Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Prevalence of Nomophobia and Its Association with Academic Performance Among Physiotherapy Students in Saudi Arabia: A Cross- Sectional Survey
Authors Aldhahir AM ![]() , Bintalib HM, Alhotye M
, Bintalib HM, Alhotye M ![]() , Alqahtani JS
, Alqahtani JS ![]() , Alqarni OA, Alqarni AA
, Alqarni OA, Alqarni AA ![]() , Alshehri KN
, Alshehri KN ![]() , Alasimi AH
, Alasimi AH ![]() , Raya RP, Alyami MM
, Raya RP, Alyami MM ![]() , Naser AY
, Naser AY ![]() , Alwafi H
, Alwafi H ![]() , Alzahrani EM
, Alzahrani EM
Received 21 April 2023
Accepted for publication 27 June 2023
Published 25 July 2023 Volume 2023:16 Pages 2091—2100
DOI https://doi.org/10.2147/JMDH.S415891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdulelah M Aldhahir,1 Heba M Bintalib,2– 4 Munyra Alhotye,5,6 Jaber S Alqahtani,7 Omar A Alqarni,8 Abdullah A Alqarni,9 Khadijah N Alshehri,10 Ahmed H Alasimi,11 Reynie P Raya,12,13 Mohammed M Alyami,14 Abdallah Y Naser,15 Hassan Alwafi,16 Eidan M Alzahrani17
1Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 2Department of Respiratory Care, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 3King Abdullah International Medical Research Centre, Jeddah, Saudi Arabia; 4UCL Respiratory, University College London, London, UK; 5Department of Respiratory Therapy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 6King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia; 7Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 8Clinical Technology Department, Respiratory Care Program, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia; 9Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 10Physical Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 11Department of Respiratory Therapy, Georgia State University, Atlanta, GA, USA; 12Faculty of Science, Universitas ‘Aisyiyah Bandung, Bandung, Indonesia; 13Institute for Global Health, Faculty of Population Health Sciences, University College London, London, UK; 14Respiratory Therapy Department, Batterjee Medical College, Khamis Mushait, Saudi Arabia; 15Department of Applied Pharmaceutical Sciences and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan; 16Faculty of Medicine, Umm Al-Qura University, Mecca, Saudi Arabia; 17Physical Therapy Department, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia
Correspondence: Abdulelah M Aldhahir, Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Saudi Arabia, Email [email protected] Heba M Bintalib, UCL Respiratory, University College London, London, UK, Email [email protected]
Background: Nomophobia is common among students in many healthcare disciplines, and its association with academic performance has been explore before. However, there is no available data on its prevalence and association with academic performance among undergraduate physiotherapy (PT) students in Saudi Arabia.
Methods: Between 22 December 2022 and 30 January 2023, a cross-sectional survey was conducted by dissemination using an online platform (Survey Monkey).
Results: In total, 806 PT students, with males accounting for 494 (61%), responded to the survey. The prevalence of nomophobia among PT students was 98.4% (793). The mean (±SD) of the total NMP-Q items scores was 49 (± 17), indicating a mild level of nomophobia. Female PT students had significantly higher nomophobia scores than the males (47 (39– 65); 44 (38– 52); (p < 0.001)). Non-smokers had significant higher nomophobia scores than smokers (46 (38– 61); 44 (38– 49); (p = 0.004)). Regarding grade point averages (GPA), the students with a GPA of less than 3.49 had the highest nomophobia score (51 (43– 74); p < 0.001)). Concerning the stage of their studies, bridging students had the highest nomophobia score (51 (34– 76); p = 0.023)). Regarding academic warnings, those who reported no academic warnings had the highest nomophobia score (46 (42– 50); p = 0.023)). Finally, regarding study hours, the students who spent ≥ five hours studying per week had the highest nomophobia score (54 (42– 68); p < 0.001)).
Conclusion: Nomophobia is common among PT students, with the majority experiencing a mild level. Being female, non-smoker, and having a higher academic performance were risk factors associated with higher nomophobia levels.
