")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 9
Prevalence of fertility desire and its associated factors among 15- to 49-year-old people living with HIV/AIDS in Addis Ababa, Ethiopia: a cross-sectional study design
Authors Adilo TM, Wordofa HM
Received 2 February 2017
Accepted for publication 20 June 2017
Published 30 August 2017 Volume 2017:9 Pages 167—176
DOI https://doi.org/10.2147/HIV.S133766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Video abstract presented by Takele Menna Adilo.
Views: 508
Takele Menna Adilo,1 Hirut Megerssa Wordofa2
1Department of Public Health, 2School of Nursing, St Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Background: The magnitude of unprotected sex to satisfy the desire for fertility among people living with HIV/AIDS (PLHIV) may rise more due to the availability of antiretroviral therapy (ART) in most HIV-affected countries. This could, however, have the risk of passing on HIV to sexual partners and children. The aim of this study, therefore, was to determine the magnitude and factors associated with the fertility desire of reproductive-age PLHIV in Addis Ababa, Ethiopia, for research-based and timely actions.
Methods: A cross-sectional study was carried out from April to June 2016 among 442 randomly selected, reproductive-age PLHIV who had been attending ART clinics in Addis Ababa. Twelve experienced and trained nurses collected the data. The questionnaire was pretested and interviewer-administered, and the interview was executed after obtaining voluntary consent from each study subject. The data were then cleaned and analyzed by using Epi Info version 3.5.4 and SPSS version 20.0, respectively. Binary logistic regression was done in order to describe the association of fertility desire with some sociodemographic and sexual behavior-related factors.
Results: Among the total 441 respondents, 54.6% reported the desire for fertility, 87% disclosed their HIV status, 24.3% had two or more sexual partners in the earlier year, and only 55.6% used a condom during their last sexual intercourse. In addition, current health status (AOR=2.03; 95% CI: 1.01–4.07) and partner being tested for HIV (AOR=6.31; 95% CI: 1.35–29.64) showed statistically significant associations with fertility desire during multivariate logistic regression analysis.
Conclusion: A considerable number of PLHIV in the study area reported a desire for having children. Current health status and partner being tested for HIV were found to be factors associated with the fertility desire among PLHIV. Thus, more efforts to effectively address the health concerns related to fertility desire and risky sexual behavior among HIV-infected people of reproductive age could play a significant role in prevention and control measures against HIV/AIDS epidemic.
Keywords: fertility desire, PLHIV, reproductive age, risky sexual behavior, Ethiopia
Introduction
It was estimated that there were about 36.7 million people living with HIV/AIDS (PLHIV) in the world in 2015. Of these, 17 million had access to antiretroviral therapy (ART).1 The contemporary projected population of Ethiopia, one of the most HIV/AIDS-affected countries in the globe, was about 90.9 million (50.8% female).2,3
The people most affected by HIV/AIDS are those who are sexually active and economically more productive falling within the 25–49 age group.4 According to some studies, the desire for having children among PLHIV is rising because of the return to normal life, including maintenance of sexual activity due to ART.5–7 After the worldwide introduction of ART, the HIV/AIDS-related illnesses and deaths have decreased considerably, and in addition, the quality of life of PLHIV has significantly been improved leading to a rise in the need for having children.8,9
The desire has increased due to the enhanced quality of life and survival as a result of the availability of ART and improvement in reproductive health services in most HIV-affected countries.10 Nevertheless, unprotected sex that is aimed at achieving fertility among PLHIV has the risk of transmitting HIV to their respective sexual partners and also to their children during birth and/or breastfeeding.6,7
The health and economic status of PLHIV can be improved due to the availability and widespread use of ART. This, in turn, may increase their need for fertility and having more children, though it has the risk of passing the virus to children.11,12 Consequently, the judgment related to fertility desire among PLHIV must be preceded by adequate knowledge of HIV and its mode of transmission. Sexual partners must also be well informed about the case as they can have a significant positive effect on the health of their families and the public at large. Although the main aim of ART is to decrease the HIV-related illnesses and deaths, and thereby extend the continued existence of PLHIV, there are still growing public health and demographic consequences of ART that are not fully understood.6,13 For instance, the sexual desire as well as an intention for fertility of PLHIV can be increased due to the expected improvements in health and economic status. This, in turn, can increase the probability of HIV transmission to the discordant couples and their fetuses or babies.14,15
As an effect of the multifaceted correlation between fertility intention and HIV/AIDS transmission, the preventive and control measures against the HIV epidemic can be challenged in many affected countries with low utilization of prevention of mother-to-child transmission (PMTCT) service and high fertility rate, like Ethiopia.16
For instance, studies from various African countries, including Ethiopia, reported that the magnitude of fertility desire and unprotected sex among PLHIV is about 37% and 69%, respectively. These findings pointed out the likelihood of HIV transmission, particularly among discordant sexual partners.17,18 Although two in every five pregnancies are unplanned globally, women living with HIV are more at the danger of unintended pregnancies.19,20 This results in the occurrence of about 1,600 new HIV infections through vertical transmission, that is, mother-to-child transmission of HIV, among the total 14,000 new infections in a day globally.21
