")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Prevalence of Obstructive Sleep Apnea Among Atrial Fibrillation Patients: A Cross-Sectional Study from Jordan
Authors Ibdah RK , Zaitoun KJ, Altawalbeh RB, Tayyem SH, Nazzal UA, Rawashdeh SI , Khader YS , Al-Mistarehi AHW , Khassawneh BY
Received 30 November 2023
Accepted for publication 1 February 2024
Published 14 February 2024 Volume 2024:17 Pages 701—710
DOI https://doi.org/10.2147/JMDH.S452589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rasheed K Ibdah,1 Khaled J Zaitoun,2 Rana B Altawalbeh,2 Saad H Tayyem,2 Ulla A Nazzal,2 Sukaina I Rawashdeh,1 Yousef S Khader,3 Abdel-Hameed W Al-Mistarehi,4 Basheer Y Khassawneh5
1Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 3Department of Community Medicine, Public Health and Family Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 4School of Medicine, Johns Hopkins Hospital, Baltimore, MD, 21287, USA; 5Department of Internal Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan
Correspondence: Khaled J Zaitoun, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan, Tel +962798652961, Email [email protected]
Background: Obstructive Sleep Apnea (OSA) is a common respiratory disorder that causes intermittent upper airway collapse during sleep and can lead to various acute cardiovascular complications. Atrial Fibrillation (AF) is the most common sustained cardiac arrhythmia and is associated with an increased risk of cardiovascular hospitalization and all-cause mortality. Our study aimed to investigate the prevalence of individuals with AF and those considered at high risk for OSA.
Methods: A cross-sectional study was conducted with a population comprising patients who had visited KAUH cardiology clinics between 2017– 2019; subjects were categorized into AF patients and general cardiology patients. Patients were surveyed for OSA using the Berlin Questionnaire to assess the degree of OSA symptoms and to classify patients into high- or low-risk groups based on their responses.
Results: Of the 656 patients, 545 met our inclusion criteria, of whom 192 were diagnosed with AF. Comparable demographic characteristics were observed between the AF and non-AF groups, barring higher rates of obesity (p=0.001) and smoking (p=0.042) in the AF group. The prevalence of high-risk OSA was significantly higher in AF patients (68.2%) compared to non-AF patients (29.4%), with an adjusted odds ratio of 2.473 times (95% CI: 1.434 − 4.266, p=0.001) greater for AF. The age, gender, and BMI categories did not differ significantly between the two groups. Binary logistic regression revealed significant associations between OSA and risk factors such as asthma (OR=4.408, 95% CI: 2.634– 7.376, p=0.001).
Conclusion: These results serve to display a statistically significant increase in high-risk OSA in existing AF patients, irrespective of the presence of conventional OSA risk factors; this could imply a more immediate and direct relationship between both diseases and calls to include routine screening for OSA in patients diagnosed, newly or otherwise, with AF.
Keywords: Berlin questionnaire, polysomnography, cross sectional study
Introduction
Obstructive sleep apnea (OSA) is a common respiratory disorder with an estimated one billion people affected worldwide,1 manifesting as repetitive episodes of complete or partial collapse of the upper airways during sleep, thus resulting in hypoxemia, hypercapnia, swings in intrathoracic pressure, and heightened sympathetic activity.2,3 These factors can lead to a myriad of acute cardiovascular consequences.4 Atrial Fibrillation (AF) is the most common type of clinically significant cardiac arrhythmia5 and is associated with an increased risk of cardiovascular hospitalization and all-cause mortality, especially in women.6
Atrial Fibrillation (AF) is the most common type of clinically significant cardiac arrhythmia5 and is associated with an increased risk of cardiovascular hospitalization and all-cause mortality, especially in women.6
The relationship between OSA and AF has been well established, with OSA having an incidence rate of 82–88% in patients with AF, which is linked to numerous major factors, including advancing age, being male, and being overweight.7–9 Although the pathophysiology of this disorder is mostly speculative, according to Goudis et al, it might involve “…apnea-induced hypoxia, intrathoracic pressure shifts, sympathovagal imbalance, atrial remodeling, oxidative stress, inflammation, and neurohumoral activation…”, with evidence supporting screening and treatment of OSA in newly diagnosed AF cases.10 Todd et al speculated that due to the dynamic interactions between both diseases, the relationship might be underestimated in individuals aged <65 as more prominent risk factors for AF like hypertension begin to overshadow the effects of OSA. Larger studies are needed to confirm this association and control for confounding factors.11–13
OSA is a commonly overlooked medical condition that often goes untreated unless patients experience discomfort.14 However, it has been established that OSA can predict the probability of relapse in patients with AF.15,16 Many studies have shown that treating OSA can improve the success rates of AF treatments, such as cardiac ablation therapy and electrical cardioversion.17 Moreover, patients who underwent treatment for OSA had a lower rate of arrhythmia recurrence and significantly better procedural outcomes when undergoing cardiac ablation therapy.18 Additionally, treating OSA can lead to overall improvement in well-being and quality of life.19 Therefore, healthcare providers, including non-medical professionals, should consider incorporating OSA management strategies in the screening process. Kawakami et al suggested the use of a portable monitor as a simple tool for managing and treating AF.20
