Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Prevalence of Myocardial Infarction With Obstructive and Non-Obstructive Coronary Arteries in a Middle-Aged Population With Chronic Airflow Limitation: A Cross-Sectional Study
Authors Sundh J ![]() , Ekström M
, Ekström M ![]() , Blomberg A, Lindberg E
, Blomberg A, Lindberg E ![]() , Malinovschi A
, Malinovschi A ![]() , Olin AC, Sköld CM, Torén K
, Olin AC, Sköld CM, Torén K ![]() , Wollmer P, Östgren CJ, Jernberg T
, Wollmer P, Östgren CJ, Jernberg T
Received 9 July 2024
Accepted for publication 16 January 2025
Published 12 February 2025 Volume 2025:20 Pages 303—312
DOI https://doi.org/10.2147/COPD.S477986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Josefin Sundh,1 Magnus Ekström,2 Anders Blomberg,3 Eva Lindberg,4 Andrei Malinovschi,5 Anna-Carin Olin,6 C Magnus Sköld,7,8 Kjell Torén,6 Per Wollmer,6 Carl Johan Östgren,9,10 Tomas Jernberg11,12
1Department of Respiratory Medicine, Faculty of Medicine and Health, Örebro University, Örebro, Sweden; 2Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Respiratory Medicine, Allergology and Palliative Medicine, Lund, Sweden; 3Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden; 4Department of Medical Sciences, Respiratory, Allergy and Sleep Research, Uppsala University, Uppsala, Sweden; 5Department of Medical Sciences, Clinical Physiology, Uppsala University, Uppsala, Sweden; 6Occupational and Environmental Medicine, School of Public Health and Community Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 7Respiratory Medicine Unit, Department of Medicine Solna and Center for Molecular Medicine, Karolinska Institutet, Stockholm, Sweden; 8Department of Respiratory Medicine and Allergy, Karolinska University Hospital, Stockholm, Sweden; 9Department of Translational Medicine, Lund University, Malmö, Sweden; 10Centre of Medical Image Science and Visualization (CMIV), Linköping University, Linköping, Sweden; 11Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 12Department of Clinical Sciences, Danderyd Hospital, Karolinska Institutet, Stockholm, Sweden
Correspondence: Josefin Sundh, Department of Respiratory Medicine, Faculty of Medicine and Health, Örebro University, Örebro, 701 82, Sweden, Tel +46702349517, Email [email protected]; [email protected]
Purpose: Myocardial infarctions (MIs) can occur in underlying obstructive coronary artery disease (MI-CAD) or in non-obstructive coronary arteries (MINOCA). The primary objectives of the study were to investigate the prevalence of MI-CAD and MINOCA in people with CAL, and to explore if CAL is an independent risk factor for MI-CAD and MINOCA. Secondary objectives were to explore these research questions stratified by sex and by smoking history.
Patients and Methods: Cross-sectional analysis of the population-based Swedish CArdioPulmonary bioImage Study (SCAPIS) of people aged 50– 64 years. CAL was defined as a post-bronchodilator ratio of forced expiratory volume in one second and forced vital capacity below 0.70. MI-CAD was defined as a self-reported MI with coronary computed tomography angiography findings of previous revascularization or at least one significant coronary stenosis (> 50%), and MINOCA as self-reported MI with no previous revascularization and no significant coronary stenosis.
Results: In total, 1735 (8.3%) of 20,882 included participants had CAL. MI-CAD was more common than MINOCA both in people with (2.8 vs 0.6%) and without CAL (1.2 vs 0.3%). Compared with those without CAL, people with CAL had an almost doubled independent risk of both MI-CAD ([adjusted OR] 1.72; [95% CI] 1.22– 2.42) and MINOCA (1.99; 1.02– 3.86). In men, CAL was associated with increased risk of MINOCA (2.63; 1.23– 5.64), and in women with increased risk for MI-CAD (3.43; 1.68– 1.26).
Conclusion: Middle-aged people with CAL have an almost doubled risk of both MI-CAD and MINOCA, compared with people without CAL. In contrast to people without CAL, the risk of MINOCA is increased in men and the risk of MI-CAD is increased in women. In a clinical context, both MI types should be considered in CAL.
Keywords: coronary atherosclerosis, COPD, smoking, sex
Introduction
People with chronic obstructive pulmonary disease (COPD) have an increased risk for both asymptomatic coronary atherosclerosis and established ischemic heart disease, which both are associated with a higher risk of premature death.1–4 The risk of myocardial infarction (MI) has been reported to be increased in people with airflow limitation, chronic bronchitis and a COPD diagnosis,5–7 and has been attributed to common risk factors such as age, smoking and systemic inflammation.7
MIs most often occur in the setting of underlying obstructive coronary artery disease (MI-CAD), but myocardial infarctions in non-obstructive coronary arteries (MINOCA) constitute 5–10% of MIs.8 Male sex is a well-known risk factor for MI-CAD, while MINOCA has been reported to be more common among women.9 In a large study of MI patients undergoing coronary angiography, COPD was more common in patients with MINOCA.10 However, population-based data on coronary artery disease status in people with chronic airflow limitation (CAL), both overall and stratified by smoking history and sex, are missing.
