Back to Journals » Infection and Drug Resistance » Volume 15
Prevalence and Trends in Antimicrobial Susceptibility Patterns of Multi-Drug-Resistance Non-Typhoidal Salmonella in Central Thailand, 2012–2019
Authors Hengkrawit K, Tangjade C
Received 22 December 2021
Accepted for publication 5 March 2022
Published 29 March 2022 Volume 2022:15 Pages 1305—1315
DOI https://doi.org/10.2147/IDR.S355213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kitchawan Hengkrawit,1 Chidchanok Tangjade2
1Pediatric Infectious Disease Unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, Nonthaburi, Thailand; 2Pediatrics Gastroenterology and Hepatology Unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, Nonthaburi, Thailand
Correspondence: Kitchawan Hengkrawit, Pediatric Infectious Disease unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, P.O.Box: 222 Moo 1, Tiwanon Road, Pak Kret, Nonthaburi, 11120, Thailand, Tel +66 2 502 2345, Fax +662 502-2305, Email [email protected]
Purpose: Multi-drug resistance of non-typhoidal Salmonella (MDR-NTS) is an increasing threat worldwide. In Thailand, data for the past decade is limited. This research is to determine the prevalence and trends of nonsusceptibility patterns of the bacteria, especially to ciprofloxacin and ceftriaxone.
Methods: This retrospective study was extracted data of patients who had non-typhoidal Salmonella (NTS) infection, from 10 hospitals between June 2011 and June 2020. Demographic data, culture reports, and antimicrobial susceptibility were included in the analysis.
Results: A total of 433 patients were identified. The most common age group was less than 15 years old (53.6%), with a median age of 12 years (IQR 57– 4). Of these people, 61.1% had gastroenteritis and 36.7% had bacteremia. The most prevalent serogroups was C (28.6%). MDR-NTS rate was 52.8% (95% CI 39– 44). The resistant rates were 43%, 32.8%, 22.8%, 6.7%, 4%, 0.45%, 0.45% for sulfamethoxazole/trimethoprim, amoxicillin-clavulanic acid, cefotaxime, ampicillin/sulbactam, piperacillin/tazobactam, imipenem and meropenem retrospectively. Resistant rates have been increasing, especially for ciprofloxacin (30%), which rose from 16.6% in 2011– 2015 to 39.5% in 2016– 2020 (prevalence rate ratio (PRR) 2.4,95% CI 1.51– 3.72) and for ceftriaxone 25.4% which rose from 16.1% to 32% (PRR 2 95% CI 1.24– 3.16). Ampicillin, norfloxacin, tetracycline, amikacin, gentamicin, and ceftazidime remained static at 62.3%, 49.5%, 33.2%, 15.2%, 8.8%, 2.8%, respectively.
Conclusion: The prevalence of MDR-NTS has been increasing over the past decade, particularly those strains which demonstrate resistance to ciprofloxacin and ceftriaxone. Finding successful treatment requires a comprehensive selection of proper antimicrobials as well as close monitoring, especially in cases with severe infection.
Keywords: multi-drug resistance, non-typhoidal Salmonella, drug-resistance pattern, ceftriaxone resistance, ciprofloxacin resistance, prevalence
Introduction
Non-typhoidal Salmonella (NTS) is a major cause of Infectious diarrhea worldwide, especially in Southeast Asia. There has been an increase in the rate of drug resistance of non-typhoidal Salmonella (DR-NTS).1–4 DR-NTS infection is associated with invasive diseases, hospitalization, and increased mortality.5 The main mechanisms of resistance are extended-spectrum ß-lactamases (ESBL), AmpC ß-lactamases (AmpC) which are resistant to cephalosporinases especially ceftriaxone or mutations of DNA gyrase enzyme and topoisomerase IV which are fluoroquinolone resistant. Mechanisms also include either horizontal gene transfer or point mutation between organisms. Ceftriaxone and ciprofloxacin resistance have been increasingly reported worldwide6–10 which is a concern for doctors. This resistance increases the risk of treatment failure. In 2020 the National Antimicrobial Resistance Surveillance Center of Thailand11 (NARST) reported NTS isolated from blood (2020) was resistant to ciprofloxacin (4.6%) and ceftriaxone (7.2%).6 However, the MDR-NTS rate was not reported by NARST. Moreover, drug resistance rates in some areas of Thailand differ greatly from the average. A previous study in rural Thailand10 (2006–2014) reported MDR-NTS 19.2% resistance to ciprofloxacin and 58.1% and 12.2% resistant to third generation cephalosporins. Data from a similar periodic study on human infections in Asian countries found MDR of 25.3% (2012–2019) in Taiwan,12 41% (2019) in Hong Kong13 and 53.8% (2014–2019) in Vietnam14 which had all potential to increase. Therefore, a study was conducted to determine the prevalence of current MDR-NTS infection from patterns of antimicrobial resistance, particularly resistance to ceftriaxone and ciprofloxacin in Nonthaburi province. Nonthaburi is in the central region of Thailand. It is very densely populated (2nd place after Bangkok).15 It is also a city of government Centers and more than a million visitors (domestic and foreign proportions; 500:1)15 per year.
Materials and Methods
Methods
The research was conducted retrospectively, by collecting patient information from ten hospitals: six district, three private, and one tertiary hospital with permission from hospital directors. The data included all patients who were diagnosed with Salmonella infections based on ICD-10 (A02.0-A02.9 (WHO. 2014–2016 ICD-10-CM Diagnosis Code A02.0–02.9 and ICD-10-CM Diagnosis Code A02.9)16 from June 2011 to June 2020. Patients with no serogroup and/or antimicrobial sensitivity testing results were excluded. Then medical records of the patients were reviewed for their demographical data including age, gender, culture (blood, stool and/or other body fluid), and antimicrobial susceptibility testing reports. Patients whose cultures were negative were excluded from the study.
