Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence of Multidrug-Resistant Pathogens Causing Neonatal Early and Late Onset Sepsis, a Retrospective Study from the Tertiary Referral Children’s Hospital
Authors Fang P ![]() , Gao K, Yang J, Li T
, Gao K, Yang J, Li T ![]() , Gong W, Sun Q
, Gong W, Sun Q ![]() , Wang Y
, Wang Y ![]()
Received 6 April 2023
Accepted for publication 17 June 2023
Published 29 June 2023 Volume 2023:16 Pages 4213—4225
DOI https://doi.org/10.2147/IDR.S416020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Panpan Fang,1,* Kaijie Gao,1 Junmei Yang,1 Tiewei Li,1 Weihua Gong,1 Qianqian Sun,1 Yingyuan Wang2,*
1Zhengzhou Key Laboratory of Children’s Infection and Immunity, Children’s Hospital Affiliated to Zhengzhou University, Henan Children’s Hospital, Zhengzhou Children’s Hospital, Zhengzhou, People’s Republic of China; 2Department of Neonatal Intensive Care Unit, Children’s Hospital Affiliated to Zhengzhou University, Henan Children’s Hospital, Zhengzhou Children’s Hospital, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Panpan Fang; Yingyuan Wang, Email [email protected]; [email protected]
Introduction: Sepsis is the most severe infectious disease with the highest mortality rate, particularly among neonates admitted to the neonatal intensive care unit (NICU). This study retrospectively analyzed the epidemiology, antibiotic resistance profiles, and prevalence of multidrug-resistant (MDR) bacteria isolated from blood or cerebrospinal fluid (CSF) cultures in order to evaluate the appropriateness of initial empirical therapy for neonatal sepsis.
Methods: A retrospective study was conducted in the NICU from January 1, 2015, to December 31, 2022. Microbiological data from patients admitted to the NICU were anonymously extracted from the Laboratory of Microbiology database. Neonatal sepsis was classified into two types: early-onset sepsis (EOS), which occurs within the first 72 hours of life, and late-onset sepsis (LOS) for those begins later.
Results: A total of 679 bacterial strains, 543 from blood and 136 from CSF, were detected in 631 neonates. Among these, 378 isolates (55.67%) were Gram-positive bacteria, and 301 isolates (44.33%) were Gram-negative bacteria. The most frequently isolated pathogens were Coagulase-negative staphylococci (CoNS) (36.52%), followed by Klebsiella pneumoniae (20.47%) and Escherichia coli (13.84%). In EOS, 121 strains were found, CoNS represented the majority (33.88%), followed by Klebsiella pneumoniae (23.97%) and Escherichia coli (8.26%). Early-onset septicemia exhibited 67 (55.37%) MDR bacteria. In LOS, 558 strains were isolated, CoNS represented the majority of pathogens (37.10%), followed by Klebsiella pneumoniae (19.71%) and Escherichia coli (15.05%). Late-onset septicemia showed 332 (59.50%) MDR bacteria. High rates of MDR were found in CoNS (76.21%), carbapenem-resistant Klebsiella pneumoniae (66.91%), and MRSA (33.33%).
Conclusion: The study revealed an alarming prevalence of MDR strains isolated from neonatal sepsis, emphasizing the necessity of finding effective prevention and treatment measures. Colistin can be used for MDR Gram-negative bacteria, while vancomycin and teicoplanin can be considered treatment therapies for staphylococcal infections.
Keywords: MDR, EOS, LOS, sepsis, bacterial strains
Introduction
Neonatal sepsis is a severe infectious disease primarily caused by pathogenic bacteria. It is characterized by the systemic inflammatory response syndrome and remains a significant factor associated with long-term morbidity and mortality in neonates.1,2 The neonatal mortality rate has remained high, with 2.6 million deaths per year over the past two decades.3 According to the Global Burden of Disease study in 2019, neonatal sepsis and other neonatal infections rank as the third leading cause of neonatal death.4 In China, between 1996 and 2015, the cause-specific mortality rate of neonatal sepsis decreased from 0.4 to 0.1 per 1000 live births (LBs), which is significantly lower than the global estimate of 2.8 per 1000 LBs in 2015.5 Notably, there is a significant variation in the mortality rate of neonatal sepsis across different regions in China.6 Based on different definitions across regions,7–9 EOS is defined as the presence of pathogenic bacteria in blood or CSF cultures within 72 hours after birth, often resulting from vertical transmission of maternal pathogens during prenatal or intrapartum infection. On the other hand, LOS refers to sepsis that occurs after 72 hours of life during the birth hospitalization and involves a larger proportion of nosocomial and community-acquired infections.10
In addition to the differences in onset time, there are significant variations in pathogen distribution and antimicrobial susceptibility between EOS and LOS. Considering these factors, the management and reduction of neonatal sepsis present significant challenges.
Antimicrobial resistance (AMR) poses a global threat to health and development. MDR is becoming increasingly prevalent among pathogenic bacteria, both in healthcare settings and the community. The emergence of drug-resistant pathogens creates substantial challenges for the healthcare system, encompassing the diagnosis, treatment, and containment of infections caused by resistant organisms.11,12
To effectively prevent and treat infections caused by MDR bacteria, particularly those leading to sepsis, continuous monitoring of microbial etiology and antimicrobial resistance profiles is essential. While numerous studies have examined the distribution of pathogens and antimicrobial resistance in sepsis,13–15 limited information is currently available on the prevalence of MDR in neonates with sepsis, particularly in developing regions such as Henan Province in central China.
This study aimed to analyze the distribution of bacteria, their antibiotic resistance profiles, and the prevalence of MDR in neonates with early and late-onset sepsis admitted to the NICU. By doing so, it provides crucial epidemiological data for guiding the initial empirical treatment of neonatal sepsis in the region.
