Back to Journals » Nature and Science of Sleep » Volume 13
Prevalence of Probable Shift Work Disorder in Non-Standard Work Schedules and Associations with Sleep, Health and Safety Outcomes: A Cross-Sectional Analysis
Authors Reynolds AC, Ferguson SA ![]() , Appleton SL
, Appleton SL ![]() , Crowther ME
, Crowther ME ![]() , Melaku YA
, Melaku YA ![]() , Gill TK
, Gill TK ![]() , Rajaratnam SMW
, Rajaratnam SMW ![]() , Adams RJ
, Adams RJ ![]()
Received 13 January 2021
Accepted for publication 3 May 2021
Published 31 May 2021 Volume 2021:13 Pages 683—693
DOI https://doi.org/10.2147/NSS.S301493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Amy C Reynolds,1,2 Sally A Ferguson,2 Sarah L Appleton,1 Meagan E Crowther,2 Yohannes Adama Melaku,1 Tiffany K Gill,3 Shantha MW Rajaratnam,4 Robert J Adams1
1Flinders Health and Medical Research Institute (Sleep Health)/Adelaide Institute for Sleep Health, Flinders University, Bedford Park, SA, Australia; 2Appleton Institute, CQ University Australia, Wayville, SA, Australia; 3Adelaide Medical School, University of Adelaide, Adelaide, SA, Australia; 4School of Psychological Sciences and Turner Institute for Brain and Mental Health, Monash University, Clayton, VIC, Australia
Correspondence: Amy C Reynolds
College of Medicine & Public Health, Flinders University, Level 2, Mark Oliphant Building, 5 Laffer Drive, Bedford Park, SA, 5042, Australia
Tel +61 4 07 525 047
Email [email protected]
Purpose: We aimed to estimate the prevalence of probable shift work disorder (pSWD) in a representative sample of Australian workers and identify sleep, health and safety correlates.
Patients and Methods: In 2019, data were collected from working respondents as part of a cross-sectional national sleep health survey conducted online (n=964 total; n=448 individuals on non-standard work schedules). We established the prevalence of pSWD according to International Classification of Sleep Disorders criteria (ICSD-R, ICSD-2 and ICSD-3). Poisson regression was used to determine crude and adjusted prevalence association (prevalence ratio, PR) of pSWD with sleep, health and safety outcomes.
Results: Overall prevalence of pSWD in workers on non-standard work schedules was 10.5%, ranging from 9.6% in early morning workers to 12.7% in rotating shift workers. In adjusted models, workers who met the criteria for pSWD were 1.8 times more likely to report both depression/bipolar disorder, and anxiety/panic disorder, and 1.7 times more likely to report work errors due to a sleep problem.
Conclusion: The prevalence of pSWD in employees engaged in non-standard work schedules is influenced by selection of factors used to quantify pSWD, including sleep/wake patterns. Higher likelihoods of mental health problems and workplace errors in those with pSWD highlight the importance of intervention and management of this under-recognised sleep disorder.
Keywords: sleep, sleep disorder, safety, mental health, occupational health, workplace
Introduction
Non-standard work schedules comprise inconsistent work arrangements which fall outside “standard” predictable, daytime work schedules (typically between 0900 and 1800).1 Around 16% of the Australian workforce habitually work shift work,2 similar to prevalence rates reported globally. In addition, recent estimates indicate 37% of workers in Australia report work hours which vary from week to week, or require them to be on call or on standby for work.2 Over half a million Australian workers hold multiple jobs; 38% of whom work 6 or 7 days a week.2 Non-standard work schedules are prevalent in Australia, and globally.
Non-standard work schedules are associated with poor health behaviours1 and adverse health outcomes, including increased susceptibility to chronic diseases.1,3,4 Shift work, the most commonly studied non-standard work schedule, has been linked with cardiovascular disease5 (eg coronary heart disease) and stroke,6 some cancers (particularly when night shift is involved),7 metabolic dysfunction (e.g. obesity)8 and type II diabetes,9 as well as increased all-cause mortality.10
Shift work, particularly involving night and rotating schedules, is associated with disturbed sleep and wake patterns, with insufficient sleep being one of the key contributors to the associations with chronic disease.11 Other aspects of non-standard work schedules including precarious or unpredictable employment, flexible work, on call or standby conditions, long work hours and overtime are also associated with poorer sleep and reduced wellbeing.12,13
Shift work disorder (SWD) is a clinical sleep disorder associated with non-standard work schedules that overlap with the usual time for sleep, the “biological night”.14 Most SWD research has focused on workers engaged in rotating and/or night shifts, meaning other non-standard work schedules (e.g. early mornings, and afternoon shifts), which also overlap the usual time for sleep, have not been routinely captured in SWD research.