Our study aims to add to the current body of knowledge, being the first of its kind to be done in Jordan and among a limited number of studies in the Middle Eastern region, by investigating the association between individuals with AF and those considered at high risk for OSA using the validated Berlin questionnaire.21 We used local data to justify and highlight the importance of implementing suitable treatment and management strategies for OSA in patients with AF in Jordan. Moreover, we aimed to investigate the impact of OSA severity on these patients and determine whether further studies could provide more information on this relationship. Through our research, we hope to call attention to the importance of proper screening tests for these patients to potentially reduce the risk of complications associated with AF, such as blood clots that may lead to stroke. This is especially crucial given the chaotic heart rhythm in AF episodes, which can increase mortality rates in patients with AF,22 and given our observing of frequent undiagnosed OSA in patients with AF. As noted by Petryszyn et al, the way the screening process is structured may be more critical than the specific technical methods used to evaluate heart rhythm.23
Methods
Study Design
A cross-sectional study was conducted, with the population comprising patients who had visited King Abdullah University Hospital cardiology clinics within the period of (2017–2019); The timing of their ECG, confirming their AF diagnosis, and the completion of the Berlin Questionnaire to assess the risk of OSA were concurrent within this time. Our focus was on the prevalence of high-risk OSA among these patients at the time of their clinical presentation for AF, rather than on a longitudinal or sequential assessment. Patients were categorized into cases (diagnosed with AF) and non-cases (without a previous history of AF). Male and female patients aged > 21 years were included in this study. Patients who were unwilling to complete the questionnaires and/or those with mental illness were excluded. Patients self-administered the Berlin Questionnaire to assess the degree of symptoms, eliminating the use of face-to-face interviews or phone surveys.
In our research, we propose utilizing the Berlin Questionnaire to identify individuals at risk for OSA and classify them according to their level of risk. This tool will provide valuable information for our study and help us better understand the prevalence and risk factors associated with OSA.
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study was approved by the Medical Research Ethical Committee and the Institutional Review Board (IRB) of Jordan University of Science and Technology (JUST) (IRB no. 22/130/2020). Written informed consent was obtained from all participants.
Validation of the Berlin Questionnaire
The Berlin Questionnaire is a patient survey that has been validated21 for identifying individuals at risk for OSA and has been shown to boost high sensitivity and negative predictive value in cases of severe OSA, emboldening its validity as an accessible and easy-to-use confirmatory screening test.24 The questionnaire aims to identify high- and low-risk individuals with OSA by assessing three risk factors: snoring behavior, daytime sleepiness or fatigue, and a history of obesity and/or hypertension. A patient is considered at high risk if they have a positive score in two or more categories; conversely, a patient is considered at low risk if they have a positive score in only one or no categories. It is a self-administered and easy-to-use tool that has been shown to be effective in predicting OSA risk.
Statistical Analysis
All data analyses were performed using SPSS Statistics 26.0. Normality assumptions were assessed through graphical methods (histograms and Q-Q plots) and formal statistical tests (Kolmogorov–Smirnov and Shapiro–Wilk tests). Despite the large sample size (N = 545), none of the continuous variables exhibited a clear normal distribution based on these assessments. As a result, non-parametric tests, such as the Mann–Whitney U-test were employed for subsequent analyses, while categorical variables were presented as numbers (percentages) and analyzed using the chi-squared test. For patients’ demographic characteristics, continuous variables were summarized using both mean ± standard deviation and median (with interquartile ranges) to provide a comprehensive description of their distribution.
Logistic regression in univariate and multivariate models was used to determine factors associated with OSA. Variables with a P value<0.05 in univariate logistic regression were a candidate and included in multivariate logistic regression. In multivariate logistic regression using the forward stepwise approach variables having a P value<0.05 was considered statistically significant. Odds ratios (ORs) and their 95% confidence intervals (CIs) were reported for each variable.
Sample Size Calculation
At a level of confidence of 95%, level of significance of 0.05, and assuming that 50% of the study population is at risk of sleep apnea, the sample size needed to estimate the prevalence within a margin error of 10% was calculated at 190 patients, Sample size was calculated using G*power (ver. 3.1.9) software.
Results
Study Population Characteristics
After applying the inclusion and exclusion criteria, 545 patients out of the initial 686 were included in the analysis. The participant selection process is depicted in the flow chart (Figure 1), with 192 (35%) of them being diagnosed with AF. (Table 1) summarizes the demographic characteristics of the study population, revealing comparable age, sex, and body mass index (BMI) distributions between the AF and non-AF groups. Notably, the prevalence of obesity, defined as BMI ≥30 kg/m2, was significantly higher among patients with AF (54.2%) than among patients without AF (38%) (p=0.001), indicating a higher obesity rate among individuals with AF. Furthermore, a significantly higher prevalence of smoking was observed in the AF group (40.1%) than in the non-AF group (31.4%) (p=0.042).