Materials and Methods
Study Design and Setting
The research conducted at the Children’s Hospital Affiliated to Zhengzhou University in Henan, China, is a retrospective study on patients with sepsis in the NICU from January 1, 2015, to December 31, 2022. The hospital is one of the largest tertiary first-class children’s hospitals in China, boasting 2200 registered beds. The NICU consists of three separate sections with a total of 200 beds, and on average, 60 newborns are admitted to the unit for various reasons and receive treatment services weekly.
In cases where a patient had multiple episodes of bloodstream infection (BSI) or CSF infection, only the first occurrence of the same type of sample was included in the data analysis. The study included patients aged ≤28 days. Neonatal sepsis was divided into two groups, early-onset sepsis and late-onset sepsis, following relevant guidelines and standards.16,17 Patients infected within 72 hours were classified into the early-onset group, while those infected later were assigned to the late-onset group. The distribution of multi-drug resistant bacteria between the two groups was subsequently compared.
The methodology of the study is illustrated in Figure 1. Duplicate strains were eliminated, and only the first tested sample from each patient was retained. Blood and CSF samples were collected using specialized bottles (BACTEC PEDS Plus/F Culture Vial) provided with the automated system BD BACTEC™. Due to the low body weight of newborns and the relatively small amount of blood that can be collected, only one blood sample was obtained from each newborn for cultivation. The plastic plug on the top of the blood culture bottle was disinfected with 75% alcohol and allowed to dry for 60 seconds. The skin at the blood collection site was disinfected with an appropriate disinfectant selected according to the patient’s condition. Venous whole blood was then collected using a syringe and transferred into the blood culture bottle for immediate examination. The second tube of cerebrospinal fluid sample was used for sterile culture after the clinical doctor performed a lumbar puncture on the neonate in the NICU.
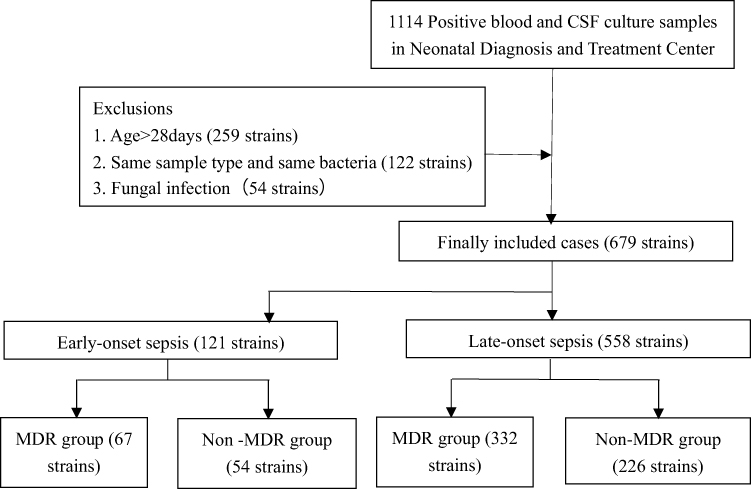 |
Figure 1 Flowchart of study participant enrollment. |
In this study, we conducted an analysis of the percentage of MDR strains isolated from different clinical NICU. The main types of antibiotics examined included aminoglycosides, cephalosporins, carbapenems, tetracyclines, and fluoroquinolones. MDR bacteria were defined as those exhibiting resistance to at least three different antibiotic groups.18
Definitions
MDR is commonly defined as non-susceptibility to at least one agent in three or more antimicrobial categories, and it is commonly defined as resistance to antimicrobial drugs from more than three classes.18,19
Another commonly used method to characterize bacteria as MDR is when they exhibit resistance to one key antimicrobial agent.20 These bacterial isolates may have public health significance as they are resistant to only one key antimicrobial agent, but they often demonstrate cross or co-resistance to multiple classes of antimicrobials, thus qualifying as MDR. Acronyms are created for bacteria based on their resistance to key antimicrobial agents, such as methicillin-resistant Staphylococcus aureus (MRSA), methicillin-resistant coagulase-negative staphylococcus (MRCNS), extended-spectrum beta-lactamases (ESBLs) (carbapenem-resistant Enterobacteriaceae bacteria producing ESBLs are not included as ESBL strains in this study), and carbapenem-resistant Enterobacteriaceae bacteria (CRE).
Data Collection
Data were collected from January 2015 to December 2022 from the laboratory database of the clinical microbiology department in the hospital. Blood and CSF specimens from all neonatal patients admitted to the ICU during the study period were sent to the hospital’s microbiology laboratory. This retrospective and analytical study obtained information from medical records and microbiology databases. The analyzed variables included gender, age of infection, infection sites, and patterns of antimicrobial drug resistance, which were stored in the WHONET system and the hospital information system.
Antimicrobial Susceptibilities
Clinical isolates were identified using the VITEK 2 Compact system (bioMérieux, France) or MALDI-TOF MS (Bruker, Germany), and antimicrobial susceptibilities were determined in vitro using VITEK-2 Compact ASTGN16 (bioMérieux, France) or the Kirby-Bauer test. The commonly tested antibiotics for gram-negative bacteria included penicillins (ampicillin, piperacillin), beta-lactam/beta-lactamase inhibitors (ampicillin/sulbactam, piperacillin/tazobactam, amoxicillin/clavulanic acid), aminoglycosides (amikacin, gentamicin), monobactams (aztreonam), fluoroquinolones (ciprofloxacin, levofloxacin), third-generation cephalosporins (ceftazidime, cefotaxime), fourth-generation cephalosporins (cefepime), carbapenems (meropenem, imipenem), amphenicols (chloramphenicol), tetracyclines (tetracycline), and polymyxins (colistin). For gram-positive bacteria, the tested antibiotics included penicillins (penicillin, oxacillin), lincosamides (clindamycin), macrolides (erythromycin), aminoglycosides (gentamicin), fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin), rifampin, tetracyclines (tetracycline), nitrofuran derivatives (nitrofurantoin), glycopeptides (vancomycin, teicoplanin), and oxazolidinones (linezolid). The results of antimicrobial susceptibility testing were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) guidelines from 2021.21 The sizes of the zones of inhibition surrounding the disks were measured using a digital caliper. Quality control was performed by testing Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, Staphylococcus aureus ATCC 25923 and ATCC 29213, Streptococcus pneumoniae ATCC 49619, and Enterococcus faecalis ATCC 29212. These quality control strains were utilized to ensure the accuracy and reliability of bacterial identification and drug sensitivity tests.