Microbial Definition
All hospitals in the study reported Salmonella culture by using O antigen to classify them as serogroups A, B, C, D, and E, based on the Kauffman-White classification.17 Antimicrobial susceptibility testing was performed using the agar disk diffusion method) each lab may be different about of type and number of antimicrobials; however, the antimicrobial susceptibility of laboratories in Thailand were interpreted according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI),18 which is under control standards set by the Department of Medical Sciences in the Ministry of Public Health.19 CLSI defines DR-NTS as NTS resistant to at least one class of antimicrobials. MDR-NTS was defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories.20
Statistical Methods
Descriptive statistics were used to analyze demographic data and prevalence. The differentiations between groups were analysis by Pearson’s chi-square and 95% confidence interval. SPSS version 21 was used as the analysis tool.
Results
The Prevalence and Characteristics
Four hundred eighty-one patients were diagnosed with NTS infection within the period of 2011 to 2020. After exclusions based on criteria, 433 patients were remained. The patients had a median age of 12, IQR (4–57), age group ≤15 years 53.6% (n= 232/433), 16–60 years 24.4% (n=106/433),> 60 years 21.7% (n= 95/433). Male 45% (n= 195/433) and female 55% (n= 238/433). The patient data came from a tertiary hospital 47.8% (n=207/433), district hospitals 25.3% (n= 135/433) and private hospitals 17% (n=91/433). Diagnosis was categorized as noninvasive 61.6% (n=267/433; 264 gastroenteritis, 1 chronic otitis media, 1 chronic ulcer, 1 abscess), invasive 38.4% (n=166/433; 159 bacteremia,1 meningitis, 1 meningitis with brain abscess, 2 osteomyelitis, 2 arthritis,1 urinary tract infection with bacteremia). The patients infected with non-drug resistance non-typhoidal Salmonella (NDR-NTS) amounted to 9.9% (n=43/433) (95% CI 3.98–9.77). Ninety percent had NTS which was resistant to at least one essential antimicrobial. 24.2% (n=105/433) (95% CI 6.15–11.51) were resistance to one class of antimicrobial (1-DR-NTS). Resistance to two classes of antimicrobial (2-DR-NTS) was 12.9% (n=56/433) (95% CI 10.21–23.67), MDR-NTS 52.8% (n=229/433) (95% CI 10.26–30.76).There were 33% (n=143/433) of the patients with underlying disease; the most common were metabolic disease 10.6% (n=46/433) (21 diabetes, 8 diabetes with hypertension, 8 diabetes with hyperlipidemia, 9 diabetes with other), hyperlipidemia 4.4% (n=19/433) and hematologic 8.3% (n=36/433)(12 thalassemia with regular blood transfusion, 8 thalassemia with non-regular blood transfusion, 8 Iron deficiency anemia, 2 G6PD, 6 other) gastrointestinal 2.8% (n=12/433), immunological 2.3% (n=10/433), (6 HIV,1 SLE, 3 other), neurological 2.7% (n=12/433) other 2.5% (n=11/433) (Table 1).
 |
Table 1 The Prevalence and Characteristics of Patients Infected with NTS Which Were Classified into Four Groups Based on the Number of Antimicrobials Resistances |
Drug-Resistant Patterns and Trends
Overall, the NTS resistance to ampicillin was 62.3% (n=270/433), norfloxacin was 49.5% (n=121/433), sulfamethoxazole/ trimethoprim was 43% (n=186/433), tetracycline was 33.2% (n=144/433), amoxicillin-clavulanic acid was 32.8% (n=142/433), ciprofloxacin was 30% (n=130/433), ceftriaxone was 25.4% (n=110/433), cefotaxime was 22.8% (n=99/433), amikacin was 15 0.2% (n=66/433), gentamicin was 8.8% (n=38/433), ampicillin/sulbactam was 6.7% (n=29/433), ceftazidime was 2.8% (n=12/433), piperacillin/tazobactam was 1.8% (n=8/433), imipenem was 0.46% (n=2/433), meropenem was 0.46% (n=2/433). Ciprofloxacin, ceftriaxone, cefotaxime, sulfamethoxazole/trimethoprim, amoxicillin-clavulanic acid, piperacillin/tazobactam, ampicillin/sulbactam imipenem and meropenem, all showed increase resistance (Figure 1A), while resistance to the other antimicrobials fluctuated or slightly decrease. (Figure 1B) Subgroup analysis of invasive NTS patients found that the trend of drug resistance was not different from that of overall NTS patients (Figure 2).
