")
Back to Journals » International Journal of General Medicine » Volume 16
Prevalence of Dyslipidemia and Its Determinants Among the Adult Population of the Jazan Region
Authors Ghazwani M , Mahmood SE , Gosadi IM , Bahri AA, Ghazwani SH, Khmees RA
Received 27 July 2023
Accepted for publication 9 September 2023
Published 18 September 2023 Volume 2023:16 Pages 4215—4226
DOI https://doi.org/10.2147/IJGM.S429462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Mousa Ghazwani,1 Syed Esam Mahmood,2 Ibrahim M Gosadi,3 Ahmed A Bahri,3 Sulaiman H Ghazwani,4 Rola A Khmees3
1Department of Pediatric Surgery, Maternity and Children Hospital, Abha, Aseer, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 4Department of Clinical Pharmacy, College of Pharmacy, Jazan University, Jazan, Saudi Arabia
Correspondence: Mousa Ghazwani, Department of Pediatric Surgery, Maternity and Children hospital, Abha, Aseer, Saudi Arabia, Tel +966598556587, Email [email protected]
Purpose: To assess the prevalence of dyslipidemia and its determinants among adults in the Jazan region of Saudi Arabia.
Methods: This data was collected during interviews utilizing a structured questionnaire. The questionnaire measured the demographics, diagnosis with dyslipidemia, and distribution of dyslipidemia determinants among the sample, including dietary habits and lifestyle practices. A chi-square test was used to examine the statistical difference between the characteristics of individuals who had reported checking their lipid profile to those who reported never performing a lipid profile check-up among participants not diagnosed with dyslipidemia.
Results: The current study included a total of 244 participants. The median age of the participants was 27 years, most participants were female (66.8%), and about 59% had a university education or above. Approximately 40% of the participants had ever had their lipid profile checked, 20.1% of the participants had been diagnosed with dyslipidemia, and 20.9% had family history of dyslipidemia. Most of the undiagnosed participants (79.9%) had more than one risk factor for developing dyslipidemia. All the participants without a dyslipidemia diagnosis had not been meeting the recommended levels of physical activity, and more than half consumed a high-fat diet. The results of the inferential analysis indicate that among those who had not been diagnosed with dyslipidemia, participants who were older than 27 years, male, unemployed, married, had a university education or above, and a minimum monthly income of 5000 Saudi Arabia Riyals were more likely to check their lipid profile compared to other groups (p-values < 0.05).
Conclusion: The findings suggest that most of the participants who had not been diagnosed with dyslipidemia are at high risk of developing dyslipidemia. About 60% of the participants had never checked their lipid profile, suggesting a need to promote routine lipid profile check-ups among individuals at high-risk for dyslipidemia.
Keywords: dyslipidemia, check-up, determinants, lipid, adult population, Saudi Arabia
Introduction
According to the World Health Organization (WHO), 39% of the world adult population has been affected by elevated blood cholesterol, with a relatively higher prevalence among women (40%) than among men (37%).1 Raised blood cholesterol can have several consequences that increase the burden of the disease. It was reported that 4.32 million fatalities in 2017 were caused by raised low-density lipoprotein (LDL) cholesterol, accounting for 7.7% of deaths worldwide that year.2 Based on the 2019 World Health Survey in Saudi Arabia, the prevalence of raised serum cholesterol ranged from 42% in urban areas to 47% in rural areas. It was also indicated that those who are better educated and/or wealthier had lower cholesterol levels than others.3
Atherosclerosis, thrombosis, coronary heart disease, and ischemic stroke are health complications that are major risk factors for dyslipidemia. Cardiovascular diseases (CVDs) are heavily influenced by abnormal lipid metabolism.4,5 In a study conducted by Song et al, the risk of CVDs in both men and women increased threefold with every unit rise in blood total cholesterol.6
Globally, CVDs are the major cause of mortality and disability among all non-communicable diseases (NCD).7,8 According to the WHO, 12 million fatalities occur worldwide each year as a result of CVDs, including heart failure, stroke, and sudden cardiac death. Although there are various efforts have been made to reduce the occurrence of CVDs, these illnesses are the leading cause of death in many nations. The result of considerable research indicates that 40–45% of deaths are caused by CVD.9
The American Academy of Family Physicians (AAFP) defines dyslipidemias as abnormalities of lipoprotein metabolism involving excessive or deficient lipoprotein production. These conditions may be characterized by an increase in total blood cholesterol, LDL cholesterol, and triglyceride concentrations as well as a reduction in high-density lipoprotein (HDL) cholesterol concentration.10 Atherosclerotic cardiovascular disease (ASCVD) is associated with serum cholesterol and its lipoprotein carriers (LDL, very low-density lipoprotein [VLDL], and HDL). Low-density lipoprotein cholesterol (LDL-C) is the predominant type of atherogenic cholesterol. VLDL is the primary transporter of triglycerides, and VLDL cholesterol is atherogenic. HDL-C does not appear to be atherogenic.
