Back to Journals » Nature and Science of Sleep » Volume 13
Prevalence of and Risk Factors for Poor Sleep During Different Trimesters of Pregnancy Among Women in China: A Cross-Sectional Study
Authors Zhang H, Li P ![]() , Fan D
, Fan D ![]() , Wu S, Rao J
, Wu S, Rao J ![]() , Lin D
, Lin D ![]() , Huang Q, Liu Z
, Huang Q, Liu Z ![]()
Received 17 February 2021
Accepted for publication 31 May 2021
Published 17 June 2021 Volume 2021:13 Pages 811—820
DOI https://doi.org/10.2147/NSS.S303763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Huishan Zhang,1,2,* Pengsheng Li,1,* Dazhi Fan,1 ShuZhen Wu,2 Jiaming Rao,1 Dongxing Lin,1 Qitao Huang,2 Zhengping Liu1,2
1Foshan Institute of Fetal Medicine, Foshan Women and Children Hospital Affiliated to Southern Medical University, Foshan, Guangdong, People’s Republic of China; 2Department of Obstetrics, Foshan Women and Children Hospital Affiliated to Southern Medical University, Foshan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhengping Liu; Qitao Huang
Department of Obstetrics, Foshan Women and Children Hospital Affiliated to Southern Medical University, No. 11 Renminxi Road, Foshan, Guangdong, 528000, People’s Republic of China
Tel +86 0757 82960793
; +86 15920454515
Email [email protected]; [email protected]
Background: The management of poor sleep during pregnancy is important for maternal and foetal health. The aim of the present study was to investigate the prevalence of poor sleep quality and risk factors for poor sleep during different trimesters of pregnancy for better management of sleep during pregnancy.
Methods: A cross-sectional study was conducted among pregnant women in Foshan Women’s and Children’s Hospital. In total, 2281 pregnant women were analysed, and the Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality. Cluster logistic regression was used to analyse the risk factors for poor sleep among all participants, and logistic regression models were built to identify potential risk factors for poor sleep quality in different trimesters of pregnancy.
Results: Over half of the participants reported poor sleep quality (51.8%). The rate of poor sleep was lowest in the second trimester. Women who were unmarried had > 12 years of education, exercised < 3 days/week, were in the third trimester, had a high level of nausea and vomiting during pregnancy (NVP) and had a history of infertility had a higher risk of poor sleep. Pregnancy-related factors contributed most to poor sleep. In the first trimester, the main risk factors for poor sleep were a history of infertility and a high level of NVP. In the second trimester, only a high level of NVP was a risk factor for poor sleep. In the last trimester, the risk factors for poor sleep were more education years, exercise < 3 days/week and high levels of NVP.
Conclusion: The prevalence and risk factors for poor sleep were different in different trimesters. Clinicians should screen and address poor sleep prior to the first and, especially, the third trimester of pregnancy. Management of poor sleep should be consistent throughout pregnancy and be adjusted in different trimesters.
Keywords: prevalence, risk factors, poor sleep, trimesters of pregnancy
Introduction
Sleep quality during pregnancy is important for maternal and foetal health.1 Poor sleep quality has become common during pregnancy. As a recent meta-analysis demonstrated, 45.7% of pregnant women had experienced poor sleep quality, as measured by the PSQI, and the cut-off point was PSQI≥5.2 A high prevalence of poor sleep was also detected among pregnant women in China (57.3%).3 The estimated rates of poor sleep were 54.3% (95% CI [30.4%, 76.3%]) in the first trimester, 49.3% (95% CI [39.4%, 59.3%]) in the second trimester and 69.6% (95% CI [54.1%, 81.6%]) in the third trimester.2 This demonstrated that the prevalence of poor sleep was high and fluctuated as pregnancy progressed. As the prevalence of poor sleep fluctuates across pregnancy, we hypothesize that the risk factors for poor sleep are different in different trimesters of pregnancy.
Researchers have reported that poor sleep quality increases the risk of systemic inflammation,4 preterm birth,5,6 longer labour,7 unplanned caesarean section,7 gestational diabetes mellitus (GDM),8,9 depression during both the prenatal and postpartum periods and suicide among pregnant women.10–12 Fortunately, good management of poor sleep during pregnancy can improve maternal and neonatal health.13–15
Previous studies showed that age, race,16 parity,17 smoking,18 obesity,19 physical activity,22 low income level, third-trimester pregnancy status and insufficient sleep duration20 were associated with poor sleep during pregnancy. However, to our knowledge, few studies have reported the prevalence and risk factors for poor sleep in different trimesters, especially among Chinese pregnant women. Scholars have suggested that all women be screened and treated for sleep problems throughout pregnancy.21 Therefore, a better understanding of the risk factors for poor sleep quality in every trimester of pregnancy will aid clinicians in providing a better health management strategy and facilitate timely intervention to prevent adverse maternal and foetal outcomes.
Thus, the aims of this study were to determine the prevalence of and risk factors for poor sleep during different trimesters of pregnancy among pregnant women in China.
Methods
Participants
Participant recruitment was based on the Foshan Women’s and Children’s Hospital affiliated with Southern Medical University. This is the largest hospital to provide maternal and child health care in Foshan. There are over 13 thousand deliveries per year. The study was conducted from December 2018 to February 2019 in the obstetrics department. The inclusion criteria were a. age over 18 years; b. pregnancy diagnosed by B ultrasonography; and c. self-professed ability. We asked 3000 pregnant women to participate in our study, and 2831 women agreed to do so. Those less than 18 years old, with serious mental diseases and incomplete questionnaires were excluded. Finally, the total sample size was 2281 pregnant women. Written informed consent was obtained from all participants. A flowchart illustrating the selection of study participants is presented in Supplementary Figure 1. The study was approved by the Human Subjects Committee of the Foshan Women’s and Children’s Hospital affiliated with Southern Medical University (FSFY-MEC-2017-056), and all methods were performed in accordance with the relevant guidelines and regulations.
