Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Prevalence of Posttraumatic Stress Disorder and Depression Among Internally Displaced Persons in Mogadishu-Somalia
Authors Ali M, Mutavi T, Mburu JM, Mathai M
Received 30 November 2022
Accepted for publication 22 February 2023
Published 28 February 2023 Volume 2023:19 Pages 469—478
DOI https://doi.org/10.2147/NDT.S398423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Mustafa Ali, Teresia Mutavi, John Maina Mburu, Muthoni Mathai
Department of Psychiatry, University of Nairobi, Nairobi, Kenya
Correspondence: Mustafa Ali, Department of Psychiatry, School of Medicine, College of Health Sciences, University of Nairobi, P.O. Box 19676-00200, Nairobi, Kenya, Email [email protected]; [email protected]
Background: Nearly 2.6 million people have been forced into displacement camps in Somalia as a result of frequent conflicts exacerbated by climate change disasters. Although the psychological impact of war and natural disasters is well documented elsewhere, little is known about the unseen scars of psychological trauma among internally displaced persons (IDPs) in Somalia. This study was carried out between January and February 2021 and sought to determine the prevalence of post-traumatic stress disorder (PTSD) and depression among IDPs and examine the association between displacement and these psychiatric conditions.
Methodology: A cross-sectional quantitative study was conducted among 401 IDPs in Mogadishu. The Harvard Trauma Questionnaire was used to determine the levels of trauma exposure and PTSD, and Hopkins Symptom Checklist-25 was used to estimate the prevalence of depression. Multivariate and bivariate analyses were performed to analyze the association between demographic and displacement variables and the outcomes of PTSD and depression.
Results: More than half (59%) of participants met the symptom criteria of depression, and nearly a third (32%) of respondents met the symptom criteria for PTSD. The most prevalent traumatic event was a lack of food or water (80.2%). Important predictive factors for the development of psychiatric morbidity were unemployment, cumulative traumatic exposure, and frequency and duration of displacement.
Conclusion: The study revealed high levels of depressive disorder and PTSD among IDPs in Mogadishu. Furthermore, this study provided evidence of IDPs’ susceptibility to trauma exposure and lack of essential services and goods. The study highlighted the importance of the provision of Mental Health and Psychosocial Support (MHPSS) services in IDP camps.
Keywords: trauma, depression, PTSD, Somalia, IDPs
Background
Every year, millions of individuals are forced to flee their homes around the globe, due to violence, war, and natural disasters, and others remain in displacement within their home countries.1 By the end of 2020, approximately 55 million individuals were reported to be living in internal displacement because of conflict and environmental hardships, and approximately 40.5 million new displacements were recorded in 2020 only. This surge in displacement was associated with conflict and natural disasters in 149 states.2
Approximately 2.6 million individuals are internally displaced in Somalia. Armed conflicts and environmental disasters affecting most parts of Somalia have caused several individuals to flee their homes.3 Most of the displacements recorded were into or within Mogadishu, which makes Mogadishu the second highest densely populated city in the world. It hosts more than 600,000 IDPs.4 Most of the displaced people came from neighboring regions: Middle and Lower Shabelle, Bay, and Bakool regions. These regions were the most affected areas of the 2011 famine, and they also experienced military offensives and clan-based conflicts.5
Internally displaced persons (IDPs) have numerous social vulnerabilities and are susceptible to mental disorders. These social vulnerabilities include poor shelter and overcrowding, lack of protection, reduced water access, food insecurity, limited access to health service, a lack of personal documentation, and the growing number of forced evictions.6
Somalia has been in turmoil and political instability for the last three decades. The country has experienced fierce conflicts between rival groups and frequent terrorist attacks since the collapse of Siad Barre’s regime in 1991.7 The World Health Organization reports that one-in-three people are affected by mental disorders, with individuals suffering from mental illnesses being subjected to stigma and social isolation. For such individuals, the burden of care is largely left to their caregivers.8
The prevalence of post-traumatic stress disorder (PTSD) and depressive disorder is frequently investigated in conflict settings, as psychological trauma is expected to be widely common among this population. A study on IDPs in Ukraine found the prevalence of PTSD to be 32%, whereas the prevalence of depression was 22%.9 In Colombia, a study found high levels of PTSD and depression in IDPs, 88% and 41%, respectively.10 Roberts11 found that (54%) of IDPs in northern Uganda, who witnessed 20 years of conflict between a rebel group (LRA) and the government’s army, had probable diagnoses of PTSD, and over two-thirds (67%) of respondents had diagnostic symptoms of depression. Among Somali refugees in Uganda, a study found the prevalence rate of PTSD to be 48%.12 Another study revealed that over one-third of Somali refugees (38.3%) in Melkadida camp in Ethiopia met the symptom criteria for depression.13 Generally, women are considered to be more likely to develop depression and PTSD than men. Moreover, Roberts11 showed a strong association between sex and PTSD. In that study, women were twice more likely than men to show symptoms of PTSD (OR = 2.01 [95% CI]) and depressive disorder (OR = 2.37 [95% CI]).14 Roberts et al14 indicated that this likelihood is due to the higher possibility of women being exposed to traumatic events, such as violent loss of partner and children, rape, and single parenthood or widowhood.
