestational age, attended the antenatal clinics at any of the aforementioned PHCs, were identified by well-trained investigators and invited to participate in our study. Women with multiple pregnancies (ie, twin pregnancies) were excluded from the study. A written informed consent was obtained from pregnant women who agreed to participate. In the next step, the consented women were given a self-administered questionnaire to be completed anonymously in a private place. The questionnaire consisted of two parts. Part one is about sociodemographic features such as age, gestational age which was calculated by last menstrual period, planning for pregnancy, education level (of the participant, her husband, and parents), income, occupation of the participant and her husband, number of household family members, previous pregnancy outcomes (ie, low birth weight LBP <defined as birth weight of <2.5 kg,20 preterm birth PTB <defined as birth at <37 weeks of gestation>20, miscarriages, stillbirth and cesarean sections), weight, height, last hemoglobin level, smoking, and alcohol consumption. Part two of the questionnaire consists of the Arabic NorVold Domestic Abuse Questionnaire (NORAQ). NorVold Domestic Abuse Questionnaire (NORAQ) is a reliable and well-validated self-administered scale that determines the prevalence of emotional, physical, and sexual violence.21–23 It consists of the following parts: 1) General physical and mental health assessments; 2) Questions about emotional, physical, sexual violence and abuse in health-care system; 3) General questions related to violence such as help-seeking behaviors. An initial pilot study to check for the clarity of questions was conducted; however, many participants were noticed to be reluctant in answering questions related to sexual violence and left that section unanswered. Therefore, only emotional and physical violence were included in the current study. Additionally, abuse in the health-care system was excluded as it was out of the scope of the current study. Recruited women were followed up until 2–4 weeks after delivery for an assessment of birth outcomes (ie, birth weight of the baby, gestational age at delivery, miscarriages, and mode of delivery). The study was carried out between 1st April 2019 and 31st March 2020 and conducted in accordance with the Declaration of Helsinki.
