")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Prevalence of cryptosporidiosis and hygiene practices among HIV/AIDS patients in southwest Uganda
Authors Nakibirango J, Mugenyi V, Nsaba D , Nsimemukama A, Rugera SP , Okongo B
Received 21 February 2019
Accepted for publication 8 May 2019
Published 18 June 2019 Volume 2019:11 Pages 141—145
DOI https://doi.org/10.2147/HIV.S206195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Juliet Nakibirango, Vincent Mugenyi, Dickson Nsaba, Aron Nsimemukama, Simon Peter Rugera, Benson Okongo
Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
Purpose: To determine the prevalence of Cryptosporidium by age, sex, and duration on antiretroviral therapy (ART) and establish hygienic malpractices that may predispose to infection.
Methods: We enrolled 138 HIV/AIDS patients on ART from June to October 2018. Stool samples were collected from study participants, wet saline preparations made and examined, stool samples concentrated using formal ether concentration, and smears stained using the modified Ziehl–Neelsen technique. Structured questionnaires were used to collect demographic data and hygienic malpractices that predisposed study participants to cryptosporidiosis infection.
Results: Of 138, 99 (71.7%) were females and 39 (28.7%) males. The age range was 9–69 years and mean age 37 years. The overall prevalence of cryptosporidiosis was three (2.17%). The most affected age-groups were 31–40 years (3.85%) and 21–30 years (3.22%), and only females (3.03%) were affected. The distribution of cryptosporidiosis according to the duration spent on ART showed that those who had spent <1 year on ART were the most affected (11.1%), followed by those who had spent 1–5 years 1 (2.2%), while those patients on ART for 6-10 years were 1 (1.7%) and those on ART for more than 10 years were not affected. There was no significant association between cryptosporidiosis and sex (P=0.272), educational background (P=0.670), handwashing (P=0.853), drinking boiled water (P=0.818), duration on ART (P=0.263), occupation (P=0.836), and age (P=0.723).
Conclusion: The prevalence reported in this study is low; however, it is still vital for clinicians to proceed to have cryptosporidiosis as the main differential in HIV/AIDS patients with gastrointestinal infections.
Keywords: Cryptosporidium, HIV/AIDS, diarrhoea, prevalence, risk factors
Introduction
Cryptosporidium infection has been reported as one of the most important causes of diarrheal illnesses worldwide, particularly in young children and immunocompromised patients, with a prevalence of 4% in developed countries and three to four times that in developing countries.1 It is one of the most common causes of diarrhea in immunocompromised patients, leading to significant morbidity and mortality worldwide.2,3 The prevalence of cryptosporidiosis is higher in people with immunodeficiency syndromes and diarrheal patients. The disease in immunocompetent persons manifests as self-limiting diarrhea, whereas in the immunosuppressed it manifests as chronic, severe diarrhea that can be fatal.4 Even patients with advanced AIDS who are on antiretroviral therapy (ART) have been reported to have Cryptosporidium infection.5