Keywords: nomophobia, physiotherapy, PT, Saudi Arabia
Introduction
Technology plays an essential role in modern life, and what enhances our immersion in it increasingly are smartphones. They have become indispensable because they are the quickest means of communication and the easiest way to access the internet and obtain information. Just as phones have indispensable benefits aimed at human comfort, their overuse has recently shown us psychological and physical consequences that ultimately lead to changes in various aspects of life. Recently, the harm caused by technology has attracted the attention of many researchers around the world, looking into problems such as impaired concentration,1 weight disorders,2 impaired cognitive function,3 dizziness,4 and nomophobia.5
Nomophobia is a psychological disorder in which a person experiences unjustified anxiety and fear if he/she cannot use his/her phone for a while, and this fear is followed by a feeling of frustration, anticipation and obsessive thoughts.1 Nomophobia is disorder of this century due to its negative impact on adolescents. Several signs and symptoms my accompany nomophobia including anxiety, respiratory alterations, trembling, perspiration, agitation, disorientation, and tachycardia.6 It is quite widespread among adults and adolescents in Saudi Arabia7,8 Several studies have shown that nomophobia is common among students of the healthcare disciplines, and it is prevalence were ranging between 83% and 85% among medical,9–11 75% among pharmacy,12 97% among respiratory therapy students13 and 88% among nursing students,14 especially during clinical training. Despite the benefits of using the phone in the clinical setting for the availability of references and professional guidelines and the ease of searching for and obtaining information, the overuse of smartphones may distract students during their clinical training, leading to mental distraction, difficulty in concentrating, attention deficit, poor quality of patients’ care and a lack of ability to remember clinical information.15 Excessive use of smartphones may lead to nomophobia, especially as students’ progress with their academic levels and during clinical training. Nomophobia is usually assessed by questionnaires, such as the NMP-Q questionnaire.16
As it has previously been reported, several studies reported the prevalence of nomophobia among students and its association with academic performance. Lepp et al reported a relationship between low grade point average and higher cell phone usage among college students in the United States.17 Additionally, it has been reported that higher academic performance was associated with higher nomophobia scores.13,18 However, no previous study has been conducted and has reported on the prevalence of nomophobia among physiotherapy students, and the extent of its association with academic performance in Saudi Arabia. Therefore, this study aims to determine the prevalence of nomophobia and assess its association with academic performance of physiotherapy students in Saudi Arabia. Moreover, the relationship between nomophobia and sociodemographic elements, such as gender, smoking status and living arrangements, will be examined.
Methods
Study Design
Between 22 December 2022 and 30 January 2023, a cross-sectional survey was conducted and disseminated using an online platform (Survey Monkey).
Questionnaire
A questionnaire comprising 32 multiple-choice closed questions was formulated and developed to achieve the study aims. The questionnaire consisted of two sections; the first section contained 12 multiple-choice closed questions related to gender, age, geographical location, marital and smoking status, living arrangements, university sector, cumulative GPA, academic year, number of absent days during last semester, academic warnings, and the number of hours spent studying per week. The second section consisted of the nomophobia questionnaire (NMP-Q). It involved 20 statements that had been formulated and validated by Yildirim and Correia.16 The NMP-Q included four main domains: the “not being able to access information” domain, which comprised four statements; the “giving up convenience” domain, which comprised five statements; the “not being able to communicate” domain, which comprised six statements, and the “losing connectedness” domain, which comprised five statements. The questionnaire employed a seven-point Likert scale where 1 was “strongly disagree” and 7 was “strongly agree”. The NMP-Q offers a score ranging from 20 to 140, where a higher score corresponds to a higher severity of nomophobia.19 A score of 20 represents the absence of nomophobia; a score between 21 and 59 represents mild nomophobia; a score between 60 and 99 indicates moderate nomophobia, and a score between 100 and 140 represents severe nomophobia. This study used the Cronbach alpha reliability test, which was 0.95, indicating that the NMP-Q had excellent internal consistency. Additionally, the questionnaire was sent to 10 PT students, not included in the total sample, as well as with study aims for their feedback.
The purpose of the study, confidentiality statements and the contact details of the lead investigator in case any questions arose were provided to the participants before they started to answer the questionnaire. Additionally, voluntary participation was ensured by asking if the participants were happy to complete the survey or not. An additional statement was provided in the survey:
By answering ‘yes’ to completing the survey questionnaire, you voluntarily agree to participate in this study and give your consent to use your anonymous data for research purposes.
Three to five minutes was assumed to be the time required to complete the survey.
Sampling Strategy
This study utilized a convenience sampling technique to approach all governmental and private PT programs across the Kingdom of Saudi Arabia. Additionally, the survey link was sent to several faculty members of PT programs across the Kingdom of Saudi Arabia to disseminate the survey to their undergraduate PT students.
Sample Size
Based on the WHO recommendations for the minimal sample size needed for a prevalence study,20 using 95% confidence interval, a standard deviation of 0.5, and a margin of error of 5%. The required sample size was 385 participants.
Ethical Approval
The Institutional Review Board of King Abdulaziz University approved the study, reference number (435–22).
Statistical Analysis
Data were collected and analyzed using the Statistical Package for Social Sciences (SPSS software, Version 28). The normality of distributions of quantitative variables was tested using the Kolmogorov–Smirnov test and histogram. As the variables were not normally distributed, the Mann–Whitney U-test and the Kruskal–Wallis test were used to examine the differences between the median nomophobia scores among participants from different demographic groups. The categorical variables were reported and presented in percentages and frequencies. Statistical significance was considered if the p < 0.05 with a 95% confidence interval.