Emotional DV is further classified into mild, moderate or severe, if the woman responds positively to any of the following questions, respectively: (i) “Have you experienced anybody, systematically and for any longer period, trying to repress, degrade, or humiliate you?”, (ii) “Have you experienced anybody, systematically and by threat or force, trying to limit your contacts with others, or totally control what you may and may not do?”, (iii) “Have you experienced living in fear because somebody, systematically and for a longer period, has threatened you or somebody close to you?”21 Similarly, mild, moderate, and severe physical DV is determined by a positive response to any of the following questions, respectively: (i) “Have you experienced anybody hitting you, smacking your face, or holding you firmly against your will?”, (ii) “Have you experienced anybody hitting you with his/her fist(s) or with a hard object, kicking you, pushing you violently, giving you a beating, thrashing you, or doing anything similar to you?”, (iii) “Have you experienced anybody threaten your life by, for instance, trying to strangle you, showing a weapon or a knife, or by any other similar act?”21
Sample Size
The sample size for the present study was calculated by using the Openepi version 3 software,24 and based on an anticipated prevalence rate of domestic violence during pregnancy of 21% from a previous study,6 an absolute precision of 3%, a confidence level of 95%, and a population size of 5000 (based on the total number of pregnant women attending the four primary health-care centers during the study period), the minimum required sample size was found to be 621 subjects.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) version 26 was used for data analysis. Sociodemographic features and participants’ responses were determined by performing a descriptive analysis of the data. The association between DV and different risk factors and outcome of pregnancy was assessed by Chi-Square testing. A multivariate analysis was conducted to mitigate the effects of confounders. A P value of ≤0.05 was considered to be statistically significant.