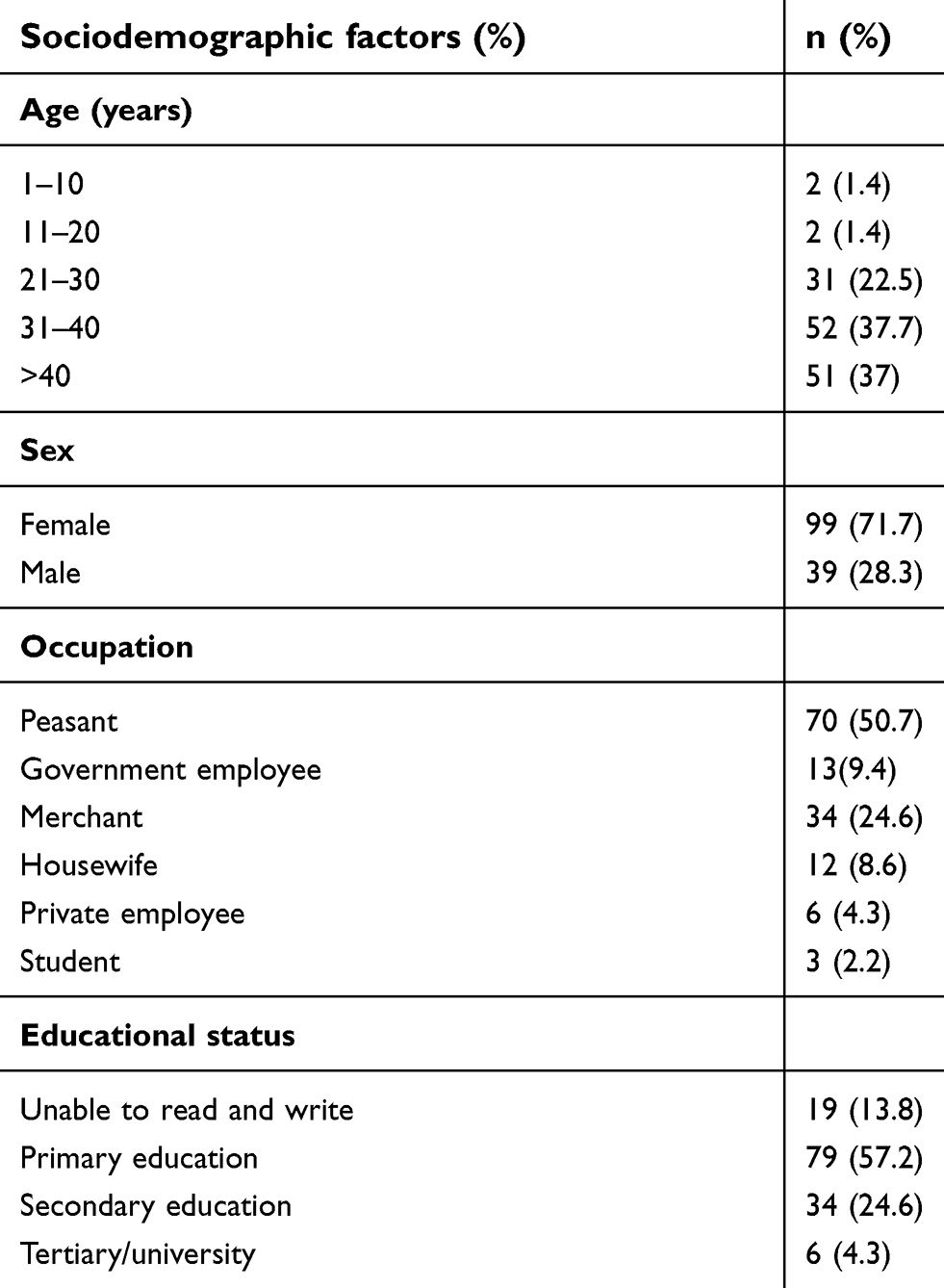 | Table 1 Sociodemographic characteristics of the study participants |
In developed countries, access to highly active ART (HAART) has considerably reduced morbidity and mortality due to cryptosporidiosis.6 Nonetheless, cryptosporidiosis remains a key threat to AIDS patients who do not have access to HAART, particularly in developing countries.7 Though the introduction of HAART has substantially reduced the risk of suffering from an opportunistic infection,8 HIV-positive patients in resource-poor settings continue to suffer from opportunistic infections due to several factors, including late HIV diagnosis, suboptimal HAART use, poor treatment adherence, drug resistance, poverty, poor nutrition, and high exposure to infectious agents.9
Various risk factors, such as using contaminated drinking water and exposure to animals, have been reported to be associated with the gastrointestinal infection.10 The rise of drug-resistant HIV variants and failure or discontinuation of ART has been associated with reemergence of Cryptosporidium infection in these patients.11
A Uganda population-based HIV-impact assessment12 indicated that the total number of adults and children of all ages living with HIV in Uganda was estimated to be approximately 1.3 million (6%). The majority of these patients live in rural areas, where access to treatment is very difficult, and this may put these HIV/AIDS patients at risk of acquiring opportunistic infections, including cryptosporidiosis.
The purpose of this study was to provide fresh insight into the prevalence of cryptosporidiosis and hygiene practices in HIV/AIDS patients attending the ART clinic at Mbarara Municipal Council Health Centre IV in southwest Uganda.
Methods
Study area and design
The study was carried out at Mbarara Municipal Council Health Centre IV in southwest Uganda. The center is located in Mbarara municipality, and is 238 km from the capital city — Kampala. It offers several outpatient services to the population of the municipality, including an ART clinic that attends to HIV/AIDS patients, voluntary testing and counseling, voluntary medical circumcision, tuberculosis treatment, elimination of mother-to-child HIV transmission, sex- and gender-based violence services, and family planning.
This was a cross sectional study carried out from June to October 2017 to determine the prevalence of cryptosporidiosis and hygiene practices among HIV/AIDS patients accessing ART at the health center. All HIV/AIDS patients who were included in the study and consented were briefed on the intentions and objectives of the study. A nonprobability simple random-sampling technique was used to recruit study participants. The sample size of 138 for this study was calculated by a statistical formula based on a 10%-prevalence study13 to have 80% power with 95% confidence-estimate precision of ~5%.