Statistical Analysis
Antimicrobial susceptibility data were analyzed using the WHONET 5.6 software (WHO, Geneva, Switzerland). Other data analyses were conducted using SPSS software (Version 21.0). GraphPad Prism 9 software (GraphPad Software, La Jolla, CA, USA) was utilized for generating graphs, and all counts were presented as percentages (%).
Results
Bacterial Distribution
In the analyzed interval (2015–2022), a total of 679 bacterial strains were identified, excluding cases with multiple isolates of the same pathogen from the same patient and infection site. Among these, 543 strains were from blood and 136 from CSF, detected in 631 neonates. Of the neonates, 583 (92.39%) had only one positive culture throughout their hospital stay, while 48 (7.61%) had multiple cultures, resulting in a total of 96 isolated strains. Among the neonates, 38 were infected with both blood and CSF simultaneously. Out of the total, 383 (60.70%) were male infants and 248 (39.30%) were female infants. Among the isolates, 378 (55.67%) were Gram-positive bacteria and 301 (44.33%) were Gram-negative bacteria, including 121 strains in early-onset infection and 558 strains in late-onset infection. In early-onset septicemia, 67 (55.37%) were MDR bacteria, while in late-onset septicemia, 332 (59.50%) were MDR bacteria. The study design is illustrated in Figure 1.
The most commonly identified microorganism throughout the entire study period (2015–2022) was CoNS, accounting for 248 (36.52%) cases. Among the CoNS, Staphylococcus epidermidis was the most prevalent with 148 (59.68%) cases, followed by Staphylococcus hominis with 41 (16.53%) cases, Staphylococcus haemolyticus with 37 (14.92%) cases, and others with 22 (8.87%) cases. Klebsiella pneumoniae (139–20.47%) and Escherichia coli (94–13.84%) were the next most frequently identified pathogens. The pathogens isolated in EOS and LOS are summarized in Table 1. The study findings suggested that there were significantly more LOS isolates than EOS, with the exception of Listeria monocytogenes.
 |
Table 1 Distribution of the Microorganisms Isolated from NICU Neonatal Sepsis, 2015–2022 |
Multidrug-Resistant Pathogens Involved in EOS and LOS
Throughout the entire study period, CoNS consistently ranked first, except in 2021 (11–25.58%). It is worth noting that the number and proportion of CoNS showed a declining trend from 2015 to 2022. Consequently, the proportion of other isolates increased, particularly Klebsiella pneumoniae and Escherichia coli. The proportion of Klebsiella pneumoniae reached as high as 32.56% in 2021, followed by Escherichia coli at 25.84% in 2019. The overall number of pathogens isolated from neonatal sepsis exhibited a declining trend since 2020 compared to the period of 2015–2019 (Table 2), which can be attributed to the impact of the 2019 novel coronavirus (COVID-19) pandemic.
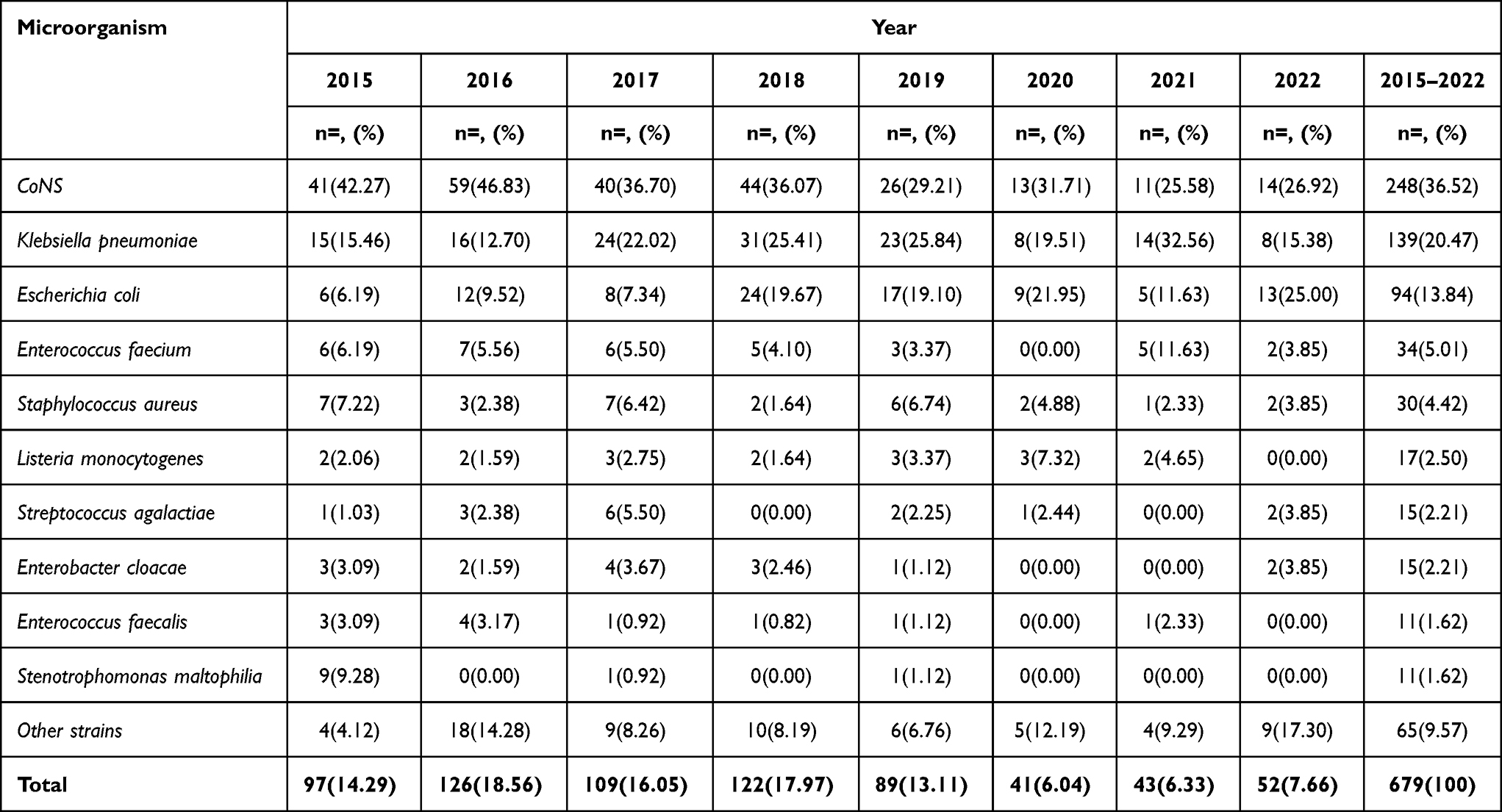 |
Table 2 Distribution of the Microorganisms Isolated from Neonatal Sepsis, 2015–2022 |
