Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Prevalence of Recurrent Aphthous Ulcers Among Dentistry Students’ in Kabul, Afghanistan: A Questionnaire-Based Study
Authors Taheri MH ![]() , Eshraqi AM, Anwari A
, Eshraqi AM, Anwari A ![]() , Stanikzai AM
, Stanikzai AM
Received 25 June 2022
Accepted for publication 6 September 2022
Published 14 September 2022 Volume 2022:14 Pages 275—279
DOI https://doi.org/10.2147/CCIDE.S378171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mohammad Haris Taheri, Ali Maisam Eshraqi, Abdurrahman Anwari, Ahmad Milad Stanikzai
Faculty of Dentistry, Kabul University of Medical Sciences, Kabul, Afghanistan
Correspondence: Mohammad Haris Taheri, Jamal Mena, Ali Abad Teaching Hospital, Dentistry Teaching Clinic, Kabul, 3rd District, Kabul, Afghanistan, Tel +93786234342, Email [email protected]
Introduction: Recurrent aphthous stomatitis (RAS) is the mouth’s most common and painful inflammatory ulcerative condition, also called aphthae or canker sores. Its prevalence is about 20% and predisposition factors involve genetics, environmental factors, and immune dysfunctions.
Objective: Reviewing the literature and no study was found to show the prevalence and associated factors of recurrent aphthous ulceration in the context of Afghanistan. Therefore, this study aimed to determine the lifetime prevalence and associated factors of recurrent aphthous ulceration among dentistry students at Kabul University of Medical Sciences, Afghanistan.
Methods: A cross-sectional questionnaire-based study was carried out among 223 dentistry students. A descriptive and inferential analysis was performed to find the association.
Results: The prevalence of (RAS) in our sample group was 30%. (68.7%) of participants had one or more family members who experienced aphthous ulcers and the association was found to be significant (X2 = 134.940; p < 0, 05). (81%) of participants experienced the condition to eating certain types of food (X2 = 165.906; p < 0, 05) and (53.7%) of them reported the same about trauma (X2 = 99.958; p < 0, 05). Regarding stress the difference was also statistically significant (X2 = 56.830; p < 0, 05).
Conclusion: We found that a considerable proportion of the study sample had experienced recurrent aphthous ulceration. Family history, stress, trauma, and dietary factors have an impact on the occurrence of RAS with no association with gender and smoking.
Keywords: recurrent aphthous ulceration, prevalence, associated factors, Afghanistan
Introduction
Recurrent aphthous ulceration is an inflammatory ulcerative condition of the oral mucosa, a shallow round ulcer with an erythematous halo covered by a yellowish-gray slough.1 It mainly occurs in the non-keratinized areas such as lips, tongue, buccal mucosa, and soft palate.2 Aphthous ulcers are classified into three groups based on their size; major, minor, and herpetiform. Minor aphthous ulceration is small (less than one cm in diameter), well-defined, shallow, and heals within two weeks without a scar. Major ulcers are bigger, and deeper and take up to six weeks to heal with scars. Herpetiform ulcers are also small (3–6mm), shallow, multiple ulcers and take weeks to heal.3 Aphthous ulceration is usually painful and interferes with eating, speaking, and swallowing.4 Oral ulcers have a negative impact on individuals’ oral health, routines, and daily lives; hence, it has the potential to increase morbidity and decrease the quality of life significantly.5
The etiology of recurrent aphthous ulcers is unclear; however, many factors are associated with stress, trauma, infection, allergy, genetic predisposition, or nutritional deficiencies.6,7 Nevertheless, it is reported as the most common oral mucosal disorder worldwide.1 The prevalence of recurrent aphthous ulceration was reported to vary from 5 to 66% in different countries.8,9 In the United States of America (USA), Shulman’s study revealed the prevalence of recurrent aphthous ulcers to be 40% in a sample of children.10 It frequently occurs among women more than men11 and increases with increasing age. Besides, minor aphthous ulcers are responsible for more than 80% of cases.12
However, to tackle the problem, it is essential to know the prevalence and risk factors of recurrent aphthous in Afghanistan. We reviewed the literature and found no study to show the prevalence of recurrent aphthous ulceration in the context of Afghanistan. Therefore, we design this study, given the limited resources, to determine the prevalence of recurrent aphthous ulceration in a sample of dentistry students at Kabul University of Medical Sciences, Kabul, Afghanistan.