Since most PLHIV are in their childbearing age, one of the unexpected effects of ART is its likelihood to increase the fertility desires of people infected and affected with HIV/AIDS.22 This effect could be even more significant in most sub-Saharan African countries where people give higher social value to fertility or childbearing couples.6 Furthermore, a study also showed that there was increased intention of childbearing among PLHIV because of the availability of ART and PMTCT programs.23
The sociocultural and economic factors influence the reproductive preferences and choices of men and women, regardless of serostatus, particularly in sub-Saharan Africa.6 Moreover, as it holds true for the general population, the pleasure, happiness, and sense of social fulfillment associated with parenthood are some of the reasons for the likely increase in fertility intentions among PLHIV.6,14 In addition, the disclosure of one’s HIV status was found to be associated with the desire for fertility among this population.17,18
In contrast, HIV/AIDS infection can affect fertility directly by causing spontaneous abortion24,25 or indirectly through decreased sexual desire, marital disruption, and use of condoms.26
However, research-based and updated data on the fertility and reproductive intentions among PLHIV are scarce.27 As Ethiopia is one of the most HIV-affected countries in the world, exploring the magnitude and factors associated with the fertility desire among sexually active people aged 15–49 years could have a pivotal contribution to the national efforts to prevent and control the epidemic.28
In general, understanding the factors associated with fertility desire was believed to play an important role in evidence-based and timely intervention by all concerned sectors and actors in Ethiopia and other similar countries.
Materials and methods
Study design and setting
This cross-sectional study was conducted at four randomly selected health centers, a regional hospital, and a tertiary-level hospital located in different sub-cities in Addis Ababa City Administration. Addis Ababa is located at 9° North latitude and 38° East longitude with altitude ranging between 2,200 and 2,800 m above sea level. In 2014, the projected population of Addis Ababa, as per the national census report of 2007, was 3,197,000, and of this, about 52% were females.2,3,29.30
In Addis Ababa, the number of people tested for HIV until 2012/2013 was 503,930. Of this, 19,149 (3.8%) persons tested positive, and it was the highest compared to all regions in the country and that of the national data (1.1%).30,31
Sampling procedure
All patients attending ART clinics of health institutions in Addis Ababa City during the study period were considered as the source population of the study. The real data collection, however, focused on those ART clinics of public hospitals and health centers in the city.
For this study, four public health centers (Arada, Bole, District 3, and District 9) and two public hospitals (St Paul’s Hospital Millennium Medical College and Ras Desta Damtew Hospital) were randomly selected from various sub-cities. Then, a random sampling technique with reasonable formulas of assumptions and 15% contingency was used, in order to get the representative samples among the HIV patients of the reproductive age group who were attending the respective ART clinics. In addition, the total number of HIV patients selected was estimated using the following single-population proportion calculation formula: n = (Z2 ´ p ´ q)/d2. As “n” was the sample size of the study, Z was the upper α/2 point of standard normal distribution, where α=0.05, and Z α/2=1.96. According to the findings of previous studies conducted in different sub-Saharan countries, the rate of contraceptive utilization and condom use among HIV-positive people was about 48%.11,32–42 Consequently, the real prevalence rate considered was p=0.48 and q=0.52 as indicated.
The maximum-allowed difference between the maximum likelihood estimate and the unknown population parameter denoted by “d” was desired to be 0.05. The required sample size was calculated as declared in the equation, and then for the possible nonresponse rate, 15% contingency was added. Thus, 442 randomly selected HIV-positive individuals who were attending ART clinics of the targeted public health facilities in Addis Ababa were taken as the final sample. Moreover, the sample size was proportionately allocated to each randomly selected health facility based on their number of ART clients during the study period. Nonetheless, those HIV-positive patients whose ages were less than 15 years, who were severely ill during the study period, and who were unable to take part in the study were excluded.
Data collection and quality control
Pretested, structured, and interviewer-administered questionnaires were used to collect the data in 2016 for assessing the magnitude and factors associated with fertility desire among HIV-positive people aged 15–49 years. Four hundred and forty-one HIV-positive patients aged 15–49 years who provided written consent to take part in the study were the sources for the collected data.
In order to ensure data quality, various actions were taken at different levels. Before the actual administration, the intended questionnaires were edited and pretested. In addition, the required training was given for data collectors and supervisors by the principal investigator (PI) and coresearchers. Twelve data collectors (nurses with BSc degree), two supervisors who had BSc degree and above in health sciences/coresearchers, and the PI carried out the process of data collection.
The prepared standard questionnaires originally in English were translated to Amharic and then back to English in order to check for regularity as well as to make effective pretests and then adjustments as required.
In addition, the pretesting of the data collection instruments was done prior to the main fieldwork using HIV-positive patients from two public health facilities which were not part of the real study. The health facilities in which the questionnaires were pretested had similar characteristics to that of the health facilities where the real study was conducted. The pretest was useful to recognize problems in clarity and exclude inappropriate questions as well as to make sure the time used up in answering. Moreover, it was aimed at improving the cross-cultural validity, precision, and reliability of the data. As a result of pretesting the research questionnaires, some unclear questions were either removed or rephrased. The data collectors were also equipped with some written “Dos and Donts” that were implemented during data collection.
