")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Prevalence of Clinical Cardiovascular Disease Risk Factors Among HIV Infected Patients on Anti-Retroviral Treatment in a Tertiary Hospital in Ethiopia
Authors Woldeyes E, Fisseha H , Mulatu HA, Ephrem A, Benti H, Alem MW, Ahmed AI
Received 3 March 2022
Accepted for publication 9 June 2022
Published 17 June 2022 Volume 2022:14 Pages 297—309
DOI https://doi.org/10.2147/HIV.S362459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Esubalew Woldeyes,1 Henok Fisseha,1 Hailu Abera Mulatu,1 Abiy Ephrem,1 Henok Benti,1 Mehari Wale Alem,2 Ahmed Ibrahim Ahmed3
1Department of Internal Medicine, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Neurosurgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Houston Methodist DeBakey Heart and Vascular Center, Houston, TX, USA
Correspondence: Esubalew Woldeyes, Email [email protected]
Background: Anti-retroviral treatment has improved mortality of human immunodeficiency virus (HIV) infected patients, which is offset by an increasing burden of cardiovascular diseases (CVD). Data regarding prevalence of cardiovascular disease risk factors in HIV infected patients in Ethiopia are very scarce. The aim of this study was to determine the prevalence of CVD risks and associated factors in patients with HIV.
Methods: A cross-sectional study was conducted on 333 patients with HIV infection, using a modified World Health Organization’s stepwise approach to surveillance questionnaire. Anthropometric and blood pressure measurement was done along with biochemical studies. Cardiovascular risk was estimated using Framingham risk score. Multivariate logistic regression was used to examine the association between cardiovascular risks and associated factors, with a p-value of < 0.05 considered statistically significant.
Results: The mean age of the participants was 45 years, and 69.2% were females. Most (80.9%) of the participants had viral load below 50 copies/mL and the mean CD4 count was 579 cells/mm3. Dyslipidemia was the most common risk factor identified in 69.4%, followed by abnormal fasting blood glucose (≥ 100 mg/dL) in 36.8%. Hypertension was diagnosed in 23.8%, while 22.8% and 11.1% had metabolic syndrome and obesity, respectively. Framingham risk score was low in 95.9%. Male gender, increasing age, high body mass index and previous ART regimen being tenofovir disoproxil fumarate, lamivudine and nevirapine increased CVD risk factors.
Conclusion: Traditional cardiovascular risk factors were high in the population studied. There is a need to raise awareness about the risk factors, and patients should have timely follow-up and care.
Keywords: human immunodeficiency virus, cardiovascular disease, risk factors
Introduction
Non-communicable diseases (NCDs) are showing an epidemic increase in sub-Saharan Africa (SSA). These NCDs include cardiovascular diseases (CVD), cancer and metabolic diseases. Much of the focus in SSA has traditionally been on infectious diseases, maternal and child health, with less focus on NCDs.1 Evidences show that low-income countries are now facing challenges from both NCDs and infectious diseases.1,2
Human immunodeficiency virus (HIV) is a global pandemic affecting more than 34 million people of which 69% (23.5 million) live in sub-Saharan Africa.3 HIV infected patients on antiretroviral therapy (ART) face a new group of complications and challenges.4 These include chronic diseases such as hypertension, diabetes, dyslipidemia, lipodystrophy and cardiovascular diseases that need their own treatment options, different from the usual infectious problems.4–6 The improved mortality of patients as a result of widespread use of ART is being offset by increasing death from CVD, cancer and liver diseases.7
A systematic review and meta-analysis showed the relative risk of CVDs to be 61% higher compared to non-infected individuals. This cardiovascular risk persisted even when patients are on ART.8 With increasing life expectancy of patients, their prolonged exposure to environmental and behavioral risks, along with prolonged exposure to ART can contribute to developing CVDs.8–10 Limited data on assessment of CVD risk factors in HIV infected people on ART from low-income countries exist.7,11,12 The incidence of NCDs brings significant adverse economic impact and strains the fragile healthcare system.13
Data regarding prevalence of cardiovascular risk factors in HIV infected patients in Ethiopia are very scanty. Available evidence suggests hypertension to be a major challenge along with diabetes, lipodystrophy and metabolic syndrome (MetS) with possible contribution of type and duration of ART to CVD risks.14–17 The prevalence of HIV in Ethiopia has shown a decline to 0.9%. However, this progress is being hampered by complacency towards preventative strategies.18 According to a recent systematic review and meta-analysis, the pooled prevalence of CVD in the general Ethiopian population was 5%.19 Therefore, it is imperative to assess the burden of CVD risk factors and determine their causes. This study aimed to fill the data gap regarding the prevalence and associated risk factors of cardiovascular risk factors in patients with HIV on ART in Ethiopian patients.
Methods
Study Design, Setting and Participants
A cross-sectional study was conducted on patients with HIV infection on ART at St. Paul’s hospital millennium medical college (SPHMMC) HIV treatment clinic in Addis Ababa, Ethiopia. Patients from urban and rural communities have follow-up in the clinic. There is no integration of HIV follow-up with CVD care services. There are a total of 4685 patients on active follow-up at adult HIV treatment clinic, with average daily patients of 70. There are 2520 patients that are expected to visit the clinic over the data collection period of 6 weeks from January 6, 2020 to February 15, 2020. As to the authors’ knowledge, despite previous studies reporting components of CVD risk factors, comprehensive assessment of CVD risk in HIV infected patients has not been reported.5,14–17 Therefore, assuming a 50% of prevalence of cardiovascular risk factors, 5% margin of error and 95% confidence interval, a sample size of 384 was calculated. Adjusting for the finite size of the population using population correction formula, the final calculated sample size was 333 patients. To minimize sampling bias, selection of participants was done using systematic random sampling from routine ART clinic visit, with every seventh patient coming in the morning for follow-up invited to participate in the study. All patients above 18 years of age who were on ART for at least 6 months and gave written consent to participate were included and pregnant patients were excluded. Patients were considered to be on ART if they were taking medications for at least 6 months, which was used in the pervious studies.