Lower educational level was significantly associated with PTSD and depression, whereas a higher educational level could be a protective factor for the development of PTSD.15 A study on the prevalence of PTSD among Syrian refugees in Turkey found that a family history of mental disorders is significantly associated with PTSD.16 A relationship was observed between PTSD and the frequency of trauma experienced. Another study on the mental health of IDPs in Sri Lanka found that a higher number of traumatic events increases the likelihood of developing PTSD and depression.17
There is a paucity of data on the burden of mental disorders among IDPs in Somalia. This study sought to determine the prevalence and associated factors of PTSD and depressive disorder among IDPs, and it is also meant to provide baseline data for future epidemiological studies on the mental health of vulnerable populations, including IDPs.
Methodology
Study Design and Participants
The study was conducted in Mogadishu, the capital and largest city of Somalia, which has a population of 2.5 million residents. A cross-sectional survey was conducted between January 1 to February 28, 2021. To determine the sample size, Kish formula18 was used. The minimum required sample size is 384. However, allowing for 10% attrition for non-response, the sample size was adjusted upwards to 422. Overall, 422 IDPs were approached and 401 consented to participate in the study. A multistage random sampling method was used. In the first stage, four districts were randomly selected from 17 administrative districts in Mogadishu (Boondheere, Hodan, Wadajir, and Dharkeynley). Approximately, 76 IDP camps were present in the four districts. These camps were proportionately sampled based on the estimated IDP population from the joint IDP Profiling report.19 In the next stage, due to restricted data and unsystematic layout of the camps, random and systematic sampling methods were not feasible. According to Collins,20 when limitations preventing the use of other methods for selecting households are present, a segmentation method can be used. A segment of the camp was randomly selected and all households within that segment were included until the required number was reached. All eligible individuals from selected households were included.
Ethical approval to conduct this study was obtained from Kenyatta National Hospital-University of Nairobi, Ethics and Research Committee (P120/03/2020). This study also complies with the declaration of Helsinki. Permission was sought from the local Benadir regional administration. Camp leaders were consulted, and their permission was obtained. Informed written consent was sought from respondents before each interview, and the process included an explanation of the purpose and nature of the study as well as an opportunity to ask any questions and seek clarification.
Upon arrival at the camp, camp leaders were approached and the nature of the study was explained.
Study respondents were recruited from households within a randomly selected section. Participants from each household were invited to participate, if they met the inclusion criteria. They provided consent after being briefed about the nature of the study.
Measures
The socio-demographic characteristics and displacement history of IDPs were collected using a researcher-designed questionnaire. Harvard Trauma Questionnaire (HTQ)21 was used to screen PTSD and identify exposure to trauma. HTQ was developed by the Harvard Program in Refugee Trauma, it is a cross-cultural screening tool that documents trauma exposure and trauma-related symptoms in IDPs and refugees. It contains four parts: I) Traumas that displaced people encounter frequently. II) Subjective description of most severe traumatic experience. III) Head injury. IV) Trauma symptoms in DSM V. Its latest edition HTQ-5 was modified to be consistent with current DSM-5 diagnostic criteria. It has been translated and adapted into several languages and cultures.22
Hopkins Symptom Checklist (HSCL-25) was used to screen for depression. This screening tool was developed by Parloff, Kelman, and Frank23 at Johns Hopkins University. HSCL-25 consists of 25 items. The first part of HSCL-25 includes 10 items assessing for anxiety symptoms, whereas the second part, which was used in this study, consists of 15 items assessing for depression symptoms. HSCL-25 contains a 4-point severity scale. It consistently correlates with major depression in the Diagnostic and Statistical Manual (DSM-IV).
The reliability and validity of the HTQ and HSCL-25 have been tested in several countries.24 HTQ and HSCL have Cronbach’s alpha of internal consistency of 0.92 and 0.85 with standard cut-off points of 2.5 and 1.75, respectively.21 In this study, both instruments were translated and adapted to the Somali language.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 24. Descriptive statistics were used to summarize the data, whereas analytical statistics were used to test for significant associations and predictors. Bivariate and multivariate analyses were performed to identify factors associated with the occurrence of depression and PTSD. In bivariate analysis, the chi-square test was used to determine statistically significant associations. Statistically significant variables (p < 0.05) and those at the margin of statistical significance (p < 0.07) were included in the logistic regression model. Adjusted odds ratios (AORs) were calculated with 95% confidence interval (CI).
Results
A total of 401 respondents, including 334 (83.3%) women, consented and participated in this study. Persons with ages of 26–35, 36–60, 18–25, and >60 years formed 37.6%, 32.0%, 23.6%, and 6.5% of the respondents, respectively. The majority of the respondents were married (69.1%), had no formal education (64.8%), and about (66.3%) were unemployed (Table 1). A total of 101 (25.3%) respondents reported a positive family history of mental illness, and 80.5% of respondents had been displaced more than once.