Moreover, the filled questionnaires were checked at the field level, first by the data collectors themselves and then by their respective supervisors on a daily base. These questionnaires were cross-checked randomly for their completeness and consistency daily by the PI. At the entry level, the data were checked carefully for invalid codes, duplicated entries, missing values, and inconsistency of records with due emphasis to the expected quality of data.
Ethical considerations
The ethical principles of respect, beneficence, and justice were practiced with due concerns throughout the data collection processes as the study subjects were PLHIV who were attending ART clinics at public health facilities in Addis Ababa.
Official letters of cooperation were also written to all health facilities selected for the actual data collection from St Paul’s Hospital Millennium Medical College. The letters were written after securing ethical clearance from the Institutional Review Board of St Paul’s Hospital Millennium Medical College prior to the field work.
In addition, informed and voluntary consent for the study were obtained from all subjects, as per the recommended principles of human research ethics. It was put into practice after giving full information to the study participants about the objectives of the study and their right to take part in the study or not. This was critical to the whole progress of the study. Last, all the data of the study were managed with confidentiality and anonymity.
Data management and statistical analysis
A computer with Epi Info software version 3.5.4 was used first to enter all the collected data, and then analyses were done using the SPSS software version 20.0. Various suitable statistical methods were used: frequency distribution, proportions, percentages, ORs, and AORs with 95% CIs.
The existing theoretical knowledge of the variables and statistical significance found during bivariate analyses was employed to choose the variables in multivariate analyses. Thus, the P-values less than 0.05 were taken as statistically significant.
Results
Sociodemographic features of study participants
Among the total 442 PLHIV interviewed for this study, 441 (99.8%) responded voluntarily. Of these, 313 (71.0%) were women. While the majority of study subjects (94.5%) were in the age range of 25–49 years, only 20 (4.5%) were in the age range of 15–24 years. With regard to marital status, 94 (21.3%), 208 (47.2%), and 139 (31.5%) were single, married, and divorced and widowed, respectively. The majority of the study subjects, that is, 244 (55.3%), were Amhara by ethnicity; 349 (79.1%) were orthodox religion followers, and 228 (51.7%) had secondary and above level of education during the study period (Table 1).
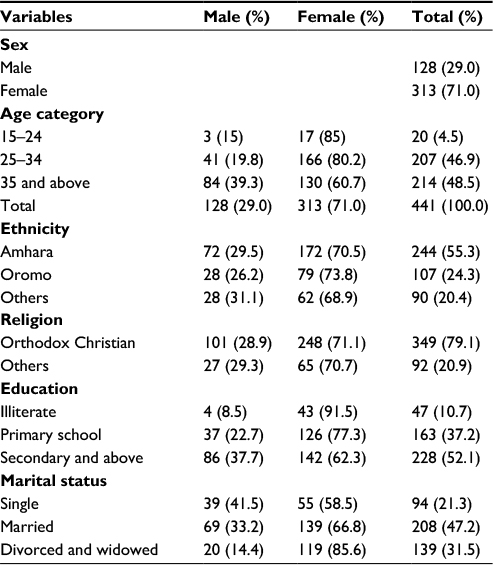 | Table 1 Sociodemographic characteristics of study participants by sex, in Addis Ababa, Ethiopia (2016) |
Sexual, clinical, and reproductive characteristics of study participants
Among the 441 participants, 418 (95.0%) ever had sexual intercourse, and 354 (85.1%) had a history of having sexual intercourse in the previous 12 months of the study period; 382 (87.0%) disclosed their HIV status to their respective sexual partners, parents, or friends, and the remaining 57 (13.0%) of the respondents did not disclose their HIV status to anyone. Moreover, 274 (75.71%) and 88 (24.3%) of the study participants reported that they had one and two or more sexual partners in the year preceding the study, respectively. Of the total participants of the study, 234 (56.4%) self-reported that they had sexual partners during the study time, of whom 204 (91.9%) responded that their partners were tested for HIV. Of those who reported partners’ test, 152 (68.5%) responded that their partners’ HIV status was positive, and the remaining 52 (31.5%) responded that their partners’ HIV status was either negative or not understood at all. Of the study subjects, 165 (37.8%) and 271 (62.2%) individuals had been on ART for 5 or less years and more than 5 years, respectively. In addition, of the total participants, those who had the CD4 count of less than or equal to 200, 201–400, and greater than 400 per microliter of blood were 48 (11.3%), 148 (34.8%), and 229 (53.9%), respectively (Table 2).
 | Table 2 Sexual, clinical, and fertility desire-related characteristics of PLHIV by sex in Addis Ababa (2016; N=441) Abbreviations: PLHIV, people living with HIV/AIDS; PMTCT, prevention of mother-to-child transmission; ART, antiretroviral therapy. |
As for the study subjects’ general perceived health status, 229 (52.4%) self-reported as very good, 109 (24.9%) reported as good, and 99 (22.7%) reported as fair or bad (Table 2).
