Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence, Pathogenic Bacterial Profile and Antimicrobial Susceptibility Pattern of Urinary Tract Infection Among Children with Congenital Anomalies of the Kidney and Urinary Tract
Authors Zhang K ![]() , Zhang Y
, Zhang Y ![]() , Chao M, Hao Z
, Chao M, Hao Z
Received 31 January 2023
Accepted for publication 15 April 2023
Published 26 June 2023 Volume 2023:16 Pages 4101—4112
DOI https://doi.org/10.2147/IDR.S399442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kaiping Zhang,1,2 Yin Zhang,2 Min Chao,2 Zongyao Hao1
1Department of Urology, The First Affiliated Hospital of Anhui Medical University; Institute of Urology, Anhui Medical University; Anhui Province Key Laboratory of Genitourinary Diseases, Anhui Medical University, Hefei, Anhui Province, 230000, People’s Republic of China; 2Department of Urology, Anhui Provincial Children’s Hospital/Children’s Hospital of Fudan University (Affiliated Anhui Branch), Hefei, Anhui Province, 230000, People’s Republic of China
Correspondence: Zongyao Hao, Department of Urology, The First Affiliated Hospital of Anhui Medical University; Institute of Urology, Anhui Medical University, Anhui Province Key Laboratory of Genitourinary Diseases, Anhui Medical University, Jixi Road, Hefei, Anhui Province, 230000, People’s Republic of China, Email [email protected]
Purpose: The study was to detect the pathogenic bacterial profile and antibiogram among children with congenital anomalies of the kidney and urinary tract (CAKUT).
Patients and Methods: A retrospective analysis was performed using medical records of urine culture results and antibiotic susceptibility results in patients with UTIs from March 2017 to March 2022. Antimicrobial susceptibility pattern was determined by a standard agar disc diffusion method.
Results: A total of 568 children were included. The proportion of culture-positive UTI was 59.15% (336/568). More than nine types of bacteria were isolated with most pathogens being Gram-negative species. Among Gram-negative isolates, the predominant bacteria were Escherichia coli (30.95%, 104/336) followed by Klebsiella pneumoniae (9.23%). Escherichia coli isolates were highly sensitive to amikacin (95.19%), ertapenem (94.23%), nitrofurantoin (93.27%), imipenem (91.35%), and piperacillin-tazobactam (90.38%) and high rate of resistant were also detected to ampicillin (92.31%), cephazolin (73.08%), ceftriaxone (70.19%), trimethoprim-sulfamethoxazole (61.54%) and ampicillin-sulbactam (57.69%). Klebsiella pneumoniae isolates showed sensitive to ertapenem (96.77%), amikacin (96.77%), imipenem (93.55%), piperacillin-tazobactam (90.32%) and gentamicin (83.87%), while highly resistant were observed to ampicillin (96.77%), cephazolin (74.19%), ceftazidime (61.29%), ceftriaxone (61.29%), and aztreonam (61.29%). The isolated Gram-positive bacteria mainly contained Enterococcus faecalis and Enterococcus faecium (each 15.77%). Enterococcus faecalis were sensitive to vancomycin, penicillin-G, tigecycline, nitrofurantoin and linezolid (100%, 94.34%, 88.68%, 88.68%, 86.79, respectively) and resistant to tetracycline (86.79%), quinupristi (83.02%), erythromycin (73.58%). Enterococcus faecium also showed a similar result. Multiple drug resistance (MDR) was observed in 264 (80.00%) of the 360 bacterial isolates. Only age was significantly associated with a culture-positive UTI.
Conclusion: A higher prevalence of culture-positive UTI was detected. Escherichia coli was the most prevalent uropathogen followed by Enterococcus faecalis and Enterococcus faecium. These uropathogens showed highly resistant to the commonly used antibiotics. Moreover, MDR was commonly observed. Thus, empiric therapy is unsatisfactory as drug sensitivity always varies over time.
Keywords: urinary tract infection, congenital anomalies of the kidney and urinary tract, multi-drug resistance, prevalence, antimicrobial susceptibility
Introduction
Urinary tract infection (UTI) is an infection caused by the spread and growth of uropathogens, as a result of the ascent of bacteria from the urethra and hematogenous spread of bacteria. The short-term symptoms include fever, urinary frequency, dysuria with or without frequency, urgency, hematuria and suprapubic pain.1 If not treated properly, it often develops health problem worldwide including recurrent UTI, renal scarring, even damage of renal function, particularly in infants less than 2 months of age.2,3 Approximately 8.4% of girls and 1.7% of boys by the age of 7 years will experience UTI, and 30% of infants and children experience recurrent infections during the first six to 12 months after initial UTI.4–6 Compared to adults, children seem to be more susceptible to UTI mainly due to an indwelling catheter, ureteral stent usage in surgery, CAKUT, or compromised immune system.7
Anatomical or functional abnormalities of kidney and urinary tract often develop UTIs easily. It has been reported that these abnormalities were explored in 30% of newborns at the first UTI episode, even in 47% of febrile newborns.8,9 Thus, UTI may be taken as a clinical presentation of CAKUT under some circumstances. The most common anomalies were vesicoureteric reflux (VUR), duplicated collecting system, posterior urethral valves (PUV), neurogenic bladder (NB), ureteral obstruction and ureteropelvic junction obstruction (UPJO). Those UTIs with CAKUT are considered to be complicated UTIs. The purposes of UTI in childhood often consist of eradication of the bacterial pathogen, identification of CAKUT, and avoidance of recurrent infections.10 Prompt diagnosis and appropriate treatment are very important for children to reduce the morbidity.