Dyslipidemia can be classified into two types: primary dyslipidemia, which results from a genetic predisposition, and secondary dyslipidemia, which is complex and frequently associated with an underlying medical condition. Secondary dyslipidemia may be inherited genetically or not; however, it is typically linked to environmental, nutritional, and behavioral variables.11 Management of dyslipidemia can be related to lifestyle modification and pharmacotherapy. Lifestyle modifications involve adhering to a diet low in fat and intake of plenty of vegetables, fruits, whole grains, and polyunsaturated and monounsaturated oils, maintaining a regular exercise routine, tobacco cessation, limiting alcohol intake and maintaining a healthy body weight.12 Statins are the first-line drugs of dyslipidemia treatment. If patients do not meet the required normal values for lipid levels with maximally tolerated statin doses, alternatives can be added. Ezetimibe should be explored for primary prevention or when LDL-C levels are near to goal, or PCSK9 inhibitors for individuals at higher risk or who require more LDL-C reduction.13
It has been demonstrated that some groups, such as those who are overweight (ie, body mass index [BMI] of 25–30 kg/m2) or obese (BMI of 30 kg/m2), have a family history of high cholesterol or triglycerides, are over 40 years of age, and/or who smoke have comparatively higher odds of developing high cholesterol or triglycerides.14 Other risk factors may include unhealthy lifestyle habits (eg, a diet high in saturated fats, lack of physical activity, and stress), other medical conditions (eg, chronic kidney disease and hypothyroidism), medications (eg, steroids and immunosuppressive medicines), and gender. According to the National Heart, Lung, and Blood Institute, men between the ages of 20 and 39 years have higher cholesterol levels than women.15
The World Health Survey in Saudi Arabia in 2019 revealed that the prevalence of hypercholesterolemia among adults in several regions in Saudi Arabia varied from 25.5% in the Al-Baha region to 63.6% in the Northern Borders region. The Jazan region was indicated to have a relatively high rate of hypercholesterolemia among adults with a prevalence of 53%.
The high prevalence of hypercholesterolemia in this region emphasizes the importance of ascertaining the prevalence of associated risk factors. Identification of the associated risk factors in the population can facilitate the provision of primary and secondary prevention strategies. Data about the prevalence of the distribution of dyslipidemia determinants in the Jazan region are currently limited. This study aims to establish the prevalence of dyslipidemia determinants among a sample of adults from Jazan and to measure the practice of routine lipid profile assessment among adults in Jazan.
Methods
Study Design and Setting
This study was accomplished by use of a cross-sectional design targeted at adult subjects attending primary healthcare centers (PHCs) in the Jazan region. The investigation was initiated after securing ethical approval from the Jazan Health Ethics Committee (approval number 2317, dated February 2023). Data collection was performed from the beginning of March until the end of April 2023. A study information sheet was shared with the participants before the recruitment. Participants were recruited after they gave verbal informed consent. A request of waiver of documenting the informed consent was approved by the Jazan Health Ethics Committee after declaring that the data collection tool is anonymous and does not require collection of any identification data. The study was conducted in accordance with the Declaration of Helsinki.
Data Collection Tool
A questionnaire was developed by consulting the relevant literature on measuring the prevalence of dyslipidemia and its determinants.16,17 The recruited individuals were interviewed using a questionnaire that consisted of three sections. The first section inquired about demographic characteristics of the participants such as age, gender, and education level. The second section was about routine dyslipidemia screening practices and whether participants had been diagnosed with dyslipidemia. The second section also asked the participants about any family history of dyslipidemia, history of chronic illnesses, and their lifestyle practices and behaviors such as sleep patterns and physical activities during the preceding week. The third section was about dietary consumption and included a food frequency questionnaire developed for Saudi Arabian populations. The validity and reliability of the utilized food frequency questionnaire is described separately.16 Participants were asked in detail about their dietary habits, including the foods they eat, their average food consumption, and their cooking methods.