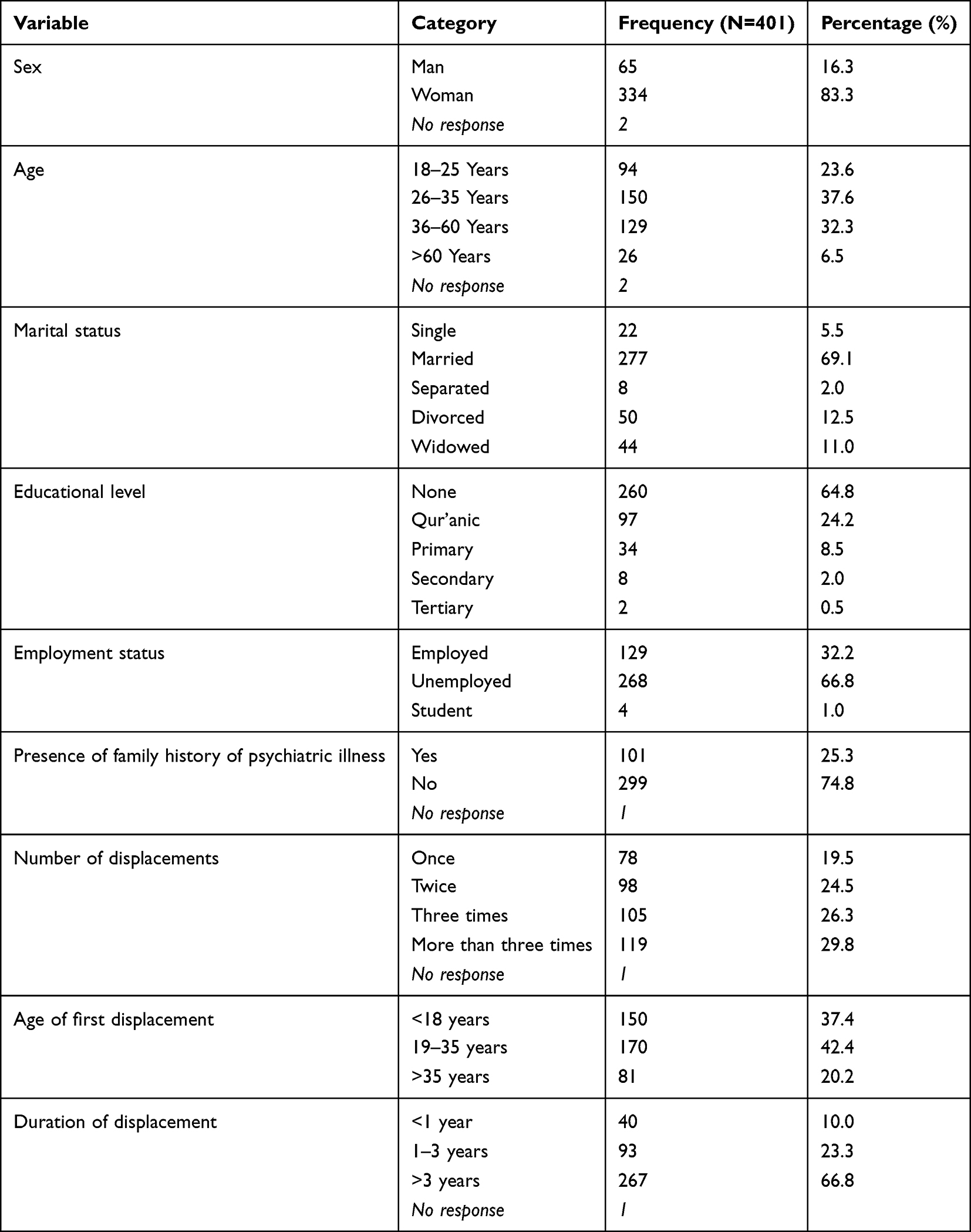 |
Table 1 Socio-Demographic Characteristics of the Respondents |
Prevalence of PTSD and Depression
A total of 129 (32.2%) participants screened positive for PTSD. In terms of depression, 238 (59.4%) participants screened positive for depression.
Frequency of Trauma Exposure
At least 26 participants reported all forms of traumatic experiences assessed. The most prevalent traumatic event was lack of food or water (80.2%), followed by ill health without access to medical care (79.9%), lack of shelter (77.9%), and combat situation (eg, shelling and grenade attacks) (55.5%). The frequency of trauma exposure is shown in Table 2.