The detection of the uropathogen contributes to antibacterial treatment of UTI. But in practice, symptomatic UTI usually requires inpatient therapy with rapid administration of empirical antibiotic before urine culture testing. Meanwhile, the higher occurrence of UTI in children with CAKUT could increase the antibacterial treatment. Conversely, the inappropriate treatment could increase the incidence of antibiotic resistance (ABR).11 ABR is a increasingly serious problem, especially in pediatric UTI.12 Therefore, there is a need to identify which bacterial strains and explore their drug susceptibility in children. It could guide effective antibacterial therapy, and even reduce the multi-drug resistance prevalence. This study was aimed at detecting urinary pathogenic bacterial profile, drug susceptibility and associated factors of culture-positive UTI among children with CAKUT.
Materials and Methods
Study Design
A retrospective study was performed in our department during the 5 years, from March 2017 to March 2022. Among hospitalized children with CAKUT, those children diagnosed with UTI were included in the current study. UTI were diagnosed based on the finding of more than 105 CFU/mL bacteria in urine. The information including age, sex of patients, the microorganism isolated, and the antimicrobial susceptibility profiles was collected who had been diagnosed with CAKUT, such as VUR, duplicated collecting system, PUV, NB, ureteral obstruction and UPJO. For imaging tests, ultrasonography, voiding cystourethrography (VCUG), intravenous pyelography (IVP), computed tomography (CT), magnetic resonance urography (MRU), and dimercaptosuccinic acid (DMSA) were performed.
Culture and Identification
A midstream urine sample was tested. The urine specimen was inoculated on Cysteine-Lactose-Electrolyte-Deficient (CLED) agar using a sterile loop (0.001 mL). Then colonies were subcultured into MacConkey agar and blood agar plates (BAP) (Oxoid, UK). After overnight incubation at 37°C for 24–48 hours, colonies were counted. The identification of bacteria was done using gram staining, colony characteristics, and biochemical test following standard procedure.13
Antimicrobial Susceptibility Testing
According to the criteria of National Committee for Clinical Laboratory Standards (NCCLs), susceptibility testing was performed. The drugs included ampicillin (AMP), ampicillin-sulbactam (SAM), ciprofloxacin (CP), levofloxacin (LEV), nitrofurantoin (FM), piperacillin-tazobactam (TZP); cephazolin (CZO), cefotetan (CTT), ceftazidime (CAZ), ceftriaxone (CRO), imipenem (IMP), amikacin (AN), tobramycin (TOB), trimethoprim-sulfamethoxazole (TMP-STX), cefoxitin (CXT); imipenem (IPM), cefotaxime (CTX), aztreonam, ertapenem, gentamicin, cefepime, quinupristin, tigecycline, penicillin-G (PG), gentamycin (GM), erythromycin (E), linezolid (LZD), vancomycin (VA), tetracycline (TC), nitrofurantoin (FM). A standard agar disc diffusion method was used to determine antimicrobial susceptibility. Antibiotic resistance rate under 20% was set as the green zone, 20–30% as the yellow zone, and the ratio over 30% as the red zone. The definition of MDR is resistance for three or more antibiotics.
Statistical Analysis
In this study, data was performed by SPSS statistical software package (version 16) (IBM Corp., Armonk, NY, USA). The proportion of children was expressed as a percentage of all children. Isolated and identified pathogens were each quantified as percentage of total isolated organisms. The susceptibility patterns and MDR to commonly prescribed antibiotics were noted as frequencies and percentages. In addition, the independent risk factor for culture positive UTI was tested by univariable logistic regression analyses. P-value less than 0.05 was considered as statistically significant.
Results
In total, we collected urine samples from 568 pediatric patients with CAKUT, indicating that the male to female ratio was 2.44:1. The age ranges from 1 month to 14 years. The abnormalities included VUR, PUV, NB, ureteral obstruction, UPJO and so on. All pediatric UTI in our study was community-acquired infection. The general characteristics of pediatric UTI patients are shown in Table 1.