In addition, 302 (72.6%) of the participants were knowledgeable about the importance of PMTCT, and 277 (66.6%) reported that their attitude toward using PMTCT service was positive. Pertinent to desire to have children, 227 (54.6%) responded that they had desired for fertility or more children, while 189 (45.4%) reported no desire or were unsure about it. Regarding why some PLHIV desire for fertility, 256 (62.3%), 71 (17.3%), and 84 (20.4%) of the respondents replied that they wanted to replace themselves, they believed HIV cannot be transmitted to their babies since they are on ART, and it is due to social pressure, respectively. Furthermore, of the total number of study subjects, only 233 (55.7%) used male condoms during the last sexual act (Table 2).
Factors associated with fertility desire among PLHIV
An attempt was made to identify the factors that are associated with fertility desire among PLHIV. In this regard, as binary logistic regression model in Table 3 shows, the factors affecting fertility desire showing statistically significant associations are found to be age being 35 and above (COR=0.62; 95% CI: 0.41–0.92), current health status (COR=2.56; 95% CI: 1.54–4.23), having sexual partner at present (COR=1.97; 95% CI: 1.33–2.92), sexual partner being tested (COR=6.57; 95% CI: 1.47–29.32), and attitude toward using PMTCT service (COR=1.64; 95% CI: 1.08–2.48).
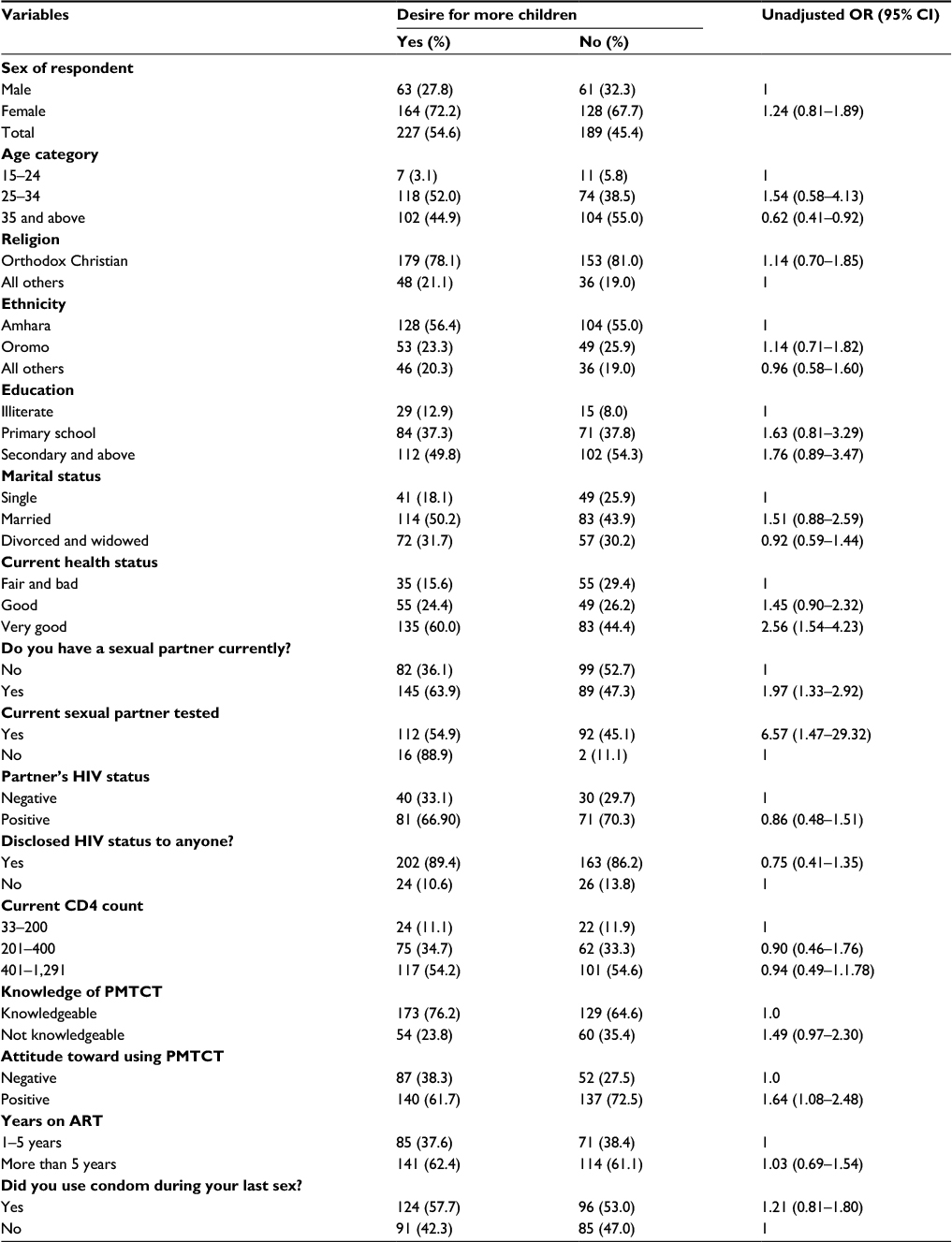 | Table 3 Factors associated with the fertility desire among PLHIV in Addis Ababa, 2016 (N=441) Abbreviations: PLHIV, people living with HIV/AIDS; PMTCT, prevention of mother-to-child transmission; ART, antiretroviral therapy. |
The variables computed with fertility desire showed statistically significant associations or P-values <0.05 during bivariate analyses were further analyzed using the multivariable logistic regression model of the independent factors associated with the outcome variable. Accordingly, current health status (AOR=2.03; 95% CI: 1.01–4.07) and partner being tested for HIV (AOR=6.31; 95% CI: 1.35–29.64) showed statistically significant associations with fertility desire among PLHIV. On the contrary, age, currently having a partner, and attitude toward PMTCT service lost their statistical significance during multivariable logistic regression analyses (Table 4).