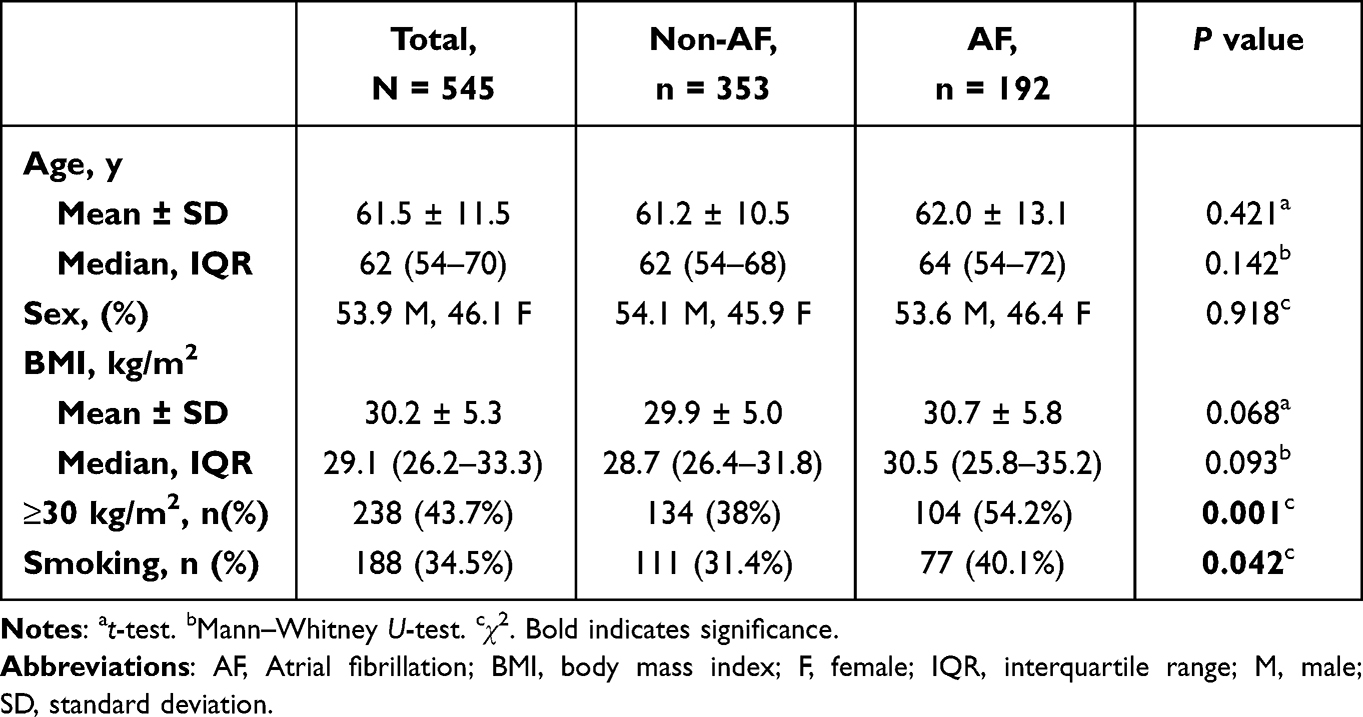 |
Table 1 Patients Demographics Characteristics |
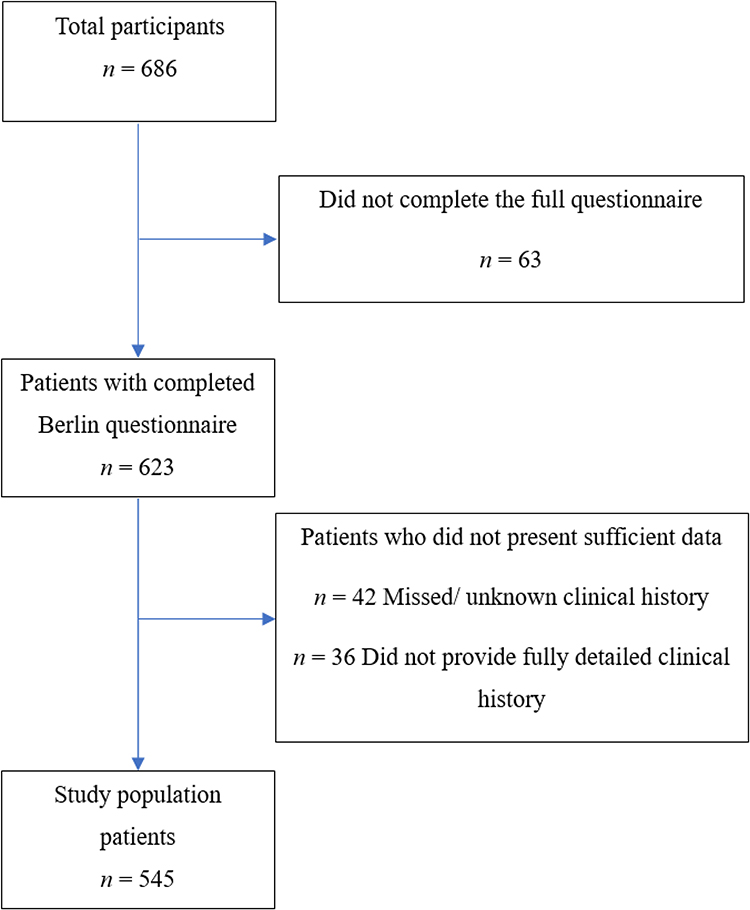 |
Figure 1 Participant selection flowchart. |
The Prevalence of OSA
The prevalence of high-risk OSA was compared between patients with and without AF. Among 192 patients with AF, 131 (68.2%) were classified as having a high risk for OSA. Among the 353 patients without AF, 104 (29.4%) were classified as having a high risk for OSA.
