Back to Journals » International Journal of General Medicine » Volume 19
Prevalence of HSV-1, HSV-2, EBV, and HHV-8 Co-Infections Among HPV-Positive Women: A Cross-Sectional Study from Iran
Authors Safarnezhad Tameshkel F, Salimi Jeda A, Sadat Ghaemi M, Ataei-Pirkooh A, Motamedaria P, Hemmasi G, Motevasselian M, Panahi Z, Karbalaie Niya MH ![]()
Received 23 February 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:19 602814
DOI https://doi.org/10.2147/IJGM.S602814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Fahimeh Safarnezhad Tameshkel,1 Ali Salimi Jeda,2 Mozhan Sadat Ghaemi,3 Angila Ataei-Pirkooh,4 Parastoo Motamedaria,4 Gholamreza Hemmasi,5 Mahtab Motevasselian,6,7 Zahra Panahi,1 Mohammad Hadi Karbalaie Niya1,4
1Gastrointestinal and Liver Diseases Research Center, Iran University of Medical Sciences, Tehran, Iran; 2Applied Virology Research Center, Biomedicine Technologies Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran; 3Department of Internal Medicine, School of Medicine, Iran University of Medical Sciences, Tehran, Iran; 4Department of Virology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran; 5Colorectal Research Center, Iran University of Medical Sciences, Tehran, Iran; 6Department of Obstetrics and Gynecology, School of Medicine, Shahid Akbar-Abadi Hospital and Firoozgar Hospital, Iran University of Medical Sciences, Tehran, Iran; 7Firoozgar Clinical Research and Development Center (FCRDC), Iran University of Medical Sciences, Tehran, Iran
Correspondence: Mohammad Hadi Karbalaie Niya, Gastrointestinal and Liver Diseases Research Center, Iran University of Medical Sciences, Tehran, 14496-14535, Iran, Tel +989354266744, Email [email protected]
Background: Interactions between human papillomavirus (HPV) and co-infecting herpesviruses remain incompletely understood. This study assessed the prevalence of HSV-1, HSV-2, Epstein–Barr virus (EBV), and HHV-8 among HPV-positive women in Iran, and evaluated associations with HPV genotypic risk groups and genotype multiplicity.
Methods: This cross-sectional study analyzed 303 residual cervical cytology samples from HPV-positive women. Herpesviruses were detected using multiplex real-time PCR. Associations between herpesvirus positivity and HPV variables were examined using Logistic regression, Fisher’s Exact Test and nonparametric statistics.
Results: Co-infection of HPV with herpesviruses were detected in 20 of 303 samples (6.6%; 95% CI: 4.1– 10.0), including HSV-1 in 2 samples (0.7%), HSV-2 in 10 samples (3.3%), EBV in 8 samples (2.6%), and HHV-8 in none of the samples. No significant associations were found between herpesvirus positivity and HPV risk group or HPV genotype multiplicity (p> 0.05). Multivariable models did not identify independent predictors; analyses were limited by the low number of herpesvirus-positive cases and wide confidence intervals.
Conclusion: Co-infection of HPV with herpesviruses were uncommon among HPV-positive women and were not measurably associated with HPV genotype patterns. The low event frequency and cytology-based sampling likely contributed to nondetection of associations. Studies using tissue-based sampling, HPV–herpesvirus viral load, and high-grade lesions are needed to clarify potential viral synergism.
Keywords: human papillomavirus, herpesviridae, co-infection, cervical cytology, multiplex real-time PCR, Iran/epidemiology
Introduction
Viral infections of the female genital tract represent a significant burden on women’s health worldwide and are major contributors to inflammatory diseases, pre-neoplastic changes, and malignancies.1 Among these infections, the Herpesviridae family and Human Papillomavirus (HPV) are of particular importance because of their high prevalence and oncogenic potential.2 High-risk HPV genotypes are well established as essential etiological agents in cervical intraepithelial neoplasia (CIN) and cervical cancer, accounting for over 99% of cases.3 However, HPV infection alone is often insufficient for cervical carcinogenesis. Most HPV infections are transient and are cleared by the immune system, with only a small proportion progressing to high-grade lesions or invasive cancer.3 This has led to increasing interest in viral or host co-factors that may promote HPV persistence, immune evasion, or signaling changes that facilitate progression to neoplasia.4
Over the past several decades, increasing evidence has suggested that co-infections with other sexually transmitted viruses—particularly herpesviruses such as HSV-1, HSV-2, Epstein–Barr virus (EBV), and Kaposi’s Sarcoma–Associated Herpesvirus (KSHV/HHV-8)—may modify HPV-associated disease outcomes.5 These viruses share similar modes of transmission and are capable of establishing lifelong latency.4,6 Their known effects on epithelial integrity, inflammation, oxidative stress, and immune modulation make them biologically plausible contributors to HPV-related pathogenesis.4,6
HSV-2, the classical cause of genital herpes, has long been investigated as a potential co-factor in cervical disease. HSV-2 infection can cause epithelial disruption and chronic cervicitis, which may facilitate HPV entry or persistence.7 Persistent infection with high-risk human papillomavirus (HPV) is the principal and unequivocally established etiological factor associated with cervical premalignant lesions and cervical cancer.8,9 EBV latent proteins such as LMP1 activate inflammatory and survival pathways (eg, NF-κB, JAK/STAT), which may enhance HPV oncogene expression or contribute to epigenetic changes associated with neoplastic progression.9,10 KSHV/HHV-8 is uncommon in cervical tissues but has been identified in subsets of HPV-positive carcinomas in certain regions. Its viral proteins (LANA-1, vIL-6, vFLIP) promote cellular survival and angiogenesis.11,12 Although evidence for KSHV involvement in cervical disease remains weak overall, biological plausibility exists based on its molecular functions.11,12
Despite these mechanistic hypotheses, epidemiological evidence regarding co-infection of HPV with herpesviruses in HPV-positive women remains inconsistent.13 Differences in study designs, diagnostic sensitivity, sample type (liquid cytology vs biopsy), and population characteristics likely contribute to the conflicting findings across published studies. In Iran, the distribution of HPV genotypes has been documented in several regions; however, systematic evaluation of co-infection of HPV with herpesviruses among HPV-positive women remains limited. Importantly, few studies have examined whether co-infections correlate with HPV risk groups (high-risk vs low-risk) in clinical, non-cancer populations.