Results
A total of 1024 subjects were invited to participate in the study. Nine hundred sixty subjects agreed to participate, which corresponded to a 93.8% response rate. Non-responders were similar to recruited subjects in terms of sociodemographic characteristics, and lack of time was the main reason for declining to participate. The mean age of recruited subjects was 30.3 ± 5.4 years, and almost half of them were employed (438, 45.6%). The majority of subjects and their spouses (>90%) had attained secondary or higher educational level. Additionally, more than half of the subjects (536, 55.8%) were married for more than five years, and about two-thirds were recruited at a gestational age of less than 28 weeks (669, 69.7%). Moreover, one-third declared that their pregnancy was unplanned (319, 33.2%, Table 1).
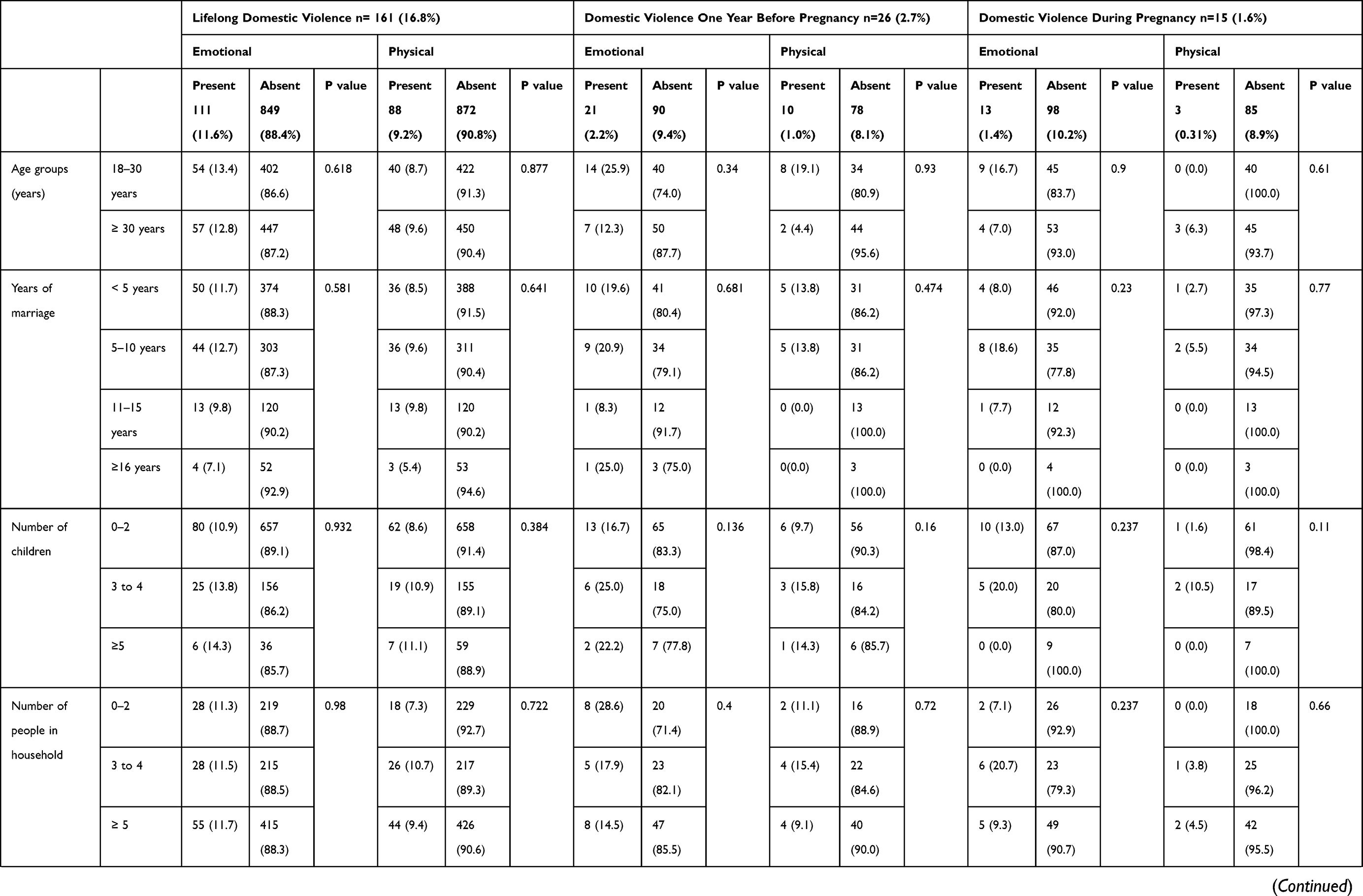 | 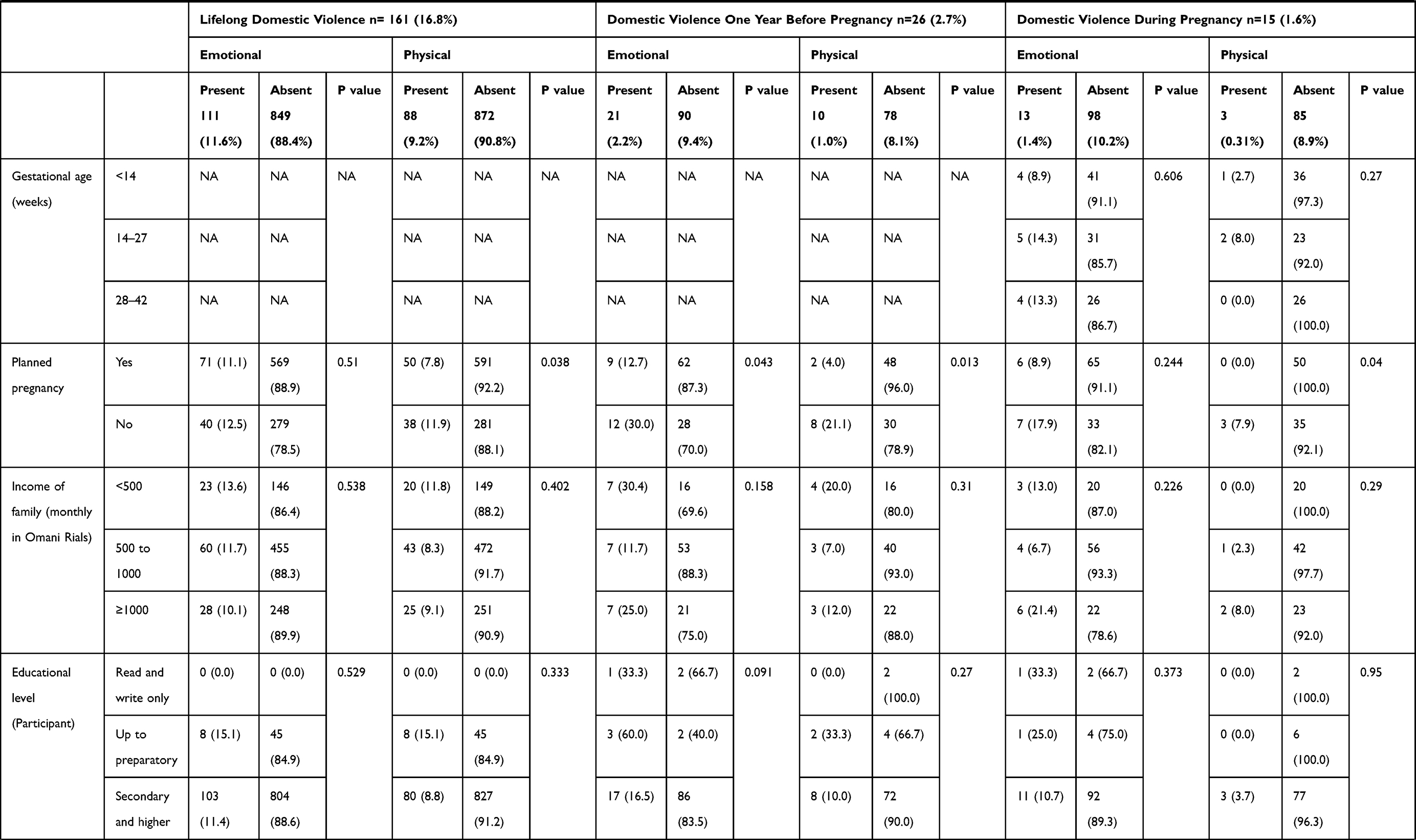 | 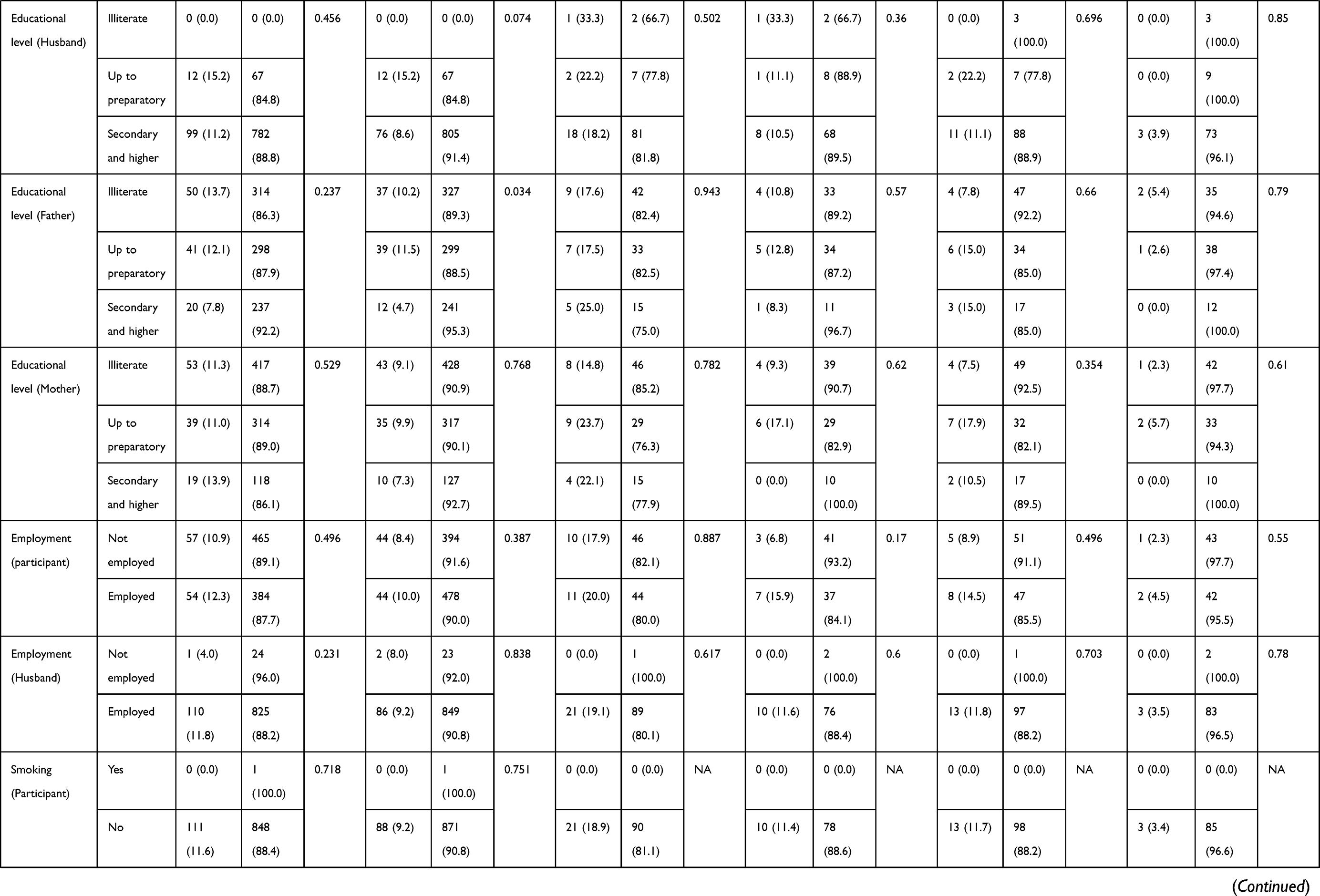 | 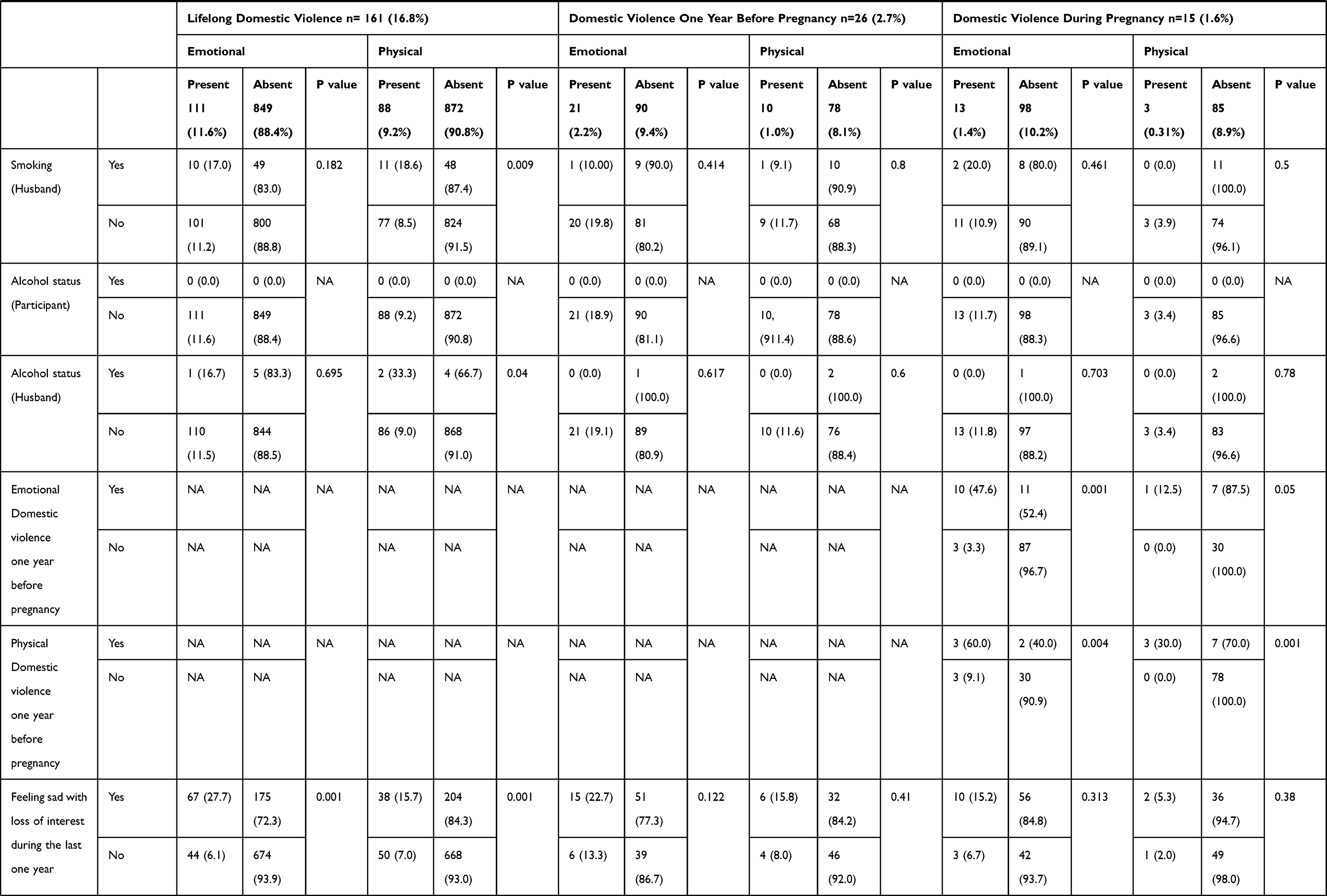 |
Table 1 Comparison of Baseline Characteristics and Risk Factors in Subjects Having Domestic Violence Across Any of the Three Periods (Lifelong, One Year Before Pregnancy and During Pregnancy) and Those Not Having Domestic Violence (N= 960) |
Overall, occurrences of lifelong DV were reported by 161 women (16.8%), of which 111 subjects (11.6%) had emotional DV, 88 (9.2%) had physical DV, and 38 (4.0%) had both emotional and physical DV. Notably, the prevalence rate of DV declined substantially in the one-year period preceding pregnancy and during pregnancy, which accounts for 2.7% and 1.6%, respectively. Emotional DV was the most common type of DV across all three periods (one year before pregnancy, during pregnancy and lifelong) (Table 2). Subjects with DV were advised to seek help from the nearest primary health-care center.