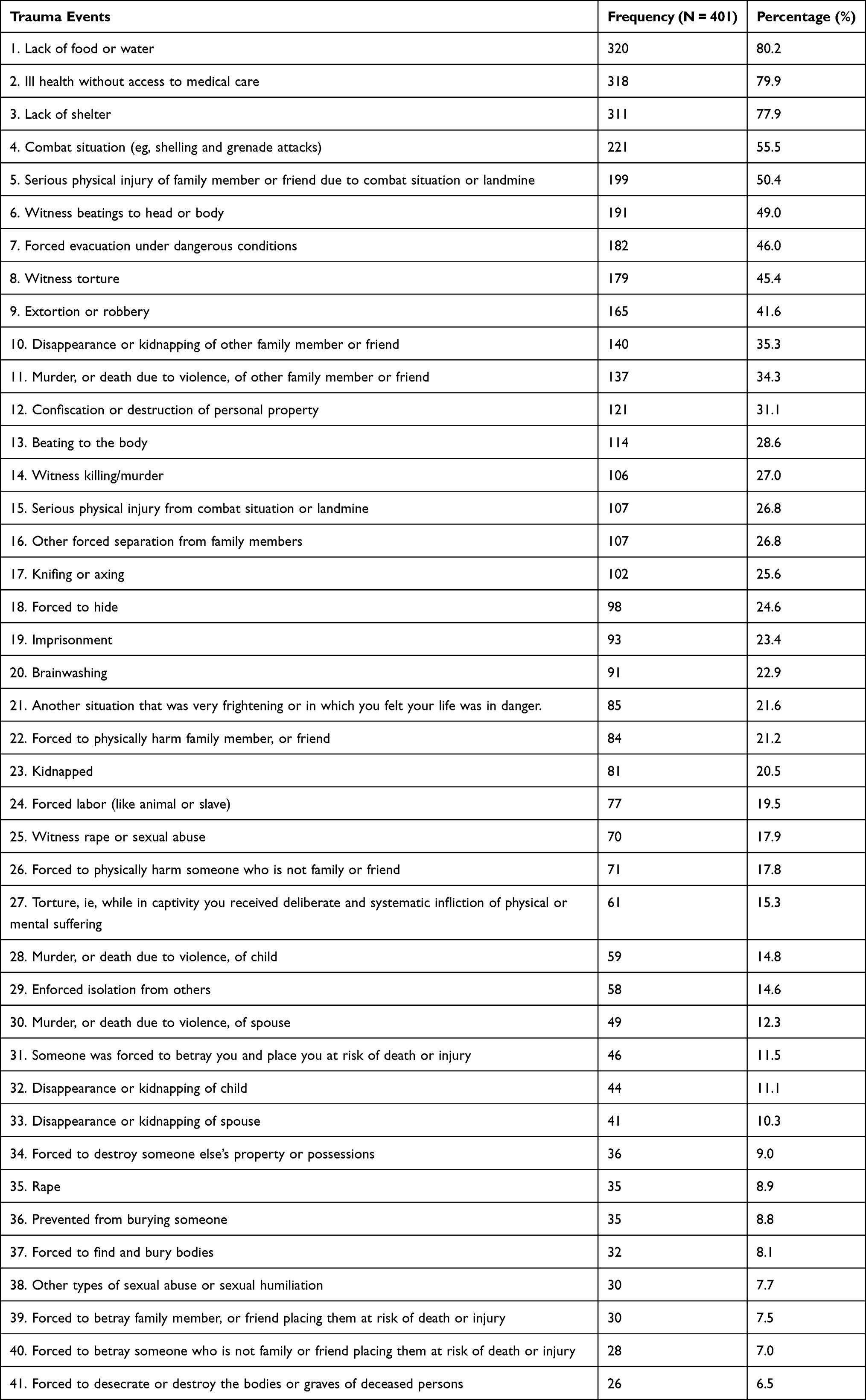 |
Table 2 Nature of Exposure to Traumatic Events |
Prevalence of Traumatic Events Recorded
A third of participants (33.2%) indicated that they had experienced 5–9 traumatic events, followed by 22.4%, 16.2%, 15.7%, and 12.5% of participants who reported experiencing 10–14, 15–19, 0–4, and ≥20 traumatic experiences, respectively.
Multivariable Analysis: Association Between Demographic Variables, Displacement Variables, and Number of Trauma Events and PTSD
Table 3 presents the adjusted odds ratio results of logistic regression analysis on the association between PTSD outcome and displacement, demographics, and trauma events (cut off ≥2.5). Participants who were unemployed were about twice more likely to be at risk of PTSD than those who were employed (aOR = 1.79; 95% CI = 1.06–3.04; p = 0.030). Respondents who had been displaced more than once were more likely to be at risk of PTSD than those who had been displaced once (aOR = 3.21; 95% CI = 1.35–7.63; p = 0.008); (aOR = 2.83; 95% CI = 1.20–6.67; p = 0.017); (aOR = 3.15; 95% CI = 1.35–7.33; p = 0.008) for those who had been displaced twice, three times, and more than three times, respectively. Participants who had been displaced when they were aged 19–35 years were 2.56 times more likely to be at risk of PTSD than those who were displaced when they were aged >35 years (aOR = 2.56; 95% CI = 1.31–5.01; p = 0.006). The number of traumatic events was significantly associated with the risk of PTSD. For every unit increase in traumatic event, the risk of being at risk of PTSD increased 1.1 times more (aOR = 1.09; 95% CI = 1.05–1.13; p < 0.001).