Therefore, the present study was conducted to determine the prevalence of HSV-1, HSV-2, EBV, and HHV-8 in HPV-positive women attending a papilloma clinic. Additionally, this study evaluates whether co-infection of HPV with herpesviruses is associated with HPV risk categories or HPV genotype multiplicity in cytology-based samples, providing new regional data for early-stage HPV-positive populations.
Materials and Methods
Study Design and Population
This cross-sectional study was conducted to investigate co-infection with herpesviruses among HPV-positive women. Samples were collected from women attending the outpatient papilloma clinic affiliated with Iran University of Medical Sciences, Tehran, Iran, between April 2022 and December 2023. Residual liquid-based cytology specimens were archived following routine HPV genotyping procedures. A total of 303 residual cervical cytology samples from patients with confirmed HPV-PCR positivity were included for Herpesviruses co-infection testing (Figure 1).
 |
Figure 1 STROBE flow diagram of participant selection and inclusion in co-infection of HPV with herpesviruses analysis. |
Inclusion criteria were: female sex, positive HPV PCR result, completed consent form, and completed questionnaire. Exclusion criteria included male patients, refusal to participate, insufficient sample volume, and negative HPV test results. The cross-sectional design does not permit causal inference; therefore, the study aims were limited to evaluating associations and prevalence patterns rather than progression or temporal outcomes. According to Bethesda System recommendations high grade squamous intraepithelial lesion (HSIL) used for CIN-2 and higher grades, and low-grade squamous intraepithelial lesions (LSIL) for CIN-1 and lower grades of cervical lesions.
Data Collection
Demographic and clinical information was collected using a questionnaire validated by a panel of specialists and completed by reviewing patient records. All participants provided informed consent. The study protocol was approved by the institutional ethics committee of the affiliated Iran University of Medical Sciences, Tehran, Iran and was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Sample Storage and Nucleic Acid Extraction
Cervical cytology samples stored at –20°C were thawed and briefly centrifuged at 3000 rpm for 30 seconds. A 200 µL aliquot of the cell pellet suspension (after discarding the supernatant) was used for DNA extraction using the VirAll Kit (ROJE Technologies, Iran), following the manufacturer’s instructions. DNA concentration and purity were measured using a NanoDrop spectrophotometer (OD 260/280 ratio 1.8–2.2 considered acceptable). The use of liquid-based cytology samples may reduce sensitivity for detecting latent herpesviruses; this limitation is acknowledged.
Herpesvirus Detection by Multiplex Real-Time PCR
Herpesvirus detection was performed using the GA Herpesviridae Multiplex Real-Time PCR Kit (Geneova, Iran), according to the manufacturer’s instructions. The assay simultaneously detects HSV-1, HSV-2, EBV, HHV-8, through multiplex fluorescent probe channels. Amplification was performed using a standardized thermal cycling protocol consisting of 40 amplification cycles. According to the manufacturer protocol, samples with Cq values <35 and a characteristic sigmoid amplification curve were considered positive, while values between 35 and 40 were interpreted as borderline depending on technical and clinical context. The reported analytical sensitivity and specificity of the kit are 99% and 98%, respectively. According to manufacturer documentation, the lower limit of detection of both the VirAll HPV Genotyping Kit and the GA Herpesviridae Multiplex PCR Kit was approximately 100 viral copies per reaction under validated assay conditions.
The assay uses three reaction tubes covering four viral targets and an internal control. Each reaction contained 15 µL of master mix and 5 µL of extracted DNA. Cycling was performed on a Rotor-Gene 6000 system with: 95°C for 10 min, 40 cycles of 95°C for 15s and 60°C for 60s. A target was considered positive if its Cq ≤ 40 with a valid amplification curve. Because several viral targets had very low detection counts, the kit’s reported sensitivity and specificity cannot be independently validated within this dataset.
Operational Definition of Co-Infection
Co-infection was defined as detection of one or more herpesviruses in an HPV-positive sample. No viral load quantification was performed; results reflect presence/absence only. Because EBV may also persist within circulating lymphocytes, detection of EBV DNA in cervical cytology samples may partially reflect latently infected inflammatory cells rather than exclusively epithelial infection.
HPV Genotyping
HPV genotyping was performed based on patient laboratory records using a multiplex PCR panel capable of detecting 38 HPV genotypes, including high-risk types (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, and 73) and low-risk types (HPV-6, 11, 40, 42, 43, 44, 54, 61, 62, 67, 70, 74, 81, 83, 84, and 91). Genotypes were grouped as high-risk (HR), low-risk (LR), or mixed HR/LR infections. Multiplicity of HPV infection was categorized as single genotype, two to four genotypes, or more than four genotypes.
Statistical Analysis
Statistical tests were conducted using SPSS. Associations between co-infection of HPV with herpesviruses and HPV risk groups were evaluated using Chi-square or Fisher’s Exact Test as appropriate. Because several contingency tables included expected cell counts <5, Fisher’s Exact Test replaced Chi-square where applicable to ensure statistical validity. Non-parametric tests (Kruskal–Wallis and Wilcoxon rank-sum) were used to compare HPV multiplicity between co-infected and non–co-infected groups. Exact 95% confidence intervals (Clopper–Pearson) were calculated for all prevalence estimates.