The prevalence of smoking was significantly different between the non-AF and AF groups (p = 0.028), indicating a higher prevalence of smoking among patients with AF. In the non-AF group, 36 (34.6%) patients were smokers, whereas 64 (48.9%) were smokers in the AF group (Table 2).
 |
Table 2 The Prevalence of High-Risk OSA in Total Study Population |
There were no significant differences observed between the non-AF and AF groups in terms of the prevalence of high-risk OSA based on age (p = 0.832), gender (p = 0.539), and BMI categories (p = 0.453). Among patients aged 21–50 years, 11.1% were at high risk for OSA, with similar proportions in both groups. For patients over 50 years of age, the prevalence of high-risk OSA was approximately 89%. Gender distribution was also comparable between the non-AF and AF groups. Furthermore, BMI categories did not differ significantly between the two groups, with approximately one-third having a BMI in the range of (18.5–29.99) and two-thirds having a BMI of 30 or higher.
Risk Factors Associated with Obstructive Sleep Apnea: Results of Binary Logistic Regression Analysis
We examined the association between several risk factors and OSA and we found that thirteen (13) factors were found to be significantly associated with higher odds of having OSA: AF, age, BMI (kg/m2), male gender, smoking, hypertension, diabetes mellitus, dyslipidemia, stroke, heart failure, COPD (Chronic Obstructive Pulmonary Disease), and asthma (Table 3).
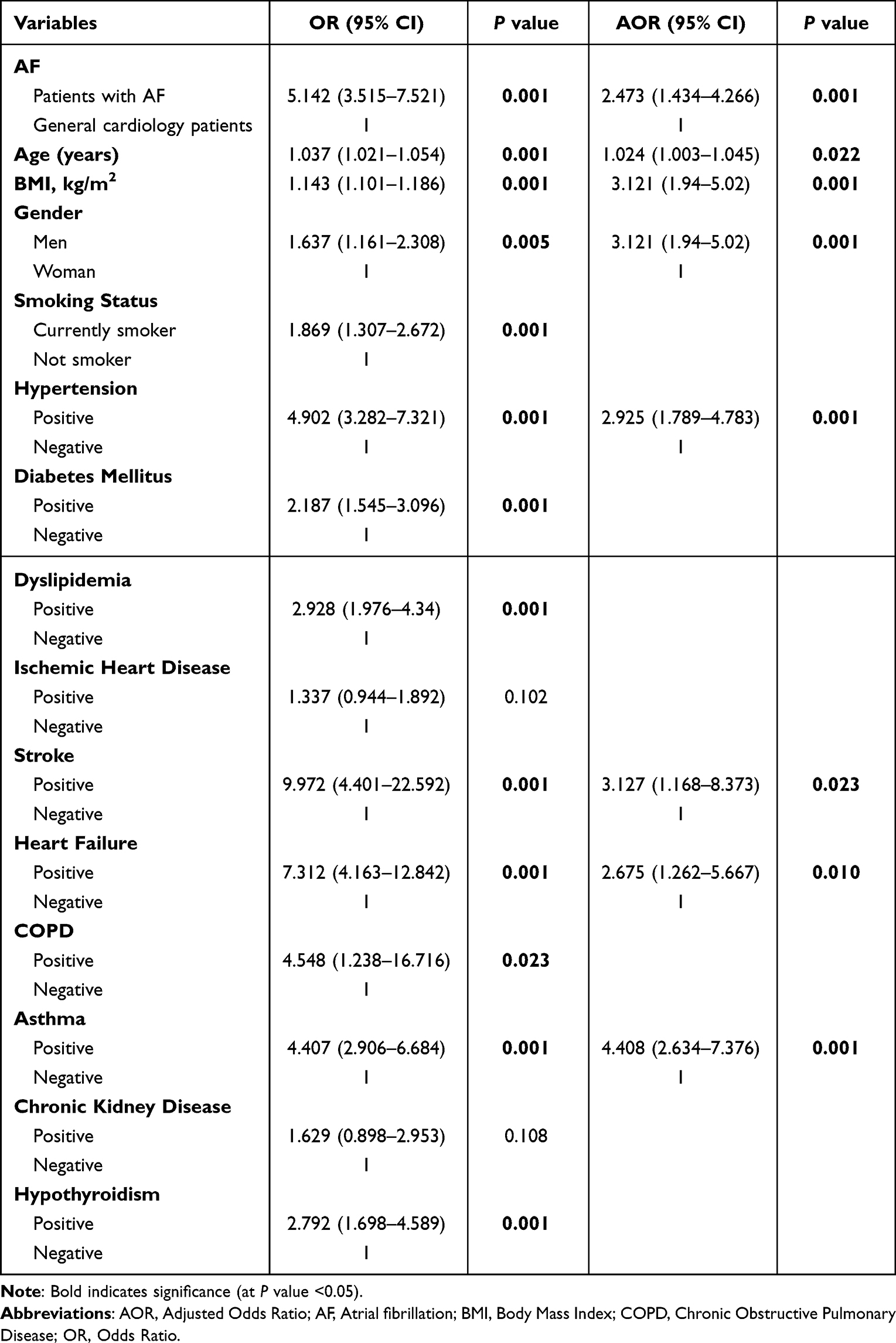 |
Table 3 Results of Binary Logistic Regression for Risk Factors of OSA in Study Population Patients |
These variables were candidates for multivariable logistic regression using a forward stepwise approach, and eight factors were found to be significantly associated with higher odds of having OSA. Notably, the Odds of OSA were 2.473 times (95% CI: 1.434 −4.266, p=0.001) greater for those with AF, asthma demonstrated the highest adjusted odds ratio (AOR) of 4.408 (95% CI: 2.634–7.376, p=0.001). Conversely, age showed the lowest AOR of 1.024 (95% CI:1.003–1.045; p=0.022) (Table 3).
Discussion
Summary
The goal of this study aimed to investigate and examine the prevalence of OSA among patients with AF in Jordan. These results, consistent with those of previously conducted studies, indicate a robust connection between the two conditions: AF patients have a higher risk of developing OSA compared to non-AF patients regardless of other factors such as obesity, smoking, and hypertension; intricate and intertwined pathophysiological interactions have been suggested as possible explanations.25 Despite this, most patients with AF and OSA have not been previously diagnosed with any sleep disorders. This highlights the need for proper screening for sleep disorders and other associated illnesses in all patients with AF, newly diagnosed or otherwise. Our findings provide further insight into how the severity of OSA symptoms is directly associated with an increased risk of developing AF.26
Interpretation
Based on our findings, along with existing literature, we see that AF patients are more likely to be diagnosed with OSA, and this might be attributed to shared risk factors between AF and OSA, including obesity, being male, older age, and smoking. Additionally, many medical conditions might play a role in exacerbating existing OSA symptoms, such as diabetes mellitus type 2, hypertension, congestive heart failure, hormonal abnormalities, and chronic lung diseases such as asthma.27 Nevertheless, if we inspect this association from a different perspective, we will find that OSA may be associated with the initiation and maintenance of AF.28