Measurement of Sleep
Sleep quality was measured with the Chinese version of the Pittsburgh Sleep Quality Index (PSQI), which is widely used. The scale was originally invented by Buysse D.J. and consists of 19 items.22 These items are grouped into seven quality domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication and daytime dysfunction. Every domain has a score from 0 to 3. The total score of PSQI ranges from 0 to 21. A higher score indicates worse sleep quality. PSQI>5 was defined as poor sleep quality, while a score ≤5 was regarded as good sleep, as in most published studies.2,10
Covariables
Covariables were categorized into three groups: 1, demographic factors; 2, lifestyle factors; and 3, pregnancy-related factors. Demographic factors included age, education, marriage and employment. Lifestyle factors included sedentary time and exercise frequency. Pregnancy-related factors included trimester of pregnancy, parity, nausea and vomiting and history of infertility.
The severity of nausea and vomiting during pregnancy (NVP) was measured by means of the Chinese version of the Pregnancy Unique Quantification of Emesis Scale (PUQE).23 The scale consists of 3 items. Every item is given a score from 1 to 5, and the total PUQE score ranges from 3 to 15. A higher score means more severe NVP. According to the recommendation of the PUQE scale, NVP was divided into mild NVP (3~6), moderate NVP (7~12) and severe NVP (13~15). We intended to compare the prevalence of poor sleep among women with severe NVP to those with mild or moderate NVP. However, the rate of severe NVP was too low (1.7%). Therefore, we chose PUQE≥11 (the five percent cut-off point) as the cut-off for high levels of NVP.
Data on other covariables, including age, employment, marriage, education, family income, sedentary time, exercise frequency, trimester of pregnancy, parity and history of infertility, were all collected by self-report. Trimesters of pregnancy were divided into first (≤12 weeks), second (13~27 weeks) and third trimesters (≥28 weeks) according to gestational age. Parity was divided into primipara and multipara. Employment was divided into employed and unemployed. Marriage was divided into married and unmarried (including divorced, widowed and single). Education was divided into ≤12 years and >12 years. Sedentary time was divided into <7 hour ≥7 hours. Exercised frequency was divided into ≥3 and <3 times per week. The question “Have you ever been diagnosed with infertility by a doctor?” was used to collect the infertility data. The answer “yes” was classified as with history of infertility and “no” was classified as without history of infertility.
Statistical Methods
In the present study, all analyses were conducted with IBM SPSS 24.0. All variables in the study except age are presented as frequencies and percentages, as they were all categorical variables. The χ2 test was used to compare the prevalence of poor sleep between different groups and to determine their bivariate correlations. Age is presented as the mean and standard deviation. Cluster logistic regression24 was used to analyse the risk factors for poor sleep among all participants and determine the independent contribution of every cluster to the regression. The calculation method of independent contribution was presented in one of our previous studies.25 The independent effect of each cluster was assessed by the corresponding R2 value, which was similar to the classical R2 in linear regression models. The independent contribution share of each cluster was calculated as the individual R2 change/total R2 change in the final model×100%. Then, we divided all participants into three subgroups according to their trimesters of pregnancy. Logistic regression was used to analyse the risk factors for poor sleep in three different trimesters of pregnancy. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were obtained to evaluate the increased risk of poor sleep quality. All statistical tests of hypotheses were two-sided, and a P-value less than 0.05 was considered statistically significant.
Results
Sleep and the Characteristics of Participants Throughout Pregnancy
A final sample comprising 2281 pregnant women with data on sleep quality was included in this study. Over half of the participants reported poor sleep quality (51.9%, 95% CI=49.8–53.9%) among all participants. The rate in the first trimester was 52.8% (95% CI=48.1–57.5%). The prevalence of poor sleep in the second trimester was the lowest (44.7%, 95% CI= 41.5–47.9%), and the rate in the last trimester was the highest (59.2%, 95% CI= 55.9–62.4%) among the three trimesters. The changing trend in the PSQI mean score throughout pregnancy was similar to the prevalence of poor sleep. We compared the PSQI mean score and prevalence of poor sleep throughout pregnancy between the present study and Sedov’s study, as shown in Figures 1A and 2A. The data for the PSQI mean score in the first trimester in Sedov’s study were unavailable, so we compared the data for only the last two trimesters between the two studies. As shown in Figure 1A, the mean score in the present study was higher in the second trimester and lower in the third trimester than in Sedov’s study. The prevalence of poor sleep quality in all trimesters of pregnancy in this study was lower than that in Sedov’s study. The changing trends in the prevalence of poor sleep in both studies were similar.