The aim of the present study was therefore to investigate the prevalence of myocardial infarctions with and without significant atherosclerosis in subjects with CAL compared with no CAL, stratified for smoking history and sex, in a middle-aged general population.
Materials and Methods
Data Collection and Design
This was a cross-sectional analysis of the population-based Swedish CArdioPulmonary bioImage Study (SCAPIS),11 where 30,154 randomly selected people aged 50–64 years were recruited and offered to complete a questionnaire and assessments including dynamic spirometry and coronary computed tomography angiography (CCTA). The procedure of data collection is presented in a flowchart (Figure 1).
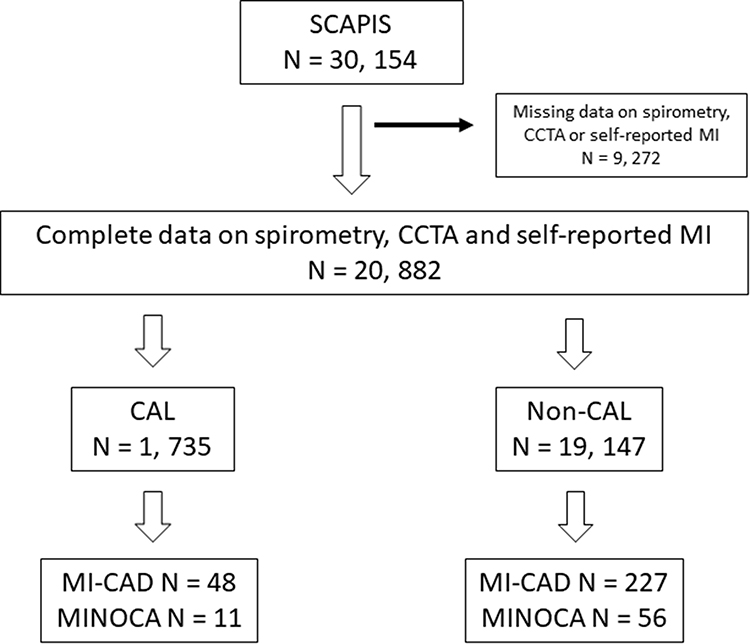 |
Figure 1 Flow chart. Flow chart data collection and outcomes. Abbreviations: CAL, chronic airflow limitation; CCTA, coronary computed tomography angiography; MI-CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with non-obstructive coronary arteries; N, number; SCAPIS, Swedish CArdioPulmonary bioImage Study. |
The dynamic spirometry assessment was performed according to European Respiratory Society (ERS)/American Thoracic Society (ATS)12 standards with the subject in a sitting position and wearing a nose clip, at least 15 min after inhalation of 400 µg of salbutamol. In all measurements, a Jaeger Master Screen PFT (Carefusion, Hoechberg, Germany) was used, providing data on the ratio of forced expiratory volume in one second (FEV1) and forced vital capacity (FVC).
CCTA was used to visualize atherosclerotic plaques noninvasively.13 Computer tomography was performed using a dedicated dual-source CT scanner equipped with a Stellar Detector (Somatom Definition Flash, Siemens Medical Solutions). For reporting coronary atherosclerosis from CCTA, the 18 coronary segment model defined by the Society of Cardiovascular Computed Tomography was used.14
The questionnaire provided self-reported data on previous physician-diagnosed MI, previously performed percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG), ongoing treatment for hypertension, hyperlipidemia and diabetes, heredity for MI, educational level, smoking status and number of pack years. From physical examination and laboratory tests, data on body mass index (BMI), systolic and diastolic blood pressure and serum levels of total cholesterol, low-density lipoprotein (LDL) cholesterol, HbA1c and C-reactive protein (CRP) were provided.
Definition of Explanation and Outcome Variables
CAL was defined as a post-bronchodilator FEV1/FVC <0.70 according to Global initiative of Obstructive Lung Disease (GOLD).15 Coronary atherosclerosis was quantified and categorized based on CCTA findings as significant (at least one existing coronary stenosis ≥50% or previously performed PCI or CABG), non-significant (at least one coronary stenosis 1–49%) or no coronary atherosclerosis. MI-CAD was defined as a self-reported MI in a person with significant coronary atherosclerosis, and MINOCA as reported MI with non-significant or no underlying coronary atherosclerosis.
Statistical Analysis
Cross-tabulations of categorical variables and mean values for continuous variables were used to present patient characteristics, coronary atherosclerosis and self-reported MI in people with and without CAL. Educational level was categorized as higher education (completed university studies) or not. Smoking status was presented as never, ex, occasional or current daily smoking, and binarized as ever smoking or never smoking in further analyses. An attrition analysis investigated differences in sex and age between the original patient population and the final study population with complete data on lung function, self-reported MI and coronary atherosclerosis.