Data Collection
Data was collected using an interview based on a structured questionnaire modified from the STEP wise approach of the World Health Organization (WHO) for NCD surveillance in developing countries.20 The data collection had three parts. The first was interviewer administered questionnaires on socio-demographic characteristics and life style factors including tobacco and alcohol consumption, diet, prior history of CVD or risks, current ART regimen and previous ART regimen, if regimen was changed; followed by the second part consisting of anthropometric and blood pressure measurement. Data were collected by trained general practitioners. Finally, biochemical analysis was done to determine serum cholesterol and fasting blood glucose (FBG). Blood samples were collected after a 12-hour overnight fasting and analyzed with COBAS 6000 chemistry machine. CD4 count and viral load done in the previous 6 months were retrieved from patient follow-up charts.
Blood pressure was measured with patients sitting on a chair, relaxed for at 30 minutes and without recent ingestion of stimulants like caffeine using a manual sphygmomanometer. Measurement was repeated after at least 5 minutes and the average blood pressure measurement was taken. The diagnosis of hypertension was made in accordance with International Society of Hypertension Global Hypertension Practice 2020 Guidelines. High normal blood pressure was considered to be systolic blood pressure (SBP) 130–139 and/or diastolic blood pressure (DBP) 85–89 mm Hg, grade 1 hypertension was considered to be SBP 140–159 and/or DBP 90–99 and grade 2 was considered to be SBP ≥160 and/or DBP ≥100 mm Hg.21 Individuals taking anti-hypertensive medications were also considered to have hypertension.
Body Mass Index (BMI) was considered normal if it was 18.5–24.9 kg/m2, 25–29.9 kg/m2 was considered overweight, 30–34.9 kg/m2 was considered class I obesity, 35–39.9 kg/m2 was considered class II obesity and above 40 was considered class III obesity. BMI <18.5 kg/m2 was considered underweight.22
Waist circumference was measured in centimeters at the midpoint between the lower margin of the lowest palpable rib and top of iliac crest. Hip circumference was measured in centimeters at the widest portion of the buttocks with the tape being held snug around the body. Waist circumference of >94/80 cm (males/females) increased risk of metabolic complications, as did waist-hip ratio of ≥0.9/0.85 (males/females) and was the cutoff used in this study.23
Metabolic syndrome was defined according to National Cholesterol Education Program Adult Treatment Panel-III (NCEP-ATP III) that includes any three of: waist circumference >102 cm (Male), >88 cm (Female); triglyceride level ≥150 mg/dL or specific medications; low High density lipoprotein-cholesterol (HDL-C)<40 mg/dL and <50 mg/dL for men and women, respectively, or specific medications; blood pressure ≥130 mmHg systolic or ≥85 mmHg diastolic or specific medications; or FBG ≥100 mg/dL or previously diagnosed type 2 diabetes or specific medications.24
Cardiovascular risk was estimated using Framingham risk score (FRS). FRS is used to estimate projections of 10-year absolute CVD risk in patients above 20 years of age to identify patients who need intensive treatment and will benefit from it. Risk factors used in the score include age, total cholesterol, HDL cholesterol, blood pressure, and cigarette smoking. It divides patients into high, moderate and low risk based on 10-year risk of >20%, 10–20%, and <10%, respectively.24 FRS is among the most commonly used scoring systems and has shown good agreement with other scoring systems. It has been studied in patients with HIV infection and hence used in this study.6,7
Data Analysis
Data were analyzed using Statistical Package for Social Sciences version 25. Data were summarized using percentages, mean, standard deviation (SD) and presented in tables and text. The independent Student’s t-test was used to compare continuous variables and the Chi square and Fisher’s exact test, when assumptions of chi-square test were not met, were used to compare categorical variables. These tests were used to make subgroup comparisons. Logistic regression was used to examine the association between cardiovascular risk and associated factors. Variables with P-value <0.2 in the univariate analysis were included in the multivariate logistic regression model. All variables with a p-value of <0.05 in the multivariate model were considered statistically significant. Little’s test was done and missing data were missing completely at random. In addition, data with less than 80% response was not included as a covariate in the regression analysis. Pairwise exclusion of missing data was used during analysis to maximize available data. Furthermore, for logistic regression analysis, the minimum required responses to determine differences with 80% power, medium effect size (0.15), alpha significance level of 5% and use of up to 15 predictors calculated using G*Power was 139 responses.25 This response was attained for variables considered in the regression analysis and therefore, pairwise exclusion of missing data did not affect adequacy of responses of the regression analysis.
Ethical Approval
This study was approved by the Institutional Review Board of SPHMMC with protocol number PM23/264. Written informed consent was obtained from all participants. Each participant’s information was collected using anonymous questionnaire and the study was conducted according to the principles expressed in the Declaration of Helsinki.
Results
Demographics and Clinical Characteristics
A total of 333 HIV infected patients on ART participated in the study, out of which, 230 (69.1%) were female. The mean age (SD) of study participants was 45 (10.4) years, with the youngest participant being 19 and the oldest 83 years old. Male participants were relatively older than females with 87.2% of males compared to 61.2% of females being above 40 years (P < 0.001). The mean duration on ART was 10.07 (3.9) years with males being on ART for longer mean years than females (P = 0.012). The mean CD4 count (SD) was 579 cells/mm3 (351) and ranged from 55 to 1477 cells/mm3. Viral load was available in 75.4% of the participants and the mean of the most recent result was 4757 copies/mL (undetectable-272,719) with 74.5% having undetectable viral load and 80.9% having viral load below 50 copies/mL (Table 1).