Method
A descriptive cross-sectional study was carried out among a consensus sample of 223 dentistry students at Kabul University of Medical Sciences, Kabul, Afghanistan. The participants of the present study were dental students who have passed the courses regarding recurrent aphthous. The study was approved by the ethics committee of Kabul University of Medical Sciences and the signed consent of all participants was obtained before handing over the questionnaire. We confirm that this study complies with the declaration of Helsinki.
A questionnaire was developed by researchers after an extensive literature review. The questionnaire contains 2 sections. The first section contains questions on the demographic characteristics of the participants such as age, gender, and class. The second section contains questions divided into 5 parts with a total of 23 questions related to the occurrence history of recurrent aphthous ulceration, family history, diet, stress, and trauma.
Statistical Analysis
The data were analyzed by using SPSS version 16.0. The frequency distribution of recurrent aphthous ulceration was calculated. A frequency table was utilized to determine the lifetime prevalence of recurrent aphthous ulcers and a chi-square test was applied to find the association of factors with recurrent aphthous ulceration. The level of significance was fixed at p < 0.05 for all comparisons.
Result
Totally, 223 students participated in the study. About half of the respondents were female (50.2%) and male (49.8%). Their age ranged from 22–28 years. Among 223 respondents, 117 (52.46%) were in the fifth grade and 106 (47.54%) were last year’s students of dentistry faculty (Table 1).
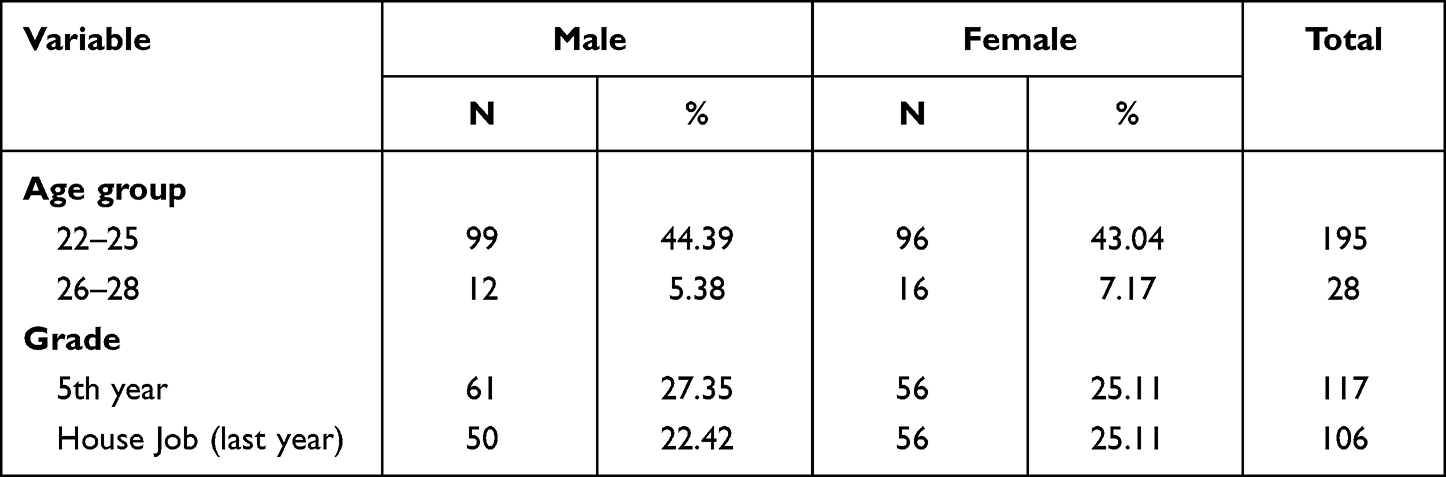 |
Table 1 Characteristics of the Study Population |
Nearly, all of the respondents (99.6%) were non-smokers. The lifetime prevalence of recurrent aphthous was found to be 30% (n=67) and nearly, two-thirds of them (n = 46; 68.7%) have one or more family members who experienced oral aphthous ulcers. Most of the respondents (n = 54; 81%) who have experienced the situation claimed that eating certain types of food was the cause of the ulcer. Besides, the majority of the experienced group (n = 36; 53.7%) reported trauma as a triggering factor for the occurrence of their oral ulcers while two-thirds of them (n = 22; 32.8%) mentioned that stress was the reason for their ulcers. The frequency distribution of all related risk factors in participants with RAS is shown below in Table 2.