In this study, we analyzed the number of patients admitted to the neonatal treatment center of our hospital and the incidence rate of neonatal sepsis. The number of hospitalized patients and the incidence rate of sepsis decreased in 2020 and 2021, while the incidence rate increased in 2022. We also examined the number of microorganisms causing neonatal sepsis and the percentage of MDR from 2015 to 2022. The number of isolated strains significantly decreased in 2020 compared to the previous year (p < 0.05). There was also a noticeable decrease in the percentage of MDR from 2015 to 2016, although without statistical significance. The results further indicated that the number of culture-positive pathogens, the number of MDR pathogens, and the MDR rate in neonatal sepsis gradually declined from 2019 to 2022 (Figure 2).
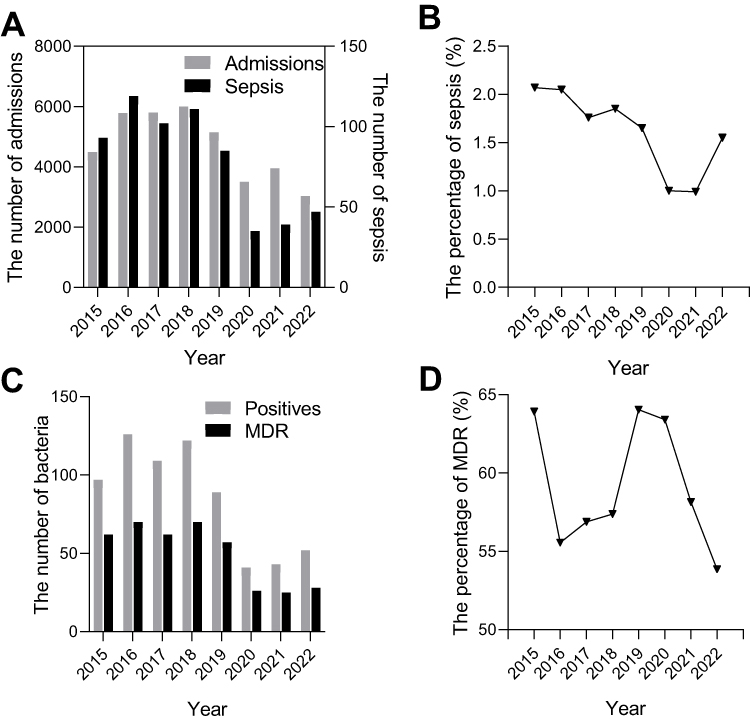 |
Figure 2 The number of neonatal admissions (A), the percentage of neonatal sepsis (B), the number of positive bacteria (C), and the percentage of MDR (D) from 2015 to 2022. Admissions: the number of neonates admitted; Positives: the number of pathogens. |
Our study also presented the distribution of MDR types in neonatal sepsis. MRCNS ranked first, with a percentage higher than 70% in both EOS and LOS. The second most prevalent MDR isolate was carbapenem-resistant Klebsiella pneumoniae, with a ratio of 64.55% in LOS and even higher at 75.86% in EOS. Additionally, the proportion of MRSA in LOS neonates is as high as 50%, which warrants close attention from clinical and drug resistance monitoring departments (Figure 3). Overall, there are significantly more LOS isolates than EOS, and the proportion of multiple drug resistance is slightly higher than that of EOS, except for carbapenem-resistant Klebsiella pneumoniae.
 |
Figure 3 The distribution (A) and prevalence (B) of different types of MDR bacteria in early and late sepsis. Abbreviations: MRCNS, methicillin-resistant coagulase negative staphylococcus; HLAR, high levels of aminoglycosides resistance Enterococcus; Kpn, Klebsiella pneumoniae; Eco, Escherichia coli; Efm, Enterococcus faecium; Sau, Staphylococcus aureus; Other, other strains. |
Antibiotic Susceptibility
Table 3 presents the drug resistance patterns of isolated Gram-positive bacteria. Methicillin resistance was observed in 76.21% of CoNS and 33.33% of Staphylococcus aureus strains. Nearly 90% of the CoNS strains were resistant to penicillin, over 80% to erythromycin, 65.73% to clindamycin, and 50.81% to trimethoprim/sulfamethoxazole. Notably, two Linezolid-resistant CoNS strains were detected. The rates of drug resistance to antimicrobial agents in CoNS isolated from EOS were generally higher than those from LOS. However, these results must be interpreted with caution, considering the possibility of sample contamination. Collecting duplicate blood cultures would have been necessary to confirm the presence of the same bacteria and support the diagnosis.
 |
Table 3 Antimicrobial Resistance Pattern of Gram Positive Coci (Number and Percentage) Causing Neonatal Sepsis from 2015 to 2022 |
In the case of Staphylococcus aureus isolates, a very high percentage of resistance was observed for penicillin (up to 96.67%), erythromycin (over 70%), and clindamycin (around 60%). In our study, a total of 30 strains of Staphylococcus aureus were isolated, of which only 2 were derived from EOS and were methicillin-sensitive strains. Enterococcus faecium exhibited a very high percentage of resistance to antimicrobial agents, including penicillin (100%), erythromycin (97.06%), rifampin (100%), and ciprofloxacin (100%). One Linezolid-resistant strain was detected. No resistance to teicoplanin and vancomycin was observed among the Gram-positive bacteria in our study.