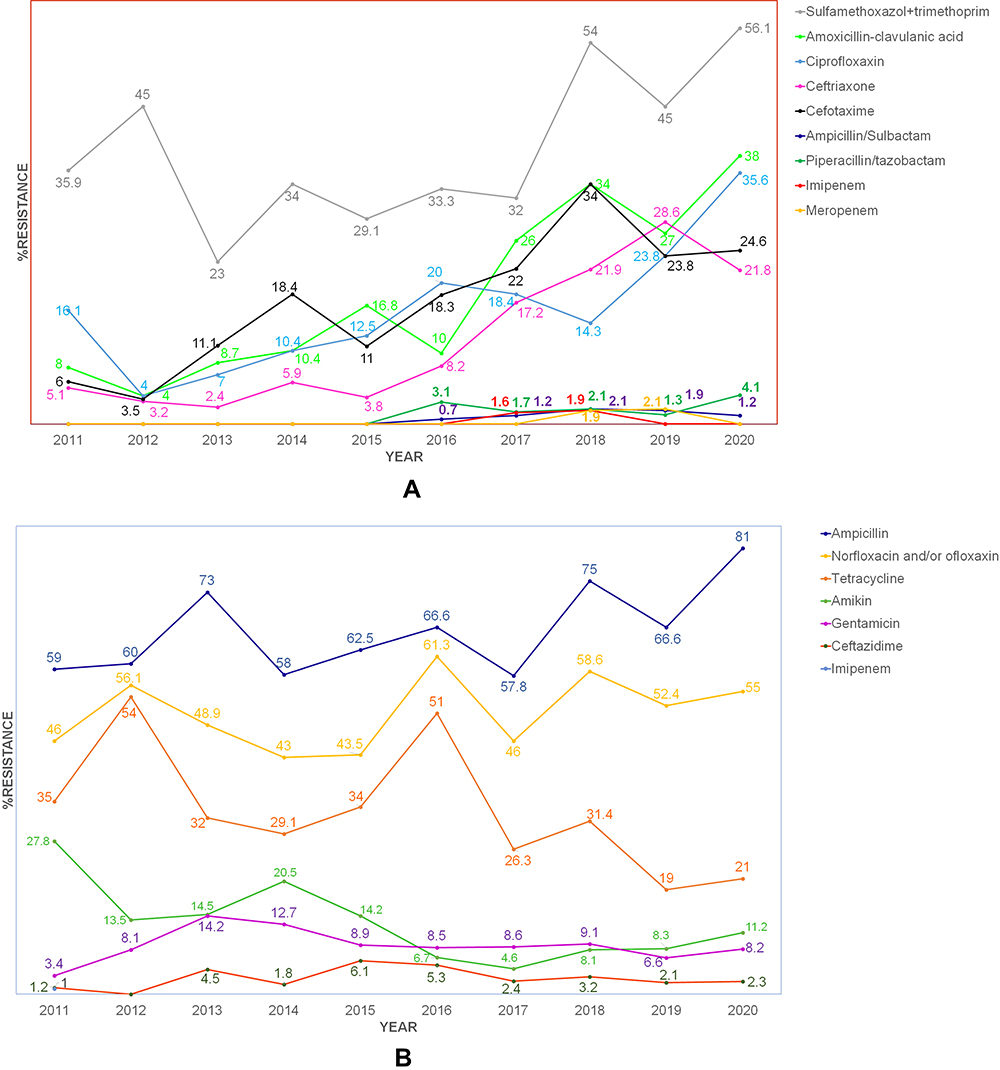 |
Figure 1 Percentage of antimicrobial resistance of all NTS patients since 2011 to 2020. By (A) shows the group of antimicrobials resistance rate which has been rising trend, while (B) shows similar or slight changes. |
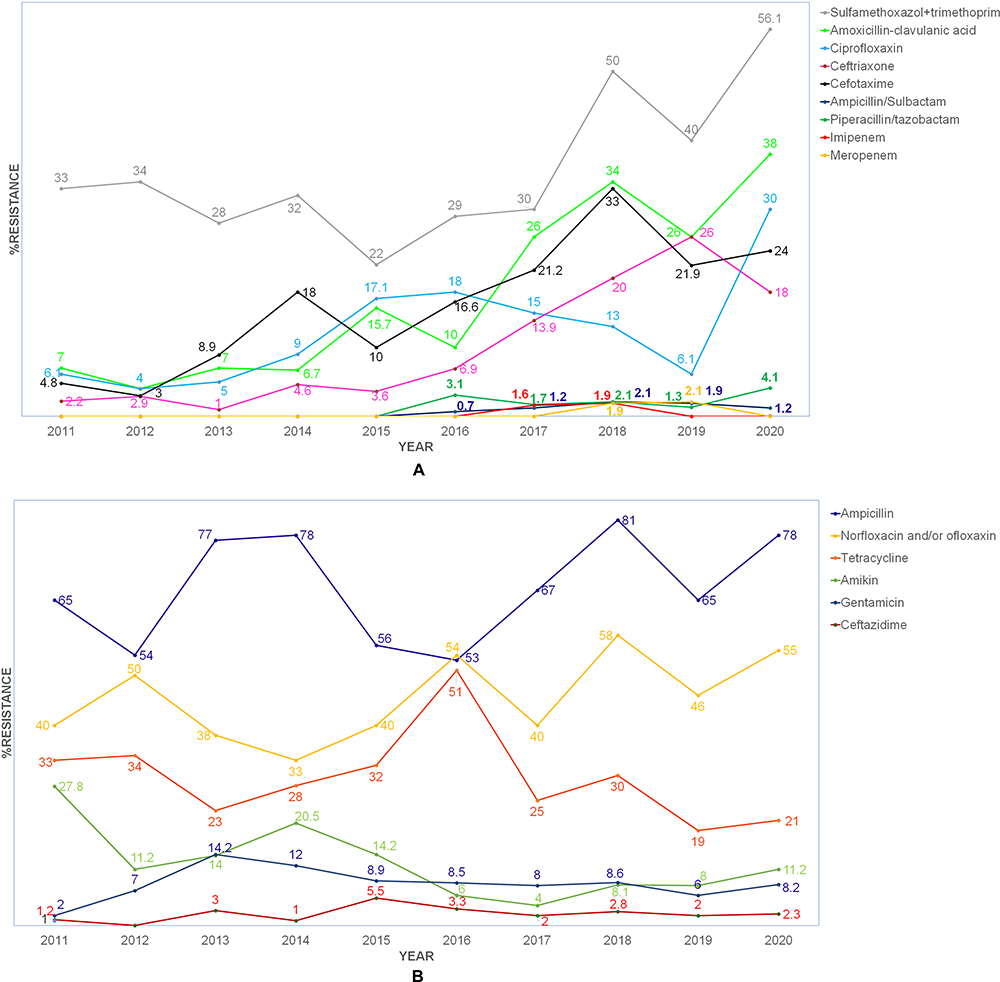 |
Figure 2 Antimicrobial resistance rate of NTS in invasive patients’ groups since 2011 to 2020. By (A) presents increase trend of non-susceptible rate of antimicrobials, while (B) presents similar or few changes. |
Ceftriaxone and Ciprofloxacin Resistances
All NTS resisted ceftriaxone at a rate of 25.4% (n=110/433) (95% CI 0.12–0.99). In 2016–2020, NTS was found to be 2 times more resistant to ceftriaxone (32%) compared to 2012–2015 (16.1%) (PRR 2.95% CI 1.24–3.16). Serogroup A had significantly increased resistance to ceftriaxone, form 1.66% (n=3/180) to 6.32% (n=16/253). Ciprofloxacin resistance was 30% (n=130/433) (95% CI 0.023–0.87) and it also increased in nonsusceptibility rate from 16.1% (n=30/180) in 2011–2015 to 32% (n=100/253) in 2016–2020 (PRR=2.4,95% CI 1.51–3.72). Among serogroup A, B and C the percentage of resistance significantly increased from 2.2% (n=4/180), 3.9% (n=7/180), and 2.8% (n=7/180), in 2012–2015 to 7.1% (n=18/253), 9.9 (n=25) and 13% (n=33/253) in 2016–2019 (PRR 3.2,95% CI 1.06–9.61), (PRR 2.5,95% CI 1.07–6.00), (PRR 3.4,95% CI 1.45–7.75) retrospectively. (Table 2.)