Prevalence and correlates of SWD are poorly understood at a population level, as prevalence has typically been reported in specific worker subgroups (e.g. nurses,15–17 police officers,18 oil rig workers,19 airline personnel).20 Studies to date in these specific groups have suggested prevalence of SWD of almost 40% in some worker populations.16
Two existing population samples reporting SWD use varying questions to determine prevalence. The questions used to establish SWD in prior studies do not fully capture the extent of “insomnia and/or excessive sleepiness” and daytime dysfunction, all of which are central to the ICSD-3 SWD diagnostic criteria. Further, challenging our understanding of prevalence rates over time are the variations in chronicity for sleepiness and daytime dysfunction measures (from 2 weeks to >3 months). This limits utility and interpretation of prevalence rates, as well as our ability to identify and manage workers at risk for SWD. ICSD-3 criteria have recently been used in a specific worker sample by Voinescu;21 however, the methods for identifying those with SWD did not seem to account for variability in sleep-wake patterns.
Additionally, in estimating prevalence of SWD, the type of shift work is often overlooked or restricted to a specific worker group (e.g. rotating or night shift workers). Given workers who do not identify as shift workers also exhibit a relationship between sleepiness and errors,22 considering the prevalence of SWD in other non-standard work schedules is timely. Further, quantifying the “disturbed sleep/wake pattern” using the current ICSD-3 criteria can be challenging in population datasets where actigraphy or sleep diary is less common. We propose a proxy measure of disturbed sleep/wake patterns such as social jetlag be used when cross-sectional designs do not allow for activity-based estimations.
The aim of our study was to establish the prevalence of SWD using current ICSD-3 diagnostic criteria, with secondary aims of determining associations of SWD with sociodemographic factors, additional non-standard work schedule factors and health and safety outcomes in Australian workers.
Patients and Methods
We conducted an online, cross-sectional survey of Australian sleep health in March and April 2019. Complete details and a Checklist for Reporting Results of Internet E-Surveys (CHERRIES) have been reported previously.23 Participants of the complete sample (n=2044) were required to be ≥18 years of age and were drawn from an existing online panel of participants maintained by Dynata (previously Research Now and Survey Sampling International, Melbourne, Australia). Three-stage randomization was used to reduce the risk of bias and ensured that participants were blinded to the topic of the survey until their suitability for participation had been determined. The survey recruitment process has previously been reported.24 Participants were provided with a study overview and the opportunity to participate. Commencing the study inferred informed consent to participate. The final sample was matched to the Australian Bureau of Statistics (ABS) estimates for a variety of sociodemographic factors including age, sex, location and education.23 The Human Research Ethics Secretariat at the University of Adelaide Office of Research Ethics, Compliance and Integrity provided ethical approval to conduct the study (H-2018-214), which was conducted in accordance with the Declaration of Helsinki.
Operationalizing Shift Work Disorder
Prevalence of probable SWD (pSWD) was established using three approaches consistent with ICSD-R, ICSD-2 and ICSD-3 criteria in order to a) facilitate comparison with existing estimates, and b) transparently establish the differences in prevalence when using different diagnostic criteria, particularly relating to inclusion of changes in total sleep time between work and non-work days, and of disturbed sleep/wake patterns (social jetlag) in the SWD definition. Briefly, the minimum diagnostic criteria for Shift Work Disorder according to ICSD-3 include: sleep/wake disturbance reflected by insomnia and/or excessive daytime sleepiness, plus reduced sleep time, in workers on a work schedule which interferes with usual sleep opportunities PLUS symptoms persisting for a minimum of 3 months PLUS disturbed sleep/wake pattern for at least 14 days (usually established with sleep log and/or actigraphy) PLUS absence of a better explanation for the sleep/wake disturbance (e.g. presence of another disorder, use of medications, poor sleep hygiene).14
Recurring work schedule that overlaps with the usual time for sleep was established by self-report response to the question “Thinking about the past 3 months, which of the following best describes your work schedule? Would you say that you worked … ” with response items of standard office hours, early morning shifts (start before 0800), afternoons (from 3pm), evenings (after 7pm), nights, rotating shifts, other, refused/do not know. Responses for other, refused/do not know were checked for open text details to see if they could be categorised according to existing criteria. Where this was not possible, data were excluded from analyses. Work schedules included in the analyses were early morning shifts, afternoons, evenings/nights (combined due to small sample size), and rotating shifts. The additional components from ICSD-3 diagnostic criteria are outlined below.
Difficulties initiating or maintaining Sleep (DIMS) – DIMS was assessed using a series of questions designed to quantify insomnia and excessive sleepiness based on ICSD-3 criteria for insomnia disorder. Criteria A specifies that workers should report insomnia and/or excessive sleepiness, with symptoms present for at least 3 months. We used the ICSD-3 requirements of DIMS/DD to meet criteria for insomnia. This meant workers needed to report at least one DIMS and one DD for >3 months. The questions used directly aligned with ICSD-3 DIMS and DD requirements for insomnia disorder.25
DIMS questions included the following
In the past month, how often have you experienced the following? Difficulty falling asleep; Waking a lot during the night; and Waking up too early and not able to get back to sleep.
Participants were coded as experiencing chronic DIMS if they reported at least one DIMS a few nights a week or more, and for >3 months.