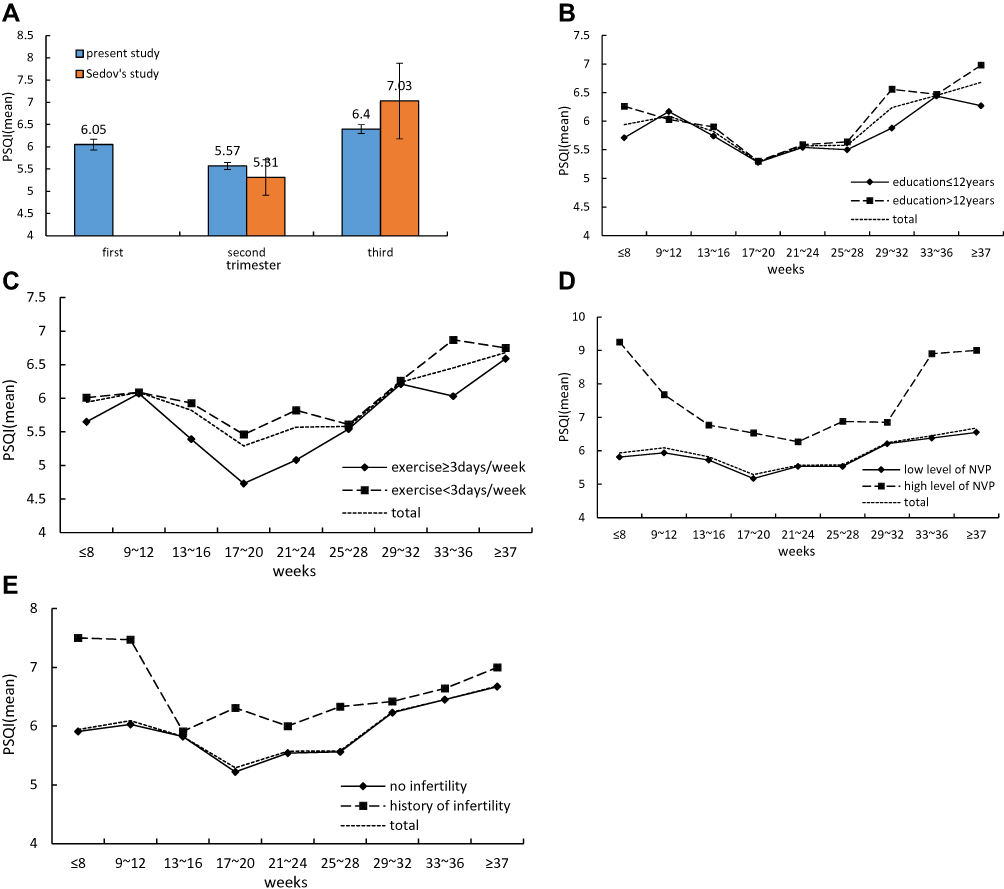 |
Figure 1 (A) Mean PSQI scores across the pregnancy between the present study and Sedov’s study. (B) Mean PSQI scores across the pregnancy among women with different level of education. (C) Mean PSQI scores across the pregnancy among women with different frequency of exercise. (D) Mean PSQI scores across the pregnancy among women with different level of NVP. (E) Mean PSQI scores across the pregnancy among women with history of infertility or not. |
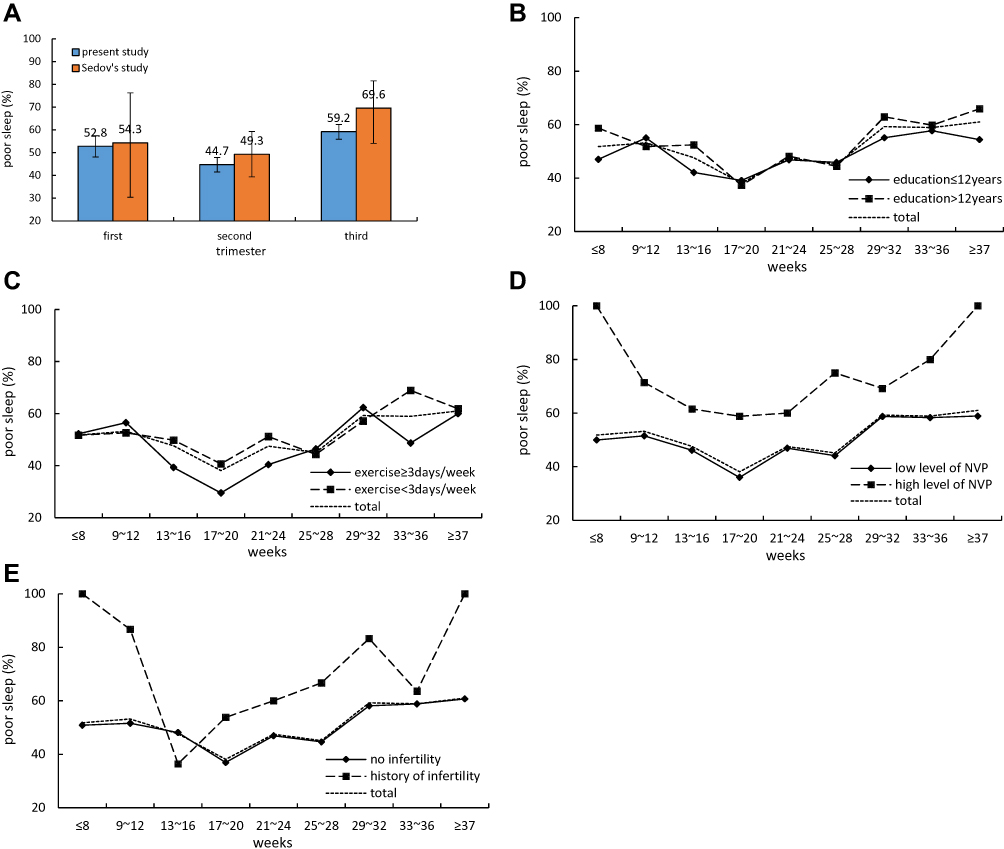 |
Figure 2 (A) Prevalence of poor sleep across the pregnancy between the present study and Sedov’s study. (B) Prevalence of poor sleep across the pregnancy between women with level of education. (C) Prevalence of poor sleep across the pregnancy between women with frequency of exercise. (D) Prevalence of poor sleep across the pregnancy between women with different level of NVP. (E) Prevalence of poor sleep across the pregnancy between women with history of infertility or not. |
The participants had a mean age of 29.70 (SD=4.75) years, and the majority of them had received over 12 years of education, were married, were employed, sat for less than 7 hours per day, exercised less than 3 days per week, were primipara, had a low level of NVP and had no history of infertility. Among all characteristics, the percentage of unmarried participants decreased from the first trimester to the third trimester, and the rates of multipara and women exercising more than 3 times per week increased throughout pregnancy. The rate of women who were sedentary for over 7 hours in the first trimester was higher than that of women in the other two trimesters (Table 1).