This is thought to be due to adverse structural and electrical changes in the myocardium resulting from hypoxemia and intrathoracic pressure swings. OSA is manifested by intermittent episodes of respiratory arrest, which present as intermittent hypoxemia that subsequently induces a sympathetic surge and chemoreflex triggering, leading to tachycardia and oxidative stress. Recurrent episodes of tachycardia concurrent with a fast heart rate can increase heart demand, leading to the development of AF. Likewise, oxidative stress resulting from OSA can negatively affect the heart’s ability to handle calcium, leading to changes in heart cells and increasing the likelihood of arrhythmias. Furthermore, OSA can cause sudden changes in pressure within the chest, which can stretch the atria of the heart, leading to their enlargement and making them more prone to AF10,29–32. Additionally, our findings of an evident association between AF and OSA in our patients could imply that AF might act as a predisposing factor for developing OSA, due to the interplay and indirect respiratory effects arising from the cardiac arrhythmia present in patients with AF.33
The observed findings revealed a correlation between high-risk OSA patients and certain factors including age, male gender, smoking, hypertension, dyslipidemia, hypothyroidism, and other comorbidities. This indicates that there are risk factors that can increase the incidence of OSA and the risk of AF correspondingly. Emerging evidence suggests that patients with severe untreated OSA have a higher rate of developing cardiovascular events34 and secondary hypertension, mainly due to fluctuating surges in systolic and diastolic blood pressure at night, accompanied by OSA episodes.35 As the incidence increases significantly with age, men are two to three times more prone to developing OSA than women; however, the incidence can be higher in females if they are overweight or after menopause.36 Despite conflicting evidence regarding the association between OSA and smoking, it is mostly thought to be due to the inflammatory effect and fluid retention caused by smoke inhalation, which aids in the narrowing and collapse of the upper airway alongside the effect of nicotine in the relaxation of the upper airway muscles and neural reflexes.37 Patients with asthma are more likely to develop OSA due to airway obstruction and remodeling; therefore, treating asthma is considered a priority to avoid exacerbated OSA.38 OSA and dyslipidemia have an indirect relationship; OSA induces persistent intermittent hypoxia events, which increase oxidative stress and sympathetic activity, resulting in increased lipoprotein and lipid peroxidation, and eventually, dyslipidemia.39
Apart from the associations, a few points are worthy of discussion regarding the demographic characteristics of the study population. Some factors were found to be associated with significantly higher rates of AF occurrence, namely, BMI (≥30 kg/m2) and smoking status; this follows an expected trend proven by many research articles highlighting the relationship between these factors and AF risk. Obesity has been established as an independent potentially modifiable risk factor for the development of AF,40,41 likely to be explained, according to Vyas and Lambiase, by a host of hemodynamic alterations influencing the size, histology, and speed of conduction, as well as inflammation and fibrosis produced by increasing epicardial adipose tissue.42 The relationship between smoking and AF has also been well established,43 with Chamberlain et al recording a staggering two-fold increase in the risk of AF directly attributed to smoking,44 and Albertsen et al observing a strong association between smoking and an increased risk of thromboembolism and mortality in patients with AF.45
Implications
Our results build on existing evidence surrounding the relationship between OSA and AF, albeit from a different point of view: looking at the prevalence of OSA in AF patients provides additional integrity to the existing relationship, and more importantly, highlights the value of screening tests for AF patients given the high degree of association between both diseases and the possible treatment approaches to be taken for the treatment of newly diagnosed OSA in patients with AF, such as Continuous Positive Airway Pressure (CPAP) therapy; such measures taken can decrease the burden of OSA in AF patients and possibly lead to an overall better prognosis.