Food items were classified into healthier and less healthy categories based on their lipid and carbohydrate contents and were then compared to other food items in the same category. Information on the lipid and carbohydrate contents was obtained from the FoodData Central data system of the US Department of Agriculture’s agricultural research services.18 Subsequently, some food items were further classified into healthier and less healthy categories based on whether they contained more saturated fats than other items in the same category (eg, red meats have more saturated fat than skinless chicken or fish), and processed foods were categorized as less healthy than their counterparts. When comparing red meats against each other, camel meat was found to be healthier than beef or lamb due to its lower fat and cholesterol content. Fruits and vegetables were classified as healthier food items. Nuts, legumes, low-fat, and non-fat dairy products were classified as healthier foods.19,20 Further classification of food items was based on the method of cooking. For example, foods that are fried were considered less healthy than those that were grilled or boiled. Based on the above classification of food items, participants were divided into groups that consumed either high fat content diets or low fat content diets.
The final version of the questionnaire was reviewed by three physicians (preventive, family medicine, and internal medicine consultants) to evaluate the validity of the content. The questionnaire was also piloted on a sample of 10 participants to test the clarity of the questions and measure the time needed to complete the questionnaire.
Data Collection Process
Participants were identified when they visited PHC clinics in several randomly selected PHCs and were subsequently approached and interviewed. Participants who completed the entire interview were considered to have been recruited successfully. The targeted participants were all adults who visited various PHCs during the recruitment process.
The study was sure to include participants who were primary healthcare attendees of all nationalities and both genders who were living in the Jazan region. Individuals who did not attend PHCs and/or who were younger than 18 years old were excluded. Interviews were performed by trained data collectors in suitable settings in the selected PHCs.
Multistage-stratified random sampling was utilized to reach the required sample size of the current investigation. The first step in the process was identifying the five governorates in the Jazan region that have relatively high population densities: Jazan, Sabya, Abu-Arish, Baish, and Samtah.21 The second stage was random selection from the 23 total PHCs in the five governorates, five of which were selected via simple random sampling with the lottery method. The last stage was proportionate stratified sampling of the study participants; a third of the attendees were recruited to the study sample.
Sample-size estimation for the survey was conducted using the StatCalc function of Epi Info. Based on current evidence from previous studies that calculated the prevalence of dyslipidemia in the Saudi population, 8% of the potential participants were chosen for this study.3 Assuming a 5% margin of error, 99% confidence level, and 20% nonresponse rate, the estimated sample size is a minimum of 235 participants.22
Data Analysis
The Statistical Package for the Social Sciences version 24.0 was used to examine the data. Frequencies and proportions were used to summarize binary and categorical data while means, medians, standard deviations, and interquartile ranges were used to summarize continuous variables according to their distribution.
The assessment of the distribution of dyslipidemia determinants among the studied sample was based on 15 items, including dietary risks such as the addition of oil or margarine to foods, consumption of visible fat, and consumption of a high-fat diet. History of smoking was included as one of the risk factors of dyslipidemia. Use of hypertension (HTN) medications and cortisone were similarly assessed as risk factors. The risk assessment involved diagnosis of medical conditions including hypothyroidism, polycystic ovarian syndrome (PCOS), HTN, and diabetes mellitus. Family history of dyslipidemia was also an assessed risk factor. Finally, a BMI above 25, a low level of physical activity (ie, less than 150 minutes per week of moderate or vigorous activity), and an age of over 35 for males and 40 for females were assessed as dyslipidemia risk factors. A score level was calculated for each participant by giving a value of 1 for each risk factor present and summing the total. The median of the dyslipidemia risk score was used to classify the sample into lower risk or higher risk categories among subjects who had not been diagnosed with dyslipidemia.
A chi-square test was used to examine the statistical difference between the demographic characteristics of individuals who had reported previously checking their lipid profile to those who reported never performing a lipid profile check-up. The later analysis was restricted to the participants who had not been diagnosed with dyslipidemia and were not on lipid lowering agents. A p-value of less than 0.05 was used to determine statistical significance.
Results
The current study included a total of 244 participants. The participants’ demographic characteristics are shown in Table 1. The median age of the participants was 27 years, most of the participants were female (66.8%), and approximately 59% of them had a university education or above. In terms of monthly income, more than half the participants (57.4%) had an average monthly income of less than 5000 Saudi Arabian Riyals. More than half of the participants (54.9%) reported living in rural areas. When the participants were asked about marital status, about (47.1%) were single and around (46.7%) were married. Finally, majority of the participants have never been smokers (83.2%), and more than half (51.6%) had a BMI greater than 25.
 |
Table 1 Demographic Characteristics of 244 Adults from Jazan Region, Saudi Arabia |
Table 2 shows the participants’ medical history, including diagnosis of dyslipidemia, other comorbidities, use of medications that can increase cholesterol levels, and family history of various diseases. The proportion of participants who reported having checked their lipid profile was 39.8%. Additionally, 20% of the recruited participants reported being diagnosed with dyslipidemia at the time of recruitment. When participants were asked about the location of their lipid profile check-up, 16% reported that they typically checked their lipid profile in private labs, while 13.1% checked their lipid profile in governmental hospitals.