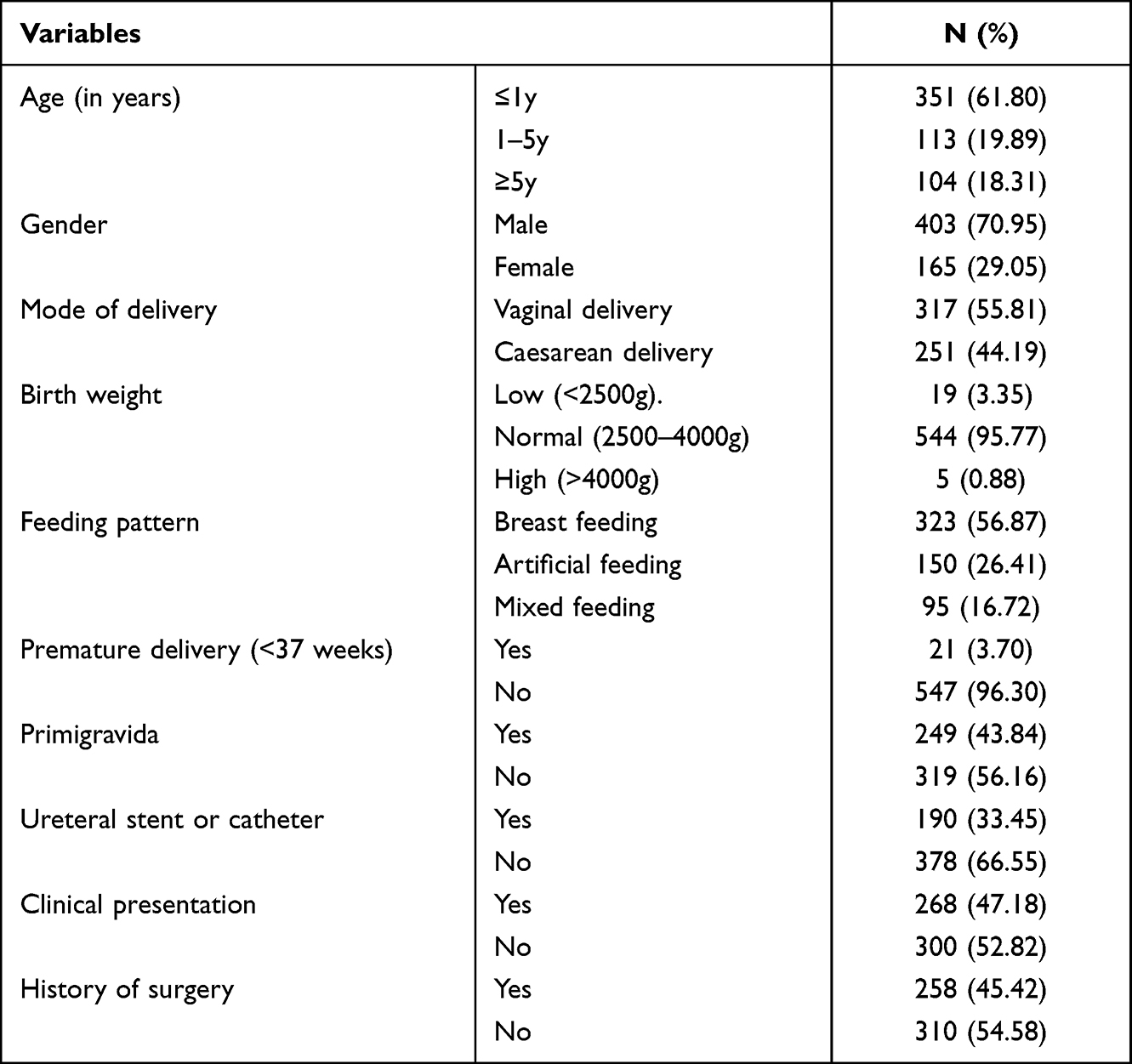 |
Table 1 Clinical Characteristics of Study Participants by Diagnosis of UTI |
Of 568 cases, there were 268 symptomatic UTI and 300 asymptomatic UTI, respectively. The overall prevalence of culture-positive UTI were 50.14% (336/568). More than nine types of bacteria were isolated in this study with majority of the isolates being Gram-negative bacteria. Among the isolates the predominant bacteria were Escherichia coli (30.95%, 104/336), followed by Klebsiella pneumoniae (9.23%) and Pseudomonas aeruginosa (4.17%). The isolated Gram-positive bacteria contained Enterococcus faecalis and Enterococcus faecium (each 15.77%). Bacterial profile isolated from urine culture of children with different CAKUT was presented in Table 2.
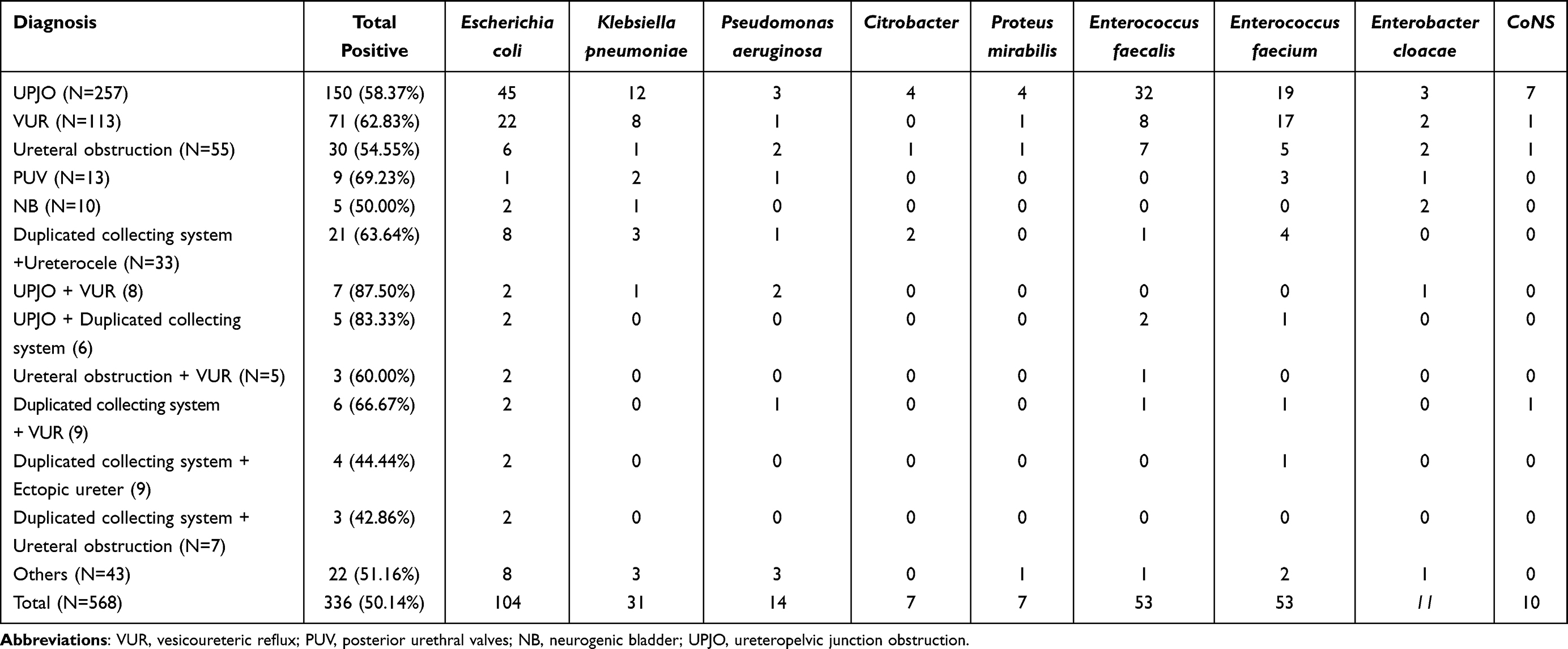 |
Table 2 Bacterial Profile Isolated from Urine Culture of Children with Different CAKUT |
In addition, we detected that more CAKUT phenotypes have the higher prevalence rate of culture-positive UTI. As shown in Table 3, the proportion of culture-positive UTI was 57.96%, 62.96%, 76.00% in different phenotypes, respectively. The isolated uropathogens mainly included Escherichia coli, Enterococcus faecalis and Enterococcus faecium in different CAKUT phenotypes.
 |
Table 3 Bacterial Profile Isolated from Urine Culture of Children with Different CAKUT Phenotypes |
The antimicrobial susceptibility pattern of each bacterial isolate are shown in Table 4 and Table 5. Of isolated Gram-negative uropathogens, Escherichia coli isolates were highly sensitive to AN (95.19%), Ertapenem (94.23%), FM (93.27%), IMP (91.35%), TZP (90.38%) and CTT (87.50%) and high rate of resistant were also detected to AMP (92.31%), CZO (73.08%), CRO (70.19%), TMP-STX (61.54%) and SAM (57.69%). In addition, Klebsiella pneumoniae isolates showed sensitive to Ertapenem (96.77%), AN (96.77%), IMP (93.55%), TZP (90.32%), Gentamicin (83.87%), TOB (83.87%), while highly resistant were observed to Amp (96.77%), CZO (74.19%), CAZ (61.29%), CRO (61.29%), and aztreonam (61.29%). With regard to Pseudomonas aeruginosa, they were sensitive to CP, LEV, TZP, AN, gentamicin and TOB (each 100%) but resident to SAM, AMP, CZO and IMP (92.86%, 85.71%, 85.71%, 78.57%). The antimicrobial susceptibility patterns of other specific isolated Gram negative bacilli are found in Table 4. As for Gram-positive bacilli, we found that Enterococcus faecalis were sensitive to VA, PG, Tigecycline, FM and LZD (100%, 94.34%, 88.68%,88.68%, 86.79, respectively) and resident to TC (86.79%), quinupristi (83.02%), E (73.58%). Likewise, Enterococcus faecium were sensitive to VA, LZD, tigecycline, quinupristin (98.11%, 96.23%, 90.57%, 79.25%), while resident to AMP (92.45%), E (90.57%), PG (86.79%), CP (71.70%), TC (66.04%) and LEV (60.38%) (Table 5).
 |
Table 4 Antimicrobial Susceptibility Patterns of Gram-Negative Bacteria Isolated from Urine Samples |
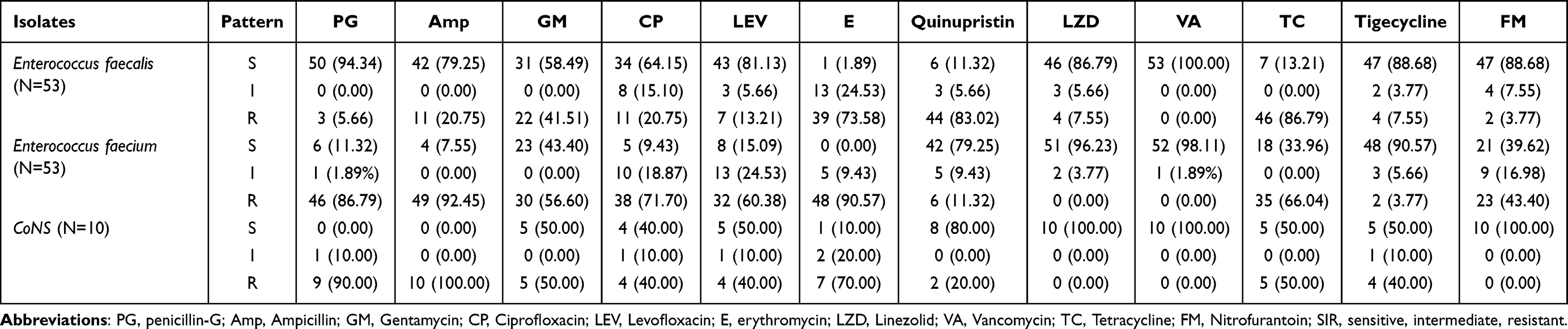 |
Table 5 Antimicrobial Susceptibility Patterns of Gram-Positive Bacteria Isolated from Urine Samples |
Among all the isolates, there were 6 fungal infections and 360 bacterial infections. Multiple drug resistance (MDR) was found in 264 of 360 bacteria isolated. Of Gram-negative uropathogens, Escherichia coli MDR were detected in 91/104. The MDR rates of Klebsiella pneumoniae, Pseudomonas aeruginosa were 67.74% and 21.43%, respectively. In terms of Gram-positive uropathogens, 81.13% of Enterococcus faecalis and 98.11% of Enterococcus faecium were also found. The detailed distribution is shown in Table 6. Univariable logistic regression analysis showed a significant association between prevalence of a culture positive UTI and age (Table 7). All the other factors were not statistically significant.