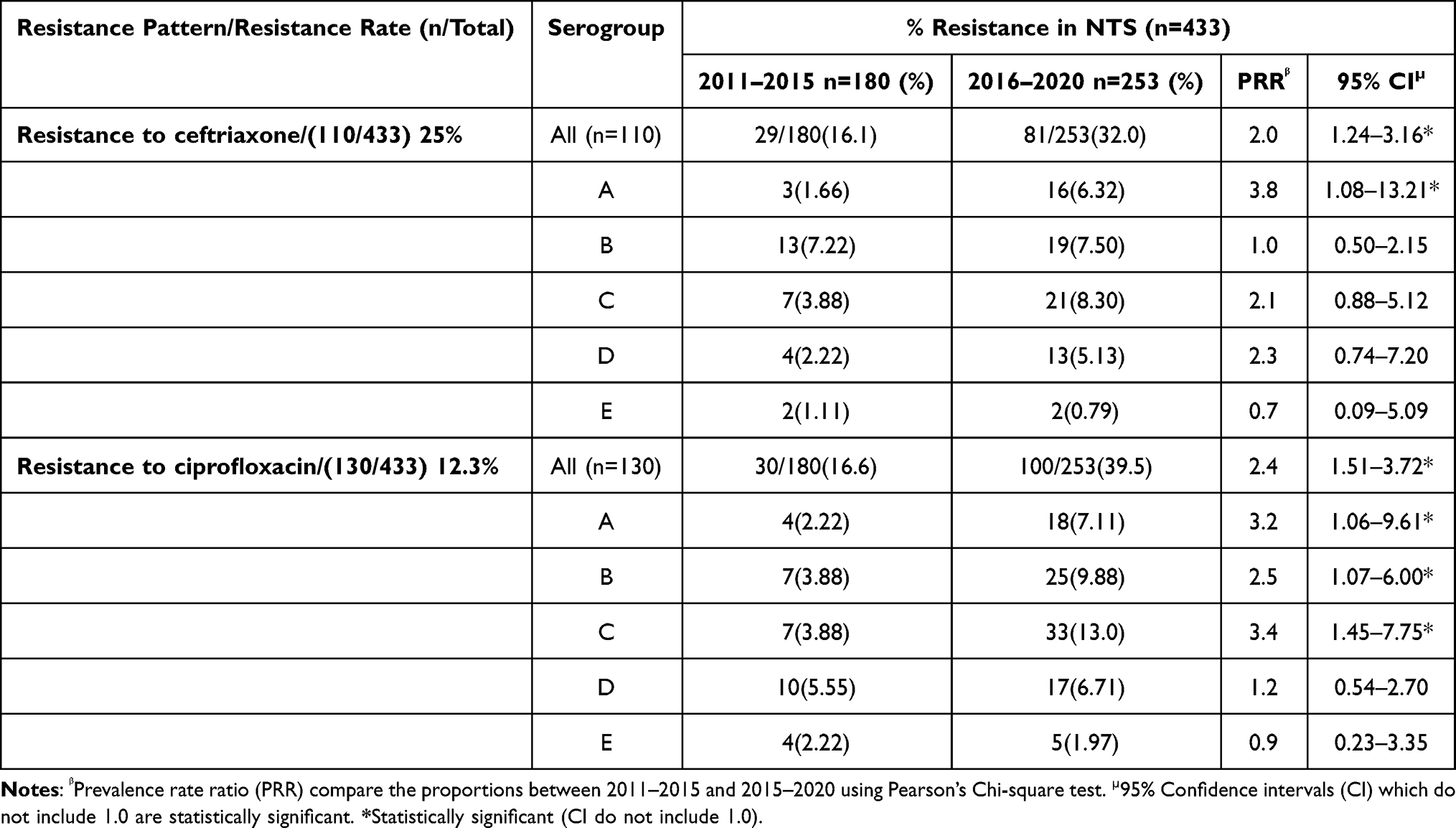 |
Table 2 Comparison the Antimicrobials Resistance Pattern (Ceftriaxone and Ciprofloxacin) by Serogroups of NTS Between 2011–2015 and 2016–2020 |
MDR-NTS Group
The MDR-NTS group was 52.8% (n=229/433) of patients. The MDR rates are showed an increasing trend. (Figure 3.) The median age in this group was 11, IQR (2–67). Patients aged 16–60 years had the highest percentage of MDR at 53.7%, followed by the age groups ≤15 and > 60 years, respectively. The ratio of males to females was 4:5 (195:238). The patient group from the tertiary hospitals had the highest proportion of MDR 62.3% (n=129/207). The non-invasive group had MDR 56.9% (n=152/267) nearly by the invasive group 56.9% (n=94/166) (Table 1). The invasive group included 91 bacteremias,1 meningitis, 1 osteomyelitis, and 1 arthritis. For the non-invasive group, all the patients were gastroenteritis patients. Of MDR-NTS patients (n=229) serogroup C had the highest MDR percentage at 28.3% (n=65/229) (95% CI 23.1–93.9). The NTS patients with metabolic syndrome that diabetes patients were found to have the highest rates of MDR 65.4% (n=21/65) (95% CI 52.9–77.8) (Table 1).