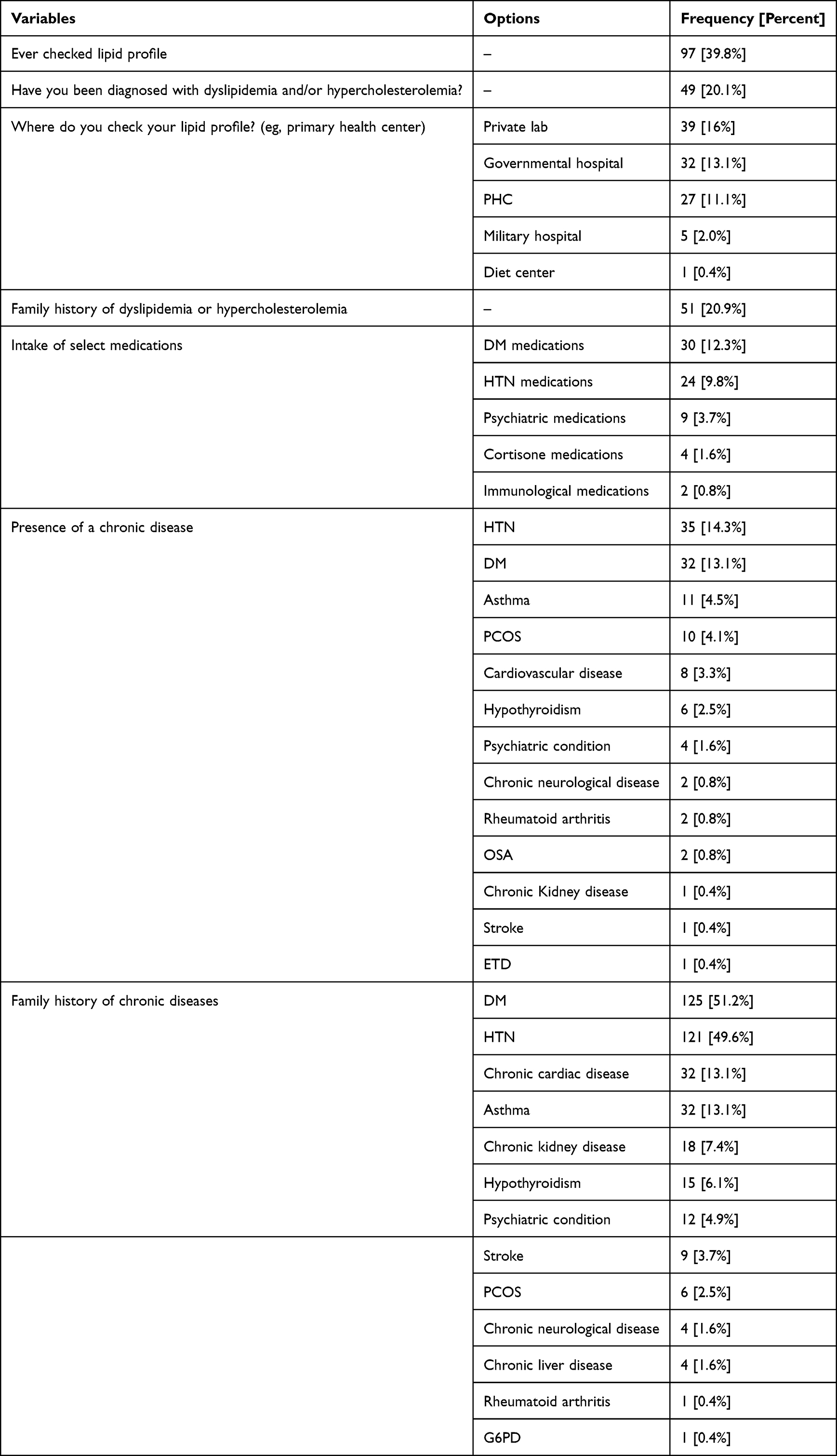 |
Table 2 Status of Dyslipidemia Diagnoses and Check-Ups, the Intake of Selected Medications, and Personal and Family History of Chronic Illnesses Among 244 Residents of the Jazan Region, Saudi Arabia |
Approximately 20.9% of participants reported having family history of dyslipidemia or hypercholesterolemia. Use of medications associated with dyslipidemia indicated that 12.3% of participants were on antidiabetic medications while 9.8% reported taking antihypertensive medications. Further, 3.7% and 1.6% of the participants reported taking psychiatric and cortisone medications, respectively.