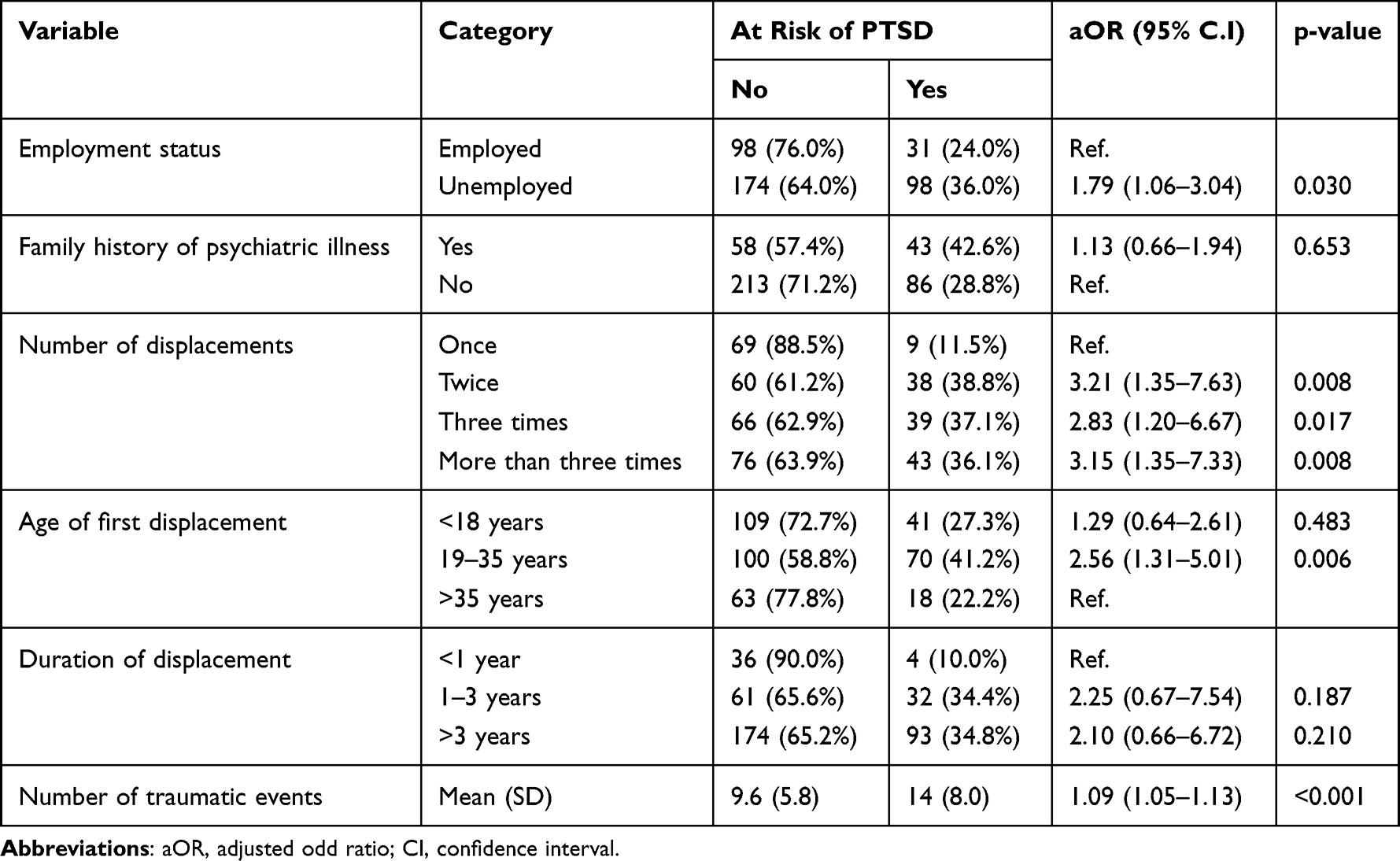 |
Table 3 Multivariate Analysis of Demographic Variables, Number of Trauma Events, and Displacement Variables Associated with PTSD |
Multivariable Analysis: Association Between Depression and Demographic Variables, Displacement Variables, and Cumulative of Trauma Events
Table 4 presents the adjusted odds ratio results of the multivariate logistic regression analysis on the association between depression outcomes and cumulative trauma exposure, demographics, and displacement variables (cut off ≥1.75). Participants who were unemployed were about twice more likely to be at risk of depression than those who were employed (aOR = 1.72; 95% CI = 1.07–2.77; p = 0.026). The risk of being depressed was 3.53 times (aOR = 3.53; 95% CI = 1.60–7.79; p = 0.002) and 3.29 times (aOR = 3.29; 95% CI = 1.36–7.97; p = 0.008) more among those who had experienced 15–19 and ≥20 traumatic events, respectively, than those who had experienced 0–4 traumatic events.