Cross-tabulations and chi-2 test were used to explore the number of MI distributed over levels of coronary atherosclerosis overall and in people with and without CAL. Proportions of MI-CAD and MINOCA were calculated in people with and without CAL, both overall and stratified by ever/never smoking and sex.
Multi-nominal logistic regression with adjustment for potential confounders was used to analyze associations of CAL with MI-CAD and MINOCA, respectively. The choice of potential confounders was based on previous knowledge16 and included sex, age, ever smoking, BMI, educational level, treatment for hypertension, treatment for diabetes mellitus and heredity for myocardial infarction. As a sensitivity analysis, the main model was repeated with additional adjustment for CRP and hyperlipidemia. Stratification and interaction analyses were used to investigate differences by smoking history and sex. The interaction analyses used interaction terms for smoking history with each relevant variable with adjustment for the main effects and the potential true confounding factors. Potential effect modification by sex was similarly investigated using stratification and interaction analyses.
Ethics Approval and Consent to Participate
The SCAPIS multicenter study complies with the Declaration of Helsinki and was approved by the Ethical Board at Umeå University, Sweden (Dnr 2010-228-31 M), and the present analysis was approved by the Swedish Ethical Review Authority (Dnr 2021-02694). Written informed consent for data collection was obtained from all participants.
Results
Patient Characteristics
Complete data on spirometry, self-reported MI and coronary atherosclerotic disease (CAD) were available in 20,882 people, by whom 1735 (8.3%) had CAL. Participants with CAL had higher mean age and were more commonly men, lower educated and ever smokers (Table 1). Proportions of self-reported MI (3.4% vs 1.5%, p < 0.001) and significant coronary atherosclerosis at CCTA (12.2 vs 8.0, p < 0.001) were significantly higher in people with CAL than in those without CAL (Table 1). An attrition analysis of the included population (n = 20,882) and people excluded due to incomplete data on spirometry, MI or CAD showed no difference by sex and age (Supplementary Table S1).