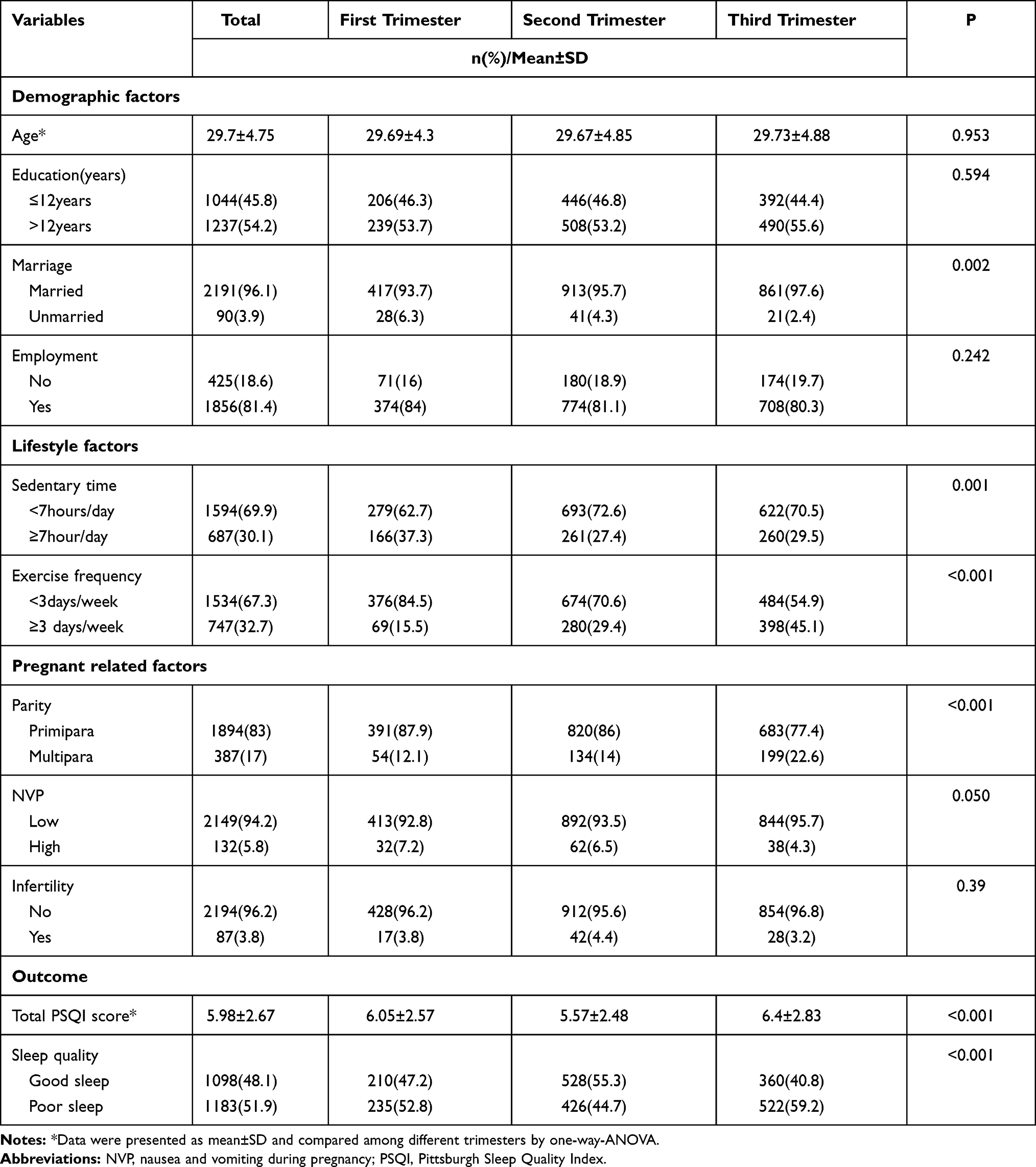 |
Table 1 Characteristics of Participants Evolve Throughout the Pregnancy |
Risk Factors for Poor Sleep Among All Participants
After inclusion of all factors into the cluster logistic regression, only marriage, education, exercise, trimester, NVP and history of infertility were included in the final model, based on statistical significance (Table 2). The results showed that unmarried women were more likely to report poor sleep than married women (OR=1.73, 95% CI=1.11–2.70, P=0.015). Women who had over 12 years of education had a higher risk of poor sleep during pregnancy than those who had fewer years of education (OR=1.19, 95% CI=1.01–1.41, P=0.045). Those who had a regular exercise routine (exercise≥3 days/week) had a lower possibility of experiencing poor sleep than those without (OR=0.77, 95% CI=0.64–0.93, P=0.006). Compared with women in the first trimester of pregnancy, those in the second trimester had a lower risk of poor sleep (OR=0.75, 95% CI=0.60–0.95, P=0.015), and those in the third trimester had a higher risk of poor sleep (OR=1.47, 95% CI=1.16–1.87, P=0.002). In addition, women with a high level of NVP and a history of infertility had an odds of 2.45 (95% CI=1.66–3.61, P<0.001) and 2.02 (95% CI=1.30–3.28, P=0.002), respectively, for poor sleep compared with those without. The independent contributions from clusters 1, 2 and 3 were 10%, 8% and 82%, respectively. Cluster 3 (pregnant-related factors) had the largest independent contribution, and cluster 2 (lifestyle factors) had the smallest.