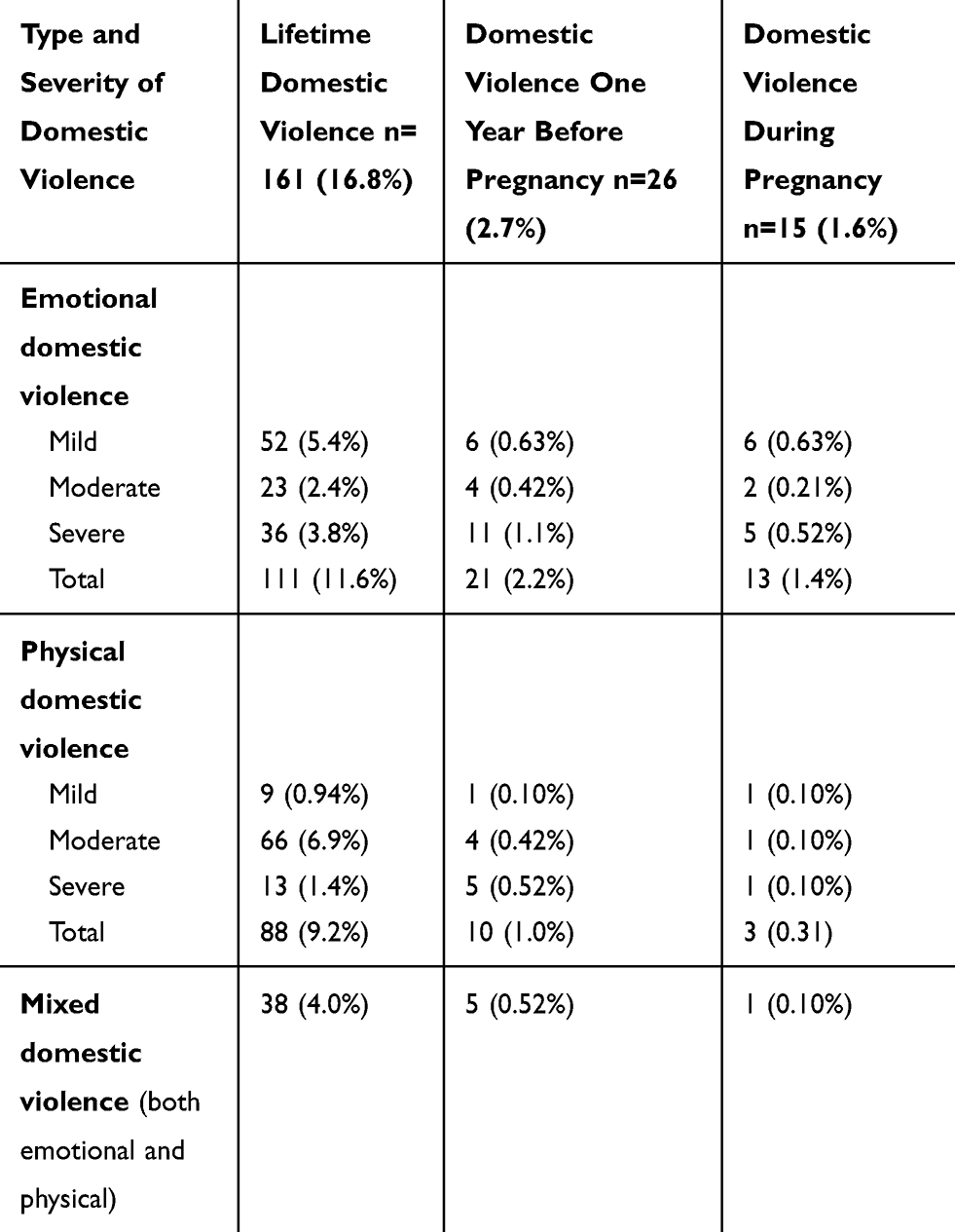 |
Table 2 Prevalence and Severity of Overall and Sub-Types of Domestic Violence (n=960) |
Univariate analysis of the data revealed a significant association between unplanned pregnancy and any type of DV during the one-year period before pregnancy. Similarly, unplanned pregnancy was found to be a significant predictor for physical (but not emotional) DV during pregnancy, and lifelong periods. Surprisingly, experiencing any type of DV one year before pregnancy was identified to be a strong predictor for DV during pregnancy. For example, 10 out of 21 subjects who experienced emotional DV during the last one year before pregnancy also reported another episode of emotional DV during pregnancy. Also, the educational level of the father and smoking and alcohol consumption status of the victim’s husband were deemed significant predictors for physical lifelong DV. Importantly, subjects with lifelong DV reported higher rates of depression, insomnia, and somatic symptoms (Table 1).
In the multivariate analysis, a significant association was identified between physical DV one year before pregnancy and unplanned pregnancy. Additionally, depression, insomnia, and somatic symptoms were significantly associated with lifelong DV. Notably, the educational level of the father and smoking and alcohol status of the husband rendered non-significant predictors of DV (Table 3).
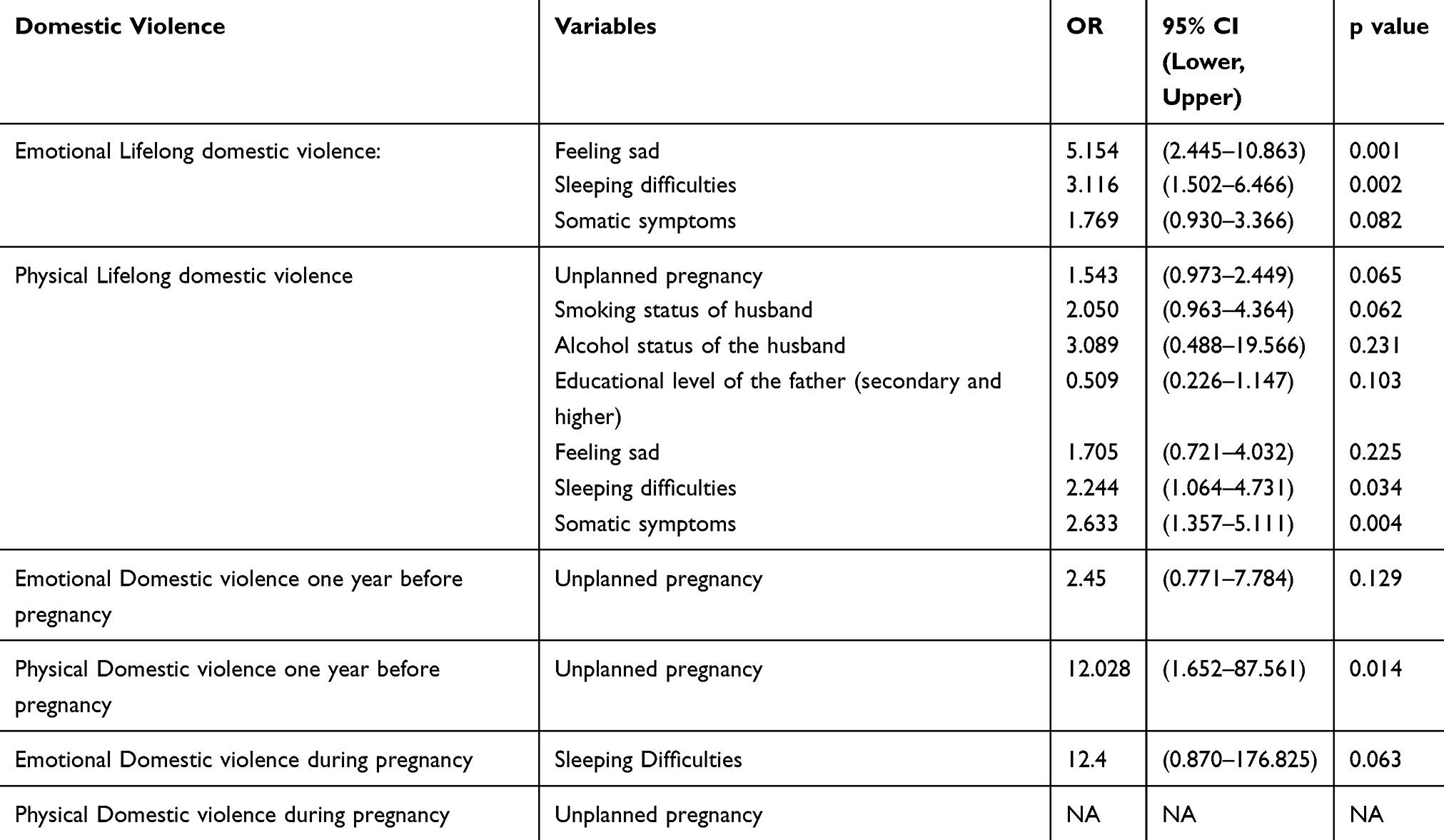 |
Table 3 Logistic Regression Analysis to Study the Likelihood That Women with Risk Factors Have Domestic Violence (n=960) |
Fifty-nine women did not respond to follow-ups and could not be approached despite our frequent attempts to contact them by phone, which corresponded to a 6.1% loss of follow up. Also, 29 women reported miscarriages at first and second trimesters.