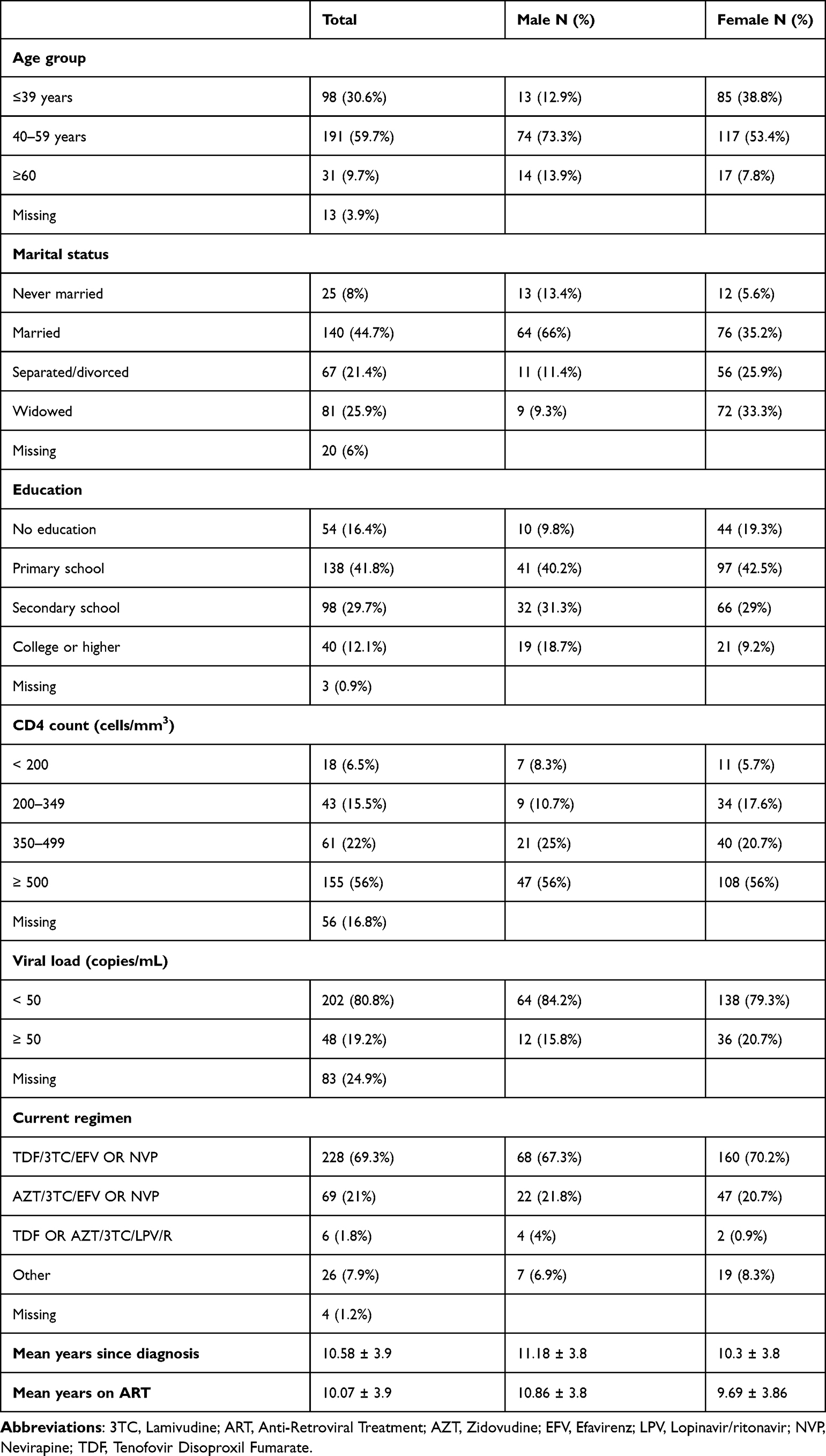 |
Table 1 Sociodemographic and Clinical Characteristics of Patients, SPHMMC, Addis Ababa, 2020 |
Cardiovascular Risk Factors
Among the participants 31 (9.3%) have ever smoked cigarettes, out of which only 6 (1.8%) were still actively smoking. Participants were asked about their intakes of alcohol and 7 participants (2.1%) consumed alcohol in the last month. Only 3 individuals (0.9%) consumed WHO recommendations of five or more servings of fruits and/or vegetables per day on average.
Hypertension was more common in males (34.3%) compared to females (19.4%) (P = 0.004). Participants above the age of 40 years had hypertension records (29.5%) compared to those below 40 years of age (10%) (P = 0.001). Obese participants also had higher records of BP in the hypertensive range (P = 0.012). Patients on Zidovudine, Lamivudine and Nevirapine ART regimen had higher BP recording (P = 0.045) (Table 2).
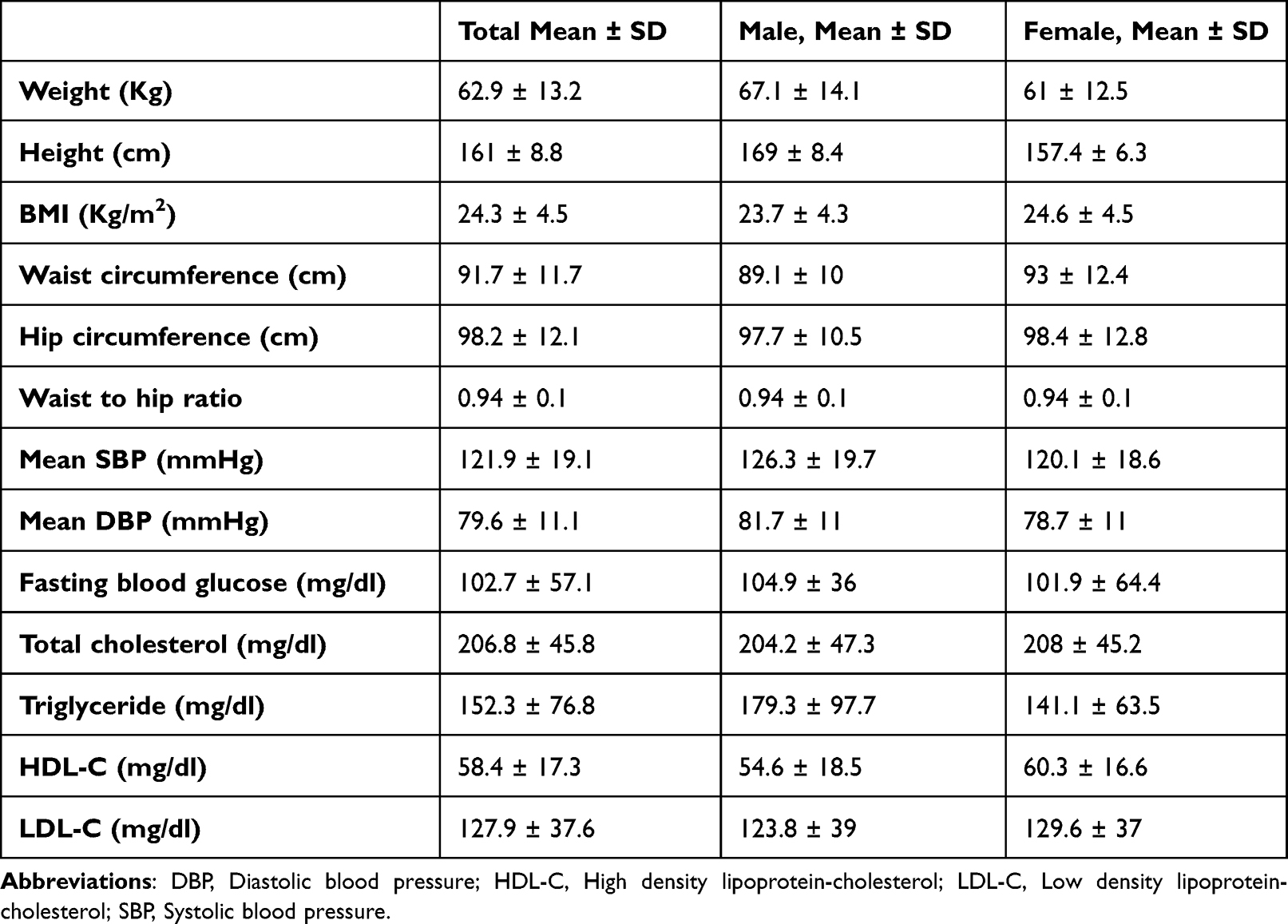 |
Table 2 Anthropometric and Biochemical Characteristics of Patients, SPHMMC, Addis Ababa, 2020 |
Participants were asked if they had ever been told to have raised blood glucose or diabetes and 15 (4.5%) responded yes. Out the 15 patients, 5 patients were on Insulin, 5 were on oral anti-hyperglycemic agent and 8 responded that they were given lifestyle advice regarding their raised blood glucose. More participants, age 40 and older (41.9%) had FBG measurements ≥100 mg/dL compared to younger ones (25%) (P = 0.013). Patients on Efavirenz containing ART regimen had higher FBG compared to individuals on Nevirapine containing ART regimen (P < 0.001) (Table 2).