Multivariable logistic regression models were constructed to evaluate predictors of co-infection of HPV with herpesviruses using only variables collected directly from participants. The primary outcome was “any co-infection of HPV with herpesviruses” (HSV-1, HSV-2, EBV, or HHV-8). Due to low event counts, Firth’s bias-reduced logistic regression was applied to reduce small-sample bias. Covariates included age (continuous), smoking status (yes/no), alcohol use (yes/no), number of lifetime sexual partners (ordinal), HPV genotype multiplicity (1, 2–4, ≥5 types), and HPV risk group (high-risk, low-risk, mixed). Separate models were also fitted for HSV-2 and EBV as outcomes. Variables were selected a priori based on biological plausibility and prior literature. Cases with missing data on lifetime sexual partners were excluded from regression analyses using complete-case analysis. Multiple imputation was considered; however, the limited number of herpesvirus-positive outcomes reduced the statistical reliability of imputed models.
Results
Demographic and Clinical Characteristics
A total of 303 HPV-positive cervical samples were analyzed. Participants ranged in age from 17 to 61 years. The mean age of participants was 32.8 ± 9.4 years (95% CI: 31.7–33.8). Most patients (60.5%) were between 25–40 years old, followed by those aged 18–25 (19.7%), whereas participants under 18 (1.6%) and over 55 (2.0%) represented the smallest groups. Participant selection and study workflow are summarized in Figure 1.
Sexual history analysis indicated that over the previous two years, 47.5% reported one sexual partner, 23.6% none, 16.8% two partners, 7.5% three partners, and 3.6% four to nine partners; 1.1% reported more than ten partners. Regarding lifetime sexual partners, 74.3% reported 2–5 partners, 5.4% reported 6–9 partners, another 5.4% only one partner, and 3.0% more than ten partners; 11.8% did not report. Most participants (67.4%) had no history of smoking, 32.5% were smokers, 76.6% did not consume alcohol, and 23.3% did. Drug use was reported by 1.6%.
Pap smear data (n = 162) showed: 67.9% normal (95% CI: 60.3–74.7), 16.7% inflammation (95% CI: 11.5–23.4), 13.0% ASC-US (95% CI: 8.2–19.6), 1.9% ASC-H (95% CI: 0.3–6.1), 0.6% cervicitis (95% CI: 0.03–3.6). Colposcopy findings (n = 36) revealed: 38.9% LSIL, 36.1% normal, 16.7% cervicitis, 8.3% HSIL.
Pap smear and colposcopy results were available only for patients who underwent additional clinical evaluation according to routine physician-directed screening and follow-up protocols; therefore, these data were not uniformly available for the entire cohort and may reflect selection bias toward higher-risk patients. Pap smear and colposcopy data were reviewed from patient medical records. Cytological diagnoses were extracted from official pathology records reviewed by experienced cytopathologists.
HPV Genotype Distribution and Co-Infections
Of the 303 HPV-positive samples, 45.2% had high-risk (HR) genotypes only (95% CI: 39.5–51.0), 27.7% low-risk (LR) only (95% CI: 22.7–33.2), and 27.1% mixed HR/LR types (95% CI: 22.2–32.6).
The most prevalent types were: HPV-16: 18.8% (95% CI: 14.6–23.7), HPV-53: 14.5% (95% CI: 10.9–19.1), HPV-52: 9.9% (95% CI: 6.9–14.1), HPV-6: 17.8% (95% CI: 13.7–22.7) (Figure 2). Multiplicity of HPV infection: 54.5% single type (95% CI: 48.7–60.2), 40.6% 2–4 types (95% CI: 35.1–46.5), 5.0% >4 types (95% CI: 2.9–8.3). Presenting grouped HPV multiplicity was necessary to maintain adequate statistical counts for valid non-parametric comparisons. Supplementary Table S1 listed the ten most frequent HPV genotypes identified in the study population.
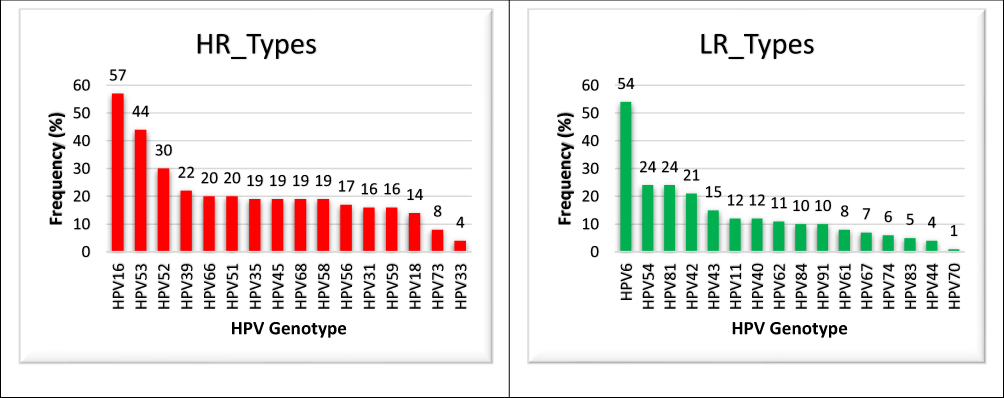 |
Figure 2 Frequency of Individual High-Risk (HR) and Low-Risk (LR) HPV Genotypes. The most prevalent types were: HPV-16: 18.8%, HPV-53: 14.5%, HPV-52: 9.9%, HPV-6: 17.8%. |
Prevalence of Co-Infection of HPV with Herpesviruses
Co-infection of HPV with herpesviruses was detected in 20 of 303 HPV-positive samples, yielding an overall prevalence of 6.6% (95% CI: 4.1–10.0) which included HSV-1 0.7% (n=2) (95% CI: 0.08–2.6), HSV-2: 3.3% (n=10) (95% CI: 1.7–6.0), EBV: 2.6% (n=8) (95% CI: 1.2–5.1), and HHV-8: 0% (n=0) (95% CI: 0–1.2). The extremely low positive counts greatly limit statistical power, increasing the risk of Type II error. Although the multiplex panel also technically supported CMV detection, CMV was not included in the predefined analytical endpoints because the study primarily focused on herpesviruses previously implicated in HPV-associated cervical epithelial alterations.