Results
A total of 806 PT students took part in this survey. The majority of the participants were male, accounting for 494 (61%) of the total responses. The mean standard deviation of the participants’ age was (M±SD 21 ± 1) years old, with the majority, 692 (86%), being single. The respondents came from various regions of the Kingdom of Saudi Arabia: 286 (35%) were from the Southern Region, 203 (25%) were from the Western Region, 166 (21%) were from the Central Region, 136 (17%) were from the Eastern Region and 15 (2%) were from the Northern Region. The majority of respondents were non-smokers 616 (77%), living with their families 591 (73%), with a majority, 804 (99%), enrolled in public universities. More than half of the respondents, 497 (61.7%), reported a cumulative GPA of 3.50–4.49, while 276 (34.2%) spent more than five hours a week studying. The majority, 589 (73.1%), reported that they had not received any academic warnings.
Full details of the sociodemographic data are presented in Table 1.
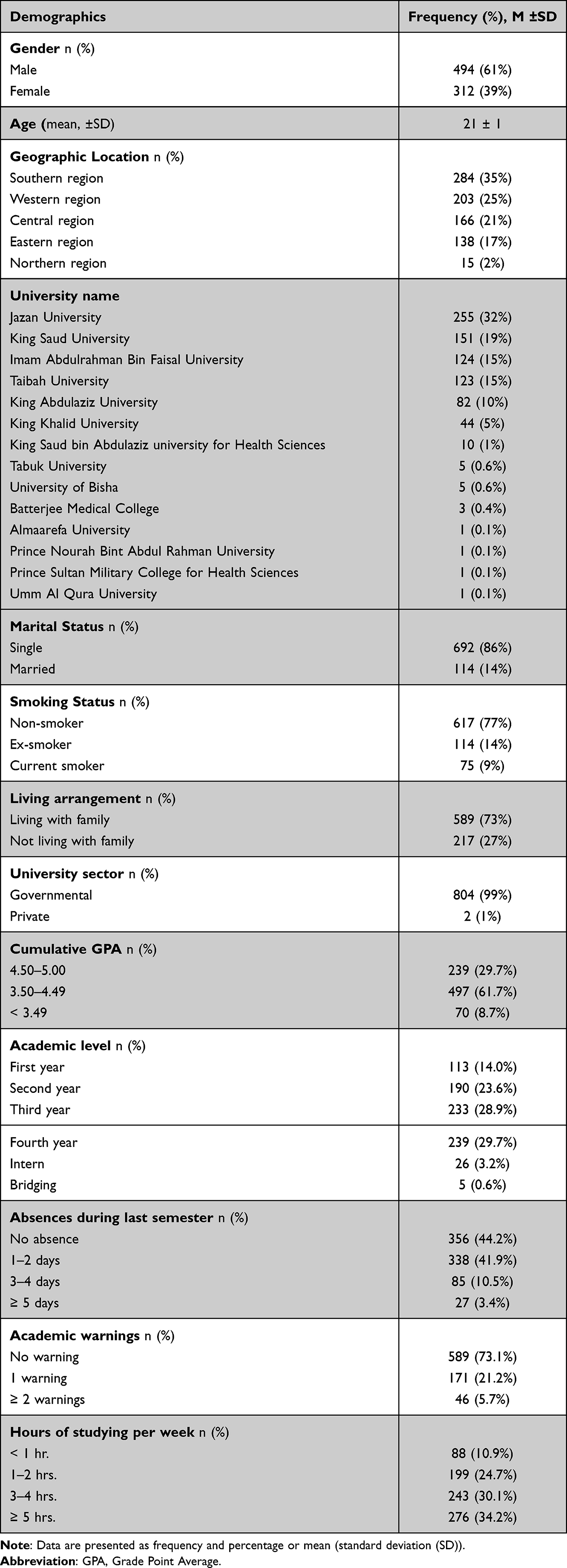 |
Table 1 Demographic Data of Physiotherapy Students (N= 806) |
The Prevalence of Nomophobia Among Physiotherapy Students
The survey data revealed a prevalence of nomophobia (98.4%) among the total respondents. The mean standard deviation of the total scores of the NMP-Q questionnaire was 49 (±17), indicating a mild level of nomophobia. The data from this questionnaire also revealed that more than half of the respondents, 603 (74.8%), had a mild level of nomophobia, while 183 (22.7%) of the respondents had a moderate level of nomophobia. Only seven (0.9%) of the respondents reported a severe nomophobia level, while 13 (1.6%) had an absence of nomophobia (Table 2). The median and interquartile ranges (IQR) of each nomophobia subscale are reported in Table 3.
 |
Table 2 Prevalence of Nomophobia Among Physiotherapy Students (N= 806) |
 |
Table 3 Physiotherapy Students’ Scores for Each NMP-Q Subscale (N= 806) |
Nomophobia and Sociodemographic Variables Among Physiotherapy Students
The survey data revealed that the female students had a significantly higher nomophobia score than the male students (female: med: 47 (IQR: 39–65); male: med: 44 (IQR: 38–52); (p <0.001)). The participants who had never smoked had a significantly higher nomophobia score compared to those who did (non-smokers: med: 46 (IQR: 38–61); smokers: med: 44 (IQR: 38–49); (p = 0.004)). Moreover, the survey data showed that PT students located in the Northern Region of the kingdom had the highest nomophobia score compared to all other regions (Northern Region: med 57 (IQR: 45–76); Western Region: med: 47 (IQR: 37–72); Southern Region: med: 45 (IQR: 45–63); Eastern Region: med: 45 (IQR: 42–52); Central Region: med: 42 (IQR: 38–50); (p <0.001)). However, no difference was found in the nomophobia score between the participants who were single or married (single: med: 45 (IQR: 38–58); married: med: 45 (IQR: 40–45); (p = 0.99)), or those who were living with their family and those who were living outside their family home (living with family: med: 45 (IQR: 38–59); living outside the family home med: 45 (IQR: 41–52); (p = 0.68)).