The mean (SD) BMI was 24.3 kg/m2 (4.5) ranging from 13.3 to 40.5 kg/m2. A total of 11.1% had obesity with 9.9% in class I, 0.9% in class II and 0.3% in class III range. Patients on Tenofovir Disoproxil Fumarate, lamivudine and Nevirapine regimen had higher proportion of obese participants (P < 0.001). Waist and hip circumference was measured in 32.1% of participants, out of which 10 (27.8%) of the males had waist circumference >94 cm and 2 (5.6%) had waist circumference above 102 cm. Female participants had higher waist circumference compared to males (P < 0.001) (Table 2).
Derangement of at least one of the four cholesterols was seen in 69.4% with individuals age 40 and older and obese participants having higher levels of abnormal lipid profile (P < 0.001 and P = 0.024, respectively). Patients on Atazanavir containing ART regimen (67.2%) had higher total cholesterol levels above 200 mg/dL compared to other regimens (48%) (P = 0.029). Out of the 82.6% of participants investigated for metabolic syndrome, older individuals >60 years had higher prevalence (P = 0.034). It was also seen more frequently in obese individuals (P = 0.016). FRS was able to be calculated in 293 of the participants and was in the low risk in 95.9% (Table 3).
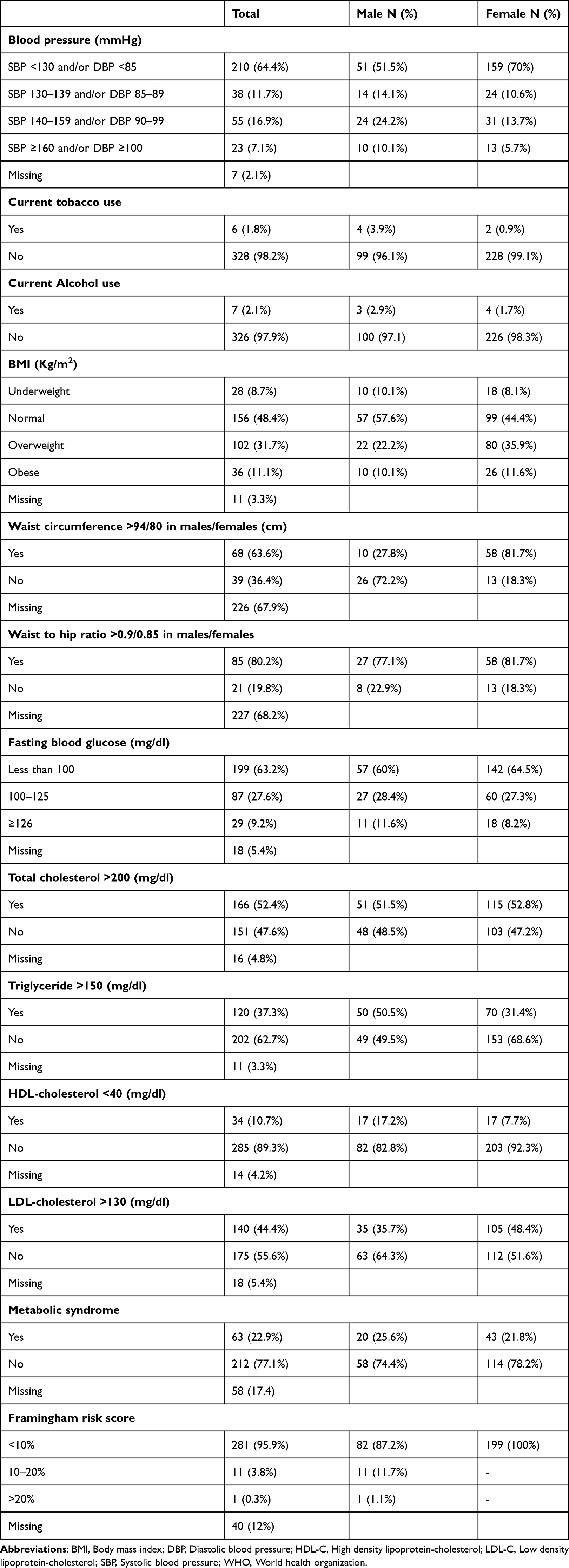 |
Table 3 Cardiovascular Risk Factors of Patients, SPHMMC, Addis Ababa, 2020 |
Cardiovascular risk factors had no difference among patients with different groups of CD4 counts and viral load. No change in the risk factors was seen with increasing duration of diagnosis.