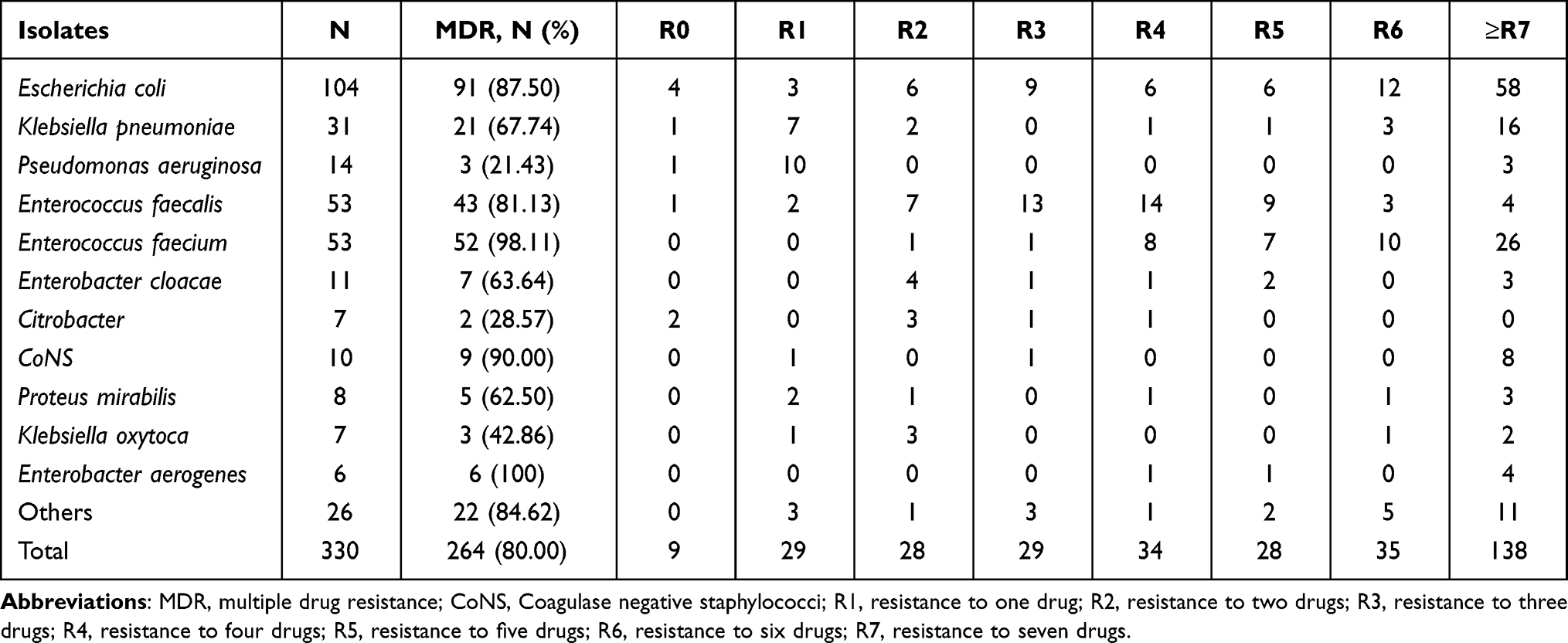 |
Table 6 Multi Drug Resistance Pattern of Bacterial Isolates from Children with UTI Accompanied by CAKUT |
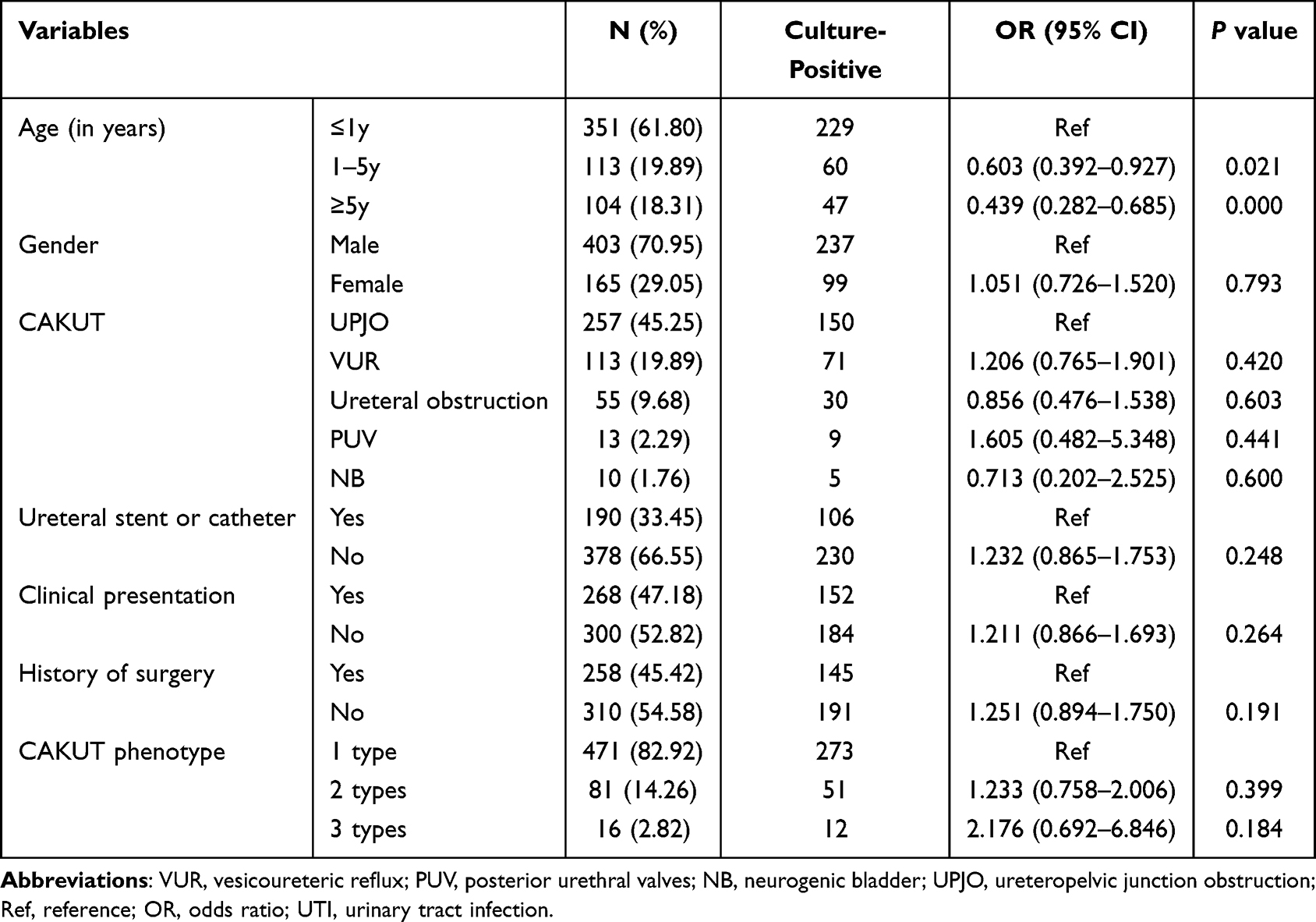 |
Table 7 Univariablee Logistic Regression Analyses for Factors Associated with UTI Among Children with CAKUT |
Discussion
UTI is a common infection in child. It has been reported that its incidence is nearly 0.7% in girls and 2.7% in boys by the age of 1 year. Up to 5% in girls and 20% in boys were diagnosed with UTI among febrile infants within the first two months of life.14,15 Anatomically, the shorter urethra in girls makes it easier for infection as well as proximity of the urethral opening to the anus.16 UTI occur more frequently in premature infant than term infant during neonatal period.17 The recurrence of UTI often occur in 30% children within 6 months for an acute UTI episode, and even up to 50% of school-age girls, which poses a major health problem of children.1,18 The higher prevalence and fear of its recurrence often results in the irrational use of antibiotics, especially for children with a history of recurrent or complicated UTI. Meanwhile, empirical treatment is also prevalent in primary hospital. The continued and irrational use of antibiotics has led to microbiota dysbiosis and antibiotic resistance, even caused other diseases.19
The CAKUT in neonates or young infants often develop UTI easily. Obstructive uropathy allows for the prolongation of bacteriuria due to poor drainage, decreasing the clearance of invading pathogens. Boys with PUV have increased risks of UTI voiding dysfunction, elevating bladder pressure stemming and ongoing renal damage. The continued bladder pressure from urine stasis or obstruction can cause VUR and increase the potential risk of renal function damage by an ascending infection.20 Approximately 20% of neonatal cases with VUR were diagnosed with UTI, and