A total of 138 stool samples were collected from consenting HIV-positive patients accessing ART at the health center. A structured questionnaire was used to obtain patients' hygiene practices (handwashing after using the toilet and before eating, drinking boiled water, duration on ART, and demographic characteristics like age, sex, level of education, and occupation). Stool samples were collected in sterile stool containers by study participants and transferred immediately to the internal medicine ward laboratory for analysis.
Samples were examined macroscopically and microscopically for any other intestinal parasites, concentrated using formal ether concentration, smears made from the deposits, air-dried at room temperature, fixed using absolute methanol for 1 minute, and stained using the modified Ziehl–Neelsen technique. Microscopic examination of each smear was done using 100× oil immersion, and approximately 200–300 microscopic fields were examined for the presence of Cryptosporidium oocysts.
Data entry and analysis
Data collected were entered in Excel spreadsheets and then exported to Stata version 12 for analysis. Descriptive demographic data are summarized as frequency and percentages. The proportion of those infected with Cryptosporidium was analyzed on the basis of sex, age-group, and duration on ART, and χ2 was used to determine the association between disease (cryptosporidiosis) and patient characteristics. P<0.05 was considered significant.
Consent
The authors confirm that all study participants were adequately informed of the aims of the study and voluntarily provided written informed consent for their details to be used in this study. Those aged <18 years had assent provided by their parents. They were also informed of the right to refuse to participate in the study or withdraw consent to participate at any time without reprisal. We also ensured that all patient-identifying information/data were anonymized, and only code numbers were used for matter of confidentiality.
Ethical approval
This study was approved by the Faculty Research Committee of Mbarara University of Science and Technology, Uganda.
Results
Sociodemographic characteristics of study participants
Of the 138 study participants, 96 (71.1%) were female and 39 (29%) male. The mean age was 37.1 years, and age distribution was 1–10 years 1.5%, 11–21 years 1.5%, 22–32 years 22%, 33–43 years 37%, and >43 years 38%. According to occupation, 78 (57.8%) were peasants, 36 (26.7%) businessmen and -women, and others 15.7%. The majority (57.2%) had stopped education at the primary level, followed by those with secondary education (24.6%) and tertiary/university 4.3%, while 13.8 % were unable to read (Table 1).
Prevalence of cryptosporidiosis
Cryptosporidium spp. and Cystoisospora belli were the only coccidia detected. The overall prevalence of Cryptosporidium spp. was three (2.17%) and C. belli one (0.72%). Other intestinal parasites detected were one each (0.72%) of Giardia lamblia, hookworm, Ascaris lumbricoides, and Schistosoma mansoni. The most affected age-groups were 31–40 years (3.85%) and 21–30 years (3.22%), and only females were affected (3.03%). The distribution of cryptosporidiosis according to duration of ART showed that those with <1 year on ART were the most affected (11.1%), followed by 1–5 years (2.2%), while those with ≥10 years ART were not affected.
Association between HIV/AIDS patients' hygiene practices and Cryptosporidium infection
Hygiene practices that were assessed using structured questionnaires were handwashing after use of the toilet and before eating, drinking boiled water, duration on ART, and demographic characteristics like, age, sex, and occupation. There was no significant association observed between Cryptosporidium and hygiene practices (handwashing χ2=0.3189, P=0.853, drinking boiled water χ2=0.4022, P=0.818, duration on ART χ2=3.9867, P=0.263) or demographic characteristics (age χ2=2.0673, P=0.723, sex χ2=1.2081, P=0.272, occupation χ2=1.4471, P=0.836).