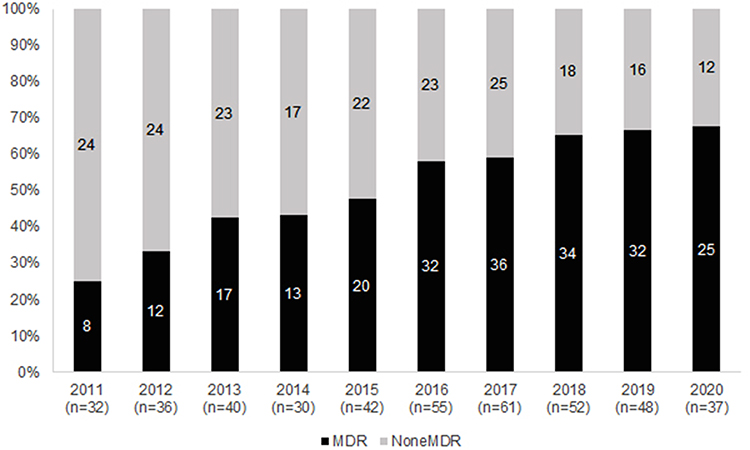 |
Figure 3 The prevalence rate and trend of MDR-NTS, 2011–2020. Black columns represent MDR-NTS. Grey columns represent NDR-NTS. |
Trends of Serogroup and Severity
The most common serogroups were C 28.6% (n=124/433) and then B 24.9% (n=108/433), D 21.9% (n=95/433) E 12.4% (n=54/433) and A 12% (n=52/433) respectively (Table 1). The serogroup C rate expanded significantly from 5% in 2011–2015 to 15% in 2016–2020 (PRR 1.5, 95% CI 0.09–0.86). With the non-serogroup C, there was no significant difference between the two time periods. The study found that the mean length of stay in hospital was longest in serogroup B (18 days) while C was 11 days, D 6 days, E 5 days, and A 4 days, respectively. The patients who were infected with serogroup C had significantly higher proportion of hospital admission longer than five days and of invasive infection than other serogroups 41% (n=82) (PRR 2.27,95% CI1.49–3.45) and 39.7% (n=66) (PRR 1.8,95% CI1.22–2.737) respectively (Table 3.). The most common serogroups which caused infections in the age groups < 15 years, 15–60 years, and > 60 years were serogroup B 34%, C 48%, and C 33.7% respectively (Figure 4).
 |
Table 3 Comparison the Length of Hospital Stays and Virulence Between NTS Serogroup |
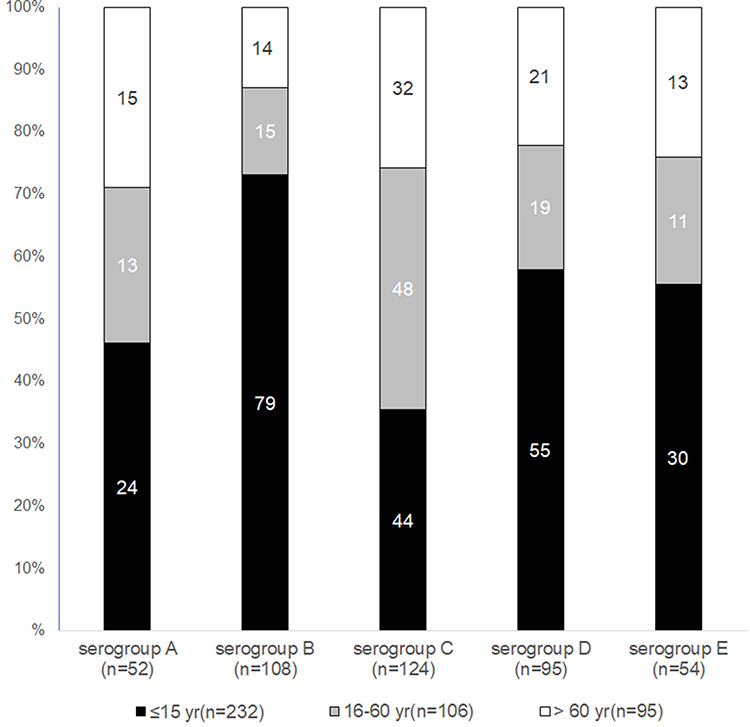 |
Figure 4 Number of infected patients NTS for each serogroup by age group. Black columns represent patients who are ≤ 15 years. Grey columns represent patients who are 16–60 years. White columns represent patients who are > 60 years. |
Discussion
The increase of MDR-NTS is a worldwide public health concern. This study presents an MDR rate of 69% which is higher than a previous study in rural Thailand (2006–2014) (19.2%)21 and higher than some studies in China (40.3%),4 America, and Europe (2–9.6-%)1,2 but lower than studies in Africa (77.2%-87.4)22–24 The increasing trend is the same as many studies worldwide6–8,25 MDR-NTS is associated with β-lactamase production. This study detected a ceftriaxone resistance rate of 25%, more than Thailand surveillance (7.2% in 2020)11 and previous studies in Thailand.1,21,23,27 The NARST presents fluctuations of the peak resistance rate at 37.5% in 2010 and 24.5% in 2015, down to 11% in 2019. The ceftriaxone resistance makes it of limited value as first-line therapy, as a choice of effective antimicrobial agents for treatment, especially for co-resistance with the fluoroquinolones (DNA gyrase and topoisomerase IV),26 which increase morbidity and mortality, also resulting in longer hospital stays, and higher costs.21,27,28
In addition, clinically sometimes patients respond well to antimicrobial while the cultures reports indicate that cultures are not susceptible which makes physicians concerned about the need to change or extended antimicrobial. For ciprofloxacin resistance, this report found 12.3% which was higher than previous studies in and near Thailand.6–8,11,21,23,29 It also showed an increase in 2016–2019 compared with the 2012–2015 period, especially in serogroup A, B, and C. By contrast, NARST showed a rise in the resistance rate from 4.3% in 2012 to 11.8% in 2015, and a subsequent decline to 6.9% in 2019 (%).11
Regarding meningitis caused by Salmonella spp., The American Academy of Pediatrics (AAP) recommends that treatment with ciprofloxacin in addition to ceftriaxone or cefotaxime should continue for 4 weeks or more30 This can reduce recurrence and relapse infection in the event of drug susceptibility. However, for patients infected with ciprofloxacin resistance NTS, it is unclear which is the best practice to prevent recurrence. Therefore, the treatment of such patients must be considered in selecting an appropriate antibiotic.31
Carbapenem resistance is rare in NTS, but in the past 10 years it has become more frequent.32–35 Carbapenem resistance is due to the production of amplified β-lactamases or AmpC spectra in combination with porin loss. The resistance mechanism also includes horizontal gene transfer of encoded genes between organisms. This is an important issue for public health that need to be more investigated and monitored. However, this resistance report is based on interpretation using the agar disk diffusion method, which may not be accurate enough to require further study and investigation at the MIC level.