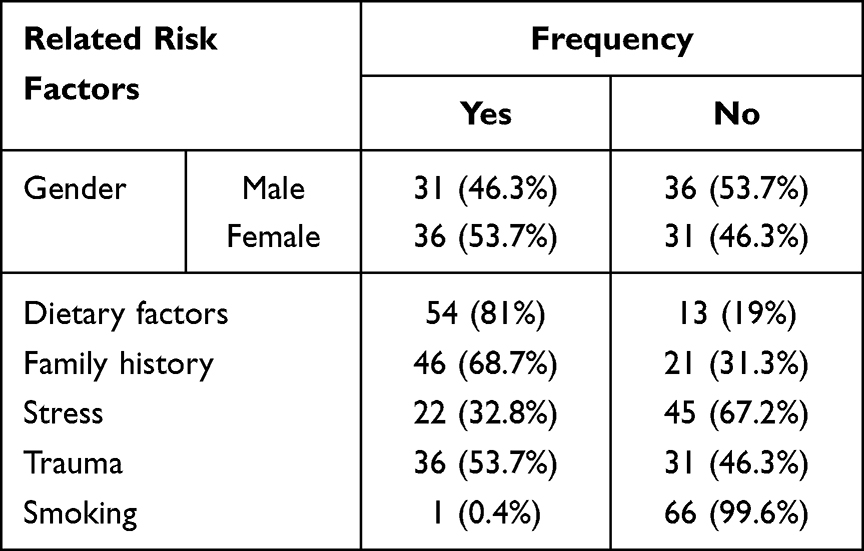 |
Table 2 The Frequency Distribution of All Possible Related Risk Factors in Participants |
The result of the chi-square test showed that gender and smoking did not have a significant association with recurrent aphthous ulcers (p> 0.05). However, certain types of food (X2 = 165.9; p<0.05), family history of recurrent aphthous ulceration (X2 = 134.9; p<0.05), trauma (X2 = 99.9; p<0.05) and stress (X2 = 56.8; p< 0.05) had statistically significant association with recurrent aphthous ulcers (Table 3).