History of chronic illnesses indicated that after dyslipidemia, the most frequently diagnosed chronic condition among the sample was hypertension (14.3%), which was closely followed by diabetes mellitus (13.1%). Similarly, inquiring about family history of chronic conditions revealed a high prevalence of family history of chronic diseases, as 51% of the participants reported family history of diabetes mellitus, and 49% of the participants reported family history of hypertension.
Distribution of dyslipidemia risk factors among the 195 undiagnosed participants is displayed in Figure 1. Physical inactivity was prevalent among the participants, as no participants reported achieving the recommended 150 minutes of physical activity per week. Analyzing eating behavior as demonstrated via the completed food frequency questionnaire indicated that almost half the participants consumed a high-fat diet. Additionally, more than 70 participants reported adding oil during cooking or prior to eating. Finally, more than half the participants had a BMI greater than 25.
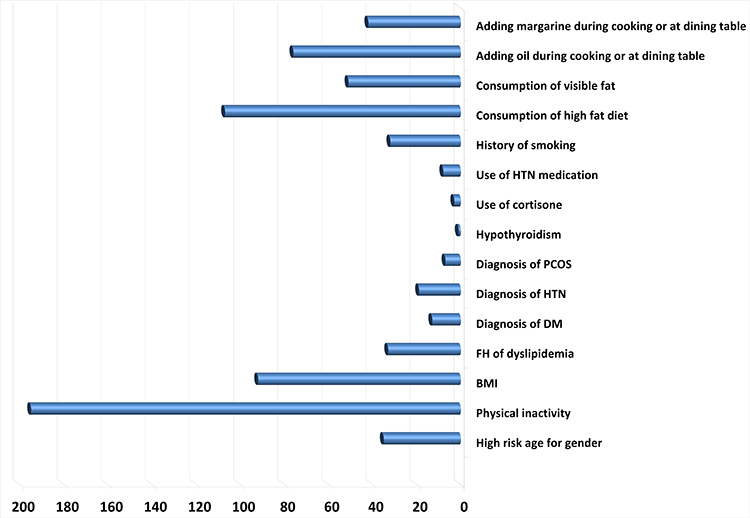 |
Figure 1 Number of individuals with dyslipidemia risk factors among 195 undiagnosed participants from the Jazan region, Saudi Arabia. |
Lipid profile check-up practices according to the demographic characteristics of the 195 undiagnosed adult participants are shown in Table 3. Age, gender, area of residence, occupation, education, marital status, and monthly income appeared to be significant indicators of whether participants had checked their lipid profile, with a p-value <0.05. Among the undiagnosed adults, older subjects were more likely to report checking their lipid profile in comparison to younger individuals. Additionally, male participants reported more frequently checking their lipid profile in comparison to female participants. When comparing the frequency of lipid profile check-ups according to occupation and level of education, housewives, unemployed individuals, and those with a university education reported more frequent lipid profile check-ups in comparison to other groups. However, this can be contributed to the effect of age, as unemployed individuals (including retired subjects) and those with higher education levels tended to be older in comparison to individuals in other categories. Subjects with higher incomes reported more frequent checking of their lipid profile, which can be partially attributed to the fact that these subjects preferred to use private labs to perform their analysis in comparison to others who reported use of freely available healthcare services provided by governmental health facilities. However, older subjects were likely to have higher income compared to those who were younger, thus contributing to the higher frequency of lipid profile check-ups among those with higher incomes. Conversely, a high BMI and being at higher risk for dyslipidemia were insignificant for lipid profile check-up.
 |
Table 3 Distribution of Having Checked Lipid Profile with Demographic Characteristics and Dyslipidemia Risk Assessment Among 195 Undiagnosed Adult Residents from the Jazan Region, Saudi Arabia |
Discussion
The findings of this cross-sectional study indicate that nearly one-fifth of the study sample was diagnosed with dyslipidemia. The study revealed that those who had never been diagnosed with dyslipidemia have multiple risk factors for developing dyslipidemia in the future.
Nearly 61% of the sample reported never checking their lipid profile. The dyslipidemia risk assessment among those who were not diagnosed with dyslipidemia indicated a high prevalence of physical inactivity and high level of consumption of food items with high lipid content, and nearly half of the undiagnosed subjects were either overweight or obese.