Herpesvirus Distribution According to Cytological Findings
Among the 162 participants with available Pap smear results, herpesvirus positivity was observed in both normal and abnormal cytology categories. HSV-2 and EBV positivity were more frequently detected among patients with ASC-US and inflammatory cytology compared with normal cytology; however, Fisher’s Exact Test demonstrated no statistically significant association between cytological category and herpesvirus positivity (p > 0.05). The limited number of abnormal cytology cases and herpesvirus-positive samples substantially reduced statistical power for subgroup comparisons. Histopathological biopsy data were unavailable for a substantial proportion of patients with abnormal cytology because biopsy sampling was selectively performed according to clinical colposcopic assessment and physician-directed management protocols. Consequently, subgroup comparison between LSIL and HSIL biopsy-confirmed lesions was not statistically feasible. Supplementary Table S2 shown distribution of HSV-2 and EBV according to cytological diagnosis.
Association Between Herpesvirus and HPV Risk Categories
No statistically significant associations were found between HPV risk groups (HR-only, LR-only, mixed) and the presence of any herpesvirus. Because expected cell counts were <5 in several comparisons, Fisher’s Exact Test was used instead of Chi-square for statistical validity. In this regard, any herpesvirus vs HPV risk category: p = 0.848, HSV-1 vs HPV risk category: p = 0.135, HSV-2 vs HPV risk category: p = 0.670, and EBV vs HPV risk category: p = 0.197. These p-values do not indicate true absence of association; they are non-significant primarily due to small sample sizes of herpesvirus-positive groups.
Among HSV-2-positive samples, 50.0% were detected in HR-only HPV infections, 20.0% in LR-only infections, and 30.0% in mixed HR/LR infections. EBV-positive samples were distributed as 62.5% HR-only, 12.5% LR-only, and 25.0% mixed infections.
Association Between Herpesvirus and HPV Genotype Multiplicity
Kruskal–Wallis and Wilcoxon tests showed no significant association between co-infection of HPV with herpesviruses and HPV genotype multiplicity: Any herpesvirus vs number of HPV types: p = 0.220, HSV-1 vs multiplicity: p = 0.406, HSV-2 vs multiplicity: p = 0.314, EBV vs multiplicity: p = 0.314. Grouped multiplicity (1, 2–4, >4 types) also showed no significant association (p = 0.421–0.746). Given the very small number of herpesvirus infections, these non-significant findings should be interpreted with caution.
Multivariable Adjusted Analysis
In multivariable Firth logistic regression analysis adjusting for age, smoking status, alcohol use, lifetime sexual partners, HPV multiplicity, and HPV risk group, no independent predictor of co-infection of HPV with herpesviruses reached statistical significance (Table 1). Wide confidence intervals reflected the low frequency of herpesvirus-positive cases and limited statistical power. Similarly, the HSV-2–specific model did not identify any significant independent predictors after adjustment (Table 2). Age and HPV multiplicity showed weak positive trends, but these did not reach significance. The EBV model was underpowered (n=8 positives), and no adjusted associations could be reliably estimated (Table 3).
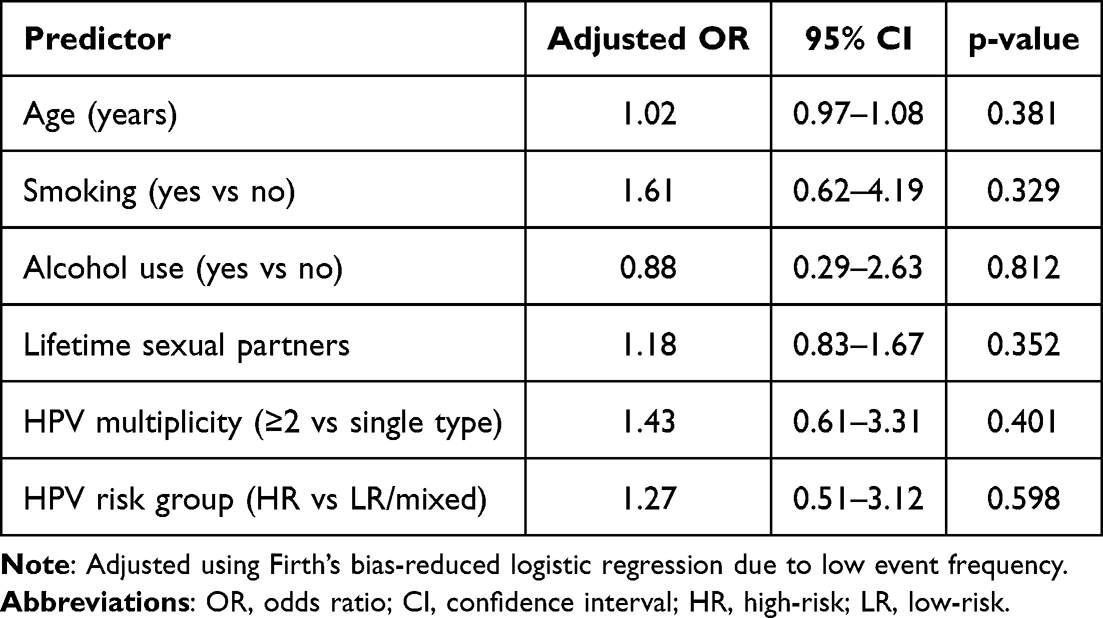 |
Table 1 Firth Logistic Regression Analysis for Predictors of Any Co-Infection of HPV with Herpesviruses (n = 20 Positive Cases) |
 |
Table 2 Firth Logistic Regression Analysis for Predictors of HSV-2 Positivity (n = 10 Positive Cases) |
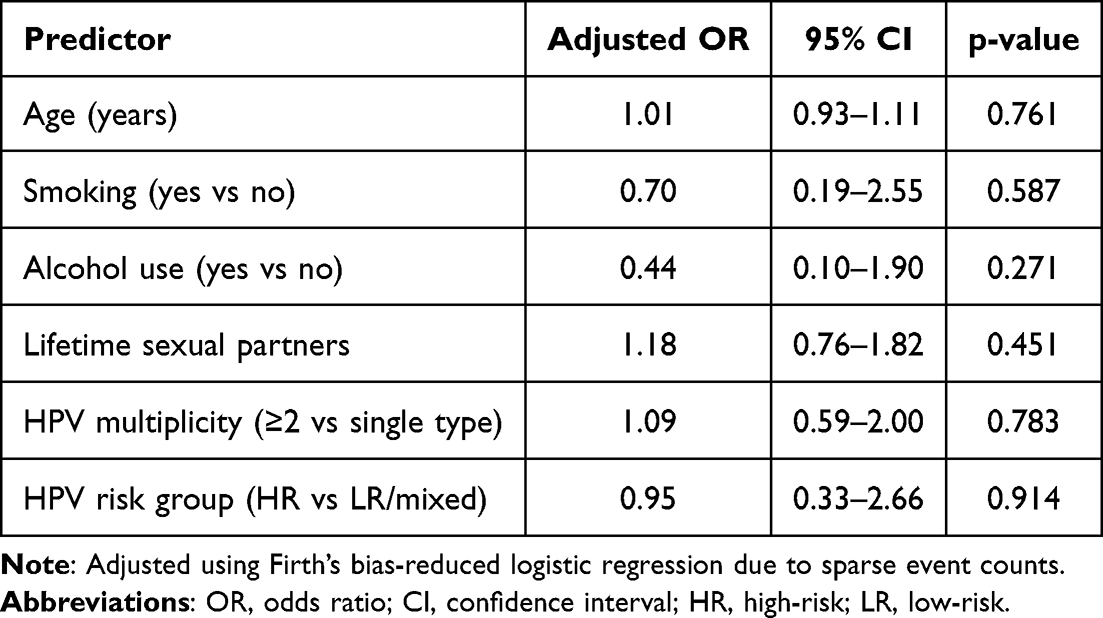 |
Table 3 Firth Logistic Regression Analysis for Predictors of EBV Positivity (n = 8 Positive Cases) |
Discussion
This cross-sectional study evaluated co-infection patterns between HPV and four herpesviruses (HSV-1, HSV-2, EBV, HHV-8) in a cohort of 303 HPV-positive women. The overall prevalence of co-infection of HPV with herpesviruses was low (6.6%), and no statistically significant associations were observed between herpesvirus positivity and HPV risk groups or HPV genotype multiplicity.While these findings align with several international reports from non-cancer populations, they also closely resemble patterns reported in multiple regional Iranian studies.