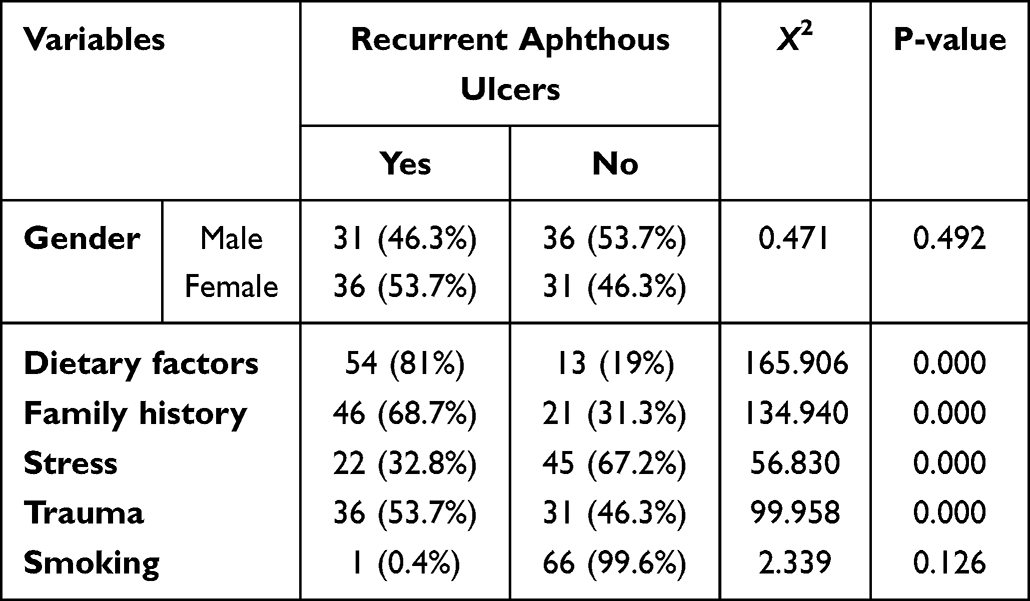 |
Table 3 Factors Associated with Recurrent Aphthous Ulceration |
Discussion
Recurrent aphthous ulcer is a common oral disorder that causes suffering and pain. Besides, it interferes with routine activities by affecting eating and wallowing. Therefore, having evidence on the prevalence and associated factors of recurrent aphthous ulceration gives policymakers insight into the proportion of communities who suffer from the condition in addition to related factors. However, the rate of this condition in different regions of the world had considerable variation.5 Hence, the present study illustrates the situation of the condition in the context of Afghanistan.
The result of this study reflects the rate of recurrent aphthous ulcers only in dental students of Kabul University of Medical Sciences. However, there is no reason to believe that this group of students is different from other students in Afghanistan. The subjects of this study were dentistry students who have passed the courses related to recurrent aphthous in their curriculum. Thus, they had enough knowledge of the signs and symptoms of the condition. Due to that, they were the right subjects for this study.
However, our study showed that the prevalence of recurrent aphthous ulcers was 30% among dentistry students at Kabul University of Medical Sciences. Comparison of the present finding with those from previous studies should be undertaken with caution because of differences in the study design, sample size, and geographical location. The result of this study was higher than that study by Muhammad Ajmal et al in Saudi Arabia conducted among dentistry students (14%).13 In contrast, it is lower than that of Safadi RA in Jordan (78%).14 This could be explained by differences that exist in the populations in terms of genetic predisposition, stress, lifestyle, and other related factors. Nevertheless, our result is also in line with studies of Du Qian et al in China (29.4%) carried out among college students15 and studies by Rabail Akbar et al conducted among students of Gulf Medical University (38.6%).4
Moreover, in this study dietary factors were claimed to be triggering recurrent aphthous ulceration, which is in line with a study in China. Du Qian et al in their study pointed out that the prevalence of recurrent aphthous ulcers was higher in those who consume sweet drinks, carbonated beverages, and fried foods, frequently.15 While Patil et al reported that foodstuff has less effect as a triggering factor for recurrent aphthous ulcers.16 Besides, family history was another important associated factor in our study, which is in line with others’ findings.17 Shi et al found a higher prevalence among those whose parents had recurrent aphthous ulceration than those whose parents did not have the condition.5 Respondents of this study claimed that stress was a triggering factor for the onset of recurrent aphthous ulcers, which is similar to others.18,19 A study by Sharma et al in India revealed that the rate of recurrent aphthous ulceration was higher among those who have experienced a severe level of stress than those who did not.20 The last finding of this study was trauma as a risk factor for the onset of recurrent aphthous ulceration. This was in line with the findings of a study in the United States21 but in contrast with another study in the United Arab Emirates.4
This study is the first to determine the prevalence and associated factors of recurrent aphthous ulceration in the context of Afghanistan. No other publication was found to address the prevalence and associated factors of this condition in Afghanistan.