Limitations
The presence of OSA was solely determined using the Berlin questionnaire, as we were unable to perform follow-up overnight sleep studies for further confirmation of the diagnoses. Although polysomnography is considered the gold standard test to confirm the diagnosis of OSA, it is thought to be time-consuming, complex, and expensive.46 Nevertheless, we consider our inability to perform PSG for diagnosis a limitation of this study.
Recommendations
Several previous studies have indicated the significance of treating OSA in patients with heart disease, particularly arrhythmias.47,48 Taking into consideration the large increase in OSA cases in cardiology clinics,49 it is necessary to consider merging the screening and diagnosing processes of OSA as a routine basis for treating arrhythmias. Positive results revealed an improvement in patients’ response to AF therapies, whether pharmacological or procedures such as cardiac ablation, when treating OSA first, regardless of other risk factors. Furthermore, this might help reduce and better control the symptoms of AF.50,51 Despite this, more evidence is needed on how management strategies and screening processes can be incorporated. Such studies might provide specialists with valuable insights into how to build targeted and individualized treatment approaches for both patients with OSA and AF.
Abbreviations
AOR, Adjusted Odds Ratio; AF, Atrial Fibrillation; BMI, Body Mass Index; CI, Confidence Intervals; CPAP, Continuous Positive Airway Pressure; F, Female; IRB, Institutional Review Board; IQR, Interquartile Range; M, Male; OSA, Obstructive Sleep Apnea; OR, Odds Ratio; PSG, Polysomnography; SD, Standard Deviation.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
All procedures performed in this study involving human participants were reviewed and ethically approved by the Institutional Review Board (IRB) at Jordan University of Science and Technology (JUST), Irbid, Jordan (IRB number: 22/130/2020). This study was conducted following the 1975 Helsinki Declaration, as revised in 2008, and later amendments or comparable ethical standards. The patients’ information was kept confidential, and the data analysis was conducted on the de-identified database.
Informed Consent
Written informed consent was obtained from all participants.
Funding
This research did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests. No writing assistance was aided in the preparation of the manuscript.
References
1. Sleep Apnea: More Common (And Serious) Than You May Think. Houston Methodist On Health. Available from: https://www.houstonmethodist.org/blog/articles/2019/oct/sleep-apnea-more-common-than-you-think/.
2. Ryan S. Mechanisms of cardiovascular disease in obstructive sleep apnoea. J Thorac Dis. 2018;10(Suppl 34):S4201. doi:10.21037/JTD.2018.08.56
3. Slowik JM, Sankari A, Collen JF Obstructive sleep apnea. StatPearls [Internet]; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459252/.