We additionally evaluated herpesvirus distribution according to cytological findings. Although HSV-2 and EBV were numerically more common among ASC-US and inflammatory cytology categories than among normal smears, these differences were not statistically significant. The low number of herpesvirus-positive samples and the predominance of normal cytology likely limited the ability to detect meaningful associations. Nevertheless, the observed trend is biologically plausible because inflammatory epithelial alterations may facilitate viral persistence and local immune dysregulation.
Accordingly, the absence of statistically significant associations in this study should not be interpreted as definitive evidence against biological interaction between HPV and herpesviruses.
The adjusted analyses did not identify significant associations between demographic or virological factors and herpesvirus positivity. However, these models were heavily constrained by the low frequency of co-infection of HPV with herpesviruses, which limits the interpretability of adjusted odds ratios. The lack of significant findings should therefore be viewed as a consequence of insufficient statistical power rather than evidence of true absence of association.
Several prior investigations in Iran provide important context for interpreting our results. Importantly, Joharinia et al reported that EBV co-infection with high-risk HPV genotypes, particularly HPV-16, HPV-18, and HPV-31, was significantly more frequent in HSIL and squamous cell carcinoma compared with LSIL lesions (p = 0.044). These findings suggest that herpesvirus co-infection may be more strongly associated with later stages of cervical disease progression rather than with early HPV infection alone. Therefore, the absence of significant associations in our predominantly non-premalignant cohort should be interpreted cautiously.14 Joharinia et al reported that EBV/HPV co-infection was significantly more frequent in HSIL and squamous cell carcinoma compared with LSIL samples (p = 0.044), suggesting that herpesvirus involvement may become more relevant during advanced stages of cervical disease progression rather than early HPV-positive states. Similarly, Baldauf et al found no significant link between HPV-16/18 and HSV/CMV in cervical biopsies from patients with neoplasia and controls, a conclusion that aligns with our own.15 Also, the comparison with Lau et al should be interpreted cautiously because their investigation focused specifically on endocervical adenocarcinoma specimens rather than non-premalignant cytology samples. Consequently, direct comparison with the present cohort is limited by substantial differences in disease stage, histopathological subtype, and tissue source.16
Aromseree et al found a significant increase in EBV/HR-HPV co-infection in HSIL and carcinoma, suggesting EBV may act as a co-factor.17 This is reinforced by Khenchouche et al and Muhsin et al, who reported high rates of EBV and CMV co-infection in squamous cell carcinoma, proposing these viruses contribute to cancer progression and may indicate a poor prognosis.18,19
Additionally, several previous investigations have evaluated the interaction between HPV and herpesviruses in cervical disease progression with variable findings across different populations and sample types. In a recent tissue-based real-time PCR study, Bakır et al reported detectable co-infection rates of high-risk HPV with HSV-2 and HHV-8 in cervical biopsy specimens,20 supporting the hypothesis that herpesviruses may contribute to local epithelial dysregulation in established cervical lesions. However, unlike the present study, their analysis focused on biopsy-confirmed tissue samples rather than residual cytology specimens, which may provide higher viral yield and improved sensitivity for latent viral detection.