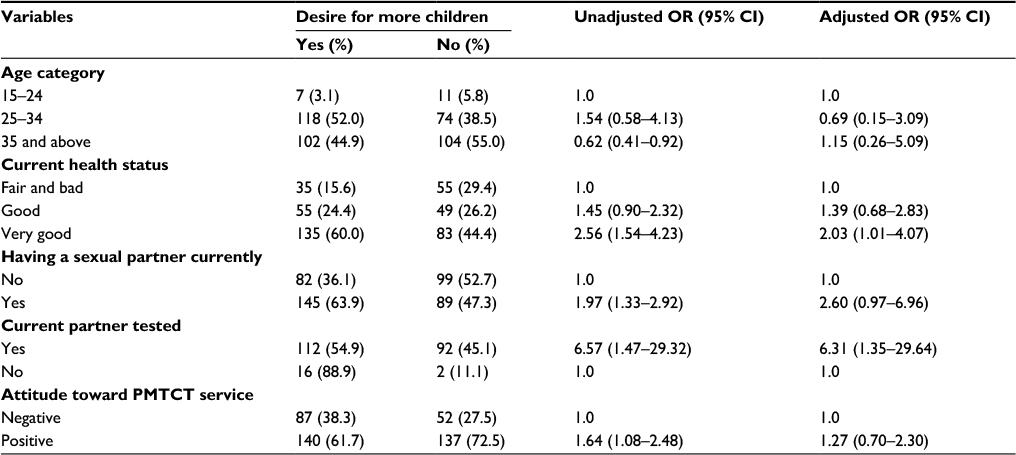 | Table 4 Multivariable logistic regression analysis of factors associated with fertility desire among PLHIV of reproductive age in Addis Ababa (2016) Abbreviations: PLHIV, people living with HIV/AIDS; PMTCT, prevention of mother-to-child transmission. |
Discussion
This cross-sectional and health facility-based study was done among reproductive-age PLHIV in Addis Ababa, Ethiopia. The lion’s share of the participants (94.5%) was above 25 years old, and females constituted 71%. This was in agreement with the prevalence of HIV/AIDS among adults in Ethiopia and globally.1,3,4,16,43–46 According to the results of this study, the greater portions of the PLHIV had completed at least secondary-level education. This is also consistent with the national progress report for the year 2014 on HIV/AIDS that showed a high rate of risky sexual behavior practices among university and secondary school students.44 Nonetheless, this result is to some extent higher than the findings of a similar study that was conducted previously in Addis Ababa among female HIV patients. The experiential disparity might appear because of the difference in study duration and inclusion of both sexes in our study.44,45
Among the 441 study participants, the proportion of fertility desires among male, female, and both sexes was 50.8%, 56.2%, and 54.6% with 95% CI of 50.6%–60.0%, respectively. The percentage of fertility desire among PLHIV in this study was higher than the findings of studies conducted previously in Fitche town, Ethiopia, and Cape Town, South Africa, which were 39.1% and 51.0%, respectively.46,47 However, it was lower than the findings of the Ethiopian demographic and health survey of 2011 and a study from Nigeria, which were 63.0% and 63.3%, respectively.17,48 The differences could be explained in terms of variations in sociodemographic characteristics of the populations and cultural concerns of having a big family size and more fertility desires.
With regard to the perceived health conditions of PLHIV during the study time, about three-fourths of the participants reported that they were either in a very good or in a good health status due to ART. This result is also consistent with the results of various earlier studies that showed a decrease in the magnitude of HIV/AIDS-related morbidity and mortality as well as new HIV infections, besides a real improvement in the quality of lives of PLHIV due to ART.8,9
According to the findings of this study, the factors that correlated with the fertility desire among PLHIV were age, current health status, having a sexual partner during the study period, current partner has been tested, and attitude toward PMTCT. Even though the aforementioned factors have demonstrated statistically significant associations with fertility desire among PLHIV during bivariate analyses, age, having a sexual partner, and attitude toward PMTCT among PLHIV lost their experiential statistical significance during multivariate analyses (Table 4).