No significant association was found between any type of DV across any periods and pregnancy outcomes (ie, low birth weight, preterm labor, delivery by cesarean section, and miscarriages) (Table 4). While the majority (about 80%) of subjects with lifelong DV reported being abused by their fathers, brothers, and husbands/ex-husbands, violent act perpetrated by husbands/ex-husbands predominated both during pregnancy and one year before pregnancy (53.3% and 57.7%, respectively) (Figure 1).
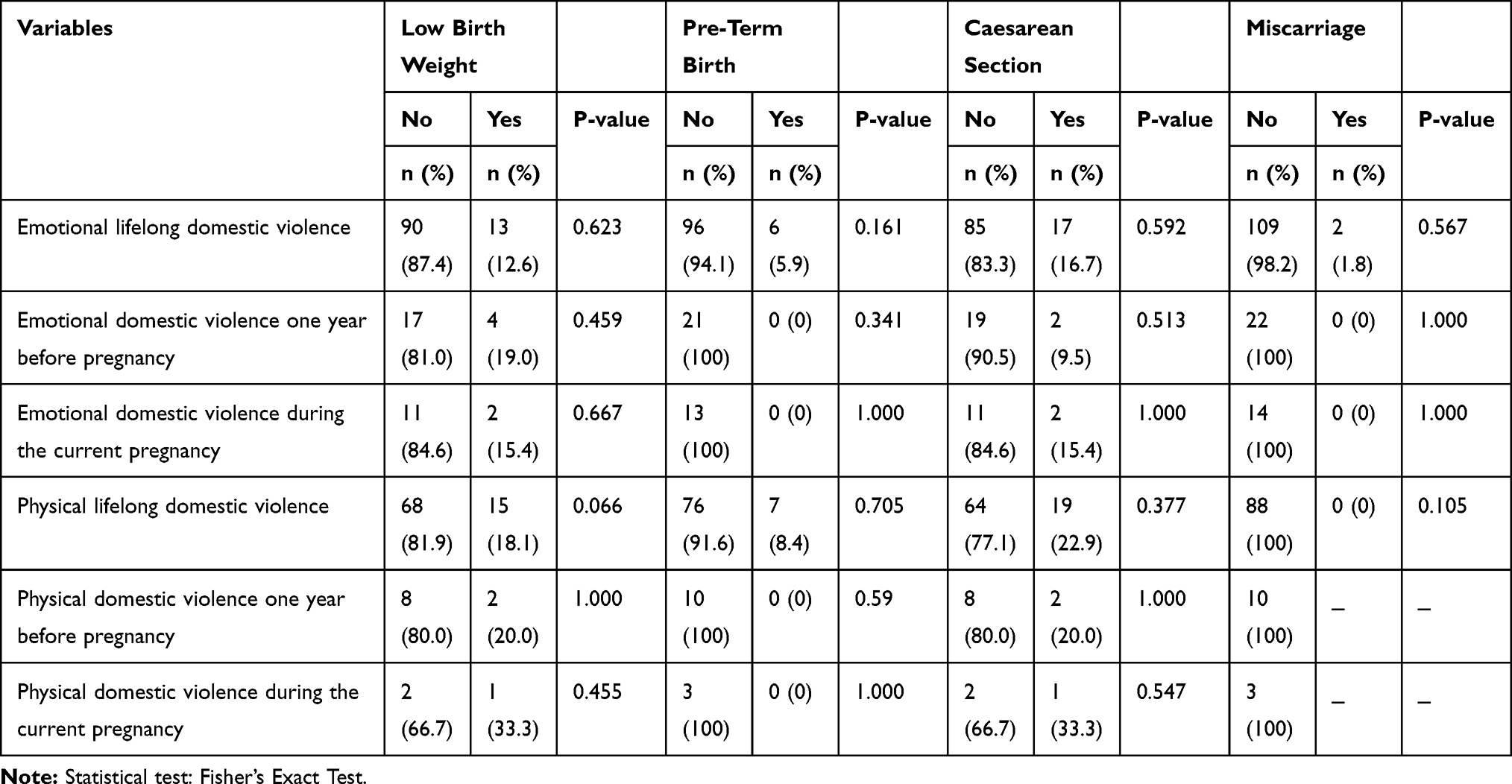 |
Table 4 Association Between Domains of Domestic Violence and Birth Outcomes |
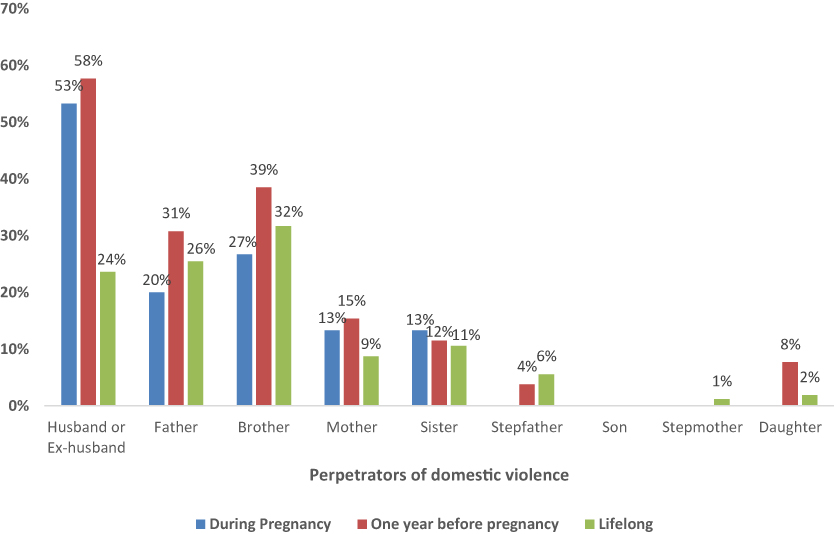 |
Figure 1 Perpetrators of domestic violence during the three periods: during pregnancy, one year before pregnancy, and lifelong. Husbands/ex-husbands were the main perpetrators one year before pregnancy and during pregnancy. For lifelong domestic violence, the majority of subjects reported being abused by their fathers, brothers, and/or husbands/ex-husbands. |
Discussion
Our study revealed that lifelong DV was reported by approximately one-fifth of pregnant women, and only a minority (1–2%) experienced DV during pregnancy or during the one-year period preceding pregnancy. DV during the one year before pregnancy is considered to be a strong predictor for experiencing DV during pregnancy. Moreover, a significant association between physical DV one year before pregnancy and unintended pregnancy was identified. Furthermore, women with lifelong DV exposures reported higher prevalence rates of depression, insomnia, and somatic symptoms. No significant impact of DV on birth outcomes has been found in the current study.