Similarly, Ahmadi et al evaluated HSV-2 together with HPV-16 and HPV-18 in Iranian cervical lesion samples and reported significantly higher HSV-2 prevalence among HPV-positive abnormal lesions compared with normal controls,21 suggesting a possible cooperative role in cervical epithelial progression. In another Iranian investigation, Chavoshpour-Mamaghani et al demonstrated increasing Epstein–Barr virus prevalence across normal, premalignant, and malignant cervical samples, further supporting the possibility that EBV involvement may become more prominent during later stages of neoplastic transformation rather than during early HPV infection alone.22
Collectively, these findings suggest that differences in sample source (cytology versus biopsy), lesion severity, viral burden, and population characteristics may substantially influence reported herpesvirus co-infection frequencies across studies.
Additional evidence from Iranian cohorts also supports this interpretation. Regarding HHV-8, our finding of no detectable HHV-8-positive samples differs from the study by Chavoshpour-Mamaghani et al, who reported HHV-8 infection in 14.5% (26/179) of normal cervical specimens among Iranian women. Differences in geographical sampling, assay sensitivity, tissue processing methods, and patient characteristics may partially explain this discrepancy. Additionally, latent herpesvirus detection may be reduced in residual cytology samples compared with tissue biopsy specimens.23 Their findings reinforce a stage-dependent pattern: HHV-8 appears more frequently in invasive lesions, potentially reflecting tissue tropism or microenvironmental differences that cytological sampling cannot capture. Similarly, our EBV and HHV-8 prevalence rates were substantially lower than those reported by Sosse et al in cervical cancer patients. However, this difference is expected because their cohort consisted exclusively of malignant cervical carcinoma cases, whereas the present study predominantly included non-premalignant outpatient screening samples. Therefore, the lower herpesvirus detection rates observed in our cohort should not be interpreted as contradictory but rather as potentially reflecting disease-stage differences in viral enrichment and tissue involvement during cervical carcinogenesis.24
Another important Iranian study by Mojarrad et al documented genotype distribution among HPV-positive individuals in Urmia.13 While this study did not evaluate herpesviruses, its findings are directly relevant: They reported high frequencies of HPV-16, HPV-52, and HPV-53—strikingly similar to our genotype distribution—which reinforces the regional consistency of HPV epidemiology and suggests that the genotype landscape in Iran may be relatively stable across provinces. These similarities indicate that the low co-infection of HPV with herpesviruses prevalence in our cohort is unlikely to be due to unusual HPV genotype patterns.
An important finding in our cohort was the relatively high prevalence of HPV-53 (14.5%). HPV-53 is considered a probable or potentially high-risk genotype but is not included in currently available prophylactic HPV vaccines. This observation may have epidemiological importance because persistent circulation of non-vaccine HPV genotypes could influence future genotype replacement patterns and co-infection dynamics in partially vaccinated populations.13
Comparisons to international studies highlight additional contrasts. While we found minimal EBV involvement, several studies from North Africa and Southeast Asia have reported substantial EBV/HPV co-detection in either high-grade lesions or cervical cancer. Khenchouche et al, for example, identified EBV in Algerian cervical carcinoma samples with a relatively high frequency.18 The disparity between our findings and these reports underscores the possibility that EBV’s oncogenic contribution may emerge primarily in advanced disease, whereas its presence in routine cytology samples—typical of early-stage patients in Iran—appears minimal.
In examining HSV-2, our detection rate of 3.3% is slightly lower than Iran’s national HSV-2 prevalence estimates among women of reproductive age. Joharinia et al14 similarly found a low rate of HSV co-detection in HPV-positive cases from their region. Zhao et al25 suggested a potential role for HSV-2 in cervical carcinogenesis. Taken together, these findings suggest that active HSV replication in the cervix is relatively uncommon in Iranian clinical settings, possibly reflecting sociocultural patterns, sexual behavior norms, or lower background HSV-2 prevalence in certain provinces compared to global averages. The primary reason for these differences is likely the clinical stage of the sampled population. Our study comprised an HPV-positive clinical cohort with a low frequency of advanced lesions (only 36 colposcopies, with LSIL being the most common finding), whereas the studies finding associations focused specifically on cancerous or high-grade pre-cancerous tissues. The oncogenic role of herpesviruses may become prominent only in later stages of disease progression, a context our study was not designed to capture.
Methodological differences also explain variation across studies. Iranian research often relies on nested PCR for herpesvirus detection,23 which is more sensitive than the multiplex real-time PCR used here. Thus, differences in primer specificity, sample type (tissue vs liquid-based cytology), and viral load thresholds likely contribute to the lower detection rates observed in our study. Geographical variations in viral endemicity (eg, Iran vs Morocco vs France) are another crucial factor influencing prevalence rates.
The present study provides valuable insights into co-infection dynamics in a real-world Iranian clinical cohort. With over 300 HPV-positive cases and standardized PCR-based detection, it offers one of the more comprehensive cytology-based assessments of co-infection of HPV with herpesviruses in the region. However, the low frequency of herpesvirus positivity significantly restricts inferential power. It remains plausible that true interactions exist but were not detectable under these sampling conditions.
The interpretation of our findings must be considered in light of several methodological limitations. Post-hoc assessment indicated that the present sample size and event frequency (20 herpesvirus-positive cases) provided limited statistical power to detect small intergroup differences (<5%) between HPV risk categories, increasing the possibility of Type II error. Iranian studies showing higher herpesvirus rates frequently used biopsy tissue rather than cytology (eg, Chavoshpour-Mamaghani et al, 2021). Therefore, our findings likely reflect the sensitivity limits of cytology for detecting latent herpesviruses. Most participants showed normal or low-grade cytology. This contrasts with Iranian cancer-based studies where herpesviruses—especially EBV and HHV-8—are substantially more common. With HSV-1 (n=2), HSV-2 (n=10), and EBV (n=8), statistical comparisons lack stability, and effect estimates cannot be interpreted as evidence of absence. Several Iranian labs emphasize PCR viral load to distinguish latent vs active herpesvirus infection, which was not available here.