Considering the various limitations of our study including the restricted study period and lack of a significant budget, led, not assess the influence of systemic conditions on the prevalence of recurrent aphthous ulcers. The study was conducted in a single institute and the data does not reflect reporting of the community as a whole. Hereupon, further observations are required with a large sample size.
Conclusion
We found that family history, stress, trauma, and dietary factors have an impact on the occurrence of RAS with no association with gender and smoking. Also, a considerable proportion of the study sample had experienced recurrent aphthous ulceration. Therefore, having evidence of the prevalence and associated factors among the Afghanistan population will help dental professionals to address this condition in their daily practice by giving proper information to their clients.
Transparency Declaration
The correspondent author (the manuscript’s guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; no important aspects of the study have been omitted, and any discrepancies from the study as planned have been explained.
Details of Ethical Approval
This research was approved by the Research and Ethics committee of Kabul University of Medical Sciences. Participants have agreed to take part in the survey and signed the consent form. We confirm that this study complies with the declaration of Helsinki.
Acknowledgment
We thank all who in one way or another contributed to the completion of this paper especially KUMS’ Research and Ethics Committee. First, we give thanks to Allah for protection and the ability to do work. We are so grateful to Professor Dr. Emal Shekaib, head of the Oral and Maxillofacial surgery department; Professor Dr. Ahmad Farid Daanish, member of the Pharmacology department; Dr. Ahmad Siyar Noormal, and the Faculty of Dentistry at the Kabul University of Medical Sciences (KUMS) for making it possible for us to conduct a study here. I give deep thanks to the students of the faculty for participating in this study.
Funding
No funding was received for carrying out this research.
Disclosure
The authors declare that there is no competing interest in this work.
References
1. Scully C, Porter S. Oral mucosal disease: recurrent aphthous stomatitis. Br J Oral Maxillofac Surg. 2008;46(3):198–206.
2. Naito M, Suzukamo Y, Wakai K, et al. One-year period prevalence of oral aphthous ulcers and oral health-related quality of life in patients with Behçet’s disease. Genet Res Int. 2014;2014:8.
3. Sciubba JJ. Oral mucosal diseases in the office setting–part I: aphthous stomatitis and herpes simplex infections. Gen Dent. 2007;55(4):347–376.
4. Akbar R, Kaur S, Pirasteh M, Tariq F, Al Tamimi D, Fuoad SA. Prevalence of recurrent aphthous ulcers in Gulf Medical University students. GMJ. 2016;5(S1):S115–S122.
5. Shi L, Wan K, Tan M, et al. Risk factors of recurrent aphthous ulceration among university students. Int J Clin Exp Med. 2015;8(4):6218.
6. Natah SS, Konttinen YT, Enattah NS, Ashammakhi N, Sharkey KA, Häyrinen-Immonen R. Recurrent aphthous ulcers today: a review of the growing knowledge. Int J Oral Maxillofac Surg. 2004;33(3):221–234.
7. Gallo CD, Mimura MA, Sugaya NN. Psychological stress and recurrent aphthous stomatitis. Clinics. 2009;64(7):645–648.
8. Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 1998;9(3):306–321.
9. Davatchi F, Tehrani BA, Jamshidi AR, et al. The prevalence of oral aphthosis in a normal population in Iran: a WHO-ILAR COPCORD study; 2008.
10. Shulman JD. Prevalence of oral mucosal lesions in children and youths in the USA. Int J Paediatr Dent. 2005;15:89–97.