Klebsiella pneumoniae and Escherichia coli were the most frequently detected pathogens among Gram-negative bacilli, accounting for 77.41% (233/301) of the negative bacilli in our study. Klebsiella pneumoniae isolated from EOS showed high resistance to cephalosporins, with over 90% of the strains resistant to third- and fourth-generation cephalosporins. Additionally, 79.31% of the EOS Klebsiella pneumoniae strains were resistant to imipenem and meropenem, significantly higher than in LOS (66.36% and 63.64%, respectively). Our study also revealed a high proportion of resistance to monobactams (Aztreonam) (over 80%) and amoxicillin/clavulanic acid (almost 90%). Apart from gentamicin, the rates of resistance to other antimicrobial agents in Klebsiella pneumoniae isolated from EOS were generally higher than those from LOS (Table 4).
 |
Table 4 Antimicrobial Resistance Pattern of Gram-Negative Bacilli (Number and Percentage) Causing Neonatal Sepsis from 2015 to 2022 |
Almost one-third of Escherichia coli isolates showed resistance to aztreonam and third-generation cephalosporins, while less than 6% exhibited resistance to carbapenems, and all carbapenem-resistant Escherichia coli strains were isolated from LOS. In contrast to Klebsiella pneumoniae, the rates of resistance to other antimicrobial agents in Escherichia coli isolated from EOS were generally lower than those from LOS. The research highlighted a more severe drug resistance situation with Klebsiella pneumoniae compared to Escherichia coli, with a statistically significant difference observed in the drug resistance rates of cefepime, cefotaxime, and ceftazidime between the two (p < 0.001) (Table 4).
Discussion
It is well known that MDR has emerged as a significant concern in intensive care unit (ICU) settings.22–24 In our study, spanning 8 years, we aimed to analyze the distribution, drug resistance patterns, and prevalence of MDR pathogens isolated from neonates with early and late-onset sepsis in a large tertiary NICU in China.
Among the MDR bacteria identified in our study, CoNS accounted for the highest proportion (47.37%), followed by Carbapenem-resistant Klebsiella pneumoniae (CRKP) (34.84%), and MRSA (2.51%). In other studies investigating MDR strains in sepsis, MDR Enterobacteriaceae were found to be the most commonly isolated microorganisms,25–27 whereas vancomycin-resistant enterococci were ranked first in another study.28 Regional differences were observed in the distribution of multidrug-resistant bacteria. The number of MDR strains associated with LOS was significantly higher than that of EOS, which is consistent with similar studies.9,29
Our study revealed that the most frequently isolated strains associated with neonatal sepsis were CoNS (36.52%), followed by Klebsiella pneumoniae (20.47%) and Escherichia coli (13.84%), in accordance with previous reviews.30 However, there were slight differences compared to a study conducted in Romania, where CoNS (51.54%), Klebsiella pneumoniae (11.34%), and Staphylococcus aureus (9.40%) were the most prevalent.12 Another study by Robledo J reported that the leading microorganisms in neonatal sepsis were CoNS (47.1%), followed by Escherichia coli (8.9%) and Staphylococcus aureus (7.5%).13 Similarly, a study conducted in China found that CoNS (38.0%) were the most common, followed by Escherichia coli (17.2%) and Klebsiella pneumoniae (11.4%).27 Notably, the number and proportion of CoNS exhibited a declining trend from 2015 to 2022, particularly in the past three years.
CoNS were the most prevalent MDR strains among the microorganisms isolated in our research. The antimicrobial resistance pattern to methicillin was observed in 76.21% of CoNS, with 82.93% in EOS and 74.88% in LOS, which was slightly lower than the CHINET surveillance data in 2016 (83.69% resistant to oxacillin)14 and in 2021 (77.7% resistant to oxacillin) (http://www.chinets.com/Data/AntibioticDrugFast). Nearly 90% of the isolated CoNS strains were resistant to penicillin, over 80% to erythromycin, 65.73% to clindamycin, and 50.81% to trimethoprim/sulfamethoxazole, which was much higher than a study conducted in Romania (78.93% resistant to penicillin, 72.96% to erythromycin, and 59.12% to clindamycin).12 Notably, we detected 2 (0.81%) linezolid-resistant CoNS strains, while a study from China reported a linezolid resistance rate of 1.6%.31 Linezolid-resistant Staphylococcus has become a new challenge for clinical anti-infective therapy. The rates of drug resistance among CoNS isolated from EOS were generally higher than those from LOS. Interestingly, CoNS were isolated in 33.88% of EOS cases and 37.10% of LOS cases, which is relatively high compared to other studies.25,32,33 This difference may be attributed to variations in the definitions of CoNS sepsis and the challenges associated with distinguishing between true infections and contaminations.34 However, with the continuous progress and widespread use of invasive diagnostic techniques in recent years, invasive infections caused by CoNS have received increasing attention.35 Collecting duplicate blood cultures would have been beneficial in identifying the same bacteria and supporting the diagnosis.36
Klebsiella pneumoniae MDR strains had a high prevalence and were the most common Gram-negative bacteria in our research. Among the strains of Klebsiella pneumoniae, 126 (90.65%) were found to be producing ESBLs. This finding is consistent with the data from the China Bacterial Resistance Surveillance Network (CHINET), which indicates that approximately 50% or more of Klebsiella pneumoniae isolates are resistant to commonly used broad-spectrum penicillins (including ampicillin-sulbactam), cephalosporins, gentamicin, and fluoroquinolones.14 In our study, we also identified a high resistance rate of over 90% among the isolated strains to third-generation and fourth-generation cephalosporins due to the circulation of ESBL strains in the region. Additionally, 61.87% of the strains were resistant to gentamicin and over 60% to fluoroquinolones. These findings suggest that these antibiotics are not suitable as empirical therapy for treating bloodstream infections caused by Klebsiella pneumoniae.14,29
Overall, 66.91% of the isolated Klebsiella pneumoniae strains were identified as CRKP, which was notably higher than in other similar studies.14,27,30,33 Among the EOS Klebsiella pneumoniae strains, 79.31% were resistant to imipenem and meropenem, significantly higher than in LOS (66.36% and 63.64%, respectively). The high percentage of CRKP infections leads to prolonged hospital stays, increased healthcare costs, and elevated mortality rates.37 The rates of drug resistance among common antimicrobial agents tested for Klebsiella pneumoniae isolated from EOS were generally higher than those from LOS, with all tested antimicrobial agents showing higher resistance rates, except for gentamicin and polymyxin B. However, other studies have reported different findings.38,39 This discrepancy suggests that different regions may require distinct antimicrobial regimens for different types of infections, underscoring the importance of antimicrobial resistance surveillance.