The findings of the current investigation can be compared to similar local or international investigations. A nationwide study by AlMuhaidib et al involved a sample of 5854 adolescents aged between 10 and 19, only 104 of whom were recruited from Jazan. It was concluded that nearly 25% of the recruited sample of adolescents were affected by dyslipidemia on a national level, as the prevalence of dyslipidemia in Jazan was 27.9%.11
Although our study was restricted to an adult population, the high prevalence of dyslipidemia risk factors suggests a potential increase in the prevalence of dyslipidemia among the population in Jazan. Furthermore, the method of assessing dyslipidemia risk factors, such as the use of a detailed FFQ, was not adopted in the study by AlMuhaidib et al in a manner that is similar to the current investigation. However, it is arguable that a similar distribution of risk factors of dyslipidemia were identified among the Saudi adolescents, including high prevalence of being overweight and certain dietary habits, such as high consumption of carbonated beverages among adolescents.
A study conducted by Enani et al that targeted 1385 adult subjects from Jeddah, Saudi Arabia, concluded that the prevalence of dyslipidemia among the sample reached 62%, and the prevalence was higher among men in comparison to women. The study by Enani et al identified a variation of dyslipidemia risk according to gender, reporting that consuming Turkish coffee or carbonated drinks, smoking, and sleeping for less than six hours were risk factors for dyslipidemia among males, while consumption of fresh vegetables was associated with a higher risk of dyslipidemia among females, which was attributed to added salad dressings.23 Our investigation did not perform a comparison of the distribution of risk factors according to the gender due to the smaller recruited sample size.
Another study conducted in Tabuk city in the north of Saudi Arabia included a sample of 400 patients diagnosed with diabetes mellitus and assessed the prevalence of dyslipidemia. The prevalence of dyslipidemia among this sample was 66.5%. The higher prevalence of dyslipidemia among patients with diabetes in comparison to our sample, which included patients with no comorbidities, is expected. However, a similar distribution of risk factors was found, including being older than 40, irregularly exercising, and being overweight or obese.24 In another similar study conducted in Jeddah, Saudi Arabia, that recruited 613 subjects who attended PHCs, it was concluded that the prevalence of dyslipidemia among the sample was 54.2%, and prediabetes was detected among 28.7% of the sample. Being in a prediabetes stage was found to be a risk factor for dyslipidemia.25
Comparing the findings of our investigation to similar regional settings revealed similar findings. A cross-sectional study was conducted by Habiba I. Ali et al in 2020 on 610 subjects in the United Arab Emirates to find associations of dyslipidemia with dietary intakes, body weight, and sociodemographic factors among adults. Around 72% of the subjects who had dyslipidemia were found to be overweight or obese. Moreover, diabetes, hypertension, and cardiovascular disease history were significantly prevalent among those who had dyslipidemia. When considering dietary habits, those with dyslipidemia appeared to be consuming higher fat content than those without dyslipidemia.26
The current investigation identified a low amount of routine check-ups for lipid profiles. This is similar to a study conducted by Gosadi et al, which targeted a sample of 516 adult subjects from Jazan to assess their practices concerning performing routine medical check-ups, including assessment of their lipid profile parameters. According to Gosadi et al, nearly 84% of their sample reported never assessing their lipid profile.27 Furthermore, in a study that targeted 675 patients diagnosed with various chronic non-communicable diseases in the Jazan region, it was concluded that only 10.5% of the patients were knowledgeable of their lipid profile parameters.28 This indicates that the practice of adults in Jazan measuring their lipid profile can be less than optimum and not consistent with the detected higher prevalence of dyslipidemia risk factors among adults in Jazan.
Dyslipidemia can be preventable, and adherence to practices reducing exposure to risk factor is essential for optimum prevention and control of dyslipidemia as well as prevention of subsequent clinical complications. In recent years, the frequency of CVD cases in the Middle East has steadily climbed. This is thought to be due to a combination of variables such as fast socioeconomic growth, lifestyle changes, urbanization, and aging. The prevalence of CVDs has been found to be 5% in the Kingdom of Saudi Arabia. Hyperlipidemia has been established as a significant risk factor for CVD.29 However, screening effort for dyslipidemia among Saudis can be suggested to be influenced via factors related to healthcare delivery.
A study was conducted in the Jazan region that targeted 234 PHC physicians and inquired about practices of the physicians regarding adherence to guidelines of obesity and hypercholesterolemia prevention. It was concluded that only 42% of the sample of physicians adhered to guidelines pertaining to screening for hypercholesterolemia. Furthermore, only 13% of the physicians were adherent to the guidelines concerning the reduction of the risk of hypercholesterolemia practices.30 Similar results were identified in a sample of 77 physicians and clinical pharmacists from the Al-Hassa region in the east of Saudi Arabia, where a low level of knowledge about the changing recommendations of the American Health Association for managing dyslipidemia was observed among the sample.31 These findings indicate the importance of ensuring the adherence of healthcare providers in order to achieve optimum primary and secondary preventive goals against dyslipidemia.