Daytime dysfunction (DD) – DD was quantified using a series of questions about daytime impairment. Nine separate questions were asked for a variety of indicators of distress or impairment, specifically ‘In the past month how often have you experienced these daytime feelings? Experienced sleepiness that interfered with your daily activities; Felt sleepy when sitting quietly during the day or early evening; Felt fatigue or exhaustion; Felt irritable or moody; Reduced motivation or energy; Reduced concentration, attention or memory; Been hyperactive, impulsive or aggressive; Had little interest or pleasure in doing things; Felt down, depressed or hopeless. Participants were coded as experiencing DD if they reported at least one DD a few nights a week or more, and for >3 months.
Total sleep time (TST) – Reduction of TST was quantified using participant reported habitual total sleep time on work days and non-work days. The essential features of SWD described in the ICSD-3 criteria indicate that sleep duration is typically shortened by 1–4 hours, so any workers who reported ≥1 hour of shorter sleep on work days in addition to DIMS and DD were considered to meet criteria A (reduction in total sleep time).
Social jetlag (SJL) – While 14 days of monitoring via diary, or using dim light melatonin onset26 is ideal to identify a disturbed sleep and wake pattern per ICSD-3 diagnostic criteria D for SWD, this was not practical or financially feasible in a population sample, so a social jetlag variable (SJL >30 min) was used. Specifically, a disturbed sleep/wake pattern was determined by calculating SJL as reported previously,27 using the Jankowski28 sleep correction. This allowed us to compare social jetlag as a function of change in sleep midpoint between work and non-work sleep schedules irrespective of time of sleep opportunities in the 24-hour day.
SWD1 (DIMS, DD): The first operational definition of pSWD was established in line with ICSD-R criteria for SWD to facilitate comparison with existing studies. This comprised a work schedule which overlaps with usual time for sleep, plus self-report of at least one difficulty initiating or maintaining sleep (DIMS) or one report of daytime dysfunction (DD) as operationalised above.
SWD2 (DIMS, DD, TST): The second operational definition of pSWD extended the first, with the additional requirement that participants had to report ≥60 minute decrease in habitual total sleep time (TST) on non-work days compared with work days.
SWD3 (DIMS, DD, TST, SJL): The final operational definition of pSWD most closely approximates the current minimum diagnostic criteria for SWD according to ICSD-3, extending SWD2 by adding an indicator of disturbance to sleep and wake patterns (SJL). To ensure participant characteristics were similar between the total non-standard working sample and the final sample, sociodemographic and occupational characteristics were compared by work schedule type (see Supplementary Table 1). Proportions were similar between the samples.
Occupational Variables
In addition to our work schedule question, work characteristics including degree of physical exertion/strain, whether respondents were required to be on call for work or not (categorised as no, or ≥ once/month), habitual work hours per week and number of jobs worked were self-reported. Having a higher non-standard work burden was determined if participants indicated they worked either >40 hours per week, or more than one job, in addition to their non-standard work schedule. Participants self-reported their current occupation, which was subsequently coded according to Australia and New Zealand Standard Classification of Occupations (ANZSCO).
Sleep and Chronotype Variables
Participants self-reported habitual bed and rise times on work and non-work days using 24-hour format, which provided time in bed (TIB) values for work and non-work days. Additionally, self-reported total sleep time (TST) was provided for work and non-work days. Participants were asked to self-report whether they felt they had a sleep problem or not; noting that this question was asked after other sleep variables to avoid introducing order effects bias. Chronotype was established using the reduced Morningness-Eveningness Questionnaire (rMEQ).29
Health and Safety Variables
For doctor-diagnosed physical and mental health conditions, participants were asked “Have you ever been told by a doctor that you have” arthritis, diabetes, high blood pressure, heartburn or reflux, depression or bipolar disorder, anxiety or panic disorder, post-traumatic stress, and asthma. Obesity was determined as a BMI >30, from participants’ self-reported height and weight. Pain which disturbs sleep was established from a response of “most nights (4–6 nights/week)” or “every night” to either of the following questions: “How often does pain stop you from going to sleep at night?” or “How often does pain wake you up at night?”
Work errors due to a sleep problem were determined from the question “Thinking about the past three months, how many days did you make errors at work because you were too sleepy or you had a sleep problem?”, and presenteeism with “Over the past 12 months how often have you gone to work despite feeling that you really should have taken sick leave because of your state of health?”
Data Analysis
Data were analysed with IBM SPSS Statistics version 26.0 (IBM Corporation, Armonk, NY). For unadjusted demographic characteristics Pearson χ2 analyses were conducted. Comparison between groups for continuous, normally distributed sleep data were analysed with Independent Samples t-tests. Missing data related to DIMS, DD, TST or SJL meant n=56 working participants were not included in final analyses.
Poisson regression analyses were conducted to determine the prevalence ratio (PR) for health and safety outcomes associated with pSWD. Unadjusted (uPR) and adjusted (aPR) models are reported, with the multivariable model adjusting for age and sex. Given the relatively small sample size of workers meeting pSWD criteria, 95% profile likelihood confidence intervals are reported over Wald confidence intervals for the exponentiated coefficient.