PLHIV who self-reported that their personal health status was good during the study period were found to have a fertility desire about two times more likely than their counterparts. This could be explained in terms of the probabilities of being improved in social, economic, and physical statuses of PLHIV due to the positive effects of ART. This finding was in accordance with most previous studies that have documented a positive relationship between ART use and desire for future fertility. For instance, a study in Brazil reported that ART use was positively associated with a woman’s desire to have a child.49 Similar positive associations between ART and fertility desire have been reported in studies from South Africa50 and India.51 The availability of PMTCT program could have also increased fertility desire.49
On the other hand, some studies did not find associations between ART use and fertility desires among PLHIV. A recent study in Soweto slums of South Africa found a lack of association between ART use and childbearing intentions.52 Similarly, the findings of the studies carried out in Nigeria and Uganda reported no association between ART use and fertility desires.17,53 Contrary to this, the finding of another study done in Nigeria revealed a negative association between ART use and fertility desires.54
Furthermore, the study participants whose sexual partners were tested for HIV were about six times more likely to have fertility desire. This can be explained in terms of being tested for HIV and by that subsequent disclosure of one’s HIV status to the sexual partners could increase options to facilitate the ability to make informed decisions on childbearing. This finding was also concurrent with the study conducted in South Africa among PLHIV.47
Last, since there were some sexual behaviors-related questions in the study that were sensitive, social desirability bias might have occurred during the process of collecting data. In addition, the findings may not be generalized to other parts of the country, as the study participants were only from the Addis Ababa City.
Conclusion
In summary, as the results of this study have demonstrated, a considerable proportion of PLHIV in Addis Ababa, Ethiopia, reported that they have a desire for fertility or to have children. The practice of unprotected sexual interaction with a likely high rate of pregnancy was observed among PLHIV. More importantly, the factors associated with fertility desire were found to be perceived health status and current partner’s undertaking of HIV test.
In addition, a considerable number of PLHIV in the study area were practicing risky sexual behavior or having multiple sexual partners (24.3%). Thus, the findings of this study give the call for more efforts to effectively address fertility desire, safe sex, and contraception-related concerns for HIV-infected and HIV-affected people in reproductive health services of various developing countries.
Furthermore, the present study was limited to exploring the magnitude and factors associated with the fertility desire among PLHIV in the capital city, Addis Ababa. Consequently, there is a need for a nationwide study with more representative sample size to strengthen much-needed pragmatic data on the determinants of fertility desire among PLHIV. Finally, further research can look at enhancing the quality of sexual and reproductive health services in health facilities, schools, and other community-based pertinent institutions to improve the quality of health and productivity of PLHIV in Ethiopia and other sub-Saharan countries.
Acknowledgments
The authors are pleased to acknowledge St Paul’s Hospital Millennium Medical College for its monetary support for this study. They thank all the study participants and workers of the involved health facilities for their very helpful commitment to make this study work a reality.
Disclosure
The authors have no conflicts of interest in this work.
References
UNAIDS. Fact sheet 2015: global statistics. Geneva: UNAIDS; 2015. Available from: www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed August 4, 2017. | ||
Central Statistical Agency. 2007 Ethiopian census, first draft. 2009. Available from: https://unstats.un.org/...census/.../presentation%20at%20Stat%20Com-UN%20Samia1. Accessed August 4, 2017. | ||
Federal Democratic Republic of Ethiopia. Report on progress towards implementation of the UN Declaration of Commitment on HIV/AIDS. Addis Ababa: Federal HIV/AIDS Prevention and Control Office; 2010. Available from: data.unaids.org/pub/report/2010/ethiopia_2010_country_progress_report_en.pdf. Accessed August 4, 2017. | ||
UNAIDS. Report on the global AIDS epidemic. 2010. Available from: www.unaids.org/globalreport/documents/20101123_GlobalReport_full_en.pdf; date accessed November 23, 2010. | ||