Our research revealed that 7.91% of the tested Klebsiella pneumoniae strains were resistant to colistin, which is lower than a study conducted in Romania (21%),12 but slightly higher than a study in Iran (6.9%).40 This poses a significant public health risk, considering the rapid emergence of MDR Gram-negative bacteria and the limited development of new anti-infective agents. Colistin has become a crucial component in clinical practice, either as monotherapy or in combination therapy.41
Escherichia coli was the second most common bacterial species after Klebsiella pneumoniae. The proportion of MDR strains of Escherichia coli was relatively low, with 44 (46.81%) strains producing ESBLs, and only 5.32% of carbapenem-resistant Escherichia coli (CREC). The detection rate of CREC was consistent with most similar studies.26,42,43 In our study, no CREC strains were detected in EOS, which was consistent with research conducted in China in 2022.33 The resistance rates to cefepime, cefotaxime, and ceftazidime were 37.23%, 50.00%, and 26.6%, respectively, and approximately 60% to fluoroquinolones in our study. According to multicenter study data, E. coli is also a major cause of bloodstream infections in China, with around 30% of the isolates showing resistance to ceftazidime, cefepime, and aztreonam, and nearly 50% resistant to fluoroquinolones.14,39
Our study demonstrated significant differences in the isolation frequency and AMR of bacteria between EOS and LOS. The research highlighted a more severe drug resistance situation in Klebsiella pneumoniae compared to Escherichia coli. Apart from the considerable variation in carbapenem resistance, there was a statistically significant difference in the drug resistance rates of Klebsiella pneumoniae and E. coli strains to cefepime, cefotaxime, and ceftazidime.
Approximately one third of the isolated Staphylococcus aureus strains were identified as methicillin-resistant Staphylococcus aureus (MRSA), which is lower than the percentages reported in other similar domestic and foreign studies,14,44–46 but higher than some other findings.47 In our research, only 30 (4.42%) strains were isolated as MRSA, which aligns with a multicenter study conducted in China (4.2%).27 However, Staphylococcus aureus contributes to invasive infections, posing a higher burden in terms of morbidity and mortality. The antibiotic resistance of MRSA has become a serious issue, necessitating the exploration of new drug regimens for MRSA infection.44,48–50
Of the Enterococcus faecium strains, 9 (26.47%) were resistant to high-level gentamicin (HLAR), which is much lower than the percentage reported in another study (57.5%).43 We detected a linezolid-resistant strain with resistance rates exceeding 90% for penicillin, erythromycin, rifampin, and ciprofloxacin, and 64.71% for levofloxacin. The resistance rates of these commonly used antibiotics were higher than in other studies (except for vancomycin, as no vancomycin-resistant strains were detected in our study).26
It is worth noting that the number of newborns admitted, positive pathogens, MDR pathogens, and the rate of multidrug resistance in neonatal sepsis gradually decreased from 2019 to 2022, as detailed in our separate study.51 Since 2019, the global public health has been threatened by the COVID-19. In response to COVID-19, our local government implemented strict preventive measures, significantly reducing the number of children from other areas referred to and visiting our facility. Furthermore, the infection management department emphasized the prevention and control of hospital infections and implemented a series of measures to strengthen and standardize antibiotic usage starting from 2020. Despite the small total number of newborns admitted, the rates of sepsis have increased in 2022 compared to 2020 and 2021.
Our findings highlight the urgent need for the rapid implementation of public health measures, including the application of antimicrobial stewardship policies and interventions to prevent and control hospital-acquired infections. Effective control measures were determined based on clinical observations, epidemiological investigations, and laboratory evidence.
Our study has some limitations. Although supported by a large sample size, it was a single-center retrospective study conducted in the central region of China, which limits the generalizability of the antibiotic resistance profiles to other regions. Additionally, detailed clinical data such as patient demographics, underlying diseases, clinical course, treatment, and prognosis were not obtained in this surveillance study, which prevented the analysis of correlations between clinical outcomes and pathogens or clinically important resistance phenotypes.
Conclusion
The study revealed a concerning prevalence of MDR strains isolated from neonatal sepsis in the central region of China, surpassing the national average level. This poses significant challenges to clinical diagnosis and treatment, emphasizing the need to identify effective prevention and treatment strategies. It is crucial to explore the local epidemiology of resistant pathogens in EOS and LOS to establish empirical therapies that are effective in neonatal intensive care units.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved the Hospital Ethics Review Board of Henan Children’s Hospital. We confirmed that all the data were anonymized and maintained with confidentiality; therefore, the requirement for informed consent has been waived because of the retrospective nature of the current study.