Latently infected herpesviruses are often present at very low copy numbers within superficial exfoliated cervical epithelial cells collected by cytology, whereas deeper epithelial or stromal compartments sampled by tissue biopsy may contain higher viral loads. Consequently, the use of residual liquid-based cytology samples may have underestimated the true prevalence of latent herpesvirus infection in this cohort. Although multiplex real-time PCR was used, quantitative viral-load analysis based on Cq values could not be consistently performed because archived laboratory records were not originally standardized for retrospective quantitative assessment. Therefore, differentiation between latent low-copy viral carriage and active viral replication was not feasible in the present study.
Type-specific HSV-1 and HSV-2 serological assays were not available in the retrospective clinical records; therefore, prior systemic exposure and distinction between genital and non-genital acquisition could not be evaluated. Information regarding prior antiviral prophylaxis or herpesvirus vaccination history was not consistently available in patients records and therefore could not be analyzed. HIV status and other immunosuppressive conditions were not systematically documented within the retrospective dataset and therefore could not be controlled for in the analyses. Separate sensitivity analysis excluding HSV-1-positive cases was not performed because only two HSV-1-positive samples were identified, limiting meaningful statistical interpretation. The relatively low prevalence of herpesvirus positivity reduced statistical power for subgroup comparisons and multivariable analyses. Inclusion of SIL and cervical cancer cohorts would substantially improve analytical robustness and disease-stage comparisons.
An additional limitation relates to potential selection bias in the availability of Pap smear and colposcopy data. These evaluations were not systematically performed for all participants and were instead obtained according to routine clinical indications and physician-directed management. As a result, patients undergoing cytological or colposcopic assessment may have disproportionately represented individuals with higher perceived clinical risk, abnormal HPV findings, or suspicious gynecological symptoms. This may have influenced the observed distribution of cytological abnormalities and limits the generalizability of subgroup analyses involving Pap smear and colposcopy findings.
Our study implications, given the collective body of Iranian studies, along with our findings. Herpesviruses appear to have a limited detectable role in early HPV-positive cytology samples in Iran, but may still contribute to oncogenic progression in later stages detectable only in tissue-based or cancer-focused research. Future Iranian research should incorporate tissue biopsies, viral load quantification, and targeted recruitment of HSIL and SCC patients to assess the possible late-stage synergy of herpesviruses and HPV.
The absence of a dedicated HSIL or cervical cancer comparison group limited the ability to directly evaluate whether herpesvirus co-infection frequencies increase with progressive cervical disease severity. Future multicenter studies incorporating biopsy-confirmed HSIL and invasive carcinoma cohorts would provide more informative comparative analysis.
Conclusion
In conclusion, co-infection of HPV with herpesviruses was relatively uncommon in this cohort of predominantly non-premalignant cervical samples. Although no statistically significant associations with HPV risk groups were identified, the findings support continued investigation of herpesvirus interactions in HPV persistence and cervical disease progression using larger longitudinal cohorts incorporating HSIL and cervical cancer populations. This growing regional evidence suggests that herpesvirus activity may be more relevant in advanced cervical lesions or tissue-based analyses than in routine screening populations. Future studies should prioritize longitudinal designs, tissue biopsies, viral load quantification, and targeted recruitment of patients with high-grade lesions (HSIL), which may better reveal potential synergistic interactions between HPV and herpesviruses during disease progression. Overall, this study provides valuable epidemiological insight from an Iranian cohort and contributes to regional data regarding HPV– co-infection of HPV with herpesviruses patterns. While co-infection of HPV with herpesviruses appear uncommon in early HPV-positive populations, their potential contribution to later stages of carcinogenesis remains an important area for continued investigation. Future studies should additionally incorporate quantitative viral-load thresholds to distinguish latent herpesvirus carriage from active viral replication. Prospective longitudinal studies evaluating whether baseline herpesvirus co-infection predicts persistent HPV infection or progression of cervical lesions over time are warranted.
Abbreviations
HPV, human papillomavirus; EBV, Epstein–Barr virus; ASC-US, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells cannot exclude HSIL; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; SCC, squamous cell carcinoma; CI, confidence intervals; CIN, cervical intraepithelial neoplasia; KSHV, Kaposi’s Sarcoma–Associated Herpesvirus; HR, High-risk; LR, Low-risk; HSV-1, Herpes simplex virus type 1; HSV-2, Herpes simplex virus type 2; HHV, Human Herpes virus; CMV, Cytomegalovirus.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. The authors support future development of standardized regional databases and public repositories for HPV and herpesvirus co-infection research to facilitate meta-analytic collaboration.
Ethics Approval
Approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.FMD.REC.1402.225).
Funding
This research received funding support from the Iran University of Medical Sciences by the grant code: 1403-2-75-30973.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haręża DA, Wilczyński JR, Paradowska E. Human papillomaviruses as infectious agents in gynecological cancers. Oncogenic properties of viral proteins. Int J Molecul Sci. 2022;23(3):1818. doi:10.3390/ijms23031818
2. Sausen DG, Shechter O, Gallo ES, et al. Herpes simplex virus, human papillomavirus, and cervical cancer: overview, relationship, and treatment implications. Cancers. 2023;15(14):3692. doi:10.3390/cancers15041095
3. Gong L, Tang Y, Xie H, et al. Predicting cervical intraepithelial neoplasia and determining the follow-up period in high-risk human papillomavirus patients. Front Oncol. 2023;13:1289030. doi:10.3389/fonc.2023.1289030
4. Olivera C, Paira DA, Olmedo A, et al. HPV and co-infections: impacts on semen inflammation, oxidative stress, and sperm quality. Front Cell Infect Microbiol. 2025;15:1539871.