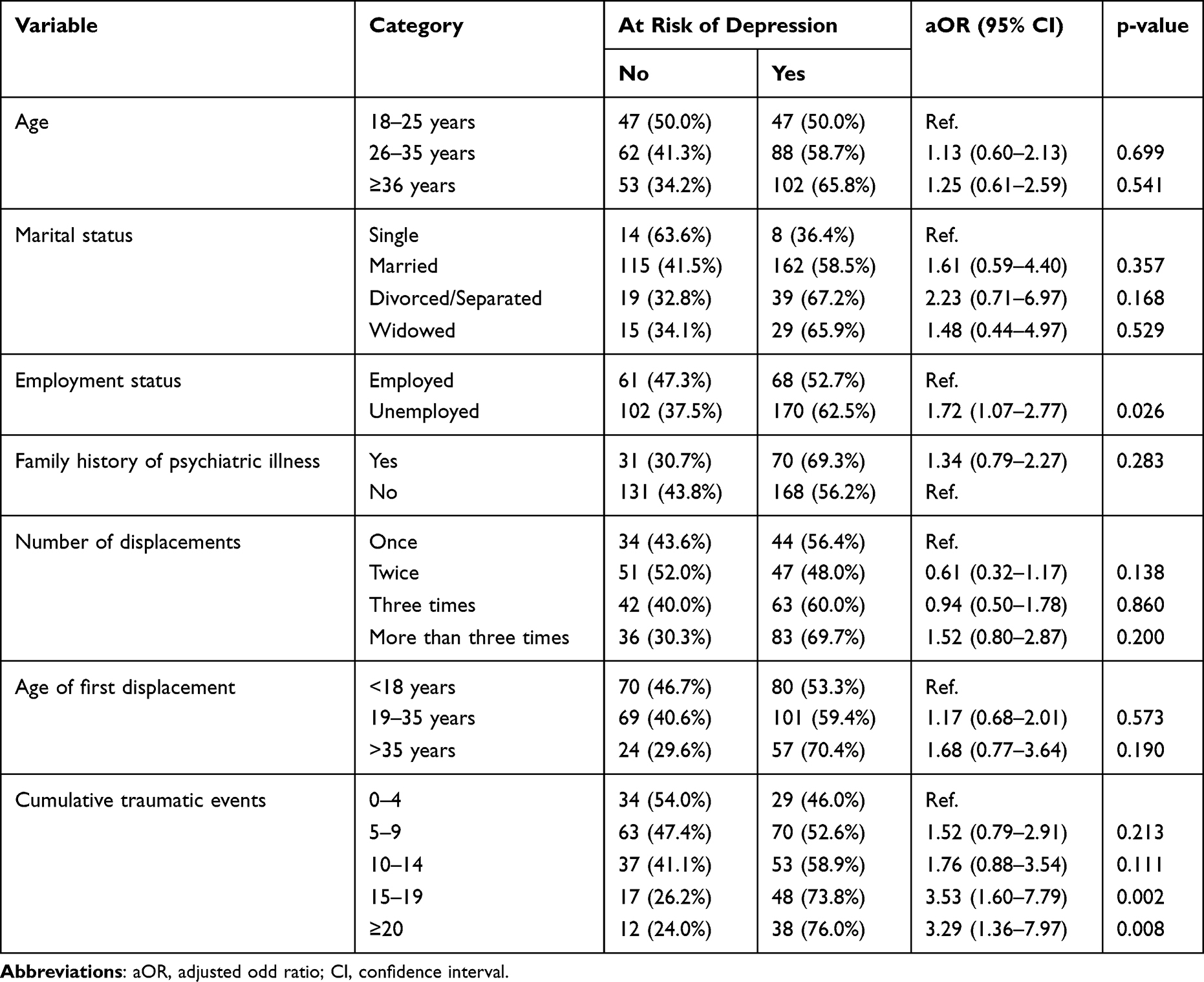 |
Table 4 Multivariate Analysis of Demographic Variables, Cumulative Trauma, and Displacement Variables Associated with Depression |
Discussion
This study revealed high levels of psychiatric disorders among the IDP population in Mogadishu. Approximately 32% of respondents met the symptom criteria for PTSD, and 59% of respondents met the symptom criteria of depression. Majority of the study participants were women (83.3%). Women and children usually represent a high proportion of residents in IDP camps at any given time. This finding is due to certain socioeconomic factors, including the far distances from home of men’s work and local conflict dynamics.25 The number of psychiatric disorders in this study was lower than that among IDPs in Uganda, where 54% and 67% of them had probable PTSD and depression, respectively.11 The rates of depression and PTSD in this study can be compared to those of a South Sudan study, which had rates of 36% and 50% for PTSD and depression, respectively.14 Additionally, the prevalence in this study was higher than those found in studies conducted in Georgia and Sri Lanka, which had prevalence rates of 23% and 14% for PTSD and 2.4% and 5% for depression, respectively.26,27 The discrepancy rates of war-related mental health conditions might be due to differences in study tools. In Georgia, the trauma screening questionnaire and the PHQ9 were used, whereas, in Sri Lanka and Uganda, the Composite International Diagnostic Interview (CIDI) and HTQ, respectively, were used. Furthermore, structured interviews, such as CIDI, yield lower levels of psychopathology than screening tools. Differences in sampling techniques are another factor that can lead to variability in psychiatric morbidities.28 The characteristics of individual communities and their culture can affect the occurrence of psychiatric morbidity, as what is considered trauma in one culture might not be perceived the same in another culture.29 The type and nature of exposed psycho-trauma could be another factor. Interpersonal violence trauma and intimate sexual violence carry the highest PTSD risk.30
In this study, unemployment was associated with depression and PTSD (aOR = 1.79; 95% CI = 1.06–3.04; p = 0.030). Unemployment has been found to be associated with poor mental health outcome in IDP settings due to scarcity of resources.27
Similar to findings from the study by Acarturk,31 respondents who had been displaced more than once were more likely to be at risk of PTSD than those who had been displaced once (aOR = 3.21; 95% CI = 1.35–7.63; p = 0.008). This finding may be related to the fact that respondents with multiple displacements were more likely to be exposed to trauma and violence than respondents who had been displaced once, probably increasing their risk to develop war-related psychiatric disorders.28 In this study, participants who had been displaced at the age of 19–35 years were 2.56 times more likely to be at risk of PTSD than those who were displaced at the age of >35 years (aOR = 2.56; 95% CI = 1.31–5.01; p = 0.006).