In Oman, the average age at marriage is about 26 years and there is a law that set the age of 18 years as the minimum age of marriage.25 A fertility rate of 2.89 per woman was reported in 2018.26 The number of registered divorce cases increased from 2521 in 2010 to 3370 in 2019.27 As per religious rules, a husband has the right to divorce his wife by repudiation. However, women also have the right to get divorced in some situations such as harm or financial rights.25 Remarkable progress of women’s rule has been noticed during the last two to three decades. For example, about two-thirds of jobs in education and health sectors were occupied by women.27 Besides, women’s participation in national parliaments has doubled during the last twenty years, albeit it is far lower when compared to men’s participation (15 women versus 154 men in 2018).27 Similarly, women’s involvement in top, middle and direct management has increased by more than threefold during the last ten years.27 As for all Omanis, pregnant women receive free antenatal care at the primary health-care center. However, there is no screening program to detect domestic violence in Oman. Besides, no specific policy or legislation is currently available and victims of abuse used to report to the local primary health-care center, where they will be assessed by a general practitioner and the case is filed to the police upon victims’ request. Occasionally, abused women may report directly to the Ministry of Social Development.
Our findings delineated a relatively low prevalence rate of DV during pregnancy, which is much lower than what has been reported in other Arab countries such as Egypt and Saudi Arabia.5,6 However, it is within the range of the WHO overall prevalence of IPV during pregnancy (1–28%) and is comparable with other studies.4,28 Also, our study corroborated the existence of an even lower rate of DV during pregnancy in relation to the pre-pregnancy period. Such patterns of violence, which decrease or cease during pregnancy, are consistent with studies elsewhere.11,29,30 Besides, the majority of recruited women who reported being abused during pregnancy had experienced previous episodes of DV one year before pregnancy, suggesting that violence during pregnancy may represent a continuation of a preexisting violence.11,29 Emotional DV was the most common type of abuse disclosed by recruited subjects across all the three periods (during pregnancy, one year before pregnancy and lifelong), which is consistent with the research literature.5,11 A lower prevalence rate of DV, one year before and during pregnancy, in the current study, could be ascribed to high educational status of both the participants and their spouses compared to prior studies that substantiated higher prevalence of DV during pregnancy.31 Additionally, recruiting women at any gestational age, especially the first and second trimesters, may lead to missing those who developed DV at later stages of pregnancy, and thereby underestimating the true prevalence of DV in our sample. Those women constituted about two-thirds of the current sample. However, this hypothesis will not explain the low prevalence of DV one year before pregnancy, which may indicate a true low prevalence of DV in the current sample. Although not yet clear, increased awareness of health and using different tactics to mitigate vulnerability to abuse during pregnancy may account for the lower prevalence of DV during pregnancy compared to one year before pregnancy.11
Interestingly, a significant proportion of women with physical DV one year before pregnancy reported that their current pregnancy was unplanned. Due to the temporal precedence of DV before pregnancy and planning of pregnancy, a potential causal relationship between these two variables might be inferred. A similar finding by the WHO multi-country study has shown that an average of 38% of women with DV reported that their pregnancy was unplanned and untimed.32 Similarly, several other studies have identified the IPV around the pregnancy period as a strong predictor for unplanned pregnancy.13,33–35 Lack of fertility control that resulted from fear and low self-esteem experienced by DV victims who might live under man control may be ascribed to the high prevalence of unintended pregnancy.
Besides being a violation of the human rights, lifelong DV has imposed negative consequences on mental and physical health in the current analysis. This was reflected by the higher prevalence of depression, anxiety, insomnia, and somatic symptoms among women with lifelong DV in the current study. Such a strong association has been extensively studied elsewhere,36 and a recent systematic review that included 19,101 women substantiated increased odds of depression and insomnia among victims of DV.17 Besides, the higher prevalence of somatic symptoms in the current cohort supports the theory of somatoform disorders in which psychological distress is translated into somatic complaints.37
Our analysis did not show any significant association between DV across any of the three periods and pregnancy outcomes. Indeed, controversial evidence exists about the impact of DV on pregnancy outcomes and our findings contradict what have been reported in the literature.5,28,38–40 A recent meta-analysis that included 50 studies attempted to explore the impact of IPV during pregnancy on birth outcomes, showed increased risks of preterm birth, low birth weight, and small for gestational age.39 However, significant heterogeneity was observed between the included studies (I2 =84% for preterm, and 91% for low birth weight).39 Another study that included 818 women with any type of IPV during pregnancy substantiated higher odds for preterm, low birth weight, and miscarriages.5 Nonetheless, our results are consistent with other studies that did not show a significant association between DV during pregnancy and preterm labor and/or low birth weight.41–43 The very low prevalence of DV during pregnancy in the current cohort might be a possible explanation for the non-significant association with pregnancy outcomes.
Implications and Recommendation
This is the first study assessing DV before and during pregnancy and its impact on birth outcomes in Oman. Moreover, this study will add a supplementary dataset to the existing fragmented evidence of DV during the perinatal period in the Middle East region. Despite the low prevalence rate of DV one year before pregnancy and during pregnancy in the current cohort, it is important to emphasize that lifelong DV is not uncommon and imposes deleterious effects on the mental and physical wellbeing of pregnant women. Based on our findings, the following recommendations are deemed important: i) More investment in assessing the prevalence of DV and implementing a suitable and early intervention to mitigate its consequences is needed. This can be achieved by implementing a high-quality population-based survey such as Demographic and Health Survey (DHS) that ensures continuous and comprehensive evaluation of DV.44 Furthermore, reporting on the United Nations’ Sustainable Development Goals (SDG) that aim at eliminating all forms of violence against women will impose an implicit role in alleviating the burden of DV.44 ii) Strengthening the role of primary health-care institutions in screening women for DV during the preconception period and at each antenatal visit will reinforce early detection and intervention of women at risk of DV. Evidence suggests that health-care workers expressed feelings of inadequacy due to lack of knowledge and skills when dealing with patients with DV.45,46 A recent qualitative study that included twenty-four obstetricians and health personnel revealed a negative attitude towards including questions about DV at prenatal visits.46 Therefore, proper training of health-care practitioners on how to approach women with DV in a sensitive way constitutes a fundamental step. Different methods of training health-care professionals may increase their awareness and skills in dealing with patients with DV. For example, multifaceted physician training that aims to change physicians’ behavior through combining education with system support intervention was found to be effective in increasing reporting and referral of DV cases.47 It includes web-based learning, workshops and experiential training.47 iii) Supporting other services that enhance early detection, rapid access, and proper dealing with victims of DV such as counseling, hotline, and shelters are necessary as well.48 While there is considerable uncertainty about the best interventions for DV during the perinatal period, a promising positive effect of home visitation programs has been illustrated.49 Moreover, an integrated approach such as the ecological model might play a pivotal role in preventing IPV and mitigating its consequences. The ecological model is a comprehensive model that aims at providing guidelines for interventions to address IPV at four levels: individual, relational, organizational and community.50
Limitations
Our findings are subject to some limitations. First, excluding illiterate women might have affected the true prevalence rate of DV. Second, using self-administered questionnaire may lead to over- or underestimation of the true prevalence rate of DV. Third, this study did not include other types of violence against women such as sexual violence, which is an important area that is often overlooked. Fourth, screening pregnant women at early gestational age might pose a predilection for missing those who experienced DV during the later stage of pregnancy. Fifth, the use of consecutive sampling methodology may affect the generalizability of our findings.