Results
Of the 2,044 participants aged 18–90 years in the original survey, 1,057 respondents (51.7%) indicated they were working in the 3 months preceding the survey. The Australian participation rate in employment (15–64 years) is 66.1%, and 14.3% for ≥65 years.30 In comparison, 60.1% of our sample’s 18–64 years and 14.6% of ≥65 years were employed. Of these 1,057 respondents, n=964 (91.2%) provided details about their current work schedules. Fifty-three percent of current workers (n=516) reported standard office hours, 20.6% (n=199) reported early morning schedules (pre-0800 start), 7.9% (n=76) reported an afternoon schedule (shift starting from 3pm onwards), 5.9% (n=57) reported evening (shift starting from 7pm) or night shift schedules, and 12.0% (n=116) reported rotating shifts.
Prevalence of Probable Shift Work Disorder (pSWD)
Prevalence overall by definition, and by work schedule, are provided in Table 1. A relationship between work schedule and pSWD was only observed when pSWD was estimated based only on at least one symptom of insomnia and/or excessive sleepiness for at least 3 months (χ23=9.49, p=0.023; see Table 1). This definition also resulted in the highest overall prevalence rate of pSWD (39.5%, n=177). When the additional criteria of ≥60 minutes less sleep on work days was included, the prevalence rate of pSWD lowered (15.0%, n=59). When social jetlag was added as a criterion for SWD to account for disturbed sleep/wake patterns, the overall prevalence of pSWD was 10.5% (n=41).
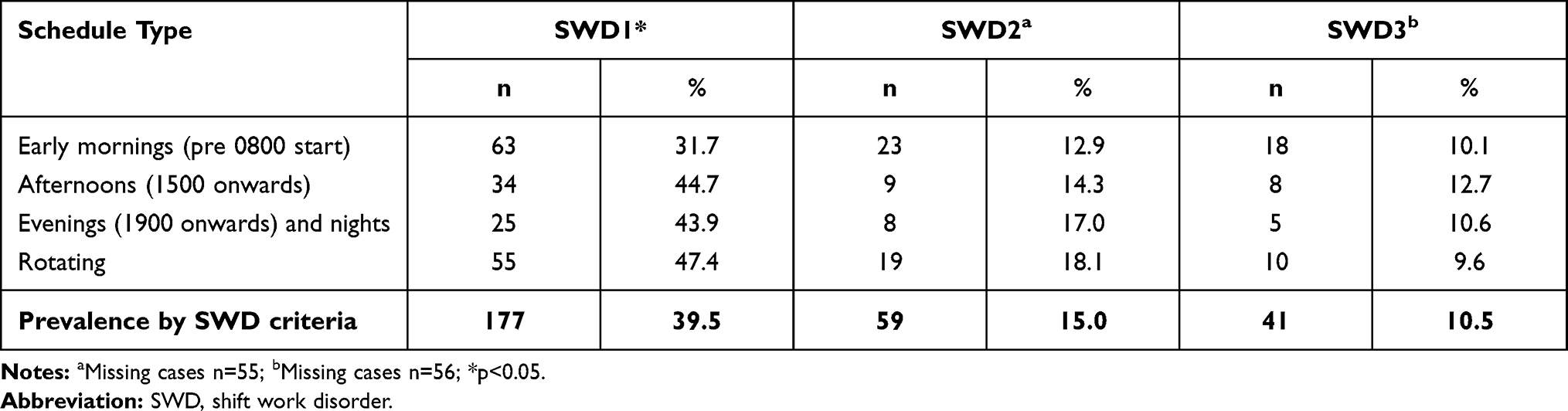 |
Table 1 Prevalence of Shift Work Disorder by Work Schedule |
All remaining analyses were conducted with SWD3 definition including SJL, to align with current ICSD-3 minimum criteria for diagnosis. As mental health outcomes were used as endpoints, we determined whether participants who reported mental health symptoms from the chronic daytime dysfunction responses (Been hyperactive, impulsive or aggressive; Had little interest or pleasure in doing things; Felt down, depressed or hopeless) needed to be removed from the analyses. However, only 11 (2.5%) of our working sample reported chronic symptoms related only to these symptoms with no other chronic DIMS or DD; of these, only two met criteria for pSWD. Sensitivity analyses revealed that removing these participants from the analyses did not change mental health endpoints (data not shown).
Characteristics of Workers with pSWD
Participant characteristics are provided by SWD3 in Table 2. Sociodemographic and occupational characteristics were not associated with a higher prevalence of SWD (all p>0.05, see Table 2).
 |
Table 2 Prevalence of Shift Work Disorder According to Demographic and Occupational Characteristics |
Sleep
Sleep variables are presented in Figure 1. Average time in bed (TIB; ±SD) did not differ significantly between workers with and without pSWD on either work days (SWD: 454.5±96.6, non-SWD: 468.6±104.8, t374=0.8, p=0.426) or non-work days (SWD: 543.2±96.0, non-SWD: 512.9±106.2, t374=−1.7, p=0.090). Total sleep time (TST) on work days was shorter in workers with pSWD (379.2±93.6) compared to those who did not (430.6±82.9; t374=3.6, p<0.001). A significant difference in TST on non-work days was also observed (SWD: 502.3±96.8, non-SWD: 462.5±95.8, t374=−2.5, p=0.015). Of those with pSWD, 20.0% did not think they had a sleep problem, 45.0% said they did think they had a sleep problem, and 35.0% felt they may have a sleep problem.
 |
Figure 1 Time in bed and total sleep time on work and non-work days. Grey boxes reflect values for participants with probable shift work disorder (SWD). Patterned boxes reflect total sleep time for both SWD and no SWD. Notes: *p<0.05; ***p<0.001; bars=SD. |
Of those with pSWD, 59.5% were neither morning or evening chronotype, 27.0% were morning type, and 13.5% were evening type. Likelihood of pSWD was not associated with chronotype (χ22=4.4, p=0.112).