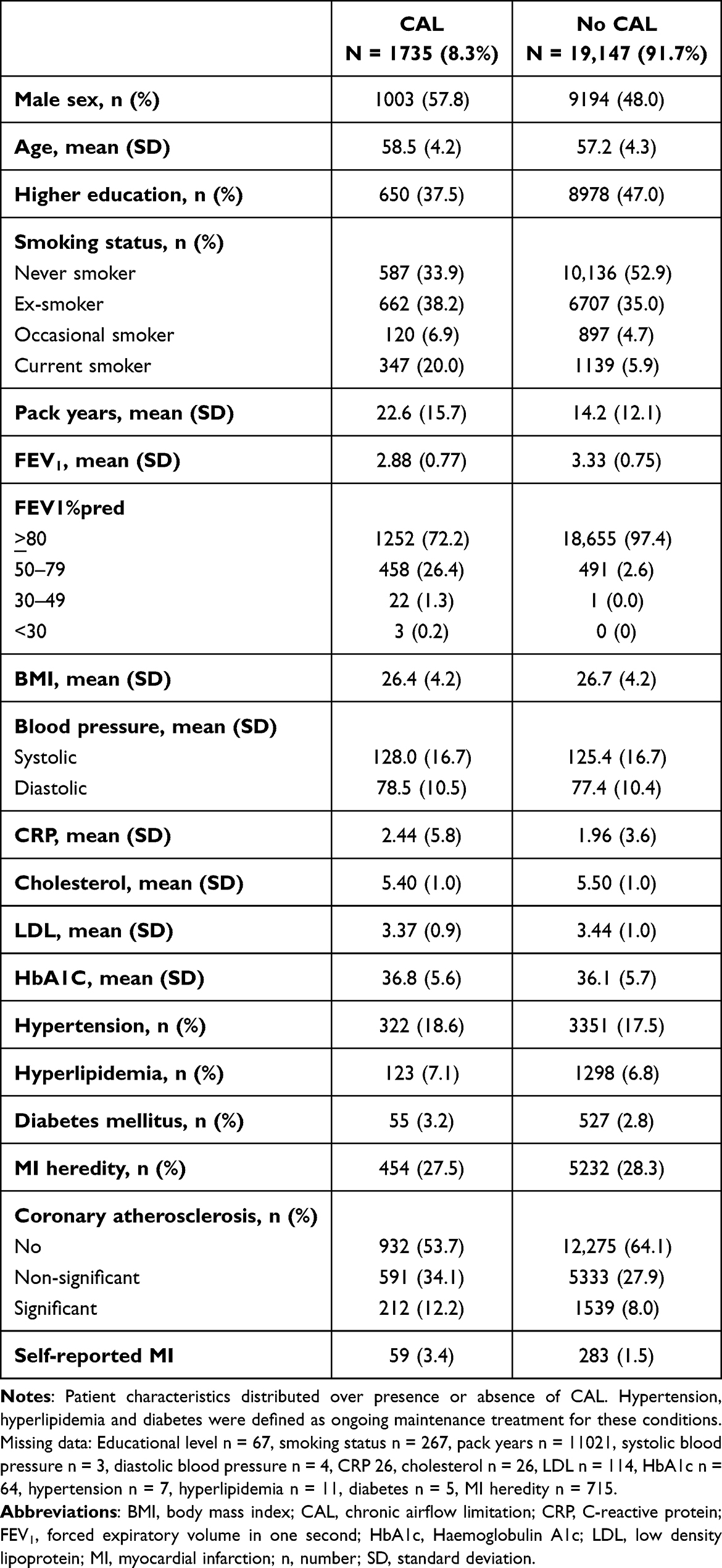 |
Table 1 Patient Characteristics |
Myocardial Infarctions in Relation to Underlying Coronary Atherosclerosis Status
Both in people with and without CAL, MI with underlying significant coronary atherosclerosis (MI-CAD) was generally more common than MI with no underlying significant coronary atherosclerosis (MINOCA) (Table 2 and Figure 2). Both MI-CAD and MINOCA were more common in people with CAL than in people without CAL (Table 2 and Figure 2). In summary, the proportion of MI-CAD was 1.2% in people without CAL and 2.7% in patients with CAL, and the corresponding proportions for MINOCA was 0.3% and 0.6%. Conversely, in patients with MI-CAD the proportion of people with CAL was 17% and in patients with MINOCA the proportion of people with CAL was 16%.
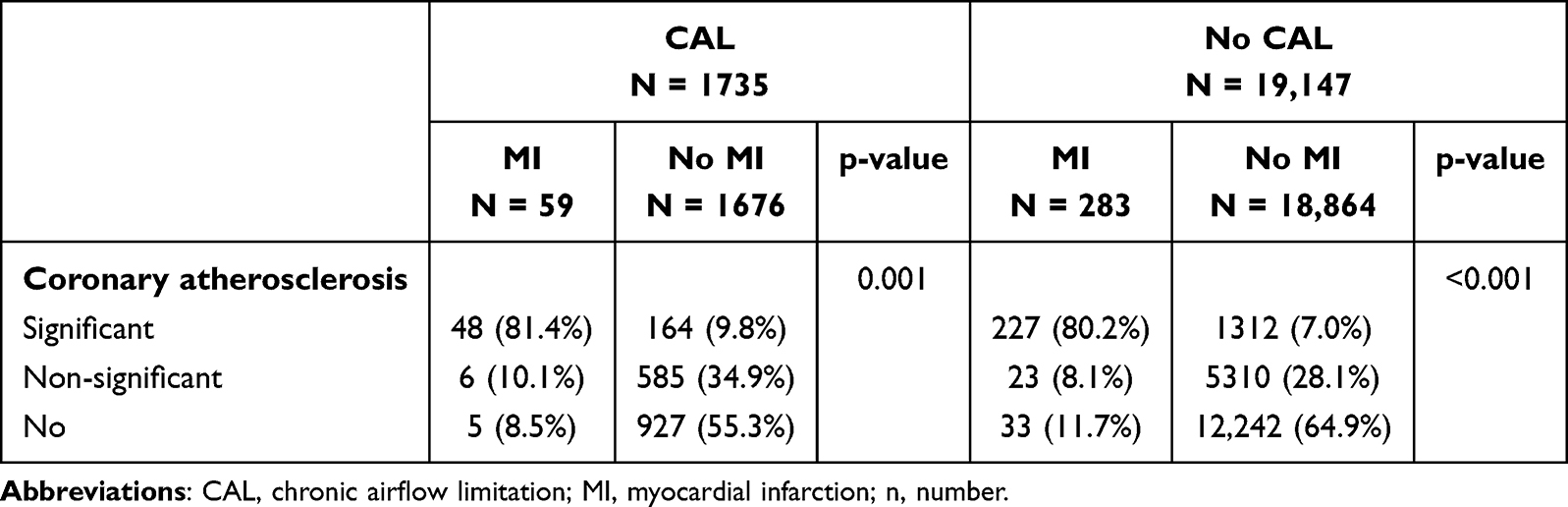 |
Table 2 Distribution of Underlying Coronary Atherosclerosis in Self-Reported MI in People With and Without CAL |
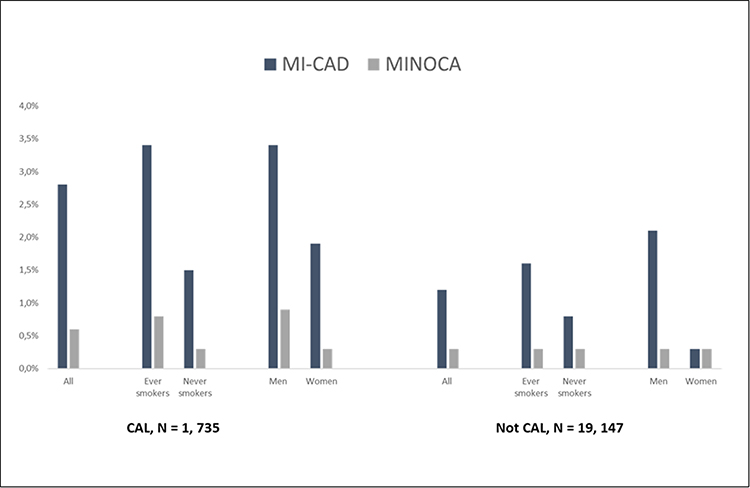 |
Figure 2 MI-CAD and MINOCA in people with and without chronic airflow limitation. Numbers and proportions of participants with MI-CAD and MINOCA in the entire study population and by smoking status and sex. Abbreviations: CAL, airflow limitation; MI-CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with non-obstructive coronary arteries; N, number. |
In multi-nominal regression, CAL was independently associated with almost doubled risk for both MI-CAD ([adjusted OR] 1.72; [95% CI] 1.22–2.42) and MINOCA (1.99; 1.02–3.86), (Figure 3). The results were essentially the same when the main model was repeated with further adjustment for CRP and hyperlipidemia (Supplementary Table S2).