Kisakye P, Akena WO, Kaye DK. Pregnancy decisions among HIV-positive pregnant women in Mulago Hospital, Uganda. Cult Health Sex. 2010;12(4):445–454. | ||
Cooper D, Harries J, Myer L, Orner P, Bracken H, Zweigenthal V. “Life is still going on”: reproductive intentions among HIV-positive women and men in South Africa. Soc Sci Med. 2007;65(2):274–283. | ||
Beyeza-Kashesya J, Ekstrom AM, Kaharuza F, Mirembe F, Neema S, Kulane A. My partner wants a child: a cross-sectional study of the determinants of the desire for children among mutually disclosed sero-discordant couples receiving care in Uganda. BMC Public Health. 2010;10:247–210. | ||
Auerbach JD. Principles of positive prevention. J Acquir Immune Defic Syndr. 2004;37(Suppl 2):S122–S125. | ||
Coetzee D, Hildebrand K, Boulle A, et al. Outcomes after two years of providing antiretroviral treatment in Khayelitsha, South Africa. AIDS. 2004;18(6):887–895. | ||
Andia I, Kaida A, Maier M, et al. Highly active antiretroviral therapy and increased use of contraceptives among HIV positive women during expanding access to antiretroviral therapy in Mbarara, Uganda. Am J Public Health. 2009;99(2):340–347. | ||
UNAIDS. 2008 report on global AIDS epidemic (full report). 2009. Available from: http://www.unaids.org/en/Knowledge. | ||
Schwartz SR, Rees H, Mehta S, Venter WD, Taha TE, Black V. High incidence of unplanned pregnancy after antiretroviral therapy initiation: findings from a prospective cohort study in South Africa. PLoS One. 2012;7(4):e36039. | ||
Mocroft A, Ledergerber B, Katlama C, et al; EuroSIDA Study Group. Decline in the AIDS death rates in the Euro SIDA study: an observational study. Lancet. 2003;362(9377):22–29. | ||
Smith DJ, Mbakwem BC. Life projects and therapeutic itineraries: marriage, fertility, and antiretroviral therapy in Nigeria. AIDS. 2007;21 Suppl 5:S37–S41. | ||
Smith DJ, Mbakwem BC. Antiretroviral therapy and reproductive life projects: mitigating the stigma of AIDS in Nigeria. Soc Sci Med. 2010;71(2):345–352. | ||
Federal Ministry of Health Ethiopia (FMoHE)/Federal HIV/AIDS Prevention and Control Office (FHAPCO). Guidelines for Prevention of Mother-to-Child Transmission of HIV in Ethiopia. Addis Ababa: FMoHE/FHAPCO; 2007. | ||
Iliyasu Z, Abubakar IS, Kabir M, Babashani M, Shuaib F, Aliyu MH. Correlates of fertility intentions among HIV/AIDS patients in northern Nigeria. Afr J Reprod Health. 2009;13(3):71–83. | ||
Debeko K, Seme A. Sexual and Reproductive Health Needs and Preferences of People Living with HIV/AIDS in Southern Nations Nationalities and Peoples Region [master’s thesis]. Addis Ababa: Department of Community Health, Addis Ababa University; 2007. | ||
Koenig LJ, Espinoza L, Hodge K, Ruffo N. Young, sera positive, and pregnant: epidemiologic and psychosocial perspectives on pregnant adolescents with human immunodeficiency virus infection. Am J Obstet Gynecol. 2007;197(3 Suppl):S123–S131. | ||
Zimbwa I, Vwalika B. Association between unplanned pregnancy and HIV seropositivity disclosure to marital/cohabitating partner among postnatal women in Lusaka, Zambia. Med J Zambia. 2010;37(4):205–215. | ||
WHO. World Health Organization Constitution. 2010. Available from: www.who.int/governance/eb/who_constitution_en.pdf. Accessed August 4, 2017. | ||
UNAIDS. Report on the global AIDS epidemic. Geneva: UNAIDS; 2008. | ||
McCarraher D, Cuthbertson C, Kung’u D, Otterness C, Johnson L, Magiri G. Sexual behavior, fertility desires and unmet need for family planning among home-based care clients and caregivers in Kenya. AIDS Care. 2008;20(9):1057–1065. | ||
Lewis JJ, Ronsmans C, Ezeh A, Gregson S. The population impact of HIV on fertility in sub-Saharan Africa. AIDS. 2004;18 Suppl 2:S35–S43. | ||
Schiltz MA, Sandfort TG. HIV-positive people, risk and sexual behaviour. Soc Sci Med. 2000;50(11):1571–1588. | ||
Getachew M, Alemseged F, Abera M, Deribew A. Factors affecting fertility decisions of married men and women living with HIV in South Wollo Zone, Northeast Ethiopia. Ethiop J Health Dev. 2010;24(3):214–220. | ||
Delvaux T, Nöstlinger C. Reproductive choice for women and men living with HIV: contraception, abortion and fertility. Reprod Health Matters. 2007;15(29 Suppl):46–66. | ||
Federal HIV AIDS Prevention and Control Office, Federal Republic of Ethiopia. Country progress report on HIV/AIDS response. Addis Ababa; 2012. Available from: http://files.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2012countries/GAP%20Report%202012.pdf. Accessed August 4, 2017. | ||
Berhane Y, Mekonnen Y, Seyoum E, Gelmon L, Wilson D. HIV/AIDS in Ethiopia: an epidemiological synthesis. Washington, DC: World Bank; 2008. | ||
The world fact-book, “Ethiopia”. 2011. [Webpage on the Internet]. Available from: www.theodora.com/wfb2011/ethiopia/index.html. Accessed August 4, 2017. | ||