Health and Work Safety Outcomes
Prevalence of individual health and safety outcomes in workers with pSWD are provided in Table 3, as unadjusted PR (Model 1) and aPR (Model 2). Participants with pSWD were more likely to report depression or bipolar disorder, and anxiety or panic disorder, compared to participants without pSWD. Workers with pSWD were 1.7 times more likely to report work errors in the preceding three months which they attributed to a sleep problem. No differences between workers were observed for chronic physical health conditions. Self-reported general health on the SF-1 did not differ between workers with and without pSWD (aPR=1.4, 95% CI: 0.8, 2.2), with both groups reporting high prevalence of fair or poor general health (pSWD=41.5%, no pSWD=30.9%).
 |
Table 3 Prevalence of Doctor Diagnosed Health Conditions and Self-Reported Safety Outcomes by Probable Shift Work Disorder (pSWD) |
Discussion
Our study provides prevalence of probable SWD (pSWD), based on current (ICSD-3) diagnostic criteria, in an online sample of Australian adults matched to census estimates for a variety of demographic characteristics. When including social jetlag as an indicator of disturbed sleep/wake patterns, a lower prevalence of workers with pSWD is found (10.5%) than when using DIMS and daytime dysfunction alone (39.5%) or with DIMS, daytime dysfunction and >1 hour less sleep on work compared with non-work days (15.0%). The prevalence of pSWD is provided across a variety of non-standard work schedules, highlighting that pSWD is a concern for between 9.6% and 12.7% of workers depending on their habitual work schedule. There was a higher prevalence of adverse mental health outcomes including depression or bipolar disorder, and anxiety or panic disorder in workers with pSWD in our sample. Our findings point to a need to identify and manage SWD in workers across all forms of non-standard work schedules in order to support mental health outcomes and reduce risk of work errors, which are more prevalent in workers on these schedules.
Comparison with Prevalence Rates from Previous ICSD Criteria for Shift Work Disorder
We presented prevalence rates aligned with the different criteria in order to facilitate comparison with previous studies. Drake et al.31 most closely aligned with our SWD1 criteria in workers on a night or rotating shift schedule for at least the previous two weeks. The authors reported prevalence rates of 31.1% and 26.1%, respectively. In contrast, our sample showed a higher prevalence of pSWD in both evening/night workers (43.9%) and rotating workers (47.4%) using the SWD1 criteria. Of note, evening workers were excluded from the Drake et al.31 analysis, while both evening and night workers were combined in the present study.
The prevalence of pSWD among night workers (17.0%), when accounting for changes to total sleep time between work and non-work days, was lower than reported from previous Australian samples using ICSD-2 criteria (32.1%),32 but higher than those working evening shift in an Eastern European country, where no SWD was detected.21 This may be a function of different questions, with previous work specifically asking participants if they felt their sleep or sleepiness problem was related to their work schedule.32 Categorisation of work schedules could also explain differences. Evening, night and rotating shift workers were grouped to form a broader “night worker” category in the work of di Milia et al.,32 while afternoon workers were grouped with workers of daytime hours to form a “day worker” category.
Our findings highlight that collapsing work schedules into groups may mask prevalence of pSWD in early morning and afternoon workers. While “early morning” workers have the lowest prevalence across all definitions of pSWD, afternoon workers have highest prevalence rates. Rotating shift workers were examined separately in a survey of workers by Voinescu,21 and showed a higher prevalence of SWD than our sample. This is likely because of our adjustment for social jetlag in line with ICSD-3 criteria, as the rate of SWD in rotating workers from Voinescu21 (17.5%) closely aligned with our prevalence (18.1%) using a definition (SWD2) which did not include adjustment for sleep/wake patterns. Family or social responsibilities may differentially impact sleep and recovery time for workers on afternoon shift but this needs to be investigated further.
Previous studies have mostly estimated pSWD in specific worker populations, which limits insight into prevalence in the broader population. The difference between ICSD-2 and ICSD-3 in our crude prevalence ratios is consistent with findings from Vanttola et al in hospital workers,33 noting that within our population sample, the prevalence of pSWD was higher in every shift schedule (9.6% - 12.7%) compared to hospital workers alone (2.5–9.5%). Sample size limited our ability to investigate occupation as a predictor of pSWD, although it is worth noting that the highest percentage of shift work cases was observed in community and personal service workers, which includes aged care, hospitality workers, and some emergency service workers (police, fire). Future population-level studies of pSWD in larger samples should consider the relationship between schedule type, occupation and SWD in more detail.