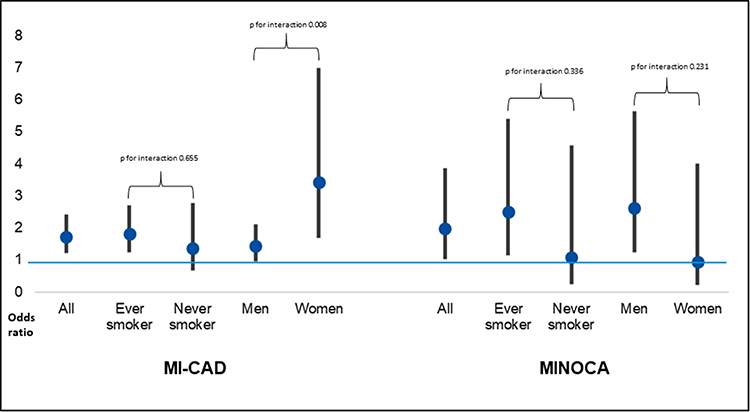 |
Figure 3 Adjusted associations of CAL with MI-CAD and MINOCA. Results from multinomial regression adjusted for CAL, adjusted for sex, age, ever smoking, BMI, educational level, treatment for hypertension, treatment for diabetes mellitus and heredity for MI. Abbreviations: BMI, Body Mass Index; CA, chronic airflow limitation; MI-CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with non-obstructive coronary arteries; N, number. |
Stratified Analyses by Smoking History and Sex
MI-CAD was more common among ever smokers than never smokers regardless of CAL. MINOCA was more common among ever smokers in people with CAL, but did not differ between ever and never smokers in people without CAL (Figure 2). In multi-nominal regression, CAL was significantly and independently associated with both MI-CAD and MINOCA compared with having no MI in ever smokers but not in never smokers (Figure 3).
MI-CAD was more common among men than women both in people with and without CAL. MINOCA was more common among men with CAL, but no sex difference was found in people without CAL (Figure 2). In addition, MI-CAD and MINOCA were equally prevalent in women without CAL (Figure 2). In stratified multi-nominal regression, CAL was independently associated with both MI-CAD and MINOCA in ever smokers but not in never smokers (Figure 3). CAL was also independently associated with MINOCA but not with MI-CAD compared with having no MI in men, and with MI-CAD but not with MINOCA compared with having no MI in women (Figure 3). The association of CAL with MI-CAD was statistically significantly stronger in women than in men (Figure 3).
Discussion
This is so far the largest study investigating associations of CAL with MI and underlying coronary atherosclerosis. The first main finding of the study was that, although MI-CAD accounts for the majority of MIs, the independent risk of both MI-CAD and MINOCA was almost doubled in patients with CAL. Secondly, the association of CAL with both MI-CAD and MINOCA was even stronger in ever smokers. Thirdly, CAL was associated with an increased risk for MI-CAD in women, and with MINOCA in men.
In summary, our findings that both MI-CAD and MINOCA are more common among people with CAL confirm results from previous studies but extend this knowledge to a population-based study. However, to our knowledge, the findings that the independent risk of both MI-CAD and MINOCA was almost doubled in patients with CAL and the specific associations of CAL with MI-CAD and MINOCA stratified by smoking history and by sex has not previously been reported.