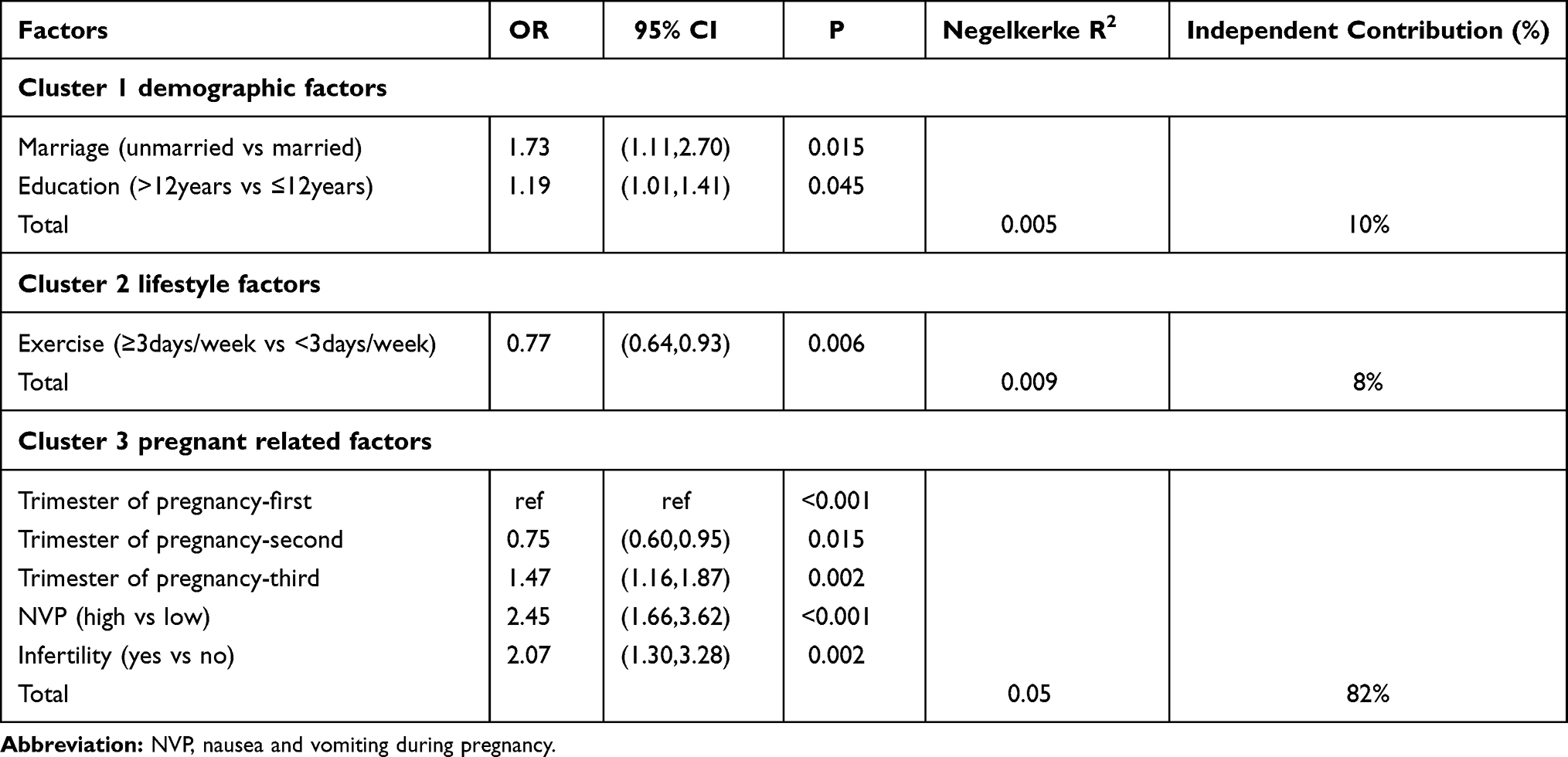 |
Table 2 Cluster Logistic Regression of Poor Sleep |
Risk Factors for Poor Sleep in Different Trimesters of Pregnancy
As sleep quality fluctuates with increasing gestational age, we analysed the interaction between each trimester and other significant factors. However, no factors showed significant interaction effects with trimester. Then, we divided the subjects into three subgroups according to the trimester of pregnancy to analyse the risk factors in different trimesters of pregnancy. The results are presented in Table 3, and as shown, the risk factors for poor sleep were different among different trimesters. In the first trimester, women with a high level of NVP (OR=2.94, 95% CI=1.29–6.73) and a history of infertility (OR=7.30, 95% CI=1.64–32.39) had a higher risk of poor sleep. In the second trimester, women with a high level of NVP had a higher risk of poor sleep (OR=2.21, 95% CI=1.30–3.77). In the last trimester, women with education >12 years (OR=1.39, 95% CI=1.05–1.83) and high levels of NVP (OR=2.85, 95% CI=1.29–6.32) were more likely to report poor sleep, and those with regular exercise (exercise ≥3 days/week) had a lower risk of poor sleep (OR=0.72, 95% CI=0.55–0.95).