Discussion
The prevalence of cryptosporidiosis in HIV/AIDS patients attending the ART clinic at the Mbarara Municipal Council Health Centre IV was three (2.17%), lower than a study carried out in Bushenyi (16.2%).13 It is lower still than that obtained from a similar study done in Kinshasa (5.4%)14 and one in Iran.15 This difference may be accounted for by the fact that in the latter study, a relatively large proportion (39%) were not on ART, whereas in our study all patients were on ART. Research has shown that the use of ART reduces the prevalence of the disease in AIDS patients.11
This study still disagreed with a similar one done16 in Kenya (prevalence 10% on microscopy and 34% on PCR), and it was not comparable either with a study in Ethiopia (26.9%).17 This disparity may be attributed to the more sensitive technique used (PCR) to detect infection with Cryptosporidium compared to our study, where only microscopy was used, and a larger sample in both the Kenyan and Ethiopian studies. However, the disparity in microscopy results may be attributed to our smaller sample.16
The prevalence obtained from this study (2.17%) contrasts with comparable studies in African countries, which yielded prevalence of 3.6% in Uganda and 34.1% in Kenya in HIV-positive patients.18 These higher values were attributed to poor hygiene, ie, eating unwashed or raw fruit and drinking underground or tap water. However, it is comparable with a similar study from the AIDS Support Organization (TASO) in Uganda, with 3.3% prevalence.19 The lower prevalence obtained in our study may have been due to a higher proportion of participants practicing good hygiene, ie, handwashing (90.6%) and drinking boiled water (88.4%). Nevertheless, our results showed no statistical significance between cryptosporidiosis and participant hygiene practices compared to the above study, this may be attributed to a small sample size used in our study.
The prevalence of cryptosporidiosis was highest among participants aged 31–40 years, followed by the age-group 21–30 years. This is similar to results obtained in the TASO study, where infection rates among HIV-positive patients were higher among patients aged 30–39 years,19 but differs from the study in Bushenyi, with high prevalence seen among those aged 25–34 years, with 52.9% prevalence.20 This higher prevalence may be attributed to poor personal hygiene and lack of sanitation services like accommodation, toilets, bathrooms, and clean water, domestic animal keeping, and contaminated soil. Participants were predominantly peasants with similar occupations, cultural traditions, and living conditions. Prevalence was still higher among females (3.03%) compared to males (0), as was the case in the study in Bushenyi,13 though different from the TASO study, which showed equal distribution of cryptosporidiosis prevalence by sex, with females 3.8% and males 3.5%.19 This was possibly because more participants were female (n=16,519) than male (n=7,848).
The prevalence of cryptosporidium by duration on ART among the study participants was 2.2% among those who had been a year on ART, 1.7% among those who had been on ART >3 years, and 0 among those who had spent >10 years on ART. This finding is comparable with another study in Uganda, where the prevalence dropped from 3.6% to 1.2% among HIV patients in their early period on ART and those who had been on ART >3 years. This study further endorses prior reports that increased vulnerability of HIV-seropositive individuals to parasitic infections is associated with CD4+ T-cell counts <200 cells/mm.3 With increased D4+ T-cell count, spontaneous clearing of the parasites take place.21
Our study revealed no statistical significance between cryptosporidiosis and sociodemographic or epidemiological characteristics of the participants (age, sex, education level, occupation, handwashing, drinking boiled water, and duration on ART), comparable with a study in Kenya.16 Other intestinal parasitic and protozoan infections found were G. lamblia, hookworm, A. lumbricoides, and S. mansoni. Both protozoa and intestinal helminthes have been commonly associated with abdominal distention, vomiting, and weight loss in children and HIV individuals.22,23
Conclusion
The prevalence of cryptosporidiosis among HIV/AIDS patients attending the ART clinic at Mbarara Municipal Council Health Center IV was low compared to other similar studies done within Uganda. However, further research should be done with a bigger sample to draw conclusions. Modified Ziehl–Neelsen staining and wet saline preparation for stools of HIV/AIDS patients with diarrhea is recommended to rule out coccidia spp. and other intestinal parasites that cause diarrhea.
Acknowledgments
We acknowledge the staff of Mbarara Municipal Health Centre IV for their support during data collection. We also acknowledge Mr Robert Wagubi of the Internal Medicine Laboratory for allowing us to use this laboratory for analysis of the stool samples.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Iqbal A, Lim YA, Surin J, Sim BL, Arez AP. High diversity of Cryptosporidium subgenotypes identified in Malaysian HIV/AIDS individuals targeting gp60 gene. PLoS One. 2012;7(2):e31139. doi:10.1371/journal.pone.0031139
2. Dehkordy AB, Rafiei A, Alavi SM, Latifi SM. Prevalence of Cryptosporidium infection in immunocompromised patients, in south-west of Iran, 2009–10. Iran J Parasitol. 2010;5(4):42.
3. Agholi M, Hatam GR, Motazedian MH. HIV/AIDS-associated opportunistic protozoal diarrhea. AIDS Res Hum Retroviruses. 2013;29(1):35–41. doi:10.1089/AID.2012.0119
4. Cabada MMMCM. Cryptosporidiosis. 2016. Available from: https://emedicine.medscape.com/article/215490-overview. Accessed May 22, 2019.