Ethiopian Public Health Institute. HIV related estimates and projections for Ethiopia. 2012. Available from: www.unaids.org/en/media/unaids/contentassets/.../data.../Ethiopia2012report.pdf. Accessed August 4, 2017. | ||
Segurado AC, Paiva V. Rights of HIV positive people with sexual and reproductive health: parenthood. Reprod Health Matters. 2007;15(29 Suppl):27–45. | ||
Bayeza Kashesya J, Kaharuza F, Mirembe F, Neema S, Ekstrom AM, Kulane A. The dilemma of safe sex and having children: challenges facing HIV sero-discordant couples in Uganda. Afr Health Sci. 2009;9(1):2–12. | ||
WHO. Sexual and reproductive health of women living with HIV/AIDS. Guidelines on care, treatment and support for women living with HIV/AIDS and their children in resource-constrained settings. Geneva: WHO; 2006. www.who.int/hiv/pub/guidelines/sexualreproductivehealth.pdf. Accessed August 4, 2017. | ||
Crepaz N, Lyles CM, Wolitski RJ, et al; HIV/AIDS Prevention Research Synthesis (PRS) Team. Do prevention interventions reduce HIV risk behaviors among people living with HIV? A meta-analytic review of controlled trials. AIDS. 2006;20(2):143–157. | ||
Kennedy CE, Medley AM, Sweat MD, O’Reilly KR. Behavioral interventions for HIV positive prevention in developing countries: a systematic review and meta-analysis. Bull World Health Organ. 2010;88(8):615–623. | ||
Barnett T, Whiteside A. AIDS in the Twenty-First Century: Disease and Globalization. 2nd ed. New York, NY: Palgrave Macmillan; 2006. | ||
Coates TJ, Richter L, Caceres C. Behavioral strategies to reduce HIV transmission: how making them work better. Lancet. 2008;372(9639):669–684. | ||
Bunnell R, Ekwaru JP, Solberg P, et al. Changes in sexual behavior and risk of HIV transmission after antiretroviral therapy and prevention interventions in rural Uganda. AIDS. 2006;20(1):85–92. | ||
Federal Ministry of Health Ethiopia (FMoHE). Health and Health Related Indicators. Addis Ababa: FMOHE; 2011. | ||
Mmbaga EJ, Leyna GH, Ezekiel MJ, Kakoko DC. Fertility desire and intention of people living with HIV/AIDS in Tanzania: a call for restructuring care and treatment services. BMC Public Health. 2013;13:86. | ||
Nduna M, Farlane L. Women living with HIV in South Africa and their concerns about fertility. AIDS Behav. 2009;13 Suppl 1:62–65. | ||
Ethiopian Public Health Institute. HIV related estimates and projections for Ethiopia. 2014. Available from https://www.unicef.org/ethiopia/ECO_HIV_Related_Estimates_and_Projections_for_Ethiopia_2014_National.pdf. Accessed August 4, 2017. | ||
Federal Democratic Republic of Ethiopia. Country progress report on the HIV response. 2014. Available from www.unaids.org/sites/default/files/country/.../ETH_narrative_report_2014.pdf. Accessed August 4, 2017. | ||
Asfaw HM, Gashe FE. Contraceptive use and method preference among HIV positive women in Addis Ababa, Ethiopia: a cross sectional survey. BMC Public Health. 2014;14(1):566. | ||
Demissie DB, Tebeje B, Tesfaye T. Fertility desire and associated factors among people living with HIV attending antiretroviral therapy clinic in Ethiopia. BMC Pregnancy Childbirth. 2014;14:382. | ||
Cooper D, Moodley J, Zweigenthal V, Bekker LG, Shah I, Myer L. Fertility intentions and reproductive health care needs of people living with HIV in Cape Town, South Africa: implications for integrating reproductive health and HIV care services. AIDS Behav. 2009;13 Suppl 1:38–46. | ||
Ethiopia demographic and health survey 2011. Addis Ababa/Calverton, MD: Central Statistical Agency/ICF International; 2012. Available from: https://dhsprogram.com/pubs/pdf/FR255/FR255.pdf. Accessed Auguest 4, 2017. | ||
Nóbrega AA, Oliveira FA, Galvão MT, et al. Desire for a child among women living with HIV/AIDS in northeast Brazil. AIDS Patient Care STDS. 2007;21(4):261–267. | ||
Myer L, Morroni C, Rebe K. Prevalence and determinants of fertility intentions of HIV-infected women and men receiving antiretroviral therapy in South Africa. AIDS Patient Care STDS. 2007;21(4):278–285. | ||
Kanniappan S, Jeyapaul MJ, Kalyanwala S. Desire for motherhood: exploring HIV-positive women’s desires, intentions and decision-making in attaining motherhood. AIDS Care. 2008;20:625–630. | ||
Kaida A, Laher F, Strathdee SA, et al. Childbearing intentions of HIV-positive women of reproductive age in Soweto, South Africa: the influence of expanding access to HAART in an HIV hyperendemic setting. Am J Public Health. 2011;101(2):350–358. | ||
Homsy J, Bunnell R, Moore D, et al. Reproductive intentions and outcomes among women on antiretroviral therapy in rural Uganda: a prospective cohort study. PLoS One. 2009;4(1):e4149. | ||
Oladapo OT, Daniel OJ, Odusoga OL, Ayoola-Sotubo O. Fertility desires and intentions of HIV-positive patients at a suburban specialist center. J Natl Med Assoc. 2005;(12):1672–1681. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.