Strengths and Limitations
The study had multiple strengths and weaknesses. The main strengths were identifying the prevalence of dyslipidemia among a sample with different demographic and clinical characteristics via multi-stage sampling. Furthermore, utilization of a validated FFQ may have provided a detailed description of dietary risk factors associated with dyslipidemia among the sample. Additionally, the current study found that many of the participants who had not been diagnosed with dyslipidemia had multiple risk factors that must be addressed and minimized as much as possible to prevent the development of dyslipidemia. However, participants were required to provide most of the data based on their recollections, subjecting the study to recall bias. Furthermore, this study was limited to inquiring about participants’ history of checking their lipid profile and history of dyslipidemia diagnosis, whereas actual measurements of lipid profile parameters might have enabled better assessment of the prevalence of dyslipidemia.
Conclusion
Our study was able to identify the prevalence of dyslipidemia among the participants. Majority of the participants had never checked their lipid profile. Multiple dyslipidemia risk factors were identified among the sample, including low levels of physical activity, high BMI levels, and consumption of food items with high levels of fat. The findings of the current investigation emphasize the importance of increasing awareness of risk of dyslipidemia among adults in the Jazan region. Additionally, modification of lifestyle associated with higher risk of dyslipidemia should be promoted among adults in the region. Furthermore, health authorities in Jazan are encouraged to adopt strategies that facilitate better routine check-ups for lipid profiles among PHC attendees in the region. Finally, future research recommendations should involve performing community-based assessments of lipid profile parameters among adults in the region, assessment of social and behavioral determinants associated with high lipid consumption, and utilization of interventional investigations to provide an evidence-based approach to modify exposure to lifestyle risk factors associated with dyslipidemia among adults in the Jazan region.
Author Contributions
All authors contributed significantly to the work that was published, whether this was in the conceptualization, study design, implementation, data collection, analysis, and interpretation or in all of these areas. They all also participated in writing, revising, or critically evaluating the article, gave their final approval for the version that would be published, agreed on the journal to which the article would be submitted, and agreed to be responsible for all aspects of the work.
Funding
This study received no support from any funding source.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The global health observatory. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3236.
2. Mattiuzzi C, Sanchis-Gomar F, Lippi G. Worldwide burden of LDL cholesterol: implications in cardiovascular disease. Nutr Metab Cardiovasc Dis. 2020;30(2):241–244. doi:10.1016/j.numecd.2019.09.008
3. Ministry of Health Saudi Arabia. World health survey Saudi Arabia 2019; 2019.
4. Saeed E, Ali R, Jalal-ud-din M, Saeed A, Jadoon RJ, Moiz M. Hypercholesterolemia in patients of ischemic stroke. J Ayub Med Coll Abbottabad. 2015;27(3):637–639.
5. Huang C, Zhang WQ, Tang WW, et al. Prevalence and related factors of dyslipidemia among urban adults aged 35 to 79 years in Southwestern China. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-96864-w
6. Song PK, Li H, Man QQ, Jia SS, Li LX, Zhang J. Trends in determinants of hypercholesterolemia among Chinese adults between 2002 and 2012: results from the national nutrition survey. Nutrients. 2017;9(3):279. doi:10.3390/nu9030279
7. Blacher J, Gabet A, Vallée A, et al. Prevalence and management of hypercholesterolemia in France, the Esteban observational study. Medicine. 2020;99(50):e23445. doi:10.1097/MD.0000000000023445
8. Mat Rifin H, Robert Lourdes TG, Abdul Majid NL, et al. Hypercholesterolemia prevalence, awareness, treatment and control among adults in Malaysia: the 2015 national health and morbidity survey, Malaysia. Glob J Health Sci. 2018;10(7):11. doi:10.5539/gjhs.v10n7p11
9. Toori MA, Kiani F, Sayehmiri F, et al. Prevalence of hypercholesterolemia, high LDL, and low HDL in Iran: a systematic review and meta-analysis. Iran J Med Sci. 2018;43(5):1.
10. Ahmed SM, Clasen ME, Donnelly JF. Management of dyslipidemia in adults. Am Fam Physician. 1998;57(9):1.
11. AlMuhaidib S, AlBuhairan F, Tamimi W, et al. Prevalence and factors associated with dyslipidemia among adolescents in Saudi Arabia. Sci Rep. 2022;12(1):16888. doi:10.1038/s41598-022-21262-9
12. Turgeon RD, Anderson TJ, Grégoire J, Pearson GJ. Updated guidelines for the management of dyslipidemia and prevention of cardiovascular disease by pharmacists. Can Pharm J. 2015;148(1):21–28. doi:10.1177/1715163514561256
13. Berberich AJ, Hegele RA. A modern approach to dyslipidemia. Endocr Rev. 2022;43(4):611–653. doi:10.1210/endrev/bnab037
14. Buendia J, Sears S, Mgbere O. Prevalence and risk factors of high cholesterol and triglycerides among people with HIV in Texas. AIDS Res Ther. 2022;19(1):43. doi:10.1186/s12981-022-00467-y
15. National Heart L, Blood Cholesterol BI. Blood cholesterol national heart, lung, and blood institute; 2022. Available from: https://www.nhlbi.nih.gov/health-topics/blood-cholesterol.