Acknowledgments
The authors would like to thank Mrs Junwen Yang (Microbiology Section, Department of Laboratory, Children’s Hospital Affiliated to Zhengzhou University) for assistance in obtaining pathogen and patient data.
Funding
This work was supported by the Key Research, Development, and Promotion Projects of Henan Province (222102310171, 222102310328 and 222102310067), and Medical Science and Technology Project of Henan Province (LHGJ20210636 and LHGJ20200607).
Disclosure
The authors report they have no potential conflicts of interest to disclose for this work.
References
1. Fleiss N, Coggins SA, Lewis AN, et al. Evaluation of the neonatal sequential organ failure assessment and mortality risk in preterm infants with late-onset infection. JAMA Netw Open. 2021;4(2):e2036518.
2. Shane AL, Sánchez PJ, Stoll BJ. Neonatal sepsis. Lancet. 2017;390(10104):1770–1780.
3. Wang H, Abajobir AA, Abate KH. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1084–1150.
4. Vos T, Lim SS, Abbafati C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
5. He C, Liu L, Chu Y, et al. National and subnational all-cause and cause-specific child mortality in China, 1996-2015: a systematic analysis with implications for the Sustainable Development Goals. Lancet Glob Health. 2017;5(2):e186–e197.
6. Dong Y, Basmaci R, Titomanlio L, et al. Neonatal sepsis: within and beyond China. Chin Med J. 2020;133(18):2219–2228.
7. Juliana AE, Holband N, Lissone NPA, et al. Incidence of early and late onset neonatal sepsis in suriname: a national tertiary hospital birth-cohort study. Pediatr Infect Dis J. 2022;41(12):1007–1011.
8. Yadav P, Yadav SK. Progress in Diagnosis and Treatment of Neonatal Sepsis: a Review Article. JNMA J Nepal Med Assoc. 2022;60(247):318–324.
9. Mariani M, Parodi A, Minghetti D, et al. Early and Late Onset Neonatal Sepsis: epidemiology and Effectiveness of Empirical Antibacterial Therapy in a III Level Neonatal Intensive Care Unit. Antibiotics. 2022;11(2):65.
10. Pace E, Yanowitz T. Infections in the NICU: neonatal sepsis. Semin Pediatr Surg. 2022;31(4):151200.
11. Ren Y, Chakraborty T, Doijad S, et al. Multi-label classification for multi-drug resistance prediction of Escherichia coli. Comput Struct Biotechnol J. 2022;20:1264–1270.
12. Golli AL, Cristea OM, Zlatian O, et al. Prevalence of Multidrug-Resistant Pathogens Causing Bloodstream Infections in an Intensive Care Unit. Infect Drug Resist. 2022;15:5981–5992.
13. Robledo J, Maldonado N, Robledo C, et al. Changes in Antimicrobial Resistance and Etiology of Blood Culture Isolates: results of a Decade (2010-2019) of Surveillance in a Northern Region of Colombia. Infect Drug Resist. 2022;15:6067–6079.
14. Hu F, Yuan L, Yang Y, et al. A multicenter investigation of 2773 cases of bloodstream infections based on China antimicrobial surveillance network (CHINET). Front Cell Infect Microbiol. 2022;12:1075185.
15. Haddad S, Jabbour JF, Hindy JR, et al. Bacterial bloodstream infections and patterns of resistance in patients with haematological malignancies at a tertiary centre in Lebanon over 10 years. J Glob Antimicrob Resist. 2021;27:228–235.
16. Simonsen KA, Anderson-Berry AL, Delair SF, et al. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014;27(1):21–47.
17. National Institute for Health and Care Excellence. Clinical Guidelines. Neonatal Infection: Antibiotics for Prevention and Treatment. London: National Institute for Health and Care Excellence (NICE) Copyright © NICE 2021; 2021.
18. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281.
19. Rafailidis PI, Kofteridis D. Proposed amendments regarding the definitions of multidrug-resistant and extensively drug-resistant bacteria. Expert Rev Anti Infect Ther. 2022;20(2):139–146.
20. Fraimow HS, Tsigrelis C. Antimicrobial resistance in the intensive care unit: mechanisms, epidemiology, and management of specific resistant pathogens. Crit Care Clin. 2011;27(1):163–205.
21. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
22. Ren Z, Yang S, Han J, et al. Reduction of antibiotic use and multi-drug resistance bacteria infection in neonates after improvement of antibiotics use strategy in a level 4 neonatal intensive care unit in southern China. Eur J Clin Microbiol Infect Dis. 2023;42(1):87–98.
23. Panigrahi K, Pathi BK, Poddar N, et al. Colistin resistance among multi-drug resistant gram-negative bacterial isolates from different clinical samples of ICU patients: prevalence and clinical outcomes. Cureus. 2022;14(8):e28317.
24. Al-Sunaidar KA, Aziz NA, Hassan Y, et al. Association of multidrug resistance bacteria and clinical outcomes of adult patients with sepsis in the intensive care unit. Trop Med Infect Dis. 2022;7(11):98.
25. Kim HJ, Oh DK, Lim SY, et al. Antibiogram of multidrug-resistant bacteria based on sepsis onset location in Korea: a multicenter cohort study. J Korean Med Sci. 2023;38(10):e75.
26. Legese MH, Asrat D, Swedberg G, et al. Sepsis: emerging pathogens and antimicrobial resistance in Ethiopian referral hospitals. Antimicrob Resist Infect Control. 2022;11(1):83.
27. Qiu Y, Yang J, Chen Y, et al. Microbiological profiles and antimicrobial resistance patterns of pediatric bloodstream pathogens in China, 2016-2018. Eur J Clin Microbiol Infect Dis. 2021;40(4):739–749.