Future Directions
As this is the first study conducted in Oman, more studies related to DV during pregnancy that include illiterate women are needed. Sexual DV before and during pregnancy is an important area that needs to be elaborated by using a qualitative type of research. Moreover, studies related to the proper intervention for DV and its effectiveness are deemed necessary. Finally, there is a need to study the pattern of DV in the postnatal period as well.
Conclusions
The prevalence of domestic violence during pregnancy and one year before pregnancy is low among Omani women compared to lifelong violence. While no significant association was found between DV and birth outcomes, the victims of lifelong domestic violence reported high rates of depression, insomnia, and somatic symptoms. Further, DV, one year before pregnancy, is a strong predictor of DV during pregnancy. Early detection and continuous monitoring of domestic violence during both the perinatal and lifelong periods, using high-quality population surveys, is essential in preventing the broad array of negative consequences. Besides, implementing a screening program at the preconception period and during each antenatal visit may help in mitigating the impacts of domestic violence.
Ethical Approval
Directorate General of Planning and Studies, Ministry of Health, MOH/DGPS/MG-34/2018.
Acknowledgment
We would like to thank women who participated in this study. We are also thankful to Mr. Sachin Jose and Dr. Sanjay Jaju for their help with statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Deanship of Research Fund, Sultan Qaboos University (RF/MED/FAMCO/19/02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Violence Against Women. World Health Organization; 2017.
2. Nations U. Declaration on the Elimination of Violence Against Women. New York: UN; 1993.
3. Elghossain T, Bott S, Akik C, Obermeyer CM. Prevalence of intimate partner violence against women in the Arab world: a systematic review. BMC Int Health Hum Rights. 2019;19(1):29. doi:10.1186/s12914-019-0215-5
4. World Health Organization. Intimate Partner Violence During Pregnancy. World Health Organization; 2011.
5. Ibrahim ZM, Sayed Ahmed WA, El-Hamid SA, Hagras AM. Intimate partner violence among Egyptian pregnant women: incidence, risk factors, and adverse maternal and fetal outcomes. Clin Exp Obstet Gynecol. 2015;42(2):212–219.
6. Rachana C, Suraiya K, Hisham AS, Abdulaziz AM, Hai A. Prevalence and complications of physical violence during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2002;103(1):26–29. doi:10.1016/S0301-2115(02)00022-2
7. Silva EP, Ludermir AB, Araújo TV, Valongueiro SA. Frequency and pattern of intimate partner violence before, during and after pregnancy. Rev Saude Publica. 2011;14(45):1044–1053. doi:10.1590/S0034-89102011005000074
8. Burch RL, Gallup Jr. GG. Pregnancy as a stimulus for domestic violence. J Fam Violence. 2004;19(4):243–247. doi:10.1023/B:JOFV.0000032634.40840.48
9. Martin SL, Mackie L, Kupper LL, Buescher PA, Moracco KE. Physical abuse of women before, during, and after pregnancy. JAMA. 2001;285(12):1581–1584. doi:10.1001/jama.285.12.1581
10. Ballard TJ, Saltzman LE, Gazmararian JA, Spitz AM, Lazorick S, Marks JS. Violence during pregnancy: measurement issues. Am J Public Health. 1998;88(2):274–276. doi:10.2105/AJPH.88.2.274
11. Van Parys AS, Deschepper E, Michielsen K, Temmerman M, Verstraelen H. Prevalence and evolution of intimate partner violence before and during pregnancy: a cross-sectional study. BMC Pregnancy Childbirth. 2014;14(1):294. doi:10.1186/1471-2393-14-294
12. Nguyen TH, Ngo TV, Nguyen VD, et al. Intimate partner violence during pregnancy in Vietnam: prevalence, risk factors and the role of social support. Glob Health Action. 2018;11(sup3):1638052. doi:10.1080/16549716.2019.1638052
13. Yakubovich AR, Stöckl H, Murray J, et al. Risk and protective factors for intimate partner violence against women: systematic review and meta-analyses of prospective–longitudinal studies. Am J Public Health. 2018;108(7):e1. doi:10.2105/AJPH.2018.304428
14. Bifftu BB, Dachew BA, Tadesse Tiruneh B, Zewoldie AZ. Domestic violence among pregnant mothers in Northwest Ethiopia: prevalence and associated factors. Adv Public Health. 2017;2017:1–6. doi:10.1155/2017/6506231
15. Al Kindi A, Al Shidhani N, Al Kiyumi M. Domestic violence among literate Omani women: prevalence, risk factors, and help-seeking behaviors. East Mediterr Health J. 2020.
16. Stöckl H, Devries K, Rotstein A, et al. The global prevalence of intimate partner homicide: a systematic review. Lancet. 2013;382(9895):859–865. doi:10.1016/S0140-6736(13)61030-2
17. Hawcroft C, Hughes R, Shaheen A, et al. Prevalence and health outcomes of domestic violence amongst clinical populations in Arab countries: a systematic review and meta-analysis. BMC Public Health. 2019;19(1):315. doi:10.1186/s12889-019-6619-2
18. Al-Azri M, Al-Lawati I, Al-Kamyani R, et al. Prevalence and risk factors of antenatal depression among Omani women in a primary care setting: cross-sectional study. Sultan Qaboos Univ Med J. 2016;16(1):e35. doi:10.18295/squmj.2016.16.01.007
19. Al Rawahi A, Al Kiyumi MH, Al Kimyani R, et al. The effect of antepartum depression on the outcomes of pregnancy and development of postpartum depression: a prospective cohort study of Omani women. Sultan Qaboos Univ Med J. 2020;20(2):e179. doi:10.18295/squmj.2020.20.02.008
20. El-Mohandes AA, Kiely M, Gantz MG, El-Khorazaty MN. Very preterm birth is reduced in women receiving an integrated behavioral intervention: a randomized controlled trial. Matern Child Health J. 2011;15(1):19–28. doi:10.1007/s10995-009-0557-z
21. Haddad LG, Shotar A, Younger JB, Alzyoud S, Bouhaidar CM. Screening for domestic violence in Jordan: validation of an Arabic version of a domestic violence against women questionnaire. Int J Womens Health. 2011;3:79. doi:10.2147/IJWH.S17135
22. Swahnberg IK, Wijma B. The NorVold Abuse Questionnaire (NorAQ) Validation of new measures of emotional, physical, and sexual abuse, and abuse in the health care system among women. Eur J Public Health. 2003;13(4):361–366. doi:10.1093/eurpub/13.4.361
23. Wijma B, Schei B, Swahnberg K, et al. Emotional, physical, and sexual abuse in patients visiting gynaecology clinics: a Nordic cross-sectional study. Lancet. 2003;361(9375):2107–2113. doi:10.1016/S0140-6736(03)13719-1