Nomophobia and Academic Performance Among Physiotherapy Students
The data from this survey indicated that PT students with a cumulative GPA of less than 3.49 had a significantly higher nomophobia score compared to other students (GPA of < 3.49: 51 (43–74); GPA of 3.50–4.49: 45 (39–56); GPA 4.50–5.00: 43 (37–57); (p <0.001)). The participants who were in a bridging physiotherapy program had the highest nomophobia score compared to all academic groups (first year: 43 (38–50); second year: 45 (39–54); third year: 44 (36–55); fourth year: 47 (39–67); internship: 50 (41–55); bridging program: 51 (34–76); (p = 0.023)). Moreover, the data showed that the participants who reported no academic warnings had the highest nomophobia score among all the groups (no warnings: 46 (42–50); one warning: 45 (38–62); ≥ two warnings: 42 (28–53); (p = 0.023)). Finally, the students who spent five hours studying or more per week had the highest nomophobia score compared to all groups (less than an hour: 43 (28–48); one to two hours: 43 (38–47); three to four hours: 44 (38–59); five hours or more: 54 (42–68); (p <0.001)).
Discussion
To the best of our knowledge, only limited studies have investigated the incidence rate of nomophobia and its association with academic achievement among students of various educational levels around the world.21,22 However, this study is the first to assess the prevalence of nomophobia and its association with academic performance among undergraduate PT students in the Kingdom of Saudi Arabia. Our study has demonstrated that nomophobia is a common psychological condition among these students, with the preponderance of study participants reporting mild levels of nomophobia. Furthermore, the nomophobia score was significantly higher among female, non-smoker, bridging PT program students who were from the Northern Region of the kingdom, had received no academic warnings, spent many hours studying, and had a cumulative GPA of less than 3.49.
Over recent years, technology has witnessed a rapid spread and has become ingrained in our daily lives. This is particularly so with the smartphone, which contributes positively to communication, entertainment, and education.23 Conversely, some studies have reported that overexposure and the excessive utilization of smartphones are closely linked to several negative consequences related to nomophobia, including psychological distress, emotional loneliness, and sleep disturbance.4,24 Further, a study conducted among 200 Indian medical students found that excessive use of mobile phones was a distractor that compromised academic performance by impairing concentration and interfering with the learning process.25
Our study results demonstrated that the prevalence rate of nomophobia was about 98% across all respondents, with most of them (74.8%) manifesting mild nomophobic behavior. These findings are consistent with several related studies that used the same assessment tool, which is the NMP-Q. These findings are relatively consistent with a recent study by Aldhahir et al that examined a sizable sample (n=1428) of respiratory therapy students in Saudi Arabia and revealed that nomophobia was prevalent in nearly 97% of them, with around 48% of them experiencing moderate levels of nomophobia.13 Corroborating our findings, many recent studies carried out among undergraduate medical students in Brazil and India indicated that approximately 99% of the entire population experienced nomophobia, with around 64–67% of the overall participants having a moderate level of nomophobia.10,26,27 Similarly, other related studies among university students in India and Ghana have shown a prevalence rate estimated at 96–99%, with 59% of the total respondents enduring a moderate level of nomophobia.28,29 Moreover, a cross-sectional study conducted among health sciences students at King Khalid University in Saudi Arabia found that the incidence percentage of nomophobia was 85.3%, with 22.1% experiencing severe nomophobia and 63.2% suffering from mild nomophobia.30 However, students of applied medical sciences were more vulnerable to severe nomophobia compared to students of medicine (34.4% vs 16.3%, respectively).31
Concerning the relative effect of sociodemographic variables on nomophobia, it was found that the mean scores of female PT students on the nomophobia scale were substantially higher on the nomophobia scale compared to male students. This can be a result of cell phone dependence, which raises the probability of developing smartphone addiction. These findings are identical to a systematic review of 40 articles collated by Notara et al, which revealed a statistically significant difference in nomophobia score in terms of gender, as female students reported a higher score than their male counterparts.32 Similar to our study, a recent study by Schwaiger & Tahir found that there was a significant relationship between gender and nomophobia scores among Pakistani students, showing that female students had higher nomophobia levels than male students.19 Further studies illustrated similar outcomes in Turkey, Spain, and India.33–36 Conversely, several previous studies indicated that the levels of nomophobia among students differed significantly from each other by gender, in favor of males as they tended to use smartphones to expand their level of independence, while females utilized the technology for communication.8,37,38 These outcomes are further contradicted by other studies in India and Iran, which demonstrated a non-significant association between a nomophobia score and gender.39,40