Predictors of CVD Risk Factors
After controlling for other variables, being a male increased the odds of having hypertension by 2.7 times (95% CI, 1.37–5.59). Being in the higher age group (≥40) increased the odds of having hypertension and dyslipidemia by 2.5 times (95% CI, 1.11–5.68) and 3.61 times (95% CI, 1.95–6.72), respectively. Being obese increased the risk of having hypertension and metabolic syndrome by 13.8 (95% CI, 2.29–83.17) times and 12 times (95% CI, 1.28–115.5), respectively, while being overweight increased the risk of having dyslipidemia by 3.67 fold (95% CI, 1.3–10.1). Previous ART regimen being Tenofovir Disoproxil Fumarate, lamivudine and Nevirapine increased the odds of being obese by 7.9 times (95% CI, 2.55–24.32) compared to other regimens. Elevated FBG had no relation with sociodemographic or clinical characteristics. The severity of infection did not contribute significantly to CVD risk factors (Table 4).
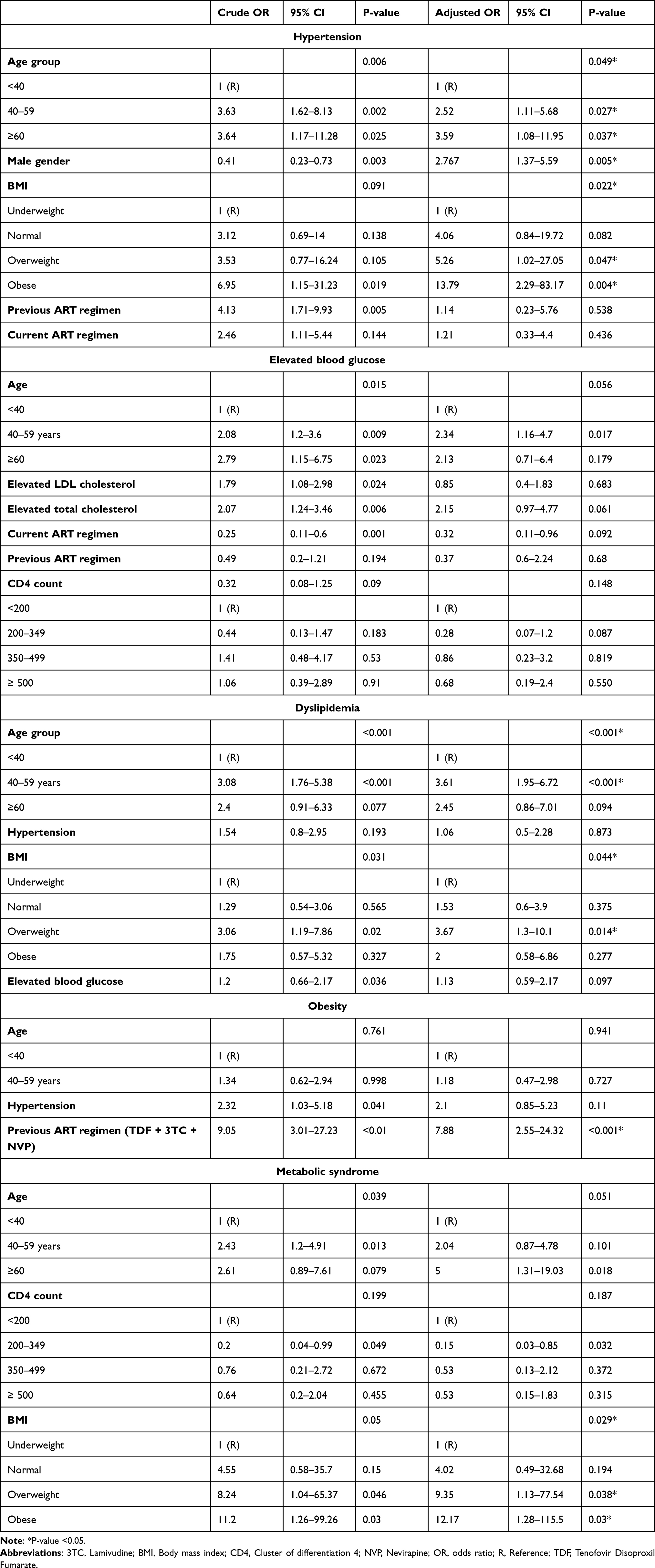 |
Table 4 Multivariate Logistic Regression Analysis of Factors Associated with CVD Risk Factors, SPHMMC, Addis Ababa, 2020 |
Discussion
The prevalence of CVD risks was high in the studied population with 69.4% having dyslipidemia, 36.8% abnormal fasting blood glucose, 23.8% hypertension, 22.8% metabolic syndrome and 11.1% having obesity.
Active smoking among our participants was seen in only 1.8%, with similar rates from studies in different parts of Ethiopia, Nigeria and Malawi.7,15,26–29 The low prevalence of smoking in general Ethiopian population of 3.21%, the lower smoking habit of females in the country and inclusion of more females in this study can justify why only a handful of current smokers participated.30 A study from Malawi reported that very low number of participants consumed the WHO recommended amount of fruits and vegetables similar to our study possibly resulting from resource limitation.29
The prevalence of hypertension was 23.8%. Previous studies done in SSA countries showed prevalence ranging from as low as 8.7% in Kenya to as high as 45.9% in Malawi.31–34 There is also a wide range of findings in previous studies in Ethiopia from 12.7% to 34.3%.5,15,16,26–28,35 Advancing age seems to be a risk for developing hypertension.5,26,28,31–33 Although not consistent in all studies, males and obese individuals tend to have hypertension more frequently.5,26,28,32,33 The difference in prevalence could be explained by the differences in criteria for defining hypertension, socio-economic status, age, life style habits, duration of HIV infection, race, type of ART and study methodology. Awareness regarding hypertension needs to be increased and future studies that evaluate the effectiveness and feasibility of screening and life style modification in HIV infected population should be done.