Taken with existing findings, our study suggests there is a need to better characterise SWD across a range of occupational and cultural contexts, and in large samples. Our findings also suggest there may be benefit in screening for SWD broadly across non-standard work schedules, as pSWD was not limited to workers of specific age, income, or domestic partnership arrangements as in previous studies.16 Screening tools in occupations with non-standard work schedules may be an appropriate and relatively easy way to identify pSWD in diverse worker groups.34 In contrast to previous findings,32 pSWD in the present study was also not associated with longer work hours. However, pSWD was associated with work factors beyond the criteria for SWD such as reporting more than one job, and/or long work hours in combination with a non-standard work schedule. Workload factors beyond work hours were not explored in previous prevalence studies, and may be useful in identifying workers at risk of pSWD.
Workers, on average, achieved less than recommended sleep on work nights, noting that those who did not meet criteria for pSWD were closer to the recommended minimum of seven hours. Self-reported time in bed for both groups does not appear to facilitate an adequate opportunity to achieve a minimum of seven hours of sleep per night on work nights. These data should be interpreted with caution given they are self-reported, and future studies should look to include objective assessments of sleep at the population level to confirm duration, quality, and timing.
While we observed no associations with physical health problems, pSWD was associated with a higher prevalence of self-reported, doctor diagnosed mental health problems. This is supportive of previous findings that depression is more common in individuals meeting pSWD criteria.16,31,35 However, depression and other mental health conditions are also associated with insomnia symptoms and poor sleep.36 It is not possible to establish the causal relationship between mental health conditions and pSWD in the present study. Our findings do highlight the need for prospective, longitudinal assessment of pSWD and mental health outcomes to best understand the trajectories of mental health conditions with exposure to non-standard work schedules.
Individuals with pSWD were more likely to report making an error at work due to a sleep problem. These findings are consistent with previous community-based studies of Australian workers, where 29% of workers recall making an error at work due to sleepiness or sleep problem, irrespective of their work schedules.22 This is particularly pertinent to safety-critical occupational contexts. These findings demonstrate a clear need to identify and address pSWD in order to improve mental health and productivity outcomes for employees on non-standard work schedules.
The present study provides prevalence estimates for pSWD according to ICSD-3 criteria in an online sample of Australian workers. We used a comprehensive collection of sleep, work schedule and timing variables to operationalise pSWD. The use of multiple DIMS and daytime dysfunction estimates over a three-month period allows for a robust calculation of DIMS which does not rely on the worker personally attributing their sleepiness or symptoms specifically to fatigue. We also included changes in total sleep time (TST) between work and non-work days, along with a measure of social jetlag, to accommodate the disturbed sleep/wake pattern component of current SWD diagnostic criteria. When pSWD is estimated with these additional selection criteria, prevalence rates are lower than previous studies. This more closely approximates current diagnostic criteria. Importantly, we were also able to demonstrate associations with sleep, health and safety outcomes in current workers, which illustrates the importance of identifying and managing SWD for individual and employer outcomes.
Limitations
The ICSD-3 definition of shift work disorder specifies that workers should have ‘a report of insomnia and/or excessive sleepiness’. By using the ICSD-3 insomnia criteria to quantify DIMS and DD for this study, it is plausible that there is some unavoidable overlap between insomnia disorder and SWD in the present analyses. This overlap in definition reflects the broader challenge of establishing that a sleep disorder is not a consequence of other medical conditions, particularly in cross-sectional data. Thus, prospective studies with relatively new workers are crucial if we are to understand the aetiology of SWD independent of other medical conditions.
The temporal association between DIMS and DD on work versus non-work days was not assessed in this study. Future investigations of SWD should consider adopting questionnaire approaches which establish whether the experience of sleepiness symptoms varies by work and non-work days, as seen in previous occupation-specific investigations of SWD, including police officers23 and firefighters37.
The ICSD-3 criteria call for objective assessment of sleep/wake patterns which was not possible in this representative dataset. In future, it would be useful to establish the validity of a standard set of questions which are usable in larger-scale epidemiologic studies against sleep logs, actigraphy and if required, polysomnography. We did not have sufficient cases to explore the relationships between occupation and pSWD. Given that prevalence estimates in studies of specific occupations vary from 3% to >60%38, there is a clear need to better establish the prevalence of SWD in large, representative population datasets, and also by occupation.
The early morning (pre-0800 start) schedule could be perceived as being one which does not interfere with the usual time for sleep, particularly if individuals are early chronotypes. However, by including TST differences on work and non-work days and social jetlag, we are able to obtain a prevalence of SWD which likely considers these factors and identifies workers at risk of pSWD. Our cross-sectional prevalence estimates are almost certainly influenced by the healthy worker effect, and do not provide insight into workers who may have experienced pSWD and modified their working arrangements accordingly. Finally, affective disorders were grouped (depression and bipolar disorder; anxiety and panic disorder) in the original questionnaire, and did not allow for analyses independently – these distinctions could be addressed in future studies.