Regarding the issue of smoking, our current study discovered that non-smokers were more prone to developing nomophobia. While some studies among university students in Oman and Turkey revealed no significant difference between nomophobia and smoking habits, this may be due to a small sample size or a lack of smoker participants.21,41 Similarly, Dib et al found in a study among the Lebanese population that nomophobia and smoking were unrelated. However, a significant correlation was reported between nomophobia and waterpipes because of the length of time spent using a hookah.42 Concerning the location of the participants, students in Saudi Arabia’s Northern Region scored higher on nomophobia than their peers in other locations. Whereas a cross-sectional study conducted among Saudi Arabian respiratory therapy students indicated that students who lived away from their families had significantly higher nomophobia scores than students who resided with their families.13 Our study outcomes may have been a result of psychological stress and smartphone addiction. According to Pavithra et al, medical students experience profound stress if they lose their cell phone, run out of battery power, or cannot access the internet network. This may result in problematic behaviors.43 Tams et al also showed that individuals with nomophobia have greater stress levels.44 Additionally, a relevant study found that utilizing smartphones in the classroom has beneficial implications for the educational process. However, excessive smartphone use may detrimentally impact students’ academic performance.45
According to our findings, students with cumulative GPAs below 3.49 had substantially higher nomophobia scores. These results are analogous to those of a related study by Erdem et al, which found that nomophobia detrimentally affected the academic success of Turkish university students.46 Likewise, several studies conducted on students of different educational levels illustrated a significant effect of nomophobia on cumulative GPA. Meanwhile, students who did not experience nomophobia reported excellent academic performance.22,29 Cheever et al noted that students with nomophobia may manifest suspicious behaviors that impede cognition and concentration, which negatively affect academic achievement.47 In a systematic review conducted by Devi et al, it was pointed out that excessive use of smartphones is significantly correlated with students’ poor academic performance. In addition, it induces detrimental psychological symptoms, including anxiety and low self-esteem.48 In a cross-sectional study among nursing students in Turkey, it was found that using smartphones in classes diverts students’ attention away from theoretical lessons.49 Therefore, our study outcomes provided valuable insights to the society since it revealed the consequences of nomophobia on students’ academic performance, which necessitates the implementation of preventive measures to reduce this phenomenon.
Furthermore, our study showed that PT students in the bridging program had a significantly higher nomophobia score compared to other academic categories. In a study carried out by Gupta et al on medical students in India, it was found that first-year students had the highest nomophobia scores, while interns had the lowest scores.50 While a recently published study on RT students in Saudi Arabia reported that third-year students scored higher than their peers on the nomophobia scale.13 In contrast, some studies have reported that there is no statistically significant association between the score of nomophobia and academic level.21,29,51 Inconsistency in the results may be due to different psychological factors, such as depression and anxiety. Studies have revealed that levels of depression and anxiety are significant indicators of the nomophobia score among university students.52,53 In a study conducted by Kim et al, students frequently used their phones for extended periods to counteract the negative impacts of depression.54 According to Green et al, individuals who are addicted to using their smartphones excessively are more likely to experience depression, which exposes them to psychosocial distress.55 As such, Kliestik et al revealed that using a smartphone frequently can be a problematic behavior since it contributes negatively to inducing symptoms of anxiety and depression.56
Interestingly, our study findings reported that students with no academic warnings and a weekly study time of five hours or more scored higher on the nomophobia scale than their peers. These findings are congruent with those of Al Aldhahir et al, who observed that RT students who did not receive any academic warnings and who spent five hours studying per week had greater nomophobia scores than their counterparts.13 Our study outcomes may be related to electronic learning on digital platforms. According to numerous studies, using smartphone technology in educational spheres has favorable impacts since it provides instant access to evidence-based materials, scientific journals, and medical applications.57–59 On the other hand, a study by Jamal et al indicated that the excessive use of smartphones among medical students was closely linked to several negative influences, including sleep disturbances, headaches, impaired memory, and concentration levels.60 Moreover, Awasthi et al found that 42% of Indian undergraduate medical students were addicted to their phones, which had a major effect on their quality of life.61 Further study is needed to identify effective interventions to mitigate the widespread of nomophobia among PT students. Additionally, anxiety and depression levels associated with nomophobic PT students are warranted.
Strength and Limitations
Being the first study to explore the prevalence of nomophobia and its association with academic performance among undergraduate PT students in Saudi Arabia is a significant strength. Furthermore, the study involves a large sample size of the target population from various regions to generalize the research results across Saudi Arabia. However, the study is limited because it used a convenience sampling technique and a self-reported questionnaire to collect data to evaluate the effect of nomophobia on academic performance, which can lead to recall bias as a result of students failing to report the truth. Additionally, our survey was distributed online; therefore, our respondents maybe the PT undergraduate students who were more active or using their smartphones. Further studies are needed to evaluate the causes of nomophobia and its association with academic performance among physiotherapy students in Saudi Arabia.