Prevalence of MI-CAD and MINOCA in People With CAL
We found the overall prevalence of self-reported MI in CAL to be 3.4%, which is about half of the previously reported MI proportion in the Swedish population-based OLIN study of CAL from the beginning of the 90s, although the severity distribution of obstructive lung function impairment was essentially unchanged.17,18 The distinction may be due to differences in age or that the incidence of myocardial infarction has decreased over time.19,20 The overall prevalence of significant coronary atherosclerosis in our study was 12.4% in people with CAL and 8.2% in those without CAL, and non-significant coronary atherosclerosis was also slightly more common in CAL. Our findings are consistent with a small study performing coronary angiography in patients with COPD, where coronary atherosclerosis increased by COPD severity from 8 to 19%21 and with another small coronary angiography study, in which the proportions of both significant and non-significant coronary arterial disease were higher in patients with CAL than without CAL.1 Our main finding that both MI-CAD and MINOCA were more common in people with CAL is consistent with previous studies of MI patients undergoing coronary angiography,9,10 but, to our knowledge, no population-based study has investigated the MI prevalence based on underlying coronary atherosclerosis in people with CAL as a marker for COPD.
Interestingly, the proportion of patients with CAL was similar in patients with MI-CAD and in patients with MINOCA. This is consistent with a previous study of risk stratification in patients with MI in obstructive and non-obstructive coronary arteries,22 suggesting that the obstructive disease in itself is an independent risk factor possibly through systemic inflammation and hypoxemia.
Stratified Analyses by Smoking History and Sex
The association of CAL with MI may have different explanations in ever smokers and never smokers. The fact that associations of CAL with both MI-CAD and MINOCA were even more pronounced in ever smokers, confirms smoking as an important risk factor for both COPD and ischemic heart disease.23 More importantly, MI-CAD was equally common in never smokers with CAL and in ever smokers without CAL and was more common among never smokers with CAL than with no CAL, again indicating that CAL itself, regardless of smoking, is associated with an increased risk for ischemic heart disease.
The general pattern that MI-CAD was more common in men than in women both when it comes to CAL and non-CAL, is in agreement with previous studies where MI-CAD is generally more common in men.10 As for MINOCA, this entity has previously been reported to be more common in women.9,10 However, our study suggests that among people with CAL, MINOCA is actually more common in men than in women, and that MI-CAD is more common than MINOCA both in men and women. After adjustment for potential confounders, the association of CAL with MINOCA in men was even higher than the risk for MI-CAD in men and, in women, the risk for MI-CAD was almost four times higher than having no MI. We speculate that this interesting finding is supported by the hypotheses that CAL may contribute to ischemic heart disease in several ways. Literature reviews have suggested that systemic inflammation may lead to endothelial dysfunction, hypercoagulability and activation of platelets increasing the risk for plaque rupture and thrombus formation, but also that hypoxemia, tachycardia and reduced venous return due to hyperinflation and increased intrathoracic pressure may contribute to increased myocardial stress.24,25 Subsequently, CAL in itself may have higher impact on MINOCA in men, where the risk for MI-CAD is already increased, and, reversely, women with CAL would more resemble the overall male group with an increased risk for MI-CAD.
MI-CAD and MINOCA in Relation to MI Types 1 and 2
In this context, the discussion of MI types 1 and 2 may also be of interest. The classical MI type 1 occurs due to a thrombus in atherosclerotic vessels, while MI type 2 is rather caused by an imbalance between oxygen supply and need in the myocardium leading to ischemic necrosis.26, As atherosclerotic plaques are the basis for MI type 1, most MI-CAD are MI type 1.27, However, MIs occurring in people with coronary artery disease may also occur due to a temporary imbalance between oxygen supply and need, for instance due to an episode of atrial fibrillation with rapid ventricular response or a hypoxic COPD exacerbation. Several studies have reported that the presence of underlying coronary atherosclerosis is lower in patients with MI type 2,27,28 but that mortality is higher in MI type 2 than in MI type 1.28,29 In a Swedish study of almost 20,000 patients with registered MI, the proportion classified as type 2 was 7%,30, but, in a Danish study, where a clinical evaluation with stricter criteria was performed, 25% were regarded as MI type 2.31, The proportion of MINOCA in our study was 18.7% in people with CAL and 19.8 in people without CAL, possibly indicating that MI type 2 in Sweden may also be more common than reported in registers and important to consider in patients with COPD.
Strengths and Limitations
The greatest strength of our study is the large population-based sample from which the study population was obtained, and the objective assessment of CAL and coronary atherosclerosis in almost all participants. The main limitation is the cross-sectional design. Although development of atherosclerosis is a lengthy process, we cannot completely rule out that some of the reported MI-CADs actually occurred before the established coronary atherosclerosis became significant. Due to attrition, there may be a selection bias of healthier people more able to perform spirometry, but we speculate that the reported associations should rather have been stronger if more patients with severe CAL had been included. Other limitations are that generalizability is limited by the rather narrow age range and that information on MI may be biased as no record review was performed. The lack of systematic investigations like cardiac magnetic resonance32,33 also means that MIs defined as MINOCA in this study may have a non-ischemic origin such as myocarditis or Takotsubo syndrome. The number of people with MINOCA among ever smokers and women with CAL were low and, subsequently, the absence of significant associations may be due to low power.