4. Fauska C, Bastiampillai T, Adams RJ, Wittert G, Eckert DJ, Loffler KA. Effects of the antipsychotic quetiapine on sleep and breathing: a review of clinical findings and potential mechanisms. J Sleep Res. 2023. doi:10.1111/JSR.14051
5. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors In Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370–2375. doi:10.1001/JAMA.285.18.2370
6. Stewart S, Hart CL, Hole DJ, McMurray JJV. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113(5):359–364. doi:10.1016/S0002-9343(02)01236-6
7. Xu Z, Wu Y, Tai J, et al. Risk factors of obstructive sleep apnea syndrome in children. J Otolaryngol Head Neck Surg. 2020;49(1):1–7. doi:10.1186/S40463-020-0404-1/TABLES/3
8. Moula AI, Parrini I, Tetta C, et al. Obstructive sleep apnea and atrial fibrillation. J Clin Med. 2022;11(5):1242. doi:10.3390/JCM11051242
9. Abumuamar AM, Dorian P, Newman D, Shapiro CM. The prevalence of obstructive sleep apnea in patients with atrial fibrillation. Clin Cardiol. 2018;41(5):601–607. doi:10.1002/clc.22933
10. Goudis CA, Ketikoglou DG. Obstructive sleep and atrial fibrillation: pathophysiological mechanisms and therapeutic implications. Int J Cardiol. 2017;230:293–300. doi:10.1016/j.ijcard.2016.12.120
11. Todd K, Mcintyre WF, Baranchuk A. Obstructive sleep apnea and atrial fibrillation. Nat Sci Sleep. 2010;2:39. doi:10.2147/NSS.S7625
12. Marulanda-Londoño E, Chaturvedi S. The interplay between obstructive sleep apnea and atrial fibrillation. Front Neurol. 2017;8:
13. Bazan V, Grau N, Valles E, et al. Obstructive sleep apnea in patients with typical atrial flutter: prevalence and impact on arrhythmia control outcome. Chest. 2013;143(5):1277–1283. doi:10.1378/chest.12-0697
14. Toraldo DM, Passali D, Sanna A, de Nuccio F, Conte L, de Benedetto M. Cost-effectiveness strategies in OSAS management: a short review. Acta Otorhinolaryngol Ital. 2017;37(6):447–453. doi:10.14639/0392-100X-1520
15. Santilli M, Manciocchi E, D’addazio G, et al. Prevalence of obstructive sleep apnea syndrome: a single-center retrospective study. Int J Environ Res Public Health. 2021;18(19):10277. doi:10.3390/IJERPH181910277
16. Garbarino S, Lanteri P, Durando P, Magnavita N, Sannita WG. Co-morbidity, mortality, quality of life and the healthcare/welfare/social costs of disordered sleep: a rapid review. Int J Environ Res Public Health. 2016;13(8):831. doi:10.3390/IJERPH13080831
17. Linz D, McEvoy RD, Cowie MR, et al. Associations of obstructive sleep apnea with atrial fibrillation and continuous positive airway pressure treatment: a review. JAMA Cardiol. 2018;3(6):532–540. doi:10.1001/jamacardio.2018.0095
18. Fein AS, Shvilkin A, Shah D, et al. Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol. 2013;62(4):300–305. doi:10.1016/J.JACC.2013.03.052
19. Saeed S, Romarheim A, Solheim E, Bjorvatn B, Lehmann S. Cardiovascular remodeling in obstructive sleep apnea: focus on arterial stiffness, left ventricular geometry and atrial fibrillation. Expert Rev Cardiovasc Ther. 2022;20(6):455–464. doi:10.1080/14779072.2022.2081547
20. Kawakami H, Saito M, Kodera S, et al. Cost-effectiveness of obstructive sleep apnea screening and treatment before catheter ablation for symptomatic atrial fibrillation. Circ Rep. 2020;2(9):507–516. doi:10.1253/CIRCREP.CR-20-0074
21. Luo JM, Huang R, Zhong X, Xiao Y, Zhou J. STOP-bang questionnaire is superior to Epworth sleepiness scales, Berlin questionnaire, and STOP questionnaire in screening obstructive sleep apnea hypopnea syndrome patients. Chin Med J. 2014;127(17):3065–3070. doi:10.3760/CMA.J.ISSN.0366-6999.20141196
22. Atrial fibrillation - symptoms and causes - mayo clinic. Available from: https://www.mayoclinic.org/diseases-conditions/atrial-fibrillation/symptoms-causes/syc-20350624.
23. Petryszyn P, Niewinski P, Staniak A, et al. Effectiveness of screening for atrial fibrillation and its determinants. A meta-analysis. Cheungpasitporn W, ed. PLoS One. 2019;14(3):e0213198. doi:10.1371/journal.pone.0213198
24. Tan A, Yin JDC, Tan LWL, Van Dam RM, Cheung YY, Lee CH. Using the Berlin questionnaire to predict obstructive sleep apnea in the general population. J Clin Sleep Med. 2017;13(3):427–432. doi:10.5664/JCSM.6496
25. Gami AS, Pressman G, Caples SM, et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110(4):364–367. doi:10.1161/01.CIR.0000136587.68725.8E
26. Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation. Circ Res. 2014;114(9):1453–1468. doi:10.1161/CIRCRESAHA.114.303211
27. Sleep apnea - symptoms and causes - mayo clinic. Available from: https://www.mayoclinic.org/diseases-conditions/sleep-apnea/symptoms-causes/syc-20377631.