Conclusion
Nomophobia is common among undergraduate PT students, with the majority experiencing a mild level. Several associated sociodemographic factors such as being female, and being a non-smoker were associated with higher nomophobia levels. Moreover, academic performance indicated by academic warnings, study time, and cumulative GPA were associated factors with the condition. Effective interventions to mitigate the widespread of moderate and severe levels of nomophobia among college students is crucially needed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. King AL, Valenca AM, Nardi AE. Nomophobia: the mobile phone in panic disorder with agoraphobia: reducing phobias or worsening of dependence? Cogn Behav Neurol. 2010;23(1):52–54. doi:10.1097/WNN.0b013e3181b7eabc
2. Kim D, Lee J, Nam JK. Latent profile of internet and internet game usage among south Korean adolescents during the COVID-19 pandemic. Front Psychiatry. 2021;12:714301. doi:10.3389/fpsyt.2021.714301
3. Al-Khlaiwi TM, Habib SS, Meo SA, et al. The association of smart mobile phone usage with cognitive function impairment in Saudi adult population. Pak J Med Sci. 2020;36(7):1628–1633. doi:10.12669/pjms.36.7.2826
4. Al-Khlaiwi T, Meo SA. Association of mobile phone radiation with fatigue, headache, dizziness, tension and sleep disturbance in Saudi population. Saudi Med J. 2004;25(6):732–736.
5. King AL, Valença AM, Silva AC, et al. ”Nomophobia”: impact of cell phone use interfering with symptoms and emotions of individuals with panic disorder compared with a control group. Clin Pract Epidemiol Ment Health. 2014;10:28–35. doi:10.2174/1745017901410010028
6. Bhattacharya S, Bashar M, Srivastava A, et al. NOMOPHOBIA: NO MObile PHone PhoBIA. J Family Med Prim Care. 2019;8(4):1297–1300. doi:10.4103/jfmpc.jfmpc_71_19
7. Humood A, Altooq N, Altamimi A, et al. The prevalence of nomophobia by population and by research tool: a systematic review, meta-analysis, and meta-regression. Psych. 2021;3:249–258. doi:10.3390/psych3020019
8. Alwafi H, Zhai S, Ouyang X, et al. Prevalence and predictors of nomophobia among the general population in two Middle Eastern countries. BMC Psychiatry. 2022;22:22. doi:10.1186/s12888-021-03681-6
9. Bano N, Khan MA, Asif U, et al. Effects of nomophobia on anxiety, stress and depression among Saudi medical students in Jeddah, Saudi Arabia. J Pak Med Assoc. 2021;71(3):854–858. doi:10.47391/JPMA.983
10. Bartwal J, Nath B. Evaluation of nomophobia among medical students using smartphone in north India. Med J Armed Forces India. 2020;76(4):451–455. doi:10.1016/j.mjafi.2019.03.001
11. Kumar A, Latha R. Nomophobia and the psycho-physiological effects of PUBG gaming on medical college student’s health and academic performance. Biomedicine. 2022;42(3):567–573. doi:10.51248/.v42i3.965
12. Cain J, Malcom DR. An assessment of pharmacy students’ psychological attachment to smartphones at two colleges of pharmacy. Am J Pharm Educ. 2019;83(7):7136. doi:10.5688/ajpe7136
13. Aldhahir AM, Bintalib HM, Siraj RA, et al. Prevalence of nomophobia and its impact on academic performance among respiratory therapy students in Saudi Arabia. Psychol Res Behav Manag. 2023;16:877–884. doi:10.2147/PRBM.S404898
14. Ayar D, Gerçeker GÖ, Özdemir EZ, Bektas M. The effect of problematic internet use, social appearance anxiety, and social media use on nursing students’ nomophobia levels. Comput Inform Nurs. 2018;36(12):589–595.
15. Aguilera-Manrique G, Márquez-Hernández VV, Alcaraz-Córdoba T, et al. The relationship between nomophobia and the distraction associated with smartphone use among nursing students in their clinical practicum. PLoS One. 2018;13(8):e0202953. doi:10.1371/journal.pone.0202953
16. Yildirim C, PaulaCorreiab A. Exploring the dimensions of nomophobia: development and validation of a self-reported questionnaire. Comput Human Behav. 2015;49:130–137. doi:10.1016/j.chb.2015.02.059
17. Lepp A, Barkley JE, Karpinski AC. The relationship between cell phone use, academic performance, anxiety, and satisfaction with life in college students. Comput Human Behav. 2014;31:343–350. doi:10.1016/j.chb.2013.10.049
18. Berdida DJE, Grande RAN. Nursing students’ nomophobia, social media use, attention, motivation, and academic performance: a structural equation modeling approach. Nurse Educ Pract. 2023;70:103645. doi:10.1016/j.nepr.2023.103645
19. Schwaiger E, Tahir R. Nomophobia and its predictors in undergraduate students of Lahore, Pakistan. Heliyon. 2020;6(9):e04837. doi:10.1016/j.heliyon.2020.e04837