led to renal scars.21,22 In addition, children with neurogenic bladder increased the risk of UTI. These children often perform clean intermittent catheterisations, which can further increase the UTI risk caused by catheter contamination and the introduction of external pathogens into the bladder.23,24 It is important to identify CAKUT early because they may serve as a reservoir for bacterial growth or recurrent infections. Thereby further examinations are necessary for children to identify whether there are anatomical or functional abnormalities of kidney and urinary tract after the diagnosis of UTI.
The urinary tract is a sterile environment and resistant to bacterial colonisation. UTI is mostly caused by Gram-negative bacterium because of its unique structure of bacterial attachment to uro-epithelial cell surface.25 These bacteria resist the attack of host defenses, namely urinary lavage and bladder voiding that decrease the bacterial counts in the lumen. E. coli is the most predominant bacterium isolated from urine, accounting for 85–90% of all cases.26 It often originates from the faecal flora, spreads across the perineum, and then invades the bladder through the opening of urethra. Other common Gram-negative pathogens include Klebsiella pneumoniae, Proteus mirabilis, Enterobacter, Citrobacter, and P. aeruginosa. Among Gram-positive bacteria pathogens, Streptococcus species and Staphylococcus species are frequently isolated. In the present study, we also found that Gram-negative bacterial isolate were more prevalent than Gram-positive bacterial isolates. Escherichia coli was the most predominant identified Gram-negative uropathogen followed by Klebsiella pneumoniae. There were Enterococcus faecalis and Enterococcus faecium in Gram-positive pathogens. Knowing the prevalence of drug-resistant bacterium could help the clinicians to make the best choice of antibiotics among children.