28. Zhang L, Hou Y, Po SS. Obstructive sleep apnoea and atrial fibrillation. Arrhythm Electrophysiol Rev. 2015;4(1):14. doi:10.15420/AER.2015.4.1.14
29. Münzel T, Camici GG, Maack C, Bonetti NR, Fuster V, Kovacic JC. Impact of oxidative stress on the heart and vasculature: part 2 of a 3-part series. J Am Coll Cardiol. 2017;70(2):212–229. doi:10.1016/J.JACC.2017.05.035
30. Dimitri H, Ng M, Brooks AG, et al. Atrial remodeling in obstructive sleep apnea: implications for atrial fibrillation. Heart Rhythm. 2012;9(3):321–327. doi:10.1016/J.HRTHM.2011.10.017
31. Latina JM, Estes NAM, Garlitski AC. The relationship between obstructive sleep apnea and atrial fibrillation: a complex interplay. Pulm Med. 2013;2013:1–11. doi:10.1155/2013/621736
32. Goyal SK. Atrial fibrillation in obstructive sleep apnea. World J Cardiol. 2013;5(6):157. doi:10.4330/wjc.v5.i6.157
33. Hudgel DW, Gordon EA, Thanakitcharu S, Bruce EN. Instability of ventilatory control in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 1998;158(4):1142–1149. doi:10.1164/ajrccm.158.4.9712105
34. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):E56–E67. doi:10.1161/CIR.0000000000000988
35. Dopp JM, Reichmuth KJ, Morgan BJ. Obstructive sleep apnea and hypertension: mechanisms, evaluation, and management. Curr Hypertens Rep. 2007;9(6):529–534. doi:10.1007/S11906-007-0095-2
36. Sleep apnea - symptoms and causes - mayo clinic. Available from: https://www.mayoclinic.org/diseases-conditions/sleep-apnea/symptoms-causes/syc-20377631.
37. Krishnan V, Dixon-Williams S, Thornton JD. Where there is smoke…there is sleep apnea: exploring the relationship between smoking and sleep apnea. Chest. 2014;146(6):1673. doi:10.1378/CHEST.14-0772
38. Dixit R. Asthma and obstructive sleep apnea: more than an association! Lung India. 2018;35(3):191. doi:10.4103/LUNGINDIA.LUNGINDIA_241_17
39. Meszaros M, Bikov A. Obstructive sleep apnoea and lipid metabolism: the summary of evidence and future perspectives in the pathophysiology of OSA-associated dyslipidaemia. Biomedicines. 2022;10(11):2754. doi:10.3390/BIOMEDICINES10112754
40. Wang TJ, Parise H, Levy D, et al. Obesity and the risk of new-onset atrial fibrillation. JAMA. 2004;292(20):2471–2477. doi:10.1001/JAMA.292.20.2471
41. Lavie CJ, Pandey A, Lau DH, Alpert MA, Sanders P. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. 2017;70(16):2022–2035. doi:10.1016/J.JACC.2017.09.002
42. Vyas V, Lambiase P. Obesity and atrial fibrillation: epidemiology, pathophysiology and novel therapeutic opportunities. Arrhythm Electrophysiol Rev. 2019;8(1):28. doi:10.15420/AER.2018.76.2
43. Heeringa J, Kors JA, Hofman A, van Rooij FJA, Witteman JCM. Cigarette smoking and risk of atrial fibrillation: the Rotterdam Study. Am Heart J. 2008;156(6):1163–1169. doi:10.1016/J.AHJ.2008.08.003
44. Chamberlain AM, Agarwal SK, Folsom AR, et al. Smoking and incidence of atrial fibrillation: results from the Atherosclerosis Risk in Communities (ARIC) Study. Heart Rhythm. 2011;8(8):1160. doi:10.1016/J.HRTHM.2011.03.038
45. Albertsen IE, Rasmussen LH, Lane DA, et al. The impact of smoking on thromboembolism and mortality in patients with incident atrial fibrillation: insights from the Danish Diet, Cancer, and Health study. Chest. 2014;145(3):559–566. doi:10.1378/CHEST.13-1740
46. Stelmach-Mardas M, Iqbal K, Mardas M, Kostrzewska M, Piorunek T. Clinical utility of Berlin questionnaire in comparison to polysomnography in patients with obstructive sleep apnea. Adv Exp Med Biol. 2017;980:51–57. doi:10.1007/5584_2017_7/COVER
47. Jean-Louis G, Zizi F, Clark LT, Brown CD, McFarlane SI. Obstructive sleep apnea and cardiovascular disease: role of the metabolic syndrome and its components. J Clin Sleep Med. 2008;4(3):261. doi:10.5664/jcsm.27191
48. Jean-Louis G, Zizi F, Brown CD, Ogedegbe G, Borer JS, McFarlane SI. Obstructive sleep apnea and cardiovascular disease: evidence and underlying mechanisms. Minerva Pneumol. 2009;48(4):277.
49. Peppard PE, Hagen EW. Is sleep apnea a growing health problem? Blog. Sleep Health. 2019;197(3):310–312. doi:10.1164/RCCM.201708-1614PP
50. Li X, Zhou X, Xu X, et al. Effects of continuous positive airway pressure treatment in obstructive sleep apnea patients with atrial fibrillation: a meta-analysis. Medicine. 2021;100(15):e25438. doi:10.1097/MD.0000000000025438
51. Sankaranarayanan R, Bansal A, Yanamaladoddi VR, et al. Atrial fibrillation in obstructive sleep apnea patients: mechanisms, risk factors, and management strategies. Cureus. 2023;15:3. doi:10.7759/CUREUS.36282
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.