20. Naing NN. Determination of sample size. Malays J Med Sci. 2003;10(2):84.
21. Qutishat M, Rathinasamy Lazarus E, Razmy AM, et al. University students’ nomophobia prevalence, sociodemographic factors and relationship with academic performance at a University in Oman. Int J Afr Nurs Sci. 2020;13:100206. doi:10.1016/j.ijans.2020.100206
22. Durak HY. Investigation of nomophobia and smartphone addiction predictors among adolescents in Turkey: demographic variables and academic performance. Soc Sci J. 2019;56(4):492–517. doi:10.1016/j.soscij.2018.09.003
23. Busch PA, Hausvik GI, Ropstad OK, et al. Smartphone usage among older adults. Comput Human Behav. 2021;121:106783. doi:10.1016/j.chb.2021.106783
24. Alzhrani AM, Aboalshamat KT, Badawoud AM, et al. The association between smartphone use and sleep quality, psychological distress, and loneliness among health care students and workers in Saudi Arabia. PLoS One. 2023;18(1):e0280681. doi:10.1371/journal.pone.0280681
25. Venkatapathy S, Bhargavan R. Impact of smartphone usage on the academic performance among medical students. J Evol Med Dent Sci. 2020;9:2020.
26. Kubrusly M, Silva PG, Vasconcelos GV, Leite ED, Santos PD, Rocha HA. Nomophobia among medical students and its association with depression, anxiety, stress and academic performance. Revista Brasileira de Educação Médica. 2021;2021:45.
27. Basu M, Shukla V, Maulik S, et al. A study on predictors of nomophobia among undergraduate medical students of a tertiary care teaching institute in Kolkata, West Bengal. J Sci Soc. 2022;49:133–139. doi:10.4103/jss.jss_36_22
28. Bajaj S, Maheshwari S, Maheshwari P. Prevalence of nomophobia among college students: an exploratory cross-sectional survey. Indian J Psychiatry Nurs. 2020;17(1):29–32.
29. Essel HB, Vlachopoulos D, Tachie-Menson A. The relationship between the nomophobic levels of higher education students in Ghana and academic achievement. PLoS One. 2021;16(6):e0252880. doi:10.1371/journal.pone.0252880
30. Hassan M, Almusa CA, Rishi K, et al. Prevalence and determinants of “no-mobile” Phobia (Nomophobia) among university students. Med J Cairo Univ. 2019;87:2581–2586. doi:10.21608/mjcu.2019.54873
31. Alahmari MS, Alfaifi AA, Alyami AH, et al. Prevalence and risk factors of nomophobia among undergraduate students of health sciences colleges at King Khalid University, Abha, Saudi Arabia. Int J Med Res Prof. 2018;4(1):429–432.
32. Notara V, Vagka E, Gnardellis C, et al. The emerging phenomenon of nomophobia in young adults: a systematic review study. Addict Health. 2021;13(2):120–136. doi:10.22122/ahj.v13i2.309
33. Arpaci I, Baloğlu M, Özteke Kozan Hİ, et al. Individual differences in the relationship between attachment and nomophobia among college students: the mediating role of mindfulness. J Med Internet Res. 2017;19(12):e404. doi:10.2196/jmir.8847
34. Moreno-Guerrero AJ, Aznar-Díaz I, Cáceres-Reche P, et al. Do age, gender and poor diet influence the higher prevalence of nomophobia among young people? Int J Environ Res Public Health. 2020;17(10):3697. doi:10.3390/ijerph17103697
35. Dasgupta P, Bhattacherjee S, Dasgupta S, et al. Nomophobic behaviors among smartphone using medical and engineering students in two colleges of West Bengal. Indian J Public Health. 2017;61(3):199–204. doi:10.4103/ijph.IJPH_81_16
36. Talan T, Kalinkara Y. An investigation of the cyberloafing and nomophobia levels of university students. Int J Res Method Educ. 2022;8(2):430–450. doi:10.46328/ijres.2708
37. Daei A, Ashrafi-Rizi H, Soleymani MR. Nomophobia and health hazards: smartphone use and addiction among university students. Int J Prev Med. 2019;10:202. doi:10.4103/ijpvm.IJPVM_184_19
38. Jilisha G, Venkatachalam J, Menon V, et al. Nomophobia: a mixed-methods study on prevalence, associated factors, and perception among college students in Puducherry, India. Indian J Psychol Med. 2019;41(6):541–548. doi:10.4103/IJPSYM.IJPSYM_130_19
39. Harish BR, Bharath J. Prevalence of nomophobia among the undergraduate medical students of Mandya Institute of Medical Sciences, Mandya. Int J Community Med Public Health. 2018;5(12):5455. doi:10.18203/2394-6040.ijcmph20184833
40. Babadi-Akashe Z, Zamani BE, Abedini Y, et al. The relationship between mental health and addiction to mobile phones among University Students of Shahrekord, Iran. Addict Health. 2014;6(3–4):93–99.