For the clinical manifestations of carbapenem resistant patients. We found all of them were adult patients. Three cases were diagnosed with gastroenteritis. Some of those patients did not receive antimicrobial drugs but they improved clinically. Only one case was bacteremia that was treated with ceftriaxone after two days of fever reduced (culture reported on day 5 after antimicrobial). In this case the physician continued ceftriaxone and stepped down to oral cephalosporin for a total of 14 days. Often, we find that in vitro and in vivo results are different. We also found the clinical response to ceftriaxone in some cases of the ceftriaxone resistance patients’ groups. While, one case was a Thai boy, 9 months old diagnosed with meningitis with multiple brain abscesses from MDR-NTS serogroup B that was sensitive to many antimicrobials except ampicillin, norfloxacin, tetracycline, and sulfamethoxazole/trimethoprim. This case received ceftriaxone at the first admission, but the clinical condition still worsened from meningitis to multiple brain abscesses, so he stayed in the hospital at 230 days. In this case, immunodeficiency states were investigated, but all were found to be normal. . In addition to antimicrobials, it is an important tool for eliminating pathogens. Immunity is also important. However, further study of the factors contributing to severe infections is required.
In practice, in cases which are suspected invasive Salmonella infection, what antimicrobials would be appropriate choice while the culture results have not been reported. The NTS in this study remained sensitive to ceftazidime (resistance rate 2.8%), like in Chinese studies.35 Ceftazidime was probably the drug of choice before carbapenem was use. Aminoglycosides groups in this study found not high-rate resistance when compared to ceftriaxone or ciprofloxacin, so may be considered concomitant therapy. However, drug selection considers pharmacokinetics and pharmacokinetic, which is clinically related. Azithromycin is a drug of choice due to effective antimicrobial agent with good intracellular penetration. Although there are currently some reports of drug resistance, the AAP guideline still recommends using it in not severe cases or for switching to oral form,30,37 which in this study lacked sensitivity data. However, further studies are required.
Major reports suggest NTS infected with S. Typhimurium (serogroup B) and S. Enteritidis (serogroup D) are predominant worldwide.14,22,29,35 But this study showed serogroup C was most common, while previous studies in Thailand21,23 show S. Choleraesuis (serogroup C1). Over the last decade, studies have shown increases in serogroup C from 22.5% to 34.7% in the United States (1995, 2012) and from 5% to 8.6% in Europe (2005, 2013) while serogroup D showed a corresponding decline in both regions (31.5% in 1995 to 28.1% in 2012 for the United States and 69.1% in 2005 40.6% in 2012 in Europe). Serogroup B showed a similar downward trend in the United States, from 1995 to 2012 (38.7% to 27.6%).2 However, in the under 15 age group, serogroup B was still found to be dominant as in many studies.8,14,21,25,29,38 Serogroup C may spread globally in the future and could develop continuous antimicrobial nonsusceptibility. MDR-NTS S. Choleraesuis (serogroup C1) is mainly a cause of invasive infection and leads to morbidity and mortality in Thailand.27,36 However, when considering the number of serogroup C cases in Table 2, similar numbers were found: C (n = 124), B (n = 108) and D (n = 95). The data collection is insufficient to make sampling bias which needs further study. This is a major problem, both locally and globally, that requires monitoring form public health and more study, particularly the serotype and minimum inhibitory concentration (MIC) which will be more clinically beneficial.