Our study showed higher magnitude of elevated FBG of >125 mg/dL of 9.2% compared with previous studies, which ranged from 5% in Thailand to 8.8% from Ethiopia.5,13,16,17,27,28,35–37 Studies from Senegal and Tanzania showed higher rates of 14.5% and 18%, respectively.38,39 Impaired fasting glucose (IFG) was seen in 27.6% which was also higher than previous findings of 14% to 19.6% in Ethiopia and Tanzania.16,17,39 Our study included only a one-time measurement of FBG. In addition, Glycated hemoglobin testing was not used due to unavailability of the test in the hospital at the time of data collection. In addition, the variation in the populations studied, differences in age, lifestyle habits and ART could explain the varying findings. The high magnitude of IFG is a potential precursor to diabetes and indicates the risk of having diabetes and CVD in the future. Patients were not aware of their abnormal FBG tests and screening asymptomatic patients is recommended to prevent adverse outcomes.17,35
Obesity in our study was seen in 11.1%. There is a large variation in obesity prevalence in HIV infected population, with as high as 16.6% in Botswana to 17.5% in United States have been seen.40,41 Studies from SSA, France and Brazil show prevalence of 2% to 13.1%.13,15,32,35,36,42–44 The studies were done in different countries on different population groups with different prevalence of obesity. Our study revealed Tenofovir Disoproxil Fumarate, lamivudine and Nevirapine regimen to be a risk for obesity, which needs to be substantiated in future studies. Weight gain is a possible occurrence after initiation of ART and is potentially associated with reduced mortality in underweight individuals. It, however, is offset by the associated increase in diabetes and CVD, and therefore needs follow-up and advice.45,46
Dyslipidemia was seen in 69.4%. Studies from Nigeria, Brazil, Greece have reported prevalence of 29.1% to 46.3% while other studies from Ethiopia have reported higher rates ranging from 48.2% to 90.2%.13,14,35,47–50 There is a difference regarding the cutoffs for abnormal values, differences in gender, age and proportion of patients taking protease inhibitor (PI) containing regimen. Increasing BMI along with advancing age were found to be predictors of dyslipidemia, which is supported by previous studies.13,49,50 Our study revealed more dyslipidemia than some comparative studies which show that risk of future cardiovascular disease with increasing age and longevity is high and needs urgent preventative measures.49
Metabolic syndrome was seen in 22.9%, higher prevalence compared to previous findings ranging from 6.2% to 21.1%.6,9,14,41 Studies from Democratic Republic of Congo and Uganda found it to be a high burden problem with prevalence of 27%, and 58%, respectively.51,52 Higher BMI was the main driver behind MetS in this study, also supported by previous reports.9,41 The differences in the prevalence could have resulted from differences in study design, patient populations, criteria used to define MetS, variation of ART regimen, particularly PIs, and variation in the prevalence of components of MetS.
Almost all of our participants were having FRS of either low or moderate risk. Previous studies also found patients in high-risk group to be low. For instance, studies from Uganda and Malawi showed high or moderate FRS risk of 2.4% and 3.6%, respectively.29,52 CVD risk profiles have good estimation of risk of likelihood of development of stroke and myocardial infarction in HIV patients in Europe and North America.52 However, translating those findings into SSA still remains unproven, as the available data are mainly cross-sectional studies.52 It is yet to be confirmed if risk scores determine the likelihood of developing CVD morbidity or mortality accurately in HIV infection, as HIV specific factors such as immunity status and lipodystrophy are not taken into account.52,53
Integrating HIV care to NCD has been recommended to be a solution to avert the burden of CVDs, including adding NCD care to HIV clinics. This can help with disease prevention and health promotion. It can lead to increased detection of CVDs which need timely care, potentially improving patient outcome. This could potentially be one solution to the growing problem of NCDs in developing countries and its benefits need to be studied further.13
There are certain limitations to our study. The cross-sectional nature of the study makes it difficult to draw definitive conclusions between CVD risks and contributing factors. Only a single record of blood glucose was done and glycated hemoglobin was not assessed, which made the diagnosis of diabetes difficult. In addition, accuracy of FRS in SSA is uncertain and future studies that validate appropriate risk scores in similar settings are needed. Regardless of these limitations, our study provided a comprehensive assessment of CVD risk factors with a large number of participants.
Conclusions
High burden of CVD risk factors was seen. CVD risk factors were independently associated with male gender, increasing age, obesity, and the type of ART patient was taking previously. The high prevalence of these risks should be recognized as it can lead to future development of cardiovascular disease. Patients should have timely follow-up and care. Health-care workers and policy makers should be aware of the high burden of these risk factors. Future well-controlled and prospective studies need to be done to further determine the effect of HIV on cardiovascular disease. The benefits and feasibility of screening and lifestyle modifications should be assessed in HIV infected population in future studies.
Supplementary Materials
Supplementary Material including the data collection questionnaire are available from the corresponding author on reasonable request.
Data Sharing Statement
The datasets used in this study are available from the corresponding author on reasonable request.
Acknowledgments
The authors wish to thank St. Paul’s Hospital Millennium Medical College staff and the patients that participated in this study.
Funding
The funding was provided by St. Paul’s Hospital Millennium Medical College.
Disclosure
All authors declare that they have no conflicts of interest regarding this work.
References
1. Dalal S, Beunza JJ, Volmink J, et al. Non-communicable diseases in sub-Saharan Africa: what we know now. Int J Epidemiol. 2011;40(4):885–901. doi:10.1093/ije/dyr050
2. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. doi:10.1016/S0140-6736(06)68770-9
3. UNAIDS. Report on the global AIDS epidemic 2012: Joint United Nations Programme on HIV/AIDS. Geneva, Switzerland; 2012.