28. Oxman D, Lohr K, Gupta E, et al. Incidence of multidrug resistant infections in emergency department patients with suspected sepsis. Am J Med Sci. 2020;360(6):650–655.
29. Størdal EH, Solevåg AL, Bjørnholt JV, et al. Sepsis treatment options identified by 10-year study of microbial isolates and antibiotic susceptibility in a level-four neonatal intensive care unit. Acta Paediatr. 2022;111(3):519–526.
30. Wang J, Zhang H, Yan J, et al. Literature review on the distribution characteristics and antimicrobial resistance of bacterial pathogens in neonatal sepsis. J Matern Fetal Neonatal Med. 2022;35(5):861–870.
31. Zhou W, Niu D, Gao S, et al. Prevalence, biofilm formation, and mass spectrometric characterization of linezolid-resistant Staphylococcus capitis isolated from a tertiary hospital in China. J Glob Antimicrob Resist. 2023:56.
32. Gowda H, Norton R, White A, et al. Late-onset Neonatal Sepsis-A 10-year Review From North Queensland, Australia. Pediatr Infect Dis J. 2017;36(9):883–888.
33. Ji H, Yu Y, Huang L, et al. Pathogen Distribution and Antimicrobial Resistance of Early Onset Sepsis in Very Premature Infants: a Real-World Study. Infect Dis Ther. 2022;11(5):1935–1947.
34. Köstlin-Gille N, Härtel C, Haug C, et al. Epidemiology of early and late onset neonatal sepsis in very low birthweight infants: data from the German neonatal network. Pediatr Infect Dis J. 2021;40(3):255–259.
35. França A. The Role of Coagulase-Negative Staphylococci Biofilms on Late-Onset Sepsis: current Challenges and Emerging Diagnostics and Therapies. Antibiotics. 2023;12(3):23.
36. Wong JR, Bauer KA, Mangino JE, et al. Antimicrobial stewardship pharmacist interventions for coagulase-negative staphylococci positive blood cultures using rapid polymerase chain reaction. Ann Pharmacother. 2012;46(11):1484–1490.
37. Aleidan FAS, Alkhelaifi H, Alsenaid A, et al. Incidence and risk factors of carbapenem-resistant Enterobacteriaceae infection in intensive care units: a matched case-control study. Expert Rev Anti Infect Ther. 2021;19(3):393–398.
38. Chaurasia S, Sivanandan S, Agarwal R, et al. Neonatal sepsis in South Asia: huge burden and spiralling antimicrobial resistance. BMJ. 2019;364:k5314.
39. Liu J, Fang Z, Yu Y, et al. Pathogens distribution and antimicrobial resistance in bloodstream infections in twenty-five neonatal intensive care units in China, 2017-2019. Antimicrob Resist Infect Control. 2021;10(1):121.
40. Narimisa N, Goodarzi F, Bavari S. Prevalence of colistin resistance of Klebsiella pneumoniae isolates in Iran: a systematic review and meta-analysis. Ann Clin Microbiol Antimicrob. 2022;21(1):29.
41. Ardebili A, Izanloo A, Rastegar M. Polymyxin combination therapy for multidrug-resistant, extensively-drug resistant, and difficult-to-treat drug-resistant gram-negative infections: is it superior to polymyxin monotherapy? Expert Rev Anti Infect Ther. 2023;21(4):387–429.
42. Liu YC, Lu CY, Yen TY, et al. Clinical characteristics and outcomes of carbapenem-resistant Enterobacterales bacteremia in pediatric patients. J Microbiol Immunol Infect. 2023;56(1):84–92.
43. Della Rocca MT, Panetta V, Durante A, et al. Pathogens distribution and antimicrobial resistance pattern of blood stream infections in Southern Italian hospital, 2016-2021 surveillance. New Microbiol. 2023;46(1):29–36.
44. Chen CH, Wu PH, Lu MC, et al. National surveillance of antimicrobial susceptibilities to ceftaroline, dalbavancin, telavancin, tedizolid, eravacycline, omadacycline, and other comparator antibiotics, and genetic characteristics of bacteremic Staphylococcus aureus isolates in adults: results from the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) program in 2020. Int J Antimicrob Agents. 2023;61(4):106745.
45. Ohnuma T, Chihara S, Costin B, et al. Association of Appropriate Empirical Antimicrobial Therapy With In-Hospital Mortality in Patients With Bloodstream Infections in the US. JAMA Netw Open. 2023;6(1):e2249353.
46. Austin ED, Sullivan SS, Macesic N, et al. Reduced Mortality of Staphylococcus aureus Bacteremia in a Retrospective Cohort Study of 2139 Patients: 2007-2015. Clin Infect Dis. 2020;70(8):1666–1674.
47. Gao K, Fu J, Guan X, et al. Incidence, Bacterial Profiles, And Antimicrobial Resistance Of Culture-Proven Neonatal Sepsis In South China. Infect Drug Resist. 2019;12:3797–3805.
48. Kufel WD, Parsels KA, Blaine BE, et al. Vancomycin plus ceftaroline for persistent methicillin-resistant Staphylococcus aureus bacteremia. Pharmacotherapy. 2023;43(1):15–23.
49. Patel D, Brown ML, Edwards S, et al. Outcomes of Daptomycin Plus Ceftaroline Versus Alternative Therapy for Persistent Methicillin-resistant Staphylococcus aureus (MRSA) Bacteraemia. Int J Antimicrob Agents. 2023;61(3):106735.
50. Jena B, Singh SS, Behera SK, et al. To decipher the phytochemical agent and mechanism for Urginea indica mediated green synthesis of Ag nanoparticles and investigation of its antibacterial activity against Methicillin-resistant Staphylococcus aureus. Environ Res. 2023;216(Pt 4):114700.
51. Li T, Li X, Gao K, et al. Changes in pathogen distribution in the blood culture of neonates before and after the COVID-19 pandemic, Henan, China. J Infect. 2023;86(2):154–225.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.