Limitations
The limitation of the study is that not all NST infections underwent antibiotic sensitivity testing, and, in each laboratory, there were differences in the types of antimicrobial tests, depending on the source of the isolated specimen (blood, urine, stool et al), so the analysis may be biased. This research lacked information of MIC and serotype of Salmonella classification because they are not routinely performed in general hospitals, they are only done in some cases prescribed by doctors’ requirements and it is also performed in some hospitals, making our data limited. Lastly, this study’s findings cannot be generalized to a general population, so further studies are needed.
Conclusion
The prevalence of MDR-NTS is still rising, especially in resistance to ceftriaxone and ciprofloxacin, which were the first drug group used for treatment. Antimicrobial selection must be carefully considered depending on drug susceptibility tests and close monitoring. In this region, the NTS serogroup C is on an upward trend when compared to other serogroups, which results in morbidity, mortality, longer hospital stays, and higher costs. Therefore continuous surveillance is imperative.
Ethical Approval
The research protocol was approved by the research ethics committee of Panyananthaphikkhu Chonprathan Medical Center, Srinakharinwirot University. All information was anonymized to maintain patients’ privacy, Declaration of Helsinki. Considering the retrospective and anonymous nature of the study, the Ethics Committee didn’t require written informed consent provided by patients.
Acknowledgments
The authors thank all patients, health practitioners and directors of all hospitals authorized to collect research data. Writing advice, the article from Professor Emeritus Colonel Sriluck Simasathien, special lecturer and advisor department of pediatrics Phramongkutklao Hospital, Bangkok, Thailand, and Professor Thanyawee Puthanakit, pediatric infectious disease specialist at the department of pediatrics, faculty of medicine, Chulalongkorn University, Bangkok, Thailand.
Funding
This work was supported by Panyananthaphikkhu Chonprathan Medical Center, Srinakharinwirot University.
Disclosure
The authors declare that they have no known competing interests in this work.
References
1. Drug-resistant Nontyphoidal Salmonella; 2019. Available from: https://www.cdc.gov/drugresistance/pdf/threats-report/nt-salmonella-508.pdf.
2. Medalla F, Hoekstra RM, Whichard JM, et al. Increase in resistance to ceftriaxone and nonsusceptibility to ciprofloxacin and decrease in multidrug resistance among salmonella strains, United States, 1996–2009. Foodborne Pathog Dis. 2013;10(4):302–309. doi:10.1089/fpd.2012.1336
3. Rabsch W, Tschäpe H, Bäumler AJ. Non-typhoidal salmonellosis: emerging problems. Microbes Infect. 2001;3(3):237–247. doi:10.1016/S1286-4579(01)01375-2
4. Zhang J, Jin H, Hu J, et al. Serovars and antimicrobial resistance of non-typhoidal Salmonella from human patients in Shanghai, China, 2006–2010. Epidemiol Infect. 2014;142(4):826–832. doi:10.1017/S0950268813001659
5. Stanaway JD, Parisi A, Sarkar K, Collaborators GBDN-TSID. The global burden of non-typhoidal salmonella invasive disease: a systematic analysis for the global burden of disease study 2017. Lancet Infect Dis. 2019;19(12):1312–1324. doi:10.1016/S1473-3099(19)30418-9
6. Chen CY, Hsieh PH, Chang CY, et al. Molecular epidemiology of the emerging ceftriaxone resistant non-typhoidal Salmonella in southern Taiwan. J Microbiol Immunol Infect. 2019;52(2):289–296. doi:10.1016/j.jmii.2018.08.007
7. Li WC, Huang FY, Liu CP, et al. Ceftriaxone resistance of nontyphoidal Salmonella enterica isolates in Northern Taiwan attributable to production of CTX-M-14 and CMY-2 beta-lactamases. J Clin Microbiol. 2005;43(7):3237–3243. doi:10.1128/JCM.43.7.3237-3243.2005
8. Jain P, Chowdhury G, Samajpati S, et al. Characterization of non-typhoidal Salmonella isolates from children with acute gastroenteritis, Kolkata, India, during 2000–2016. Braz J Microbiol. 2020;51(2):613–627. doi:10.1007/s42770-019-00213-z
9. Lee K, Yong D, Yum JH, Kim HH, Chong Y. Diversity of TEM-52 extended-spectrum beta-lactamase-producing non-typhoidal Salmonella isolates in Korea. J Antimicrob Chemother. 2003;52(3):493–496. doi:10.1093/jac/dkg385
10. Narasanna R, Chavadi M, Chandrakanth K. Prevalence of multidrug-resistant Salmonella typhi in typhoid patients and detection of blaCTX-M2 and blaCTX-M9 genes in cefetoxime-mediated extended spectrum β-lactamase-producing Salmonella typhi isolates. Biomed Res. 2018;29(14):3015–3021. doi:10.4066/biomedicalresearch.29-18-794