5. Baldauf J, Dreyfus M, Monlun E, et al. Role of herpes virus simplex and cytomegalovirus as cofactors of papillomavirus in dysplastic and cancerous lesions of the uterine cervix. Chirurgie Memoires de L’academie de Chirurgie. 1992;118:652–12.
6. Guidry JT, Scott RS. The interaction between human papillomavirus and other viruses. Virus Res. 2017;231:139–147. doi:10.1016/j.virusres.2016.11.002
7. Lu L, Fan M, Li X, et al. Herpesvirus-associated diseases: biomarkers and advancements in clinical research. Virol J. 2025;22(1):177. doi:10.1093/infdis/jiae497
8. Sutter J, Hope JL, Wigdahl B, et al. Immunological control of herpes simplex virus type 1 infection: a non-thermal plasma-based approach. Viruses. 2025;17(5):600. doi:10.3390/v17050600
9. Xiao Q, Liu Y, Li T, et al. Viral oncogenesis in cancer: from mechanisms to therapeutics. Signal Transduct Target Ther. 2025;10(1):151. doi:10.1038/s41392-025-02156-6
10. Damania B, Kenney SC, Raab-Traub N. Epstein-Barr virus: Biology and clinical disease. Cell. 2022;185(20):3652–3670. doi:10.1016/j.cell.2022.08.039
11. Rigney J, Zhang K, Greas M, et al. A review of KSHV/HHV8-associated neoplasms and related lymphoproliferative lesions. Lymphatics. 2025;3(3):20. doi:10.3390/lymphatics3030020
12. Losay VA, Damania B. Unraveling the Kaposi Sarcoma-Associated Herpesvirus (KSHV) lifecycle: an overview of latency, lytic replication, and KSHV-associated diseases. Viruses. 2025;17(2):177. doi:10.3390/v17020177
13. Mojarrad S, Najmafshar M, Jahromi ZK, et al. Prevalence and genotype distribution of human papillomavirus in individuals referred to a laboratory in Urmia, Iran. Infect Agent Cancer. 2025;20(1):13. doi:10.1186/s13027-025-00616-4
14. Joharinia N, Faghihinezhad S, Seyedi K, et al. Co-existing of HSV1/2 or EBV Infection with the presence of high-risk HPV DNA in cervical lesions in the southwest of Iran. Asian Pacific J Cancer Prevent. 2020;21(5):1459. doi:10.31557/APJCP.2020.21.5.1459
15. Baldauf JJ, Dreyfus M, Ritter J, et al. A PCR study on the coexistence of herpes simplex virus, cytomegalovirus and human papillomavirus DNAs in cervical neoplasia. Int J Gynecol Cancer. 1996;6(5):389–395. doi:10.1046/j.1525-1438.1996.06050389.x
16. Lau H-Y, Twu N-F, Chen PC-H, et al. The relationship between human papillomavirus and Epstein-Barr virus infections in relation to age of patients with cervical adenocarcinoma. Taiwanese J Obs Gynecol. 2009;48(4):370–374. doi:10.1016/S1028-4559(09)60324-3
17. Aromseree S, Pientong C, Sunthamala N, et al. Co-infection of Epstein-Barr virus (EBV) with high risk Human papillomavirus (HR-HPV) is a significant risk of cervical cancer. Int J Infect Dis. 2012;16:e69. doi:10.1016/j.ijid.2012.05.186
18. Khenchouche A, Sadouki N, Boudriche A, et al. Human papillomavirus and Epstein-Barr virus co-infection in cervical carcinoma in Algerian women. Virol J. 2013;10(1):340. doi:10.1186/1743-422X-10-340
19. Muhsin J. Evaluation of the possible role of HPV16, CMV and EBV in Cervical Carcinoma progression using In Situ Hybridization technique. Diyala J Med. 2016;11(1):37–43.
20. Bakır A, Yüzügüldü B, Tanık EB, et al. Investigation of the prevalence of high-risk human papillomavirus, human herpesvirus-8, and herpes simplex virus-2 in cervical biopsy samples using the real-time PCR method. Trop Med Infect Dis. 2025;10(7):200. doi:10.3390/tropicalmed10070200
21. Ahmadi M, Rasi H, Mostafazadeh M, et al. Analysis of cervical lesions for presence of HSV-2 and HPV-16 and HPV-18 in Iranian patients by PCR. Horm Mol Biol Clin Investig. 2017;31(3). doi:10.1515/hmbci-2017-0019
22. Chavoshpour-Mamaghani S, Shoja Z, Jalilvand S. The prevalence of epstein-barr virus in normal, premalignant, and malignant uterine cervical samples in Iran. Intervirology. 2024;67(1):64–71. doi:10.1159/000538734
23. Chavoshpour-Mamaghani S, Shoja Z, Mollaei-Kandelous Y, et al. The prevalence of human herpesvirus 8 in normal, premalignant, and malignant cervical samples of Iranian women. Virol J. 2021;18(1):144. doi:10.1186/s12985-021-01618-z
24. Alaoui Sosse S, Tadlaoui Anouar K, Benhessou M, et al. Viral co-infection of oncogenic human papillomavirus with Epstein–Barr Virus, Human herpesvirus 8 and Herpes Simplex Virus type 2 in malignant cervical cancer. Res Sq. 2022. doi:10.21203/rs.3.rs-2230441/v1
25. Zhao Y, Cao X, Zheng Y, et al. Relationship between cervical disease and infection with human papillomavirus types 16 and 18, and herpes simplex virus 1 and 2. J Med Virol. 2012;84(12):1920–1927. doi:10.1002/jmv.23391
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.