4. Triant VA. Cardiovascular disease and HIV infection. Curr HIV/AIDS Rep. 2013;10(3):199–206. doi:10.1007/s11904-013-0168-6
5. Ataro Z, Ashenafi W, Fayera J, Abdosh T. Magnitude and associated factors of diabetes mellitus and hypertension among adult HIV-positive individuals receiving highly active antiretroviral therapy at Jugal Hospital, Harar, Ethiopia. HIV AIDS. 2018;11(10):181–192.
6. Mashinya F, Alberts M, Van Geertruyden JP, Colebunders R. Assessment of cardiovascular risk factors in people with HIV infection treated with ART in rural South Africa: a cross sectional study. AIDS Res Ther. 2015;12(1):42. doi:10.1186/s12981-015-0083-6
7. Edward AO, Oladayo AA, Omolola AS, Adetiloye AA, Adedayo PA. Prevalence of traditional cardiovascular risk factors and evaluation of cardiovascular risk using three risk equations in Nigerians living with human immunodeficiency virus. N Am J Med Sci. 2013;5(12):680–688. doi:10.4103/1947-2714.123251
8. Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of cardiovascular disease among people living with HIV: a systematic review and meta-analysis. HIV Med. 2012;13(8):453–468. doi:10.1111/j.1468-1293.2012.00996.x
9. Osoti A, Temu TM, Kirui N, et al. Metabolic syndrome among antiretroviral Therapy-Naive versus experienced HIV-infected patients without preexisting cardiometabolic disorders in Western Kenya. AIDS Patient Care STDS. 2018;32(6):215–222. doi:10.1089/apc.2018.0052
10. Paula AA, Falcão MC, Pacheco AG. Metabolic syndrome in HIV-infected individuals: underlying mechanisms and epidemiological aspects. AIDS Res Ther. 2013;10(1):32. doi:10.1186/1742-6405-10-32
11. Bloomfield GS, Hogan JW, Keter A, et al. Hypertension and obesity as cardiovascular risk factors among HIV seropositive patients in Western Kenya. PLoS One. 2011;6(7):e22288. doi:10.1371/journal.pone.0022288
12. Muronya W, Sanga E, Talama G, Kumwenda JJ, van Oosterhout JJ. Cardiovascular risk factors in adult Malawians on long-term antiretroviral therapy. Trans R Soc Trop Med Hyg. 2011;105(11):644–649. doi:10.1016/j.trstmh.2011.07.016
13. Ekrikpo UE, Akpan EE, Ekott JU, et al. Prevalence and correlates of traditional risk factors for cardiovascular disease in a Nigerian ART-naive HIV population: a cross-sectional study. BMJ Open. 2018;8(7):e019664. doi:10.1136/bmjopen-2017-019664
14. Berhane T, Yami A, Alemseged F, et al. Prevalence of lipodystrophy and metabolic syndrome among HIV positive individuals on highly active anti-retroviral treatment in Jimma, South West Ethiopia. Pan Afr Med J. 2012;13:43.
15. Gebrie A. Hypertension among people living with human immunodeficiency virus receiving care at referral hospitals of Northwest Ethiopia: a cross-sectional study. PLoS One. 2020;15(8):e0238114. doi:10.1371/journal.pone.0238114
16. Mohammed AE, Shenkute TY, Gebisa WC. Diabetes mellitus and risk factors in human immunodeficiency virus-infected individuals at Jimma University Specialized Hospital, Southwest Ethiopia. Diabetes Metab Syndr Obes. 2015;15(8):197–206. doi:10.2147/DMSO.S80084
17. Fiseha T, Belete AG. Diabetes mellitus and its associated factors among human immunodeficiency virus-infected patients on anti-retroviral therapy in Northeast Ethiopia. BMC Res Notes. 2019;12(1):372. doi:10.1186/s13104-019-4402-1
18. Federal HIV/AIDS Prevention and Control Office. HIV prevention in Ethiopia: National Road Map (2018–2021); 2018. Available from: https://ethiopia.unfpa.org/en/publications/hiv-prevention-ethiopia-national-road-map-2018-2021.
19. Angaw DA, Ali R, Tadele A, Shumet S. The prevalence of cardiovascular disease in Ethiopia: a systematic review and meta-analysis of institutional and community-based studies. BMC Cardiovasc Disord. 2021;21(1):37. doi:10.1186/s12872-020-01828-z
20. WHO STEPS Instrument (Core and Expanded).The WHO STEPwise approach to noncommunicable disease risk factor surveillance (STEPS). Geneva; Switzerland; World Health Organization; 2016.
21. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
22. World Health Organization. Physical Status: the use and interpretation of anthropometry: report of a World Health Organization (WHO) expert committee. Geneva, Switzerland: World Health Organization; 1995.
23. World Health Organization (WHO) Waist circumference and waist-Hip ratio: report of a WHO expert consultation. Geneva, 8–11 December 2008. Geneva, Switzerland: WHO; 2011.
24. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–3421. doi:10.1161/circ.106.25.3143
25. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
26. Fiseha T, Belete AG, Dereje H, Dires A. Hypertension in HIV-infected patients receiving antiretroviral therapy in Northeast Ethiopia. Int J Hypertens. 2019;23(2019):4103604.
27. Sachithananthan V, Loha E, Gose M. Prevalence of diabetes mellitus, hypertension and lipodystrophy in HAART receiving HIV patients in Southern Ethiopia. Int STD Res Rev. 2013;1(1):1–11. doi:10.9734/ISRR/2013/1897
28. Getahun Z, Azage M, Abuhay T, Abebe F. Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia. J Comorb. 2020;10(2235042):2235042X1989931. doi:10.1177/2235042X19899319
29. Divala OH, Amberbir A, Ismail Z, et al. The burden of hypertension, diabetes mellitus, and cardiovascular risk factors among adult Malawians in HIV care: consequences for integrated services. BMC Public Health. 2016;16(1):1243. doi:10.1186/s12889-016-3916-x
30. Guliani H, Gamtessa S, Çule M. Factors affecting tobacco smoking in Ethiopia: evidence from the demographic and health surveys. BMC Public Health. 2019;19(1):938. doi:10.1186/s12889-019-7200-8
31. Mutemwa M, Peer N, De Villiers A, et al. Prevalence, detection, treatment, and control of hypertension in human immunodeficiency virus (HIV)-infected patients attending HIV clinics in the Western Cape Province, South Africa. Medicine. 2018;97(35):e12121. doi:10.1097/MD.0000000000012121
32. Benzekri NA, Seydi M, Doye N, et al. Increasing prevalence of hypertension among HIV-positive and negative adults in Senegal, West Africa, 1994–2015. PLoS One. 2018;13(12):e0208635. doi:10.1371/journal.pone.0208635
33. Brennan AT, Jamieson L, Crowther NJ, et al. Prevalence, incidence, predictors, treatment, and control of hypertension among HIV-positive adults on antiretroviral treatment in public sector treatment programs in South Africa. PLoS One. 2018;13(10):e0204020. doi:10.1371/journal.pone.0204020
34. Nguyen KA, Peer N, Mills EJ, Kengne AP. Burden, determinants, and pharmacological management of hypertension in HIV-positive patients and populations: a systematic narrative review. AIDS Rev. 2015;17(2):83–95.