11. Pongissawaranun W, Laohapand P. Epidemiologic study on recurrent aphthous stomatitis in a Thai dental patient population. Community Dent Oral Epidemiol. 1991;19(1):52–53.
12. Peretz B. Major recurrent aphthous stomatitis in an 11-year-old girl: case report. J Clin Pediatr Dent. 1994;18(4):309–312.
13. Ajmal M, Ibrahim L, Mohammed N, Al-Qarni H. Prevalence and psychological stress in recurrent aphthous stomatitis among female dental students in Saudi Arabia. Clujul Medl. 2018;91(2):216.
14. Safadi RA. Prevalence of recurrent aphthous ulceration in Jordanian dental patients. BMC Oral Health. 2009;9(1):1–5.
15. Du Q, Ni S, Fu Y, Liu S. Analysis of dietary-related factors of recurrent aphthous stomatitis among college students. Evid Based Complement Altern Med. 2018;2018. doi:10.1155/2018/2907812
16. Patil S, Reddy SN, Maheshwari S, Khandelwal S, Shruthi D, Doni B. Prevalence of recurrent aphthous ulceration in the Indian Population. J Clin Exp Dent. 2014;6(1):e36.
17. Maheswaran T, Yamunadevi A, Ayyappan S, Panda A, Sivakumar JS, Vaithiyanadane V. Prevalence and family history of recurrent aphthous stomatitis among the students of a dental institution in south India. J Indian Acad Dent Spec Res. 2014;1:53.
18. Byahatti SM. Incidence of Recurrent Aphthous ulcers in a group of the student population in Libya: a Questionnaire Study. Arch Cran Oro Fac Sc. 2013;1(2):26–30.
19. Delavarian Z, Rasekhi J, Seyyedi A, Salah S. Psychological assessment of patients with oral aphthous ulcers. J Islam Dent Assoc Iran. 2014;26(4):267–273.
20. Sharma M, Gupta R, Singh S. Correlation of psychological stress with recurrent aphthous stomatitis among dental students in an educational institution. Int J Appl Dent Sci. 2017;3(4):455–458.
21. Wray D, Graykowski EA, Notkins AL. Role of mucosal injury in initiating recurrent aphthous stomatitis. Br Med J. 1981;283(6306):1569–1570.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Drug Resistance Patterns and Trends in Patients with Suspected Drug-Resistant Tuberculosis in Dalian, China: A Retrospective Study
Pan Y, Yu Y, Lu J, Yi Y, Dou X, Zhou L
Infection and Drug Resistance 2022, 15:4137-4147
Published Date: 30 July 2022
Prevalence and Factors Associated with Hepatitis B Infection Among Outpatient Adults in South-Western Uganda
Rugaatwa Ndibarema E, Olum R, Ayebare D, Kabakyenga J
Hepatic Medicine: Evidence and Research 2022, 14:163-172
Published Date: 19 October 2022
Prevalence and Factors Associated with Alcohol Consumption Among Secondary School Students in Nekemte, Ethiopia: A Cross-Sectional Study
Shibiru T, Arulandhu A, Belete A, Etana J, Amanu W
Substance Abuse and Rehabilitation 2023, 14:35-47
Published Date: 12 May 2023
Prevalence and Associated Factors of Anemia Among Hospital Admitted Patients in Eastern Ethiopia
Yusuf MU, Abdurahman N, Asmerom H, Atsbaha T, Alemu A, Weldegebreal F
Journal of Blood Medicine 2023, 14:575-588
Published Date: 15 November 2023
Prevalence and Associated Factors of Chronic Obstructive Pulmonary Disease Among Adults in Neno District, Malawi: A Cross-Sectional Analytical Study
Zaniku HR, Connolly E, Aron MB, Matanje BL, Ndambo MK, Talama GC, Munyaneza F, Ruderman T, Rylance J, Dullie LW, Lalitha R, Banda NPK, Muula AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:389-401
Published Date: 5 February 2024