16. Gosadi IM, Alatar AA, Otayf MM, et al. Development of a Saudi food frequency questionnaire and testing its reliability and validity. Saudi Med J. 2017;38(6):636–641. doi:10.15537/smj.2017.6.20055
17. AHA. American Heart Association recommendations for physical activity in adults and kids. HeartOrg. 2018;501(c):2020.
18. U.S. DEPARTMENT OF AGRICULTURE. U.S. Department of agriculture (agricultural research service) website (food data central); 2023. Available from: https://fdc.nal.usda.gov/download-datasets.html#bkmk-1.
19. Baba WN, Rasool N, Selvamuthukumara M, Maqsood S. A review on nutritional composition, health benefits, and technological interventions for improving consumer acceptability of camel meat: an ethnic food of Middle East. J Ethnic Foods. 2021;8(1):18. doi:10.1186/s42779-021-00089-1
20. The American Heart Association. The American Heart Association diet and lifestyle recommendations; 2021. Available from: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/nutrition-basics/aha-diet-and-lifestyle-recommendations.
21. General Authority for Statistics. Population distribution (Saudis and Non Saudis) in governorates of Jazan Region; 2011. Available from: https://www.stats.gov.sa/en/4601.
22. Alshammari S, Alenazi H, Alshammari H. Knowledge, attitude and practice towards early screening of colorectal cancer in Riyadh. J Family Med Prim Care. 2020;9(5):2273. doi:10.4103/jfmpc.jfmpc_290_20
23. Enani S, Bahijri S, Malibary M, et al. The association between dyslipidemia, dietary habits and other lifestyle indicators among non-diabetic attendees of primary health care centers in Jeddah, Saudi Arabia. Nutrients. 2020;12(8):2441. doi:10.3390/nu12082441
24. Alzaheb RA, Altemani AH. Prevalence and associated factors of dyslipidemia among adults with type 2 diabetes mellitus in Saudi Arabia. Diabetes Metab Syndr Obes. 2020;13. doi:10.2147/DMSO.S246068
25. Al Amri T, Bahijri S, Al-Raddadi R, et al. The association between prediabetes and dyslipidemia among attendants of primary care health centers in Jeddah, Saudi Arabia. Diabetes Metab Syndr Obes. 2019:12. doi:10.2147/DMSO.S233717
26. Ali H, Elmi F, Stojanovska L, Ibrahim N, Ismail L, Al Dhaheri A. Associations of dyslipidemia with dietary intakes, body weight status and sociodemographic factors among adults in the United Arab Emirates. Nutrients. 2022;14:3405. doi:10.3390/nu14163405
27. Gosadi IM, Ayoub RA, Albrahim HT, et al. An assessment of the knowledge and practices of adults in Jazan, Saudi Arabia, concerning routine medical checkups. Patient Prefer Adherence. 2022;16:1955–1969. doi:10.2147/PPA.S376345
28. Gosadi IM, Daghriri KA, Otayf AA, et al. Are patients affected by chronic non-communicable diseases aware of their own clinical and laboratory parameters? A cross-sectional study from the south of Saudi Arabia. Saudi J Biol Sci. 2021;28(5):2951–2955. doi:10.1016/j.sjbs.2021.02.032
29. Al-Hassan YT, Fabella EL, Estrella E, Aatif M. Prevalence and determinants of dyslipidemia: data from a Saudi university clinic. Open Public Health J. 2018;11(1):416–424. doi:10.2174/1874944501811010416
30. Gosadi IM. Utilization of evidence-based guidelines for prevention of obesity and hypercholesterolemia among primary healthcare physicians in southwest of Saudi Arabia. Medicine. 2021;100(49). doi:10.1097/MD.0000000000028152
31. Zaitoun MF, Iflaifel MH, Almulhim LA, Al-Ghamdi MA, Ibrahim YA. Awareness of physicians and clinical pharmacists about ACC/AHA guidelines for dyslipidemia management: a cross sectional study. J Pharm Bioallied Sci. 2019;11(2):181–186. doi:10.4103/JPBS.JPBS_59_18
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.