Conclusion
According to ICSD-3 criteria, pSWD impacts one in ten current Australian workers engaged in various non-standard work schedules. The higher prevalence of mental health conditions and workplace errors in those with pSWD illustrates a need to identify and manage vulnerable workers to improve individual wellbeing, as well as workplace productivity and safety. Similar sleep profiles in those with and without pSWD suggest that sleep education and sleep hygiene strategies are unlikely to be the only pathway to improve. Identifying workers with pSWD provides important opportunities for referral to specialised sleep services, where tailored management plans including known interventions for pSWD such as sleep scheduling, melatonin, and use of modafinil, can be considered. This has implications for improving mental health in workers on non-standard work schedules, and is likely also important for managing workplace errors given the higher likelihood seen in participants with pSWD.
Disclosure
The online survey was funded by the not-for-profit Australian Sleep Health Foundation, using an unrestricted grant from Merck, Sharp & Dohme (MSD Australia) Pty Limited, awarded to RJA, SLA, TKG and ACR. MSD played no role in study design, execution, analysis or publication. SWR has been a consultant and a program leader for the Alertness CRC, a director of the Sleep Health Foundation, and has received funds for research or consultancies paid to Monash from Vanda Pharmaceuticals, Circadian Therapeutics, Teva Pharmaceuticals, Shell, Rio Tinto, BHP Billiton, Alertness CRC & Seeing Machines. Dr Amy C Reynolds reports grants from Sleep Health Foundation/Merck Sharp and Dohme, during the conduct of the study; personal fees from Sealy Australia, outside the submitted work.
Dr Sarah Appleton reports grants from Sleep Health Foundation, during the conduct of the study; and received an honorarium from Dove Press as Associate Editor-in-Chief of Nature and Science of Sleep.
Professor Shantha Rajaratnam reports grants from Vanda Pharmaceuticals, grants from Philips Respironics, Cephalon, Rio Tinto, BHP Billiton, Shell, non-financial support from Optalert, as well as non-financial support from Compumedics, Teva Pharmaceuticals, and Circadian Therapeutics, outside the submitted work.
Dr Robert Adams reports grants from Sleep Health Foundation, during the conduct of the study; and grants from ResMed Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Winkler MR, Mason S, Laska MN, Christoph MJ, Neumark-Sztainer D. Does non-standard work mean non-standard health? Exploring links between non-standard work schedules, health behavior, and well-being. SSM Popul Health. 2018;4:135–143. doi:10.1016/j.ssmph.2017.12.003
2. Australian Bureau of Statistics. Working time arrangements. Contract No.: 6342.0. 2013.
3. Åkerstedt T, Wright KP. Sleep loss and fatigue in shift work and shift work disorder. Sleep Med Clin. 2009;4(2):257–271. doi:10.1016/j.jsmc.2009.03.001
4. Drake C, Wright JK. Shift work, shift-work disorder, and jet lag. Princ Pract Sleep Med. 2011;1:784–798.
5. Torquati L, Mielke GI, Brown WJ, Kolbe-Alexander T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand J Work Environ Health. 2018;44(3):229–238. doi:10.5271/sjweh.3700
6. Vyas MV, Garg AX, Iansavichus AV, et al. Shift work and vascular events: systematic review and meta-analysis. BMJ. 2012;345:e4800. doi:10.1136/bmj.e4800
7. Haus EL, Smolensky MH. Shift work and cancer risk: potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med Rev. 2013;17(4):273–284. doi:10.1016/j.smrv.2012.08.003
8. van Drongelen A, Boot CR, Merkus SL, Smid T, van der Beek AJ. The effects of shift work on body weight change - a systematic review of longitudinal studies. Scand J Work Environ Health. 2011;37(4):263–275. doi:10.5271/sjweh.3143
9. Axelsson J, Puttonen S. Night shift work increases the risk for type 2 diabetes. Evid Based Med. 2012;17(6):193. doi:10.1136/ebmed-2012-100649
10. Lin X, Chen W, Wei F, Ying M, Wei W, Xie X. Night-shift work increases morbidity of breast cancer and all-cause mortality: a meta-analysis of 16 prospective cohort studies. Sleep Med. 2015;16(11):1381–1387. doi:10.1016/j.sleep.2015.02.543
11. Kecklund G, Axelsson J. Health consequences of shift work and insufficient sleep. BMJ. 2016;355:i5210. doi:10.1136/bmj.i5210
12. Benach J, Vives A, Tarafa G, Delclos C, Muntaner C. What should we know about precarious employment and health in 2025? Framing the agenda for the next decade of research. Int J Epidemiol. 2016;45(1):232–238. doi:10.1093/ije/dyv342
13. Bamberg E, Dettmers J, Funck H, Krahe B, Vahle-Hinz T. Effects of on-call work on well-being: results of a daily survey. Appl Psychol Health Well Being. 2012;4(3):299–320. doi:10.1111/j.1758-0854.2012.01075.x
14. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
15. Waage S, Pallesen S, Moen B, et al. Predictors of shift work disorder among nurses: a longitudinal study. Sleep Med. 2014;15(12):1449–1455. doi:10.1016/j.sleep.2014.07.014
16. Flo E, Pallesen S, Magerøy N, et al. Shift work disorder in nurses – assessment, prevalence and related health problems. PLoS One. 2012;7(4):e33981. doi:10.1371/journal.pone.0033981
17. Chen D, Jiang M, Shi X, et al. Predictors of the initiation of shift work disorder among Chinese intern nurses: a prospective study. Sleep Med. 2020;68:199–206. doi:10.1016/j.sleep.2019.11.1263
18. Rajaratnam SMW, Barger LK, Lockley SW, et al. Sleep disorders, health, and safety in police officers. JAMA. 2011;306(23):2567. doi:10.1001/jama.2011.1851
19. Waage S, Moen BE, Pallesen S, et al. Shift work disorder among oil rig workers in the North Sea. Sleep. 2009;32(4):558–565. doi:10.1093/sleep/32.4.558
20. Vanttola P, Härmä M, Viitasalo K, et al. Sleep and alertness in shift work disorder: findings of a field study. Int Arch Occ Env Hea. 2019;92(4):523–533. doi:10.1007/s00420-018-1386-4
21. Voinescu BI. Common sleep, psychiatric, and somatic problems according to work schedule: an internet survey in an Eastern European country. Int J Behav Med. 2018;25(4):456–464. doi:10.1007/s12529-018-9719-y
22. Ferguson SA, Appleton SL, Reynolds AC, et al. Making errors at work due to sleepiness or sleep problems is not confined to non-standard work hours: results of the 2016 Sleep Health Foundation national survey. Chronobiol Int. 2019;36(6):758–769. doi:10.1080/07420528.2019.1578969
23. Appleton SL, Reynolds AC, Gill TK, Melaku YA, Adams R. Waking to use technology at night, and associations with driving and work outcomes: a screenshot of Australian adults. Sleep. 2020;43(8). doi:10.1093/sleep/zsaa015
24. Adams RJ, Appleton SL, Taylor AW, et al. Sleep health of Australian adults in 2016: results of the 2016 Sleep Health Foundation national survey. Sleep Health. 2017;3(1):35–42. doi:10.1016/j.sleh.2016.11.005
25. Sweetman AM, Melaku YA, Lack L, et al. Prevalence and associations of co-morbid insomnia and sleep apnoea in an Australian population-based sample. Sleep Med. 2021;82:9–17. doi:10.1016/j.sleep.2021.03.023
26. Broussard JL, Reynolds AC, Depner CM, Ferguson SA, Dawson D, Wright KP. Circadian rhythms versus daily patterns in human physiology and behavior. In: Kumar V, editor. Biological Timekeeping: Clocks, Rhythms and Behaviour. New Delhi: Springer India; 2017:279–295.
27. Lang CJ, Reynolds AC, Appleton SL, et al. Sociodemographic and behavioural correlates of social jetlag in Australian adults: results from the 2016 National Sleep Health Foundation Study. Sleep Med. 2018;51:133–139. doi:10.1016/j.sleep.2018.06.014
28. Jankowski KS. Social jet lag: sleep-corrected formula. Chronobiol Int. 2017;34(4):531–535. doi:10.1080/07420528.2017.1299162
29. Adan A, Almirall H. Horne & Östberg morningness-eveningness questionnaire: a reduced scale. Pers Individ Dif. 1991;12(3):241–253. doi:10.1016/0191-8869(91)90110-W
30. Australian Bureau of Statistics. Labour force, Australia, detailed: Australian Bureau of Statistics; 2021. Available from: https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia-detailed/feb-2021.
31. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Sleep. 2004;27(8):1453–1462. doi:10.1093/sleep/27.8.1453
32. Di Milia L, Waage S, Pallesen S, Bjorvatn B. Shift work disorder in a random population sample – prevalence and comorbidities. PLoS One. 2013;8(1):e55306. doi:10.1371/journal.pone.0055306
33. Vanttola P, Puttonen S, Karhula K, Oksanen T, Härmä M. Prevalence of shift work disorder among hospital personnel: a cross-sectional study using objective working hour data. J Sleep Res. 2020;29:e12906. doi:10.1111/jsr.12906
34. Barger LK, Ogeil RP, Drake CL, O’Brien CS, Ng KT, Rajaratnam SMW. Validation of a questionnaire to screen for shift work disorder. Sleep. 2012;35(12):1693–1703. doi:10.5665/sleep.2246
35. Kalmbach DA, Arnedt JT, Song PX, Guille C, Sen S. Sleep disturbance and short sleep as risk factors for depression and perceived medical errors in first-year residents. Sleep. 2017;40(3). doi:10.1093/sleep/zsw073
36. Jansson-Frojmark M, Lindblom K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J Psychosom Res. 2008;64(4):443–449. doi:10.1016/j.jpsychores.2007.10.016
37. Barger, LK, Rajaratnam, SMW, Wang, W, et al. Common sleep disorders increase risk of motor vehicle crashes and adverse health outcomes in firefighters. Journal of Clinical Sleep Medicine. 2015;1(3):233–240.
38. Taniyama Y, Nakamura A, Yamauchi T, Takeuchi S, Kuroda Y. Shift-Work Disorder and Sleep-Related Environmental Factors in the Manufacturing Industry. Journal of UOEH. 2015;37(1):1–10.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.