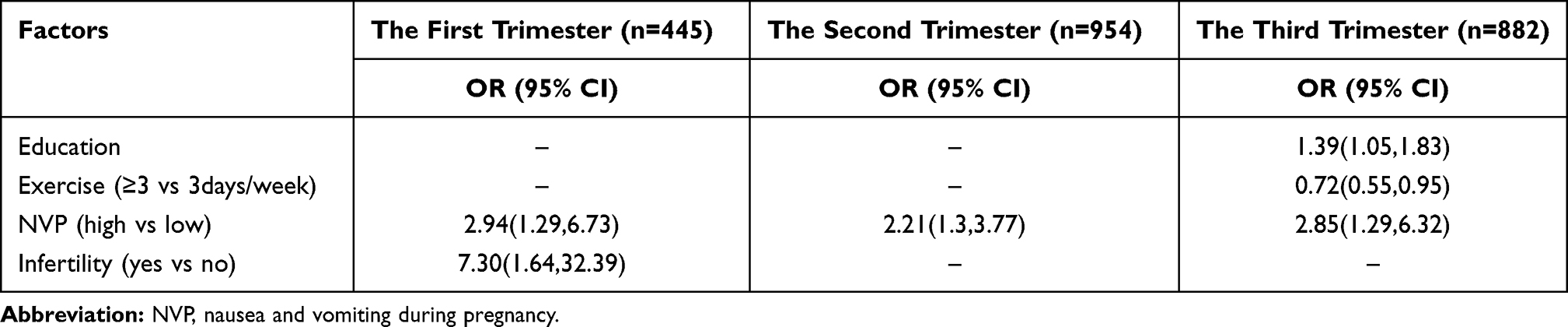 |
Table 3 Risk Factors of Poor Sleep in Different Trimesters |
To better understand the distribution of sleep quality across pregnancy among the above four factors, we constructed Figures 1B–E and 2B–E. Regarding education, the results showed that women with education >12 years had obviously higher scores only during ≤8 weeks, 29~32 weeks and ≥37 weeks. The data at other time points were similar between the two groups (Figures 1B and 2B). For exercise, women who exercised ≥3 days/week had lower PSQI mean scores across pregnancy, but regarding the prevalence of poor sleep, the lines of the two groups crossed each other (Figures 1C and 2C). Regarding NVP, women with a high level of NVP had a higher PSQI mean score and prevalence of poor sleep across pregnancy, especially at the start and end of pregnancy (Figures 1D and 2D). Finally, regarding a history of infertility, women with previous infertility scored higher on the PSQI across pregnancy, and their prevalence of poor sleep was almost higher than that of women without infertility, except during the third trimester (Figures 1E and 2E). Marriage was originally included in the regression model of all participants but did not remain in the three-subgroup regression model, possibly due to the sample size. We were still able to obtain statistically significant results with the small sample, but a larger effect should have been observed. Thus, although small sample sizes do not invalidate findings, they make it harder to detect associations or differences.26
Discussion
In the present study, we studied the prevalence and risk factors for poor sleep among all participants and in different trimesters of pregnancy among pregnant women in China. The prevalence of poor sleep was 51.9% among all participants. Women who married, received >12 years of education, exercise <3 days/week, in the third trimester, had a high level of NVP and a history of infertility had a higher risk of poor sleep during pregnancy. Pregnancy-related factors contributed most to poor sleep quality. The main risk factors for poor sleep were different among the three trimesters of pregnancy. In the first trimester, the main risk factors for poor sleep were a history of infertility and a high level of NVP. In the second trimester, only a high level of NVP was a risk factor for poor sleep. In the last trimester, the risk factors for poor sleep were more education years, exercise <3 days/week and high levels of NVP.
The prevalence of poor sleep was 51.9%, much higher than that of the general population (26.5%) in China18 and slightly higher than that in Sedov’s study (45.7%).2 The prevalences of poor sleep in Sedov’s and the present study presented decreasing trends from the first trimester to the second trimester and increasing trends from the second trimester to the third trimester. The PSQI score and prevalence of poor sleep were highest in the third trimester. Taken together, these data implied that it was important for clinicians to screen for and address sleep problems prior to the first and, especially, the third trimester of pregnancy.
The risk factors for poor sleep among all participants were unmarried status, education over 12 years, exercise less than 3 days per week, third-trimester pregnancy status, a high level of NVP and a history of infertility. Unmarried women were shown to have a higher risk of poor sleep in the present study. However, it was hard to find previous studies to support this result, as there is a lack of studies on this relationship. In fact, in most societies globally, it is stressful for an unmarried woman to have a baby, which may lead to more mental stress and a higher risk of poor sleep among unmarried pregnant women.