24. Dean AG, Sullivan KM, Soe MM OpenEpi: open source epidemiologic statistics for public health, version. 2013.
25. United Nations Development Programme (UNDP). Oman, gender justice & law; 2018. Available from: https://arabstates.unfpa.org/en/publications/gender-justice-law-oman.
26. Plecher H. Oman - fertility rate 2008–2018; 2020. Available from: https://www.statista.com/statistics/455499/fertility-rate-in-oman/#:~:text=In%202018%2C%20the%20fertility%20rate,to%202.89%20children%20per%20woman.
27. National Centre for Statistics & Information. Oman, Statistical Year Book. 2019.
28. Janssen PA, Holt VL, Sugg NK, Emanuel I, Critchlow CM, Henderson AD. Intimate partner violence and adverse pregnancy outcomes: a population-based study. Am J Obstet Gynecol. 2003;188(5):1341–1347. doi:10.1067/mob.2003.274
29. Taillieu TL, Brownridge DA. Violence against pregnant women: prevalence, patterns, risk factors, theories, and directions for future research. Aggress Violent Behav. 2010;15(1):14–35. doi:10.1016/j.avb.2009.07.013
30. Bağcıoğlu E, Vural M, Karababa İF, Akşin M, Selek S. Decrease in domestic violence during pregnancy: a study from Turkey. J Interpers Violence. 2014;29(2):203–216.
31. Alebel A, Kibret GD, Wagnew F, et al. Intimate partner violence and associated factors among pregnant women in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2018;15(1):1–2. doi:10.1186/s12978-018-0637-x
32. Pallitto CC, García-Moreno C, Jansen HA, Heise L, Ellsberg M, Watts C. Intimate partner violence, abortion, and unintended pregnancy: results from the WHO Multi-country Study on Women’s Health and Domestic Violence. Int J Gynaecol Obstet. 2013;120(1):3–9. doi:10.1016/j.ijgo.2012.07.003
33. Martin-de-Las-Heras S, Velasco C, de Dios Luna J, Martin A. Unintended pregnancy and intimate partner violence around pregnancy in a population-based study. Women Birth. 2015;28(2):101–105. doi:10.1016/j.wombi.2015.01.003
34. Kuhlmann AS, Shato T, Fu Q, Sierra M. Intimate partner violence, pregnancy intention and contraceptive use in Honduras. Contraception. 2019;100(2):137–141. doi:10.1016/j.contraception.2019.03.050
35. Wang T, Liu Y, Li Z, et al. Prevalence of intimate partner violence (IPV) during pregnancy in China: a systematic review and meta-analysis. PLoS One. 2017;12(10):e0175108. doi:10.1371/journal.pone.0175108
36. Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C. Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. Lancet. 2008;371(9619):1165–1172. doi:10.1016/S0140-6736(08)60522-X
37. Straight ES, Harper FW, Arias I. The impact of partner psychological abuse on health behaviors and health status in college women. J Interpers Violence. 2003;18(9):1035–1054. doi:10.1177/0886260503254512
38. Rodrigues T, Rocha L, Barros H. Physical abuse during pregnancy and preterm delivery. Am J Obstet Gynecol. 2008;198(2):171–e1. doi:10.1016/j.ajog.2007.05.015
39. Donovan BM, Spracklen CN, Schweizer ML, Ryckman KK, Saftlas AF. Intimate partner violence during pregnancy and the risk for adverse infant outcomes: a systematic review and meta‐analysis. BJOG. 2016;123(8):1289–1299. doi:10.1111/1471-0528.13928
40. Hill A, Pallitto C, McCleary-Sills J, Garcia-Moreno C. A systematic review and meta-analysis of intimate partner violence during pregnancy and selected birth outcomes. Int J Gynaecol Obstet. 2016;133(3):269–276. doi:10.1016/j.ijgo.2015.10.023
41. Abujilban S, Mrayan L, Al-Modallal H, Isaa EA. Effects of intimate partner physical violence on newborns’ birth outcomes among Jordanian birthing women. J Interpers Violence. 2017;32(24):3822–3838. doi:10.1177/0886260515603975
42. Berenson AB, Wiemann CM, Wilkinson GS, Jones WA, Anderson GD. Perinatal morbidity associated with violence experienced by pregnant women. Am J Obstet Gynecol. 1994;170(5):1760–1769. doi:10.1016/S0002-9378(12)91846-3
43. Grimstad H, Schei B, Backe B, Jacobsen G. Physical abuse and low birthweight: a case-control study. BJOG. 1997;104(11):1281–1287. doi:10.1111/j.1471-0528.1997.tb10975.x
44. Women UN. Violence Against Women: What is at Stake? Status of Arab Women Report 2017. Beirut: United Nations Economic and Social Commission for Western Asia; 2017.
45. Cann K, Withnell S, Shakespeare J, Doll H, Thomas J. Domestic violence: a comparative survey of levels of detection, knowledge, and attitudes in healthcare workers. Public Health. 2001;115(2):89–95.
46. Procentese F, Di Napoli I, Tuccillo F, Chiurazzi A, Arcidiacono C. Healthcare professionals’ perceptions and concerns towards domestic violence during pregnancy in Southern Italy. Int J Environ Res Public Health. 2019;16(17):3087. doi:10.3390/ijerph16173087
47. Zaher E, Keogh K, Ratnapalan S. Effect of domestic violence training: systematic review of randomized controlled trials. Can Fam Physician. 2014;60(7):618–624.
48. Bennett L, Riger S, Schewe P, Howard A, Wasco S. Effectiveness of hotline, advocacy, counseling, and shelter services for victims of domestic violence: a statewide evaluation. J Interpers Violence. 2004;19(7):815–829. doi:10.1177/0886260504265687
49. Van Parys AS, Verhamme A, Temmerman M, Verstraelen H, Vermund SH. Intimate partner violence and pregnancy: a systematic review of interventions. PLoS One. 2014;9(1):e85084. doi:10.1371/journal.pone.0085084
50. Di Napoli I, Procentese F, Carnevale S, Esposito C, Arcidiacono C. Ending intimate partner violence (IPV) and locating men at stake: an ecological approach. Int J Environ Res Public Health. 2019;16(9):1652. doi:10.3390/ijerph16091652
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.