Interpretation and Clinical Implications
The most important interpretations of this study are that CAL in itself is an independent risk factor for MI, possibly due to underlying systemic inflammation and hypoxemia. This is supported by the fact that middle-aged people with CAL had a doubled risk for MI both with and without underlying significant coronary heart disease, that the risk for MI-CAD was the same in never smokers with CAL as in ever smokers without CAL, and that the risk for MINOCA was increased in men and the risk for MI-CAD increased in women, contrarily to people with normal lung function.
The implication of this study is that in clinical praxis both MI-CAD och MINOCA should be considered in people with COPD and coronary syndrome, and that optimized treatment of COPD is warranted to prevent myocardial infarctions. Future research should focus on the prognostic impact of different treatment options in patients with COPD.
Conclusion
Middle-aged people with CAL have an almost doubled risk of MI both with and without underlying significant coronary atherosclerosis, compared with people with normal lung function. In contrast to people without CAL, the risk of MINOCA is increased in men and the risk of MI-CAD is increased in women. The risk of MI-CAD in never smokers with CAL was equal to the risk of MI-CAD in ever smokers without CAL, indicating that CAL in itself is an independent risk factor for MI. In a clinical context, both MI types should be considered in CAL.
Disclosure
Prof. Dr. Anna-Carin Olin reports personal fees from PExA AB, personal fees from Chiesi, outside the submitted work; In addition, Prof. Dr. Anna-Carin Olin has a patent WO2009045163 issued to PExA AB, a patent WO2013117747 pending to PExA AB. Prof. Dr. CM Sköld reports grants, personal fees from Boehringer Ingelheim, personal fees from Pfizer, personal fees from Glaxo Smith Kline, personal fees from AstraZeneca, personal fees from Grifols, personal fees from CSL Behring, personal fees from Chiesi, outside the submitted work. Prof. Dr. Per Wollmer reports personal fees from Chiesi Pharma, outside the submitted work. Josefin Sundh reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi and Novartis. Tomas Jernberg reports a grant from MSD and a consulting fee from Amgen to the institution. The author(s) report no other conflicts of interest in this work.
References
1. Kim JJ, Kim D-B, Jang S-W, et al. Relationship between airflow obstruction and coronary atherosclerosis in asymptomatic individuals: evaluation by coronary CT angiography. Int J Cardiovasc Imaging. 2018;34(4):641–648. doi:10.1007/s10554-017-1259-z
2. Finkelstein J, Cha E, Scharf SM. Chronic obstructive pulmonary disease as an independent risk factor for cardiovascular morbidity. Int J Chron Obstruct Pulmon Dis. 2009;4:33–349. doi:10.2147/copd.s3948
3. Curkendall SM, deLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16(1):63–70. doi:10.1016/j.annepidem.2005.04.008
4. Mannino DM, Thorn D, Swensen A, et al. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962–969. doi:10.1183/09031936.00012408
5. Walker M, Shaper AG, Phillips AN, Cook DG. Several decades ago, low forced expiratory volume as well a chronic bronchitis were first shown to be associated with a higher risk of myocardial infarction. Int J Epidemiol. 1989;18(3):602–606. doi:10.1093/ije/18.3.602
6. Haider AW, Larson MG, O’Donnell CJ, et al. The association of chronic cough with the risk of myocardial infarction: the Framingham Heart Study. Am J Med. 1999;106(3):279–284. doi:10.1016/S0002-9343(99)00027-3
7. Rothnie KJ, Yan R, Smeeth L, et al. Risk of myocardial infarction (MI) and death following MI in people with chronic obstructive pulmonary disease (COPD): a systematic review and metaanalysis. BMJ Open. 2015;5:e007824. doi:10.1136/bmjopen-2015-007824
8. Scalone G, Niccoli G, Crea F, et al. Pathophysiology, diagnosis and management of MINOCA: an update. Eur Heart J Acute Cardiovasc Care. 2019;8(1):54–62. doi:10.1177/2048872618782414
9. Dees D, Rahimi F, Amann M, et al. Prevalence and causes of myocardial infarction with non-obstructive coronary arteries in a contemporary cohort of patients with suspected myocardial infarction. J Clin Med. 2021;10(21):5188. doi:10.3390/jcm10215188
10. Ishii M, Kaikita K, Sakamoto K, et al. Characteristics and in-hospital mortality of patients with myocardial infarction in the absence of obstructive coronary artery disease in super-aging society. Int J Cardiol. 2020;301:108–113. doi:10.1016/j.ijcard.2019.09.037
11. Bergström G, Berglund G, Blomberg A, et al. The Swedish CArdioPulmonary bioimage study: objectives and design. J Intern Med. 2015;278(6):645–659. doi:10.1111/joim.12384
12. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi:10.1183/09031936.05.00034805
13. Bergström G, Persson M, Adiels M, et al. Prevalence of subclinical coronary artery atherosclerosis in the general population. Circulation. 2021;144(12):916–929. doi:10.1161/CIRCULATIONAHA.121.055340
14. Raff GL, Chair, Abidov A, et al. Society of Cardiovascular Computed Tomography. SCCT guidelines for the interpretation and reporting of coronary computed tomographic angiography. J Cardiovasc Comput Tomogr. 2009;3:122–136. doi:10.1016/j.jcct.2009.01.001
15. Global initiative for obstructive lung disease (GOLD). Global strategy for prevention, diagnosis and management of COPD. Available from: www.goldcopd.org.