5. O’Connor RM, Shaffie R, Kang G, Ward HD. Cryptosporidiosis in patients with HIV/AIDS. Int AIDS Soc J. 2011;25(5):549–560.
6. Zardi E, Picardi A, Afeltra A. Treatment of cryptosporidiosis in immunocompromised hosts. Chemotherapy. 2005;51(4):193–196. doi:10.1159/000086920
7. Werneck‐Silva AL, Prado IB. Gastroduodenal opportunistic infections and dyspepsia in HIV-infected patients in the era of Highly Active Antiretroviral Therapy. J Gastroenterol Hepatol. 2009;24(1):135–139. doi:10.1111/j.1440-1746.2008.05700.x
8. Iqbal A, Lim YA, Surin J, Sim BL. High diversity of Cryptosporidium subgenotypes identified in Malaysian HIV/AIDS individuals targeting gp60 gene. PLoS One. 2012;7(2):e31139. doi:10.1371/journal.pone
9. Moges N, Kassa G. Prevalence of opportunistic infections and associated factors among HIV positive patients taking anti-retroviral therapy in DebreMarkos Referral Hospital, Northwest Ethiopia. J AIDS Clin Res. 2014;5(5):1–300. doi:10.4172/2155-6113.1000301
10. Dwivedi KK, Prasad G, Saini S, Mahajan S, Lal S, Baveja UK. Enteric opportunistic parasites among HIV infected individuals: associated risk factors and immune status. Jpn J Infect Dis. 2007;60(2/3):76.
11. O’Connor RM, Shaffie R, Kang G, Ward HD. Cryptosporidiosis in patients with HIV/AIDS. Medscape. 2011;25(5):549–560.
12. Moh U. Uganda Population Based HIV Impact Assessment Survey. Ministry of Health Uganda: 2016.
13. Agwu E, Oming S, Moazzam M. Prevalence of Cryptosporidiosis among diarrhea patients attending clinics in Bushenyi district of Uganda. SPPJ. 2010;1(1):0014–0019.
14. Wumba R, Longo-Mbenza B, Menotti J, et al. Epidemiology, clinical, immune and molecular profiles of microsporidiosis and cryptosporidiosis among HIV/AIDS patients. PubMed. 2012;5:603–611.
15. Sangani GS, Mirjalali H, Farnia S, Rezaeian M. Prevalence of intestinal coccidial infections among different groups of immunocompromised patients. Iran J Parasitol. 2016;11(3):332.
16. Wanyiri JW, Kanyi H, Maina S, et al. Cryptosporidiosis in HIV/AIDS patients in Kenya: clinical features, epidemiology, molecular characterization and antibody responses. PubMed. 2014;2(91):319–328.
17. Adamu H, Petros B, Zhang G, et al. Distribution and clinical manifestations of Cryptosporidium species and subtypes in HIV/AIDS patients in Ethiopia. PLoS Negl Trop Dis. 2014;8(4):e2831. doi:10.1371/journal.pntd.0002831
18. Squire SA, Una R. Cryptosporidium and Giardia in Africa: current and future challenges. Parasites Vectors. 2017;10:157. doi:10.1186/s13071-017-2494-9
19. Rubaihayo J, Tumwesigye NM, Konde-Lule J, et al. Frequency and distribution patterns of opportunistic infections associated with HIV/AIDS in Uganda. BMC Res Notes. 2016;9(1):501. doi:10.1186/s13104-016-1938-1
20. Agwu E. Prevalence of Cryptosporidiosis among diarrhea patients attending clinics in Bushenyi district of Uganda. SPPJ. 2015;1,(1):0014–0020.
21. Khalil S, Mirdha BR, Sinha S, et al. Intestinal parasitosis in relation to anti-retroviral therapy, CD4+ T-cell count and diarrhea in HIV patients. Korean J Parasitol. 2015;53(6):705. doi:10.3347/kjp.2015.53.6.789
22. Banisch DM, El-Badry A, Klinnert JV, Ignatius R, El-Dib N. Simultaneous detection of Entamoeba histolytica/dispar, Giardia duodenalis and cryptosporidia by immunochromatographic assay in stool samples from patients living in the Greater Cairo Region, Egypt. World J Microbiol Biotechnol. 2015;31(8):1251–1258. doi:10.1007/s11274-015-1875-5
23. Morawski BM, Yunus M, Kerukadho E, et al. Hookworm infection is associated with decreased CD4+ T cell counts in HIV-infected adult Ugandans. PLoS Negl Trop Dis. 2017;11(5):e0005634. doi:10.1371/journal.pntd.0005634
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.