The relationship between sleep and education was interesting in that higher educational level was a risk factor for poor sleep. Some studies reported similar results,3,27 but others found that women with lower education had a higher likelihood of poor sleep.21 Some studies have demonstrated that there is no relationship between them.28 In general, women with a higher educational level had more knowledge and skills to maintain health and had better sleep quality. However, women with a higher educational level might experience more pressure and worse sleep because they tend to undertake a more important role in the workplace. This situation may be worse for women in the last trimester of pregnancy, as shown in Table 3 and Figures 1B and 2B. This may be because many women a lower educational level quit jobs to be housewives, but most of the women with a higher educational level continue working in the last trimester of pregnancy. Further studies focusing on educational level and sleep should include other covariables, such as work status, mental health and health knowledge.
Regarding lifestyle, the relationship between exercise and sleep quality implied that exercise was important to maintain good sleep quality, especially in the last trimester. A recent systematic review reported that exercise could enhance the quality of sleep,29 and a clinical randomized controlled trial demonstrated that exercise training improves sleep quality.30 Across pregnancy, the sleep quality among women with exercise ≥3 days/week was better than that of women with less exercise, especially in the third trimester. Thus, clinicians should advise pregnant women to exercise more frequently, especially in the last trimester.
Among the three clusters, pregnancy-related factors contributed most to poor sleep. Three pregnancy-related factors, namely, trimester of pregnancy, NVP and history of infertility, were found to be related to sleep quality during pregnancy. Women with a high level of NVP had a higher risk of poor sleep in both the whole regression model and three-subgroup regression models. NVP is a common and uncomfortable aspect of pregnancy. This discomfort during pregnancy makes it difficult for women to sleep well or at all. EnginYıldırım’s31 research also found that women with HG had higher PSQI scores. The ORs of poor sleep among women with high levels of NVP in the first and third trimesters were higher than those of women in the second trimester. Figures 1D and 2D also supports these results. Additionally, it was easy to understand that the odds ratio was highest in the first trimester, as most NVPs were present in the first trimester. Curiously, the odds ratio was also high in the third trimester. Women with high levels of NVP should be screened for sleep quality, especially in the first and third trimesters.
Women with a history of infertility tended to report poor sleep more often in the present study. Similar results were present only in the first-trimester subgroup regression. This may be because women with a history of infertility may be more anxious about pregnancy and more likely to have poor sleep quality, especially in the first trimester, when pregnancy is not very stable However, no previous study has focused on a history of infertility and poor sleep. The sample size may need to be enlarged in future studies to verify this result. Obstetricians should pay more attention to sleep quality among pregnant women with a history of infertility in the first trimester.
In conclusion, the prevalence and risk factors for poor sleep were different among different trimesters. Clinicians should screen and address poor sleep prior to the first and third trimesters of pregnancy, especially the third trimester. The management of poor sleep should be consistent throughout pregnancy and be adjusted in different trimesters.
Strengths and Limitations
Although many pregnant women complain of poor sleep quality during pregnancy, few studies have reported the different risk factors for poor sleep quality during different trimesters of pregnancy. This study presents the prevalence of and risk factors for poor sleep quality across pregnancy. In addition, an interesting factor, history of infertility, was found to be related to poor sleep quality, especially in the first trimester.
However, this study had several limitations. First, data on some variables, such as obstructive sleep apnoea, restless legs syndrome, workforce status and body mass index, which were reported to be related to sleep quality, were not collected in this study. In addition, self-report questionnaires may lead to some report bias. Last, as a cross-sectional study, we cannot determine the causality between factors and outcome variables.
Data Sharing Statement
Available upon request to the first author.
Ethical Approval
The study was approved by the Human Subjects Committee of the Foshan Women’s and Children’s Hospital affiliated with Southern Medical University (FSFY-MEC-2017-056), and all methods were performed in accordance with the relevant guidelines and regulations. The study was conducted in accordance with the Declaration of Helsinki.
Consent to Participants
Informed consent was obtained from all individual participants included in the study.
Acknowledge
We are grateful to all of the women who participated in this study and all staff who helped collect the data.
Funding
There is no funding for the study.
Disclosure
The authors declare that they have no conflicts of interest. No funding influenced the design, data collection, analysis or interpretation of the study.