16. Swedish Medical Product Agency. Att förebygga aterosklerotisk hjärt-kärlsjukdom med läkemedel - behandlingsrekommendation. Information från Läkemedelsverket. 2014;25:20–33. Swedish.
17. Eriksson B, Lindberg A, Müllerova H, et al. Association of heart diseases with COPD and restrictive lung function-results from a population survey. Respir Med. 2013;107(1):98–106. doi:10.1016/j.rmed.2012.09.011
18. Eriksson B, Backman H, Bossios A, et al. Only severe COPD is associated with being underweight: results from a population survey. ERJ Open Res. 2016;2(3):00051–2015. doi:10.1183/23120541.00051-2015
19. Gershon A, Hwee J, Victor JC, et al. Mortality trends in women and men with COPD in Ontario, Canada, 1996–2012. Thorax. 2015;70(2):121–126. doi:10.1136/thoraxjnl-2014-205956
20. Hambraeus K, Tydén P, Lindahl B, et al. Time trends and gender differences in prevention guideline adherence and outcome after myocardial infarction: data from the SWEDEHEART registry. Eur J Prev Cardiol. 2016;23(4):340–348. doi:10.1177/2047487315585293
21. Dursunoglu N, Dursunoglu D, Yıldız Aİ, et al. Severity of coronary atherosclerosis in patients with COPD. Clin Respir J. 2017;11(6):751–756. doi:10.1111/crj.12412
22. Armillotta M, Amicone S, Bergamaschi L. Predictive value of Killip classification in MINOCA patients. Eur J Intern Med. 2023;117:57–65. doi:10.1016/j.ejim.2023.08.011
23. Iwamoto H, Yokoyama A, Kitahara Y, et al. Airflow limitation in smokers is associated with subclinical atherosclerosis. Am J Respir Crit Care Med. 2009;179(1):35–40. doi:10.1164/rccm.200804-560OC
24. MacDonald MI, Shafuddin E, King PT, et al. Cardiac dysfunction during exacerbations of chronic obstructive pulmonary disease. Lancet Respir Med. 2016;4(2):138–148. doi:10.1016/S2213-2600(15)00509-3
25. Goedemans L, Bax JJ, Delgado V, et al. COPD and acute myocardial infarction. Eur Respir Rev. 2020;29(156):190139. doi:10.1183/16000617.0139-2019
26. Thygesen K, Alpert JS, White HD, et al. Universal definition of myocardial infarction. Circulation. 2007;116:2634–2653. doi:10.1161/CIRCULATIONAHA.107.187397
27. Ambrose JA, Loures-Vale A, Javed U, et al. Angiographic correlates in Type 1 and 2 MI by the universal definition. JACC Cardiovasc Imaging. 2012;5:463–464. doi:10.1016/j.jcmg.2011.12.016
28. Saaby L, Poulsen TS, Diederichsen ACP, et al. Mortality rate in type 2 myocardial infarction: observations from an unselected hospital cohort. Am J Med. 2014;127:295–302. doi:10.1016/j.amjmed.2013.12.020
29. Stein GY, Herscovici G, Korenfeld R, et al. Type-II myocardial infarction-patient characteristics, management and outcomes. PLoS One. 2014;9:e84285. doi:10.1371/journal.pone.0084285
30. Baron T, Hambraeus K, Sundström J, et al. Type 2 myocardial infarction in clinical practice. Heart. 2015;101:101–106. doi:10.1136/heartjnl-2014-306093
31. Saaby L, Poulsen TS, Hosbond S, et al. Classification of myocardial infarction: frequency and features of type 2 myocardial infarction. Am J Med. 2013;126:789–797. doi:10.1016/j.amjmed.2013.02.029
32. Popa A, Cionca C, Agoston R, et al. The role of magnetic resonance imaging in risk stratification of patients with acute myocarditis. Diagnostics. 2024;14(13):1426. doi:10.3390/diagnostics14131426
33. Bergamaschi L, Foà A, Paolisso P, et al. Prognostic role of early cardiac magnetic resonance in myocardial infarction with nonobstructive coronary arteries. JACC Cardiovasc Imaging. 2024;17(2):149–161. doi:10.1016/j.jcmg.2023.05.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.