41. Işcan G, Yildirim Baş F, Özcan Y, et al. Relationship between “nomophobia” and material addiction “cigarette” and factors affecting them. Int J Clin Pract. 2021;75(4):e13816. doi:10.1111/ijcp.13816
42. Dib JE, Hallit R, Akel M, et al. Association between personality traits/dimensions and fear of no mobile phone connectivity (nomophobia): results of a Lebanese national study. Prim Care Companion CNS Disord. 2022;24(5). doi:10.4088/PCC.21m03036
43. Pavithra MB, Madhukumar S, Ts MM. A study on nomophobia - mobile phone dependence, among students of a medical college in Bangalore. Nat J Community Med. 2015;6:340–344.
44. Tams S, Legoux R, Léger P-M. Smartphone withdrawal creates stress: a moderated mediation model of nomophobia, social threat, and phone withdrawal context. Comput Human Behav. 2018;81:1–9. doi:10.1016/j.chb.2017.11.026
45. Lăzăroiu G, Kovacova M, Siekelova A, Vrbka J. Addictive behavior of problematic smartphone users: the relationship between depression, anxiety, and stress. Rev Contemp Philos. 2020;19:50–56.
46. Erdem H, Kalkin G, Türen U, Deniz M. Üniversite öğrencilerinde Mobil telefon yoksunluğu korkusunun (nomofobi) akademik başariya etkisi --- the effects of no mobile phone phobia (nomofobi) on academic performance among undergraduate students. Süleyman Demirel Üniversitesi İktisadi ve İdari Bilimler Fakültesi Dergisi. 2016;21:923–936.
47. Cheever NA, Rosen LD, Carrier LM, et al. Out of sight is not out of mind: the impact of restricting wireless mobile device use on anxiety levels among low, moderate and high users. Comput Human Behav. 2014;37:290–297. doi:10.1016/j.chb.2014.05.002
48. Devi U, Dutta R. A review paper on prevalence of nomophobia among students and its impact on their academic achievement. J Positve Sch Psychol. 2022;6(3):5397–5405–5397–5405.
49. Çatiker A, Büyüksoy GDB, Özdil K. Correlation between nomophobia, fear of missing out and academic success. Bagimlilik Dergisi. 2022;23(3):1. doi:10.51982/bagimli.1015083
50. Mengi A, Singh A, Gupta V. An institution-based study to assess the prevalence of Nomophobia and its related impact among medical students in Southern Haryana, India. J Family Med Prim Care. 2020;9(5):2303–2308. doi:10.4103/jfmpc.jfmpc_58_20
51. Marletta G, Trani S, Rotolo G, et al. Nomophobia in healthcare: an observational study between nurses and students. Acta Biomed. 2021;92(S2):e2021031. doi:10.23750/abm.v92iS2.11505
52. Çakmak Tolan Ö, Karahan S. The relationship between nomophobia and depression, anxiety and stress levels of university students. Int J Psychol Educ Stu. 2022;9(1):115–129. doi:10.52380/ijpes.2022.9.1.559
53. Augner C, Hacker GW. Associations between problematic mobile phone use and psychological parameters in young adults. Int J Public Health. 2012;57(2):437–441. doi:10.1007/s00038-011-0234-z
54. Kim E, Cho I, Kim EJ. Structural equation model of smartphone addiction based on adult attachment theory: mediating effects of loneliness and depression. Asian Nurs Res. 2017;11(2):92–97. doi:10.1016/j.anr.2017.05.002
55. Green M, Kovacova M, Valaskova K. Smartphone addiction risk, depression psychopathology, and social anxiety. Anal Metaphys. 2020;19:52–58.
56. Kliestik T, Scott J, Musa H, Suler P. Addictive smartphone behavior, anxiety symptom severity, and depressive stress. Anal Metaphys. 2020;19:45–51.
57. Gavali MY, Khismatrao DS, Gavali YV, Patil KB. Smartphone, the new learning aid amongst medical students. J Clin Diagn Res. 2017;11(5):Jc05–jc08.
58. Vinay KV, Vishal K. Smartphone applications for medical students and professionals. J Health Allied Sci NU. 2013;03(01):59–62. doi:10.1055/s-0040-1703635
59. Mohapatra D, Mohapatra M, Chittoria R, et al. The scope of mobile devices in health care and medical education. Int J Adv Med Health Res. 2015;2:3–8. doi:10.4103/2349-4220.159113
60. Jamal A, Sedie R, Haleem KA, et al. Patterns of use of ‘smart phones’ among female medical students and self-reported effects. J Taibah Univ Medical Sci. 2012;7:45–49. doi:10.1016/j.jtumed.2012.07.001
61. Awasthi S, Kaur A, Solanki H, et al. Smartphone use and the quality of life of medical students in the Kumaun Region, Uttarakhand. J Family Med Prim Care. 2020;9(8):4252–4258. doi:10.4103/jfmpc.jfmpc_805_20
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.