A dose–response relationship was observed between trauma exposure and psychiatric morbidity in this study, as the more one was exposed to traumatic events, the higher one was at risk of psychiatric disorders. The number of traumatic exposures was predictive for both mental health disorders (aOR = 1.09; 95% CI = 1.05–1.13; p < 0.001), (aOR = 3.53; 95% CI = 1.60–7.79; p = 0.002). This finding is consistent with those of other studies, which found significant correlations between poor mental health outcomes and cumulative trauma exposure.11,13,28,32,33
This study has a few limitations. First, due to the cross-sectional design used, recall bias was likely, and this also meant that its findings cannot be generalized across Somalia. In addition to that, this also prevented us from concluding the causal relationships of the associations we found. Secondly, precision might be lowered by the selected sampling method (multistage cluster sampling method). Thirdly, Women’s overrepresentation in the study may lead to gender bias. Finally, the study tools were not validated in the local context, although the tools were cross-cultural and specially developed for displaced people, with excellent internal consistency.
Conclusion
This study revealed a high prevalence of depressive disorders and PTSD among IDPs in Mogadishu. Furthermore, this study provided evidence of IDPs’ susceptibility to trauma exposure and, importantly, the lack of essential services and goods. The most prevalent traumatic events reported were lack of food or water, ill health without access to medical care, lack of shelter, and combat situation (eg, shelling and grenade attacks). Important predictive factors for the development of psychiatric morbidity were unemployment, cumulative traumatic exposure, and frequency and duration of displacement.
Recommendations
We recommend that, first, screening and necessary interventions should be provided for IDPs suffering from PTSD and depression. Additionally, a referral system for psychiatric disorders should be established. Second, governmental and nongovernmental agencies working on the welfare of IDPs should provide an inclusive social support and protection agenda to alleviate psychosocial distress and prevent further exposure to postmigration trauma within the camp.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNHCR. Handbook for the protection of internally displaced persons; 2010. Available from: https://www.unhcr.org/4c2355229.pdf.
2. Internal Displacement Monitoring Centre. Internal displacement in a changing climate; 2022. Available from: https://www.internal-displacement.org/sites/default/files/publications/documents/grid2021_idmc.pdf.
3. United Nations Office for the Coordination of Humanitarian Affairs. Somali humanitarian needs overview; 2018. Available from: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/20172911_somalia_humanitarian_needs_overview_2018.pdf.
4. IDMC. UnSettlement: Urban Displacement in the 21st Century Thematic Series City of Flight New and Secondary Displacements in Mogadishu, Somalia. IDMC; 2018.
5. UNHCR. Internal displacement profiling in Mogadishu; 2016. Available from: https://reliefweb.int/report/somalia/internal-displacement-profiling-mogadishu-april-2016.
6. OCHA. Somalia humanitarian fund annual report 2018; 2018. Available from: https://www.unocha.org/sites/unocha/files/Somalia%20HF%20Annual%20report%202018.pdf.
7. Donner S, Schwarz R. BTI 2018 Country report. 2018.
8. World Health Organization. A situation analysis of mental health in Somalia. Available from: https://reliefweb.int/report/somalia/situation-analysis-mental-health-somalia.