35. Abebe SM, Getachew A, Fasika S, Bayisa M, Girma Demisse A, Mesfin N. Diabetes mellitus among HIV-infected individuals in follow-up care at University of Gondar Hospital, Northwest Ethiopia. BMJ Open. 2016;6(8):e011175. doi:10.1136/bmjopen-2016-011175
36. da Cunha GH, Franco KB, Galvão MTG, et al. Diabetes mellitus in people living with HIV/AIDS: prevalence and associated risk factors. AIDS Care. 2020;32(5):600–607. doi:10.1080/09540121.2019.1695727
37. Paengsai N, Jourdain G, Chaiwarith R, et al. Incidence and clinical outcomes of diabetes mellitus in HIV-infected adults in Thailand: a retrospective cohort study. BMC Public Health. 2018;18(1):1079. doi:10.1186/s12889-018-5967-7
38. Diouf A, Cournil A, Ba-Fall K, et al. Diabetes and hypertension among patients receiving antiretroviral treatment since 1998 in Senegal: prevalence and associated factors. ISRN AIDS. 2012;2012:621565. doi:10.5402/2012/621565
39. Maganga E, Smart LR, Kalluvya S, et al. Glucose metabolism disorders, HIV and antiretroviral therapy among Tanzanian Adults. PLoS One. 2015;10(8):e0134410. doi:10.1371/journal.pone.0134410
40. Crum-Cianflone N, Tejidor R, Medina S, Barahona I, Ganesan A. Obesity among patients with HIV: the latest epidemic. AIDS Patient Care STDS. 2008;22(12):925–930. doi:10.1089/apc.2008.0082
41. Tshikuka JG, Magafu MG, Rankgoane-Pono G, et al. Overweight and obesity among recipients of antiretroviral therapy at HIV clinics in Gaborone, Botswana: factors associated with change in body mass index. AIDS Res Treat. 2020;4(2020):8016791.
42. Yitbarek GY, Engidaw MT, Ayele BA, Tiruneh SA, Alamir MT. Magnitude of obesity/overweight and its associated factors among HIV/AIDS patients on antiretroviral therapy in Jimma Zone Hospitals, South West Ethiopia: hospital-based cross-sectional study. Diabetes Metab Syndr Obes. 2020;21(13):1251–1258. doi:10.2147/DMSO.S247221
43. Guehi C, Badjé A, Gabillard D, et al. High prevalence of being overweight and obese HIV-infected persons, before and after 24 months on early ART in the ANRS 12136 Temprano Trial. AIDS Res Ther. 2016;13(1):12. doi:10.1186/s12981-016-0094-y
44. Obry-Roguet V, Brégigeon S, Cano CE, et al. Risk factors associated with overweight and obesity in HIV-infected people: aging, behavioral factors but not cART in a cross-sectional study. Medicine. 2018;97(23):e10956. doi:10.1097/MD.0000000000010956
45. Bailin SS, Gabriel CL, Wanjalla CN, Koethe JR. Obesity and weight gain in persons with HIV. Curr HIV/AIDS Rep. 2020;17(2):138–150. doi:10.1007/s11904-020-00483-5
46. Yuh B, Tate J, Butt AA, et al. Weight change after antiretroviral therapy and mortality. Clin Infect Dis. 2015;60(12):1852–1859. doi:10.1093/cid/civ192
47. Touloumi G, Kalpourtzi N, Papastamopoulos V, et al. Cardiovascular risk factors in HIV infected individuals: comparison with general adult control population in Greece. PLoS One. 2020;15(3):e0230730. doi:10.1371/journal.pone.0230730
48. Mesquita EC, Coelho LE, Amancio RT, et al. Severe infection increases cardiovascular risk among HIV-infected individuals. BMC Infect Dis. 2019;19(1):319. doi:10.1186/s12879-019-3894-6
49. Tadewos A, Addis Z, Ambachew H, Banerjee S. Prevalence of dyslipidemia among HIV-infected patients using first-line highly active antiretroviral therapy in Southern Ethiopia: a cross-sectional comparative group study. AIDS Res Ther. 2012;9(1):31. doi:10.1186/1742-6405-9-31
50. Kemal A, Teshome MS, Ahmed M, et al. Dyslipidemia and associated factors among adult patients on antiretroviral therapy in armed force comprehensive and specialized hospital, Addis Ababa, Ethiopia. HIV AIDS. 2020;2(12):221–231.
51. Katoto PD, Thienemann F, Bulabula ANH, et al. Prevalence and risk factors of metabolic syndrome in HIV-infected adults at three urban clinics in a post-conflict setting, eastern Democratic Republic of the Congo. Trop Med Int Health. 2018;23(7):795–805. doi:10.1111/tmi.13073
52. Muyanja D, Muzoora C, Muyingo A, Muyindike W, Siedner MJ. High prevalence of metabolic syndrome and cardiovascular disease risk among people with HIV on stable ART in Southwestern Uganda. AIDS Patient Care STDS. 2016;30(1):4–10. doi:10.1089/apc.2015.0213
53. Knobel H, Jericó C, Montero M, et al. Global cardiovascular risk in patients with HIV infection: concordance and differences in estimates according to three risk equations (Framingham, SCORE, and PROCAM). AIDS Patient Care STDS. 2007;21(7):452–457. doi:10.1089/apc.2006.0165
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.