References
1. Lu Q, Zhang X, Wang Y, et al. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: a systematic review and meta-analysis. Sleep Med Rev. 2021;58:101436. doi:10.1016/j.smrv.2021.101436
2. Sedov ID, Cameron EE, Madigan S, Tomfohr-Madsen LM. Sleep quality during pregnancy: a meta-analysis. Sleep Med Rev. 2018;38:168–176. doi:10.1016/j.smrv.2017.06.005
3. Gao M, Hu J, Yang L, et al. Association of sleep quality during pregnancy with stress and depression: a prospective birth cohort study in China. BMC Pregnancy Childbirth. 2019;19(1):444. doi:10.1186/s12884-019-2583-1
4. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev. 2019;99(3):1325–1380. doi:10.1152/physrev.00010.2018
5. Wang L, Jin F. Association between maternal sleep duration and quality, and the risk of preterm birth: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth. 2020;20(1):125. doi:10.1186/s12884-020-2814-5
6. Blair LM, Porter K, Leblebicioglu B, Christian LM. Poor sleep quality and associated inflammation predict preterm birth: heightened risk among African Americans. Sleep. 2015;38(8):1259–1267. doi:10.5665/sleep.4904
7. Zafarghandi N, Hadavand S, Davati A, Mohseni SM, Kimiaiimoghadam F, Torkestani F. The effects of sleep quality and duration in late pregnancy on labor and fetal outcome. J Maternal Fetal Neonat Med. 2012;25(5):535–537. doi:10.3109/14767058.2011.600370
8. Cai S, Tan S, Gluckman PD, et al. Nocturnal sleep quality and sleep duration in pregnancy and risk of gestational diabetes mellitus. Sleep. 2017;40(2). doi:10.1093/sleep/zsw058
9. Wang H, Leng J, Li W, et al. Sleep duration and quality, and risk of gestational diabetes mellitus in pregnant Chinese women. Diabetic Med. 2017;34(1):44–50. doi:10.1111/dme.13155
10. Gelaye B, Addae G, Neway B, et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J Affect Disorders. 2017;209:195–200. doi:10.1016/j.jad.2016.11.020
11. Tae H, Jeong BR, Chae J-H. Sleep problems as a risk factor for suicide: are certain specific sleep domains associated with increased suicide risk? J Affect Disorders. 2019;252:182–189. doi:10.1016/j.jad.2019.04.053
12. Okun ML, Mancuso RA, Hobel CJ, Schetter CD, Coussons-Read M. Poor sleep quality increases symptoms of depression and anxiety in postpartum women. J Behav Med. 2018;41(5):703–710. doi:10.1007/s10865-018-9950-7
13. Sönmez A, Aksoy Derya Y. Effects of sleep hygiene training given to pregnant women with restless leg syndrome on their sleep quality. Sleep & Breathing = Schlaf & Atmung. 2018;22(2):527–535. doi:10.1007/s11325-018-1619-5
14. Kempler L, Sharpe L, Bartlett D. Sleep education during pregnancy for new mothers. BMC Pregnancy Child. 2012;12:155. doi:10.1186/1471-2393-12-155
15. Bacaro V, Benz F, Pappaccogli A, et al. Interventions for sleep problems during pregnancy: a systematic review. Sleep Med Rev. 2020;50:101234. doi:10.1016/j.smrv.2019.101234
16. Reid KJ, Facco FL, Grobman WA, et al. Sleep during pregnancy: the nuMoM2b pregnancy and sleep duration and continuity study. Sleep. 2017;40(5). doi:10.1093/sleep/zsx045.
17. Naghi I, Keypour F, Ahari SB, Tavalai SA, Khak M. Sleep disturbance in late pregnancy and type and duration of labour. J Obstet Gynaecol. 2011;31(6):489–491. doi:10.3109/01443615.2011.579196
18. Liao Y, Xie L, Chen X, et al. Sleep quality in cigarette smokers and nonsmokers: findings from the general population in central China. BMC Public Health. 2019;19(1):808. doi:10.1186/s12889-019-6929-4
19. Kalmbach DA, Cheng P, Sangha R, et al. Insomnia, short sleep, and snoring in mid-to-late pregnancy: disparities related to poverty, race, and obesity. Nat Sci Sleep. 2019;11:301–315. doi:10.2147/NSS.S226291
20. Xu X, Liu D, Zhang Z, Sharma M, Zhao Y. sleep duration and quality in pregnant women: a cross-sectional survey in China. Int J Environ Res Public Health. 2017;14(7):817. doi:10.3390/ijerph14070817
21. Mindell JA, Cook RA, Nikolovski J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015;16(4):483–488. doi:10.1016/j.sleep.2014.12.006
22. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatr Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Chenglin L, Guozhen X, Shaohua Z, He H. Gynecology do: the reliability and validity of the chinese version of pregnancyunique quantification of emesis and nausea. China Contin Med Educ. 2019.
24. Zhang H-S, Li Y, Mo H-Y, et al. A community-based cross-sectional study of sleep quality in middle-aged and older adults. Qual Life Res. 2017;26(4):923–933. doi:10.1007/s11136-016-1408-1
25. Zhang H-S, Mai Y-B, Li W-D, et al. Sleep quality and health service utilization in Chinese general population: a cross-sectional study in Dongguan, China. Sleep Med. 2016;27–28.
26. Samuels P. Re: does Sample Size really affect on result of research?; 2018. Available from: https://www.researchgate.net/post/Does-Sample-Size-really-affect-on-result-of-research/5a8be57a217e20022024a292/citation/download.
27. Shobeiri F, Ebrahimi R, Khodakarami B, Roshanei GJ. Sleep quality and its predictive factors in nulliparous pregnant women. Biol Sci C. 2016;7(6):287–293.
28. Conlon RPK, Wang B, Germeroth LJ, Cheng Y, Buysse DJ, Levine MD. Demographic, pregnancy-related, and health-related factors in association with changes in sleep among pregnant women with overweight or obesity. Int J Behav Med. 2020.
29. Yang S-Y, Lan S-J, Yen -Y-Y, Hsieh Y-P, Kung P-T, Lan S-H. Effects of exercise on sleep quality in pregnant women: a systematic review and meta-analysis of randomized controlled trials. Asian Nurs Res. 2020;14(1):1–10. doi:10.1016/j.anr.2020.01.003
30. Jurado-Fasoli L, De-la-o A, Molina-Hidalgo C, Migueles JH, Castillo MJ, Amaro-Gahete FJ. Exercise training improves sleep quality: a randomized controlled trial. Eur J Clin Invest. 2020;50(3):e13202. doi:10.1111/eci.13202
31. Yıldırım E, Demir E. The relationship of hyperemesis gravidarum with sleep disorders, anxiety and depression. J Obstet Gynaecol. 2019;39(6):793–798. doi:10.1080/01443615.2019.1572725
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.