9. Roberts B, Makhashvili N, Javakhishvili J, et al. Mental health care utilisation among internally displaced persons in Ukraine: results from a nation-wide survey. LSHTM Res Online. 2017;1–12. doi:10.1017/S2045796017000385
10. Richards A, Ospina-duque J, Barrera-valencia M, et al. Posttraumatic stress disorder, anxiety and depression symptoms, and psychosocial treatment needs in Colombians internally displaced by armed conflict: a mixed-method evaluation. Psychol Trauma. 2011;3(4):384–393. DOI:10.1037/a0022257
11. Roberts B, Ocaka KF, Browne J, Oyok T, Sondorp E. Factors associated with post-traumatic stress disorder and depression amongst internally displaced persons in northern Uganda. BMC Psychiatry. 2008;8:1–9. doi:10.1186/1471-244X-8-38
12. Onyut LP, Neuner F, Ertl V, Schauer E, Odenwald M, Elbert T. Trauma, poverty and mental health among Somali and Rwandese refugees living in an African refugee settlement – an epidemiological study. Confl Health. 2009;3(1):1–16. doi:10.1186/1752-1505-3-6
13. Feyera F, Mihretie G, Bedaso A, Gedle D, Kumera G. Prociated factors among Somali refugee at melkadida camp, southeast Ethiopia: a cross-sectional study evalence of depression and ass. BMC Psychiatry. 2015;15(1):1–7. doi:10.1186/s12888-015-0539-1
14. Roberts B, Damundu EY, Lomoro O, Sondorp E. Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC Psychiatry. 2009;9:1–10. doi:10.1186/1471-244X-9-7
15. Housen T, Lenglet A, Ariti C, et al. Prevalence of anxiety, depression and post-traumatic stress disorder in the Kashmir Valley. BMJ Glob Health. 2017;2(4):e000419. doi:10.1136/bmjgh-2017-000419
16. Alpak G, Unal A, Bulbul F, et al. Post-traumatic stress disorder among Syrian refugees in Turkey: a cross-sectional study. Int J Psychiatry Clin Pract. 2015;19(1):45–50. doi:10.3109/13651501.2014.961930
17. Husain F, Anderson M, Becknell K, Blanton C, Araki D. Prevalence of war-related mental health in Postwar Jaffna District, Sri Lanka. JAMA. 2011;306(5):522–531.
18. Kish L. Survey Sampling. John Wiley & Sons Inc; 1965.
19. Joint IDP Profiling Service. Internal displacement profiling in Mogadishu report. 2016.
20. Collins G. Thematic guidelines: sampling guidelines for vulnerability analysis. 2004.
21. Mollica RF. The Harvard Trauma Questionnaire: validation a cross-cultural instrument for measuring torture, trauma, and post traumatic stress disorder in refugees. 1992.
22. Berthold SM, Mollica RF, Silove D, Tay AK, Lavelle J. The HTQ-5: revision of the Harvard Trauma Questionnaire for measuring torture, trauma and DSM-5 PTSD symptoms in refugee populations. Eur J Public Health. 2018;1–7. doi:10.1093/eurpub/cky256
23. Parloff MB, Kelman HC, Frank JD. Comfort, effectiveness, and self-awareness as criteria of improvement in psychotherapy. Am J Psychiatr. 1954;111:343–352. doi:10.1176/ajp.111.5.343
24. Oruc L, Kapetanovic A, Pojskic N, et al. International Journal of Culture and Screening for PTSD and depression in Bosnia and Herzegovina: validating the Harvard Trauma Questionnaire and the Hopkins Symptom Checklist. Int J Culture Mental Health. 2009:37–41. doi:10.1080/17542860802456620
25. Internal Displacement Monitoring Centre. Global report on internal displacement; 2020. Available from: https://www.internal-displacement.org/global-report/grid2020/.
26. Makhashvili N, Chikovani I, Mckee M, Bisson J, Patel V, Roberts B. Mental disorders and their association with disability among internally displaced persons and returnees in Georgia. J Trauma Stress. 2014;509–518. doi:10.1002/jts
27. Siriwardhana C, Adikari A, Pannala G, et al. Prolonged internal displacement and common mental disorders in Sri Lanka: the COMRAID study. PLoS One. 2013;8(5):e64742. doi:10.1371/journal.pone.0064742
28. Madoro D, Habtamu K, Habtamu Y, et al. Post-traumatic stress disorder and associated factors among internally displaced people in South Ethiopia: a cross-sectional study. Neuropsychiatr Dis Treat. 2020;Volume 16:2317–2326. doi:10.2147/NDT.S267307
29. Herbert J, Forman E. Cross-cultural perspectives on posttraumatic stress. In: Rosen G, Frueh B, editors. Clinician’s Guide to Posttraumatic Stress Disorder. Wiley; 2010:235–261.
30. Kessler RC, Aguilar-Gaxiola S, Alonso J, et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur J Psychotraumatol. 2017;8. doi:10.1080/20008198.2017.1353383
31. Acarturk C, Cetinkaya M, Senay I, Gulen B, Aker T, Hinton D. Prevalence and predictors of posttraumatic stress and depression symptoms among Syrian refugees in a refugee camp. J Nervous Mental Dis. 2017;1–6. doi:10.1097/NMD.0000000000000693
32. Essizoglu A, Keser I. Post-traumatic stress disorder in internally displaced people subjected to displacement by armed forces. J Trauma Stress Disord Treat Res. 2014. doi:10.4172/2324-8947.1000122
33. Mahmood HN, Ibrahim H, Goessmann K, Ismail AA, Neuner F. Post-Traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Confl Health. 2019;13(1):1–11. doi:10.1186/s13031-019-0238-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.