Of isolated Gram-negative uropathogens, we found that Escherichia coli isolates were highly sensitive to AN (95.19%), Ertapenem (94.23%), FM (93.27%), IMP (91.35%) and TZP (90.38%) and high rate of resistant were presented to AMP, CZO, CRO, TMP-STX and SAM (95–55%). In addition, Klebsiella pneumoniae isolates showed sensitive to Ertapenem (96.77%), AN (96.77%), IMP (93.55%), TZP (90.32%), Gentamicin (83.87%), TOB (83.87%), while they were highly resistant to Amp (96.77%), CZO (74.19%), CAZ (61.29%), CRO (61.29%), and aztreonam (61.29%). With regard to Pseudomonas aeruginosa, they were sensitive to CP, LEV, TZP, AN, Gentamicin and TOB (each 100%) but resident to SAM, AMP, CZO and IMP (93–75%). As for Gram-positive bacilli, the sensitivity of Enterococcus faecalis to VA, PG, Tigecycline, FM and LZD was 100–80% and residence to TC (86.79%), Quinupristi (83.02%), E (73.58%). Likewise, we also detected that Enterococcus faecium were sensitive to VA, LZD, Tigecycline, Quinupristin (99–80%) and resident to AMP, E, PG, CP, TC and LEV (93–60%). This implies that ampicillin cannot be used as empirical therapy for pediatric UTI with urinary abnormalities.
Due to increasing antimicrobial resistance pattern and empirical therapy leading to treatment failure, antimicrobial treatment has gradually become more complicated. The emergence and spread of AMR among uropathogens is increasing, especially in regions with limited resources. The overall prevalence of MDR was 80% in our study, especially in Enterococcus faecium (90%) and Escherichia coli (87.50%).
Study Limitations
There are some limitations regarding our findings in this study. Firstly, this study was carried out with the patients from a single center, which could not be representative of the overall values of antibiotic sensitivity and resistance rate. Secondly, our study was a retrospective study. Thirdly, some asymptomatic UTIs could be managed with outpatient antibiotics and carry a universal good progress, which led to some loss of data. Therefore, it is urgently needed to conduct nationwide and multicenter studies on the antibiotic susceptibility and resistance in future.
Conclusions
As a result, our study revealed a higher prevalence of culture-positive UTI among children with CAKUT. Escherichia coli was the most predominant isolate followed by Enterococcus faecalis and Enterococcus faecium. Age was significantly associated with culture positive UTI. Majority of the isolates were resistant to the commonly prescribed antibiotics, therefore culture and antibiotic susceptibility testing was recommended before giving treatment to prevent antimicrobial resistance at least. Further large-scale studies are warranted to examine the generalizability of our findings.
Abbreviations
UTI, urinary tract infection; CAKUT, congenital anomalies of the kidney and urinary tract; VUR, vesicoureteric reflux; PUV, posterior urethral valves; NB, neurogenic bladder; UPJO, ureteropelvic junction obstruction; Amp, Ampicillin; SAM, Ampicillin and Sulbactam; CP, Ciprofloxacin; LEV, Levofloxacin; FM, Nitrofurantoin; TZP, Piperacillin and Tazobactam; CZO, Cephazolin; CTT, Cefotetan; CAZ, Ceftazidime; CRO, Ceftriaxone; IMP, Imipenem; AN, Amikacin; TOB, Tobramycin; TMP-STX, Trimethoprim-sulfamethoxazole; CXT, Cefoxitin; IPM, Imipenem; CTX, Cefotaxime; CoNS, Coagulase negative staphylococcus; PG, penicillin-G; Amp, Ampicillin; GM, Gentamycin; CP, Ciprofloxacin; LEV, Levofloxacin; E, erythromycin; LZD, Linezolid; VA, Vancomycin; TC, Tetracycline; FM, Nitrofurantoin; MDR, resistance for three or more antibiotics; OR, odds ratio.
Ethics Approval
The study was approved by the Ethics Committee of Anhui Provincial Children’s Hospital/Children’s Hospital of Fudan University (Affiliated Anhui Branch), Hefei, China (No. 2022122101). The ethics committee waived the need for written informed consent provided by participants due to the retrospective nature of this study. Children’ anonymous information was provided from the microbiology hospital laboratory, which isolated the strains. The study completely followed the principles outlined in the Declaration of Helsinki.
Acknowledgment
We are grateful to all the authors for their contributions to this study.
Funding
This work was supported by the Natural Science Foundation of Anhui Province (1908085MH246) and the Natural Science Foundation of China (82070724).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stephens GM, Akers S, Nguyen H, Woxland H. Evaluation and management of urinary tract infections in the school-aged child. Prim Care. 2015;42(1):33–41. doi:10.1016/j.pop.2014.09.007
2. Larcombe J. Urinary tract infection in children. Am Fam Physician. 2010;82(10):1252–1256.
3. Mangiarotti P, Pizzini C, Fanos V. Antibiotic prophylaxis in children with relapsing urinary tract infections: review. J Chemother. 2000;12(2):115–123. doi:10.1179/joc.2000.12.2.115
4. Nuutinen M, Uhari M. Recurrence and follow-up after urinary tract infection under the age of 1 year. Pediatr Nephrol. 2001;16(1):69–72. doi:10.1007/s004670000493
5. Tullus K, Shaikh N. Urinary tract infections in children. Lancet. 2020;395(10237):1659–1668. doi:10.1016/S0140-6736(20)30676-0
6. Hellström A, Hanson E, Hansson S, Hjälmås K, Jodal U. Association between urinary symptoms at 7 years old and previous urinary tract infection. Arch Dis Child. 1991;66(2):232–234. doi:10.1136/adc.66.2.232
7. Desai DJ, Gilbert B, McBride CA. Paediatric urinary tract infections: diagnosis and treatment. Aust Fam Physician. 2016;45(8):558–563.
8. Sastre JB, Aparicio AR, Cotallo GD, Colomer BF, Hernandez MC; Grupo de Hospitales Castrillo. Urinary tract infection in the newborn: clinical and radio imaging studies. Pediatr Nephrol. 2007;22(10):1735–1741. doi:10.1007/s00467-007-0556-5
9. Bonadio W, Maida G. Urinary tract infection in outpatient febrile infants younger than 30 days of age: a 10-year evaluation. Pediatr Infect Dis J. 2014;33(4):342–344. doi:10.1097/INF.0000000000000110
10. Banno Y, Sugiyama T. Predicting factors of clinically significant urological anomalies after initial urinary tract infection among 2- to 24-month-old children. Acta Paediatr. 2022;111(6):1274–1281. doi:10.1111/apa.16341
11. Albaramki JH, Abdelghani T, Dalaeen A, et al. Urinary tract infection caused by extended-spectrum β-lactamase-producing bacteria: risk factors and antibiotic resistance. Pediatr Int. 2019;61(11):1127–1132. doi:10.1111/ped.13911
12. Voicu MN, Ahmet AM, Turcu-Stiolica M, Turcu-Stiolica A, Barbulescu AL, Popescu F. Antibiotic resistance, still a global challenge. Curr Health Sci J. 2021;47(2):284–289. doi:10.12865/CHSJ.47.02.20
13. Cheesbrough M. Biochemical tests to identify bacteria. In: District Laboratory Practice in Tropical Countries, Part 2. Cambridge, UK: Cambridge University Press; 2000:63–70.
14. Chang SL, Shortliffe LD. Pediatric urinary tract infections. Pediatr Clin North Am. 2006;53(3):379–400. doi:10.1016/j.pcl.2006.02.011
15. Simões e Silva AC, Oliveira EA. Update on the approach of urinary tract infection in childhood. J Pediatr. 2015;91(6 Suppl 1):S2–S10. doi:10.1016/j.jped.2015.05.003
16. McGuire L. A seat on the aisle, please! The essential guide to urinary tract problems in women. Mayo Clin Proc. 2007;82(1):130. doi:10.1016/S0025-6196(11)60976-2
17. Schlager TA. Urinary tract infections in infants and children. Microbiol Spectr. 2016;4(5):10. doi:10.1128/microbiolspec.UTI-0022-2016
18. Korbel L, Howell M, Spencer JD. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr Int Child Health. 2017;37(4):273–279. doi:10.1080/20469047.2017.1382046
19. Konstantinidis T, Tsigalou C, Karvelas A, Stavropoulou E, Voidarou C, Bezirtzoglou E. Effects of antibiotics upon the gut microbiome: a review of the literature. Biomedicines. 2020;8(11):502. doi:10.3390/biomedicines8110502
20. Chase J, Austin P, Hoebeke P, McKenna P; International Children’s Continence Society. The management of dysfunctional voiding in children: a report from the Standardisation Committee of the International Children’s Continence Society. J Urol. 2010;183(4):1296–1302. doi:10.1016/j.juro.2009.12.059
21. Cleper R, Krause I, Eisenstein B, Davidovits M. Prevalence of vesicoureteral reflux in neonatal urinary tract infection. Clin Pediatr. 2004;43(7):619–625. doi:10.1177/000992280404300706
22. Olbing H, Smellie JM, Jodal U, Lax H. New renal scars in children with severe VUR: a 10-year study of randomized treatment. Pediatr Nephrol. 2003;18(11):1128–1131. doi:10.1007/s00467-003-1256-4
23. Dinh A, Davido B, Duran C, et al. Urinary tract infections in patients with neurogenic bladder. Med Mal Infect. 2019;49(7):495–504. doi:10.1016/j.medmal.2019.02.006
24. Pavlović K, Hrkać A, Kožul IS, Zalihić D, Zalihić A, Gilja I. Long-term results of augmentation ileocystoplasty in spinal cord injury patients. Cent European. J Urol. 2021;74(2):178–184.
25. Amiri FN, Rooshan MH, Ahmady MH, Soliamani MJ. Hygiene practices and sexual activity associated with urinary tract infection in pregnant women. East Mediterr Health J. 2009;15(1):104–110. doi:10.26719/2009.15.1.104
26. Kahlmeter G. Prevalence and antimicrobial susceptibility of pathogens in uncomplicated cystitis in Europe. The ECOaSENS study. Int J Antimicrob Agents. 2003;22(Suppl 2):49–52. doi:10.1016/S0924-8579(03)00229-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.