11. National Antimicrobial Resistant Surveillance Center T. The situation of drug resistance 2000–2020 (6M); 2020.
12. Chang YJ, Chen YC, Chen NW, et al. Changing antimicrobial resistance and epidemiology of non-typhoidal Salmonella infection in Taiwanese Children. Front Microbiol. 2021;12:648008. doi:10.3389/fmicb.2021.648008
13. Woh PY, Yeung MPS, Goggins WB, et al. Genomic epidemiology of multidrug-resistant nontyphoidal Salmonella in young children hospitalized for gastroenteritis. Microbiol Spectrum. 2021;9(1):e0024821. doi:10.1128/Spectrum.00248-21
14. Duong VT, The HC, Nhu TDH, et al. Genomic serotyping, clinical manifestations, and antimicrobial resistance of nontyphoidal salmonella gastroenteritis in hospitalized children in Ho Chi Minh City, Vietnam. J Clin Microbiol. 2020;58(12):e01465–20. doi:10.1128/JCM.01465-20
15. Situation Domestic Travellers by Province: 2010 – 2019. Tourism and sport statistics. Available from:http://statbbi.nso.go.th/staticreport/page/sector/en/17.aspx.
16. WHO: 2014–2016 ICD-10-CM Diagnosis Code A02.0-02.9 Salmonella infection. Available from: https://www.icd10data.com/ICD10CM/Codes/A00-B99/A00-A09/A02-/A02.9.
17. Grimont PA, Weill FX. Antigenic formulae of the Salmonella Serovars. WHO Collaborating Centre for Reference and Research on Salmonella; 2007.
18. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
19. Bureau of Laboratory Quality S. History and Authority. Available from: http://blqs.dmsc.moph.go.th/en/page-view/22.
20. Magiorakos A, Srinivasan RB, Carey Y, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
21. Whistler T, Sapchookul P, McCormick DW, et al. Epidemiology and antimicrobial resistance of invasive non-typhoidal Salmonellosis in rural Thailand from 2006–2014. PLoS Negl Trop Dis. 2018;12(8):e0006718–e0006718. doi:10.1371/journal.pntd.0006718
22. Kariuki S, Mbae C, Onsare R, et al. Multidrug-resistant nontyphoidal Salmonella hotspots as targets for vaccine use in management of infections in endemic settings. Clin Infect Dis. 2019;68(Suppl 1):S10–S15. doi:10.1093/cid/ciy898
23. Srijan A, Lurchachaiwong W, Wongstitwilairoong B, Bodhidatta L, Mason C, Swierczewski B. Prevalence and antimicrobial resistance of non-typhoid Salmonella in military personnel, 1988–2013. Asian Pac J Trop Med. 2018;11:387–392. doi:10.4103/1995-7645.234767
24. Tack B, Marie-France P, Barbé B, et al. Non-typhoidal Salmonella bloodstream infections in Kisantu, DR Congo: emergence of O5-negative Salmonella Typhimurium and extensive drug resistance. PLoS Negl Trop Dis. 2020;14(4):e0008121. doi:10.1371/journal.pntd.0008121
25. Miriam W, Nathan K. Recent trends in the epidemiology of non-typhoid Salmonella and antimicrobial resistance: the Israeli experience and worldwide review. Curr Opin Infect Dis. 2005;18(6):513–521. doi:10.1097/01.qco.0000186851.33844.b2
26. Gunell M, Webber MA, Kotilainen P, et al. Mechanisms of resistance in nontyphoidal strains exhibiting a nonclassical quinolone resistance phenotype. Antimicrob Agents Chemother. 2009;53(9):3832–3836. doi:10.1128/AAC.00121-09
27. Kulwichit W, Chatsuwan T, Unhasuta C, Pulsrikarn C, Bangtrakulnonth A, Chongthaleong A. Drug-resistant nontyphoidal Salmonella bacteremia, Thailand. Emerg Infect Dis. 2007;13(3):501–502. doi:10.3201/eid1303.061059
28. Liang Z, Ke B, Deng X, et al. Serotypes, seasonal trends, and antibiotic resistance of non-typhoidal Salmonella from human patients in Guangdong Province, China, 2009–2012. BMC Infect Dis. 2015;15:53. doi:10.1186/s12879-015-0784-4
29. Lee H-Y, Su L-H, Tsai M-H, et al. High rate of reduced susceptibility to ciprofloxacin and ceftriaxone among nontyphoid clinical isolates in Asia. Antimicrob Agents Chemother. 2009;53(6):2696–2699. doi:10.1128/AAC.01297-08
30. Wen SCH, Best E, Nourse C. Non-typhoidal Salmonella infections in children: review of literature and recommendations for management. J Paediatr Child Health. 2018;53(10):936–941. doi:10.1111/jpc.13585
31. Price EH, de Louvois J, Workman MR. Antibiotics for Salmonella meningitis in children. J Paediatr Child Health. 2017;53(10):936–941.
32. Javier F, Beatriz G, Rosario RM. Resistance to carbapenems in non-typhoidal Salmonella enterica serovars from humans, animals and food. Vet Sci. 2018;5(2):40. doi:10.3390/vetsci5020040
33. Day MR, Meunier D, Doumith M, de Pinna E, Woodford N, Hopkins KL. Carbapenemase-producing Salmonella enterica isolates in the UK. Antimicrob Agents Chemother. 2015;70(7):2165–2167. doi:10.1093/jac/dkv075
34. Changab YJ, Chena MC, Feng Y, et al. Highly antimicrobial-resistant Nontyphoidal Salmonella from retail meats and clinical impact in children, Taiwan. Pediatr Neonatol. 2020;61(4):432–438. doi:10.1016/j.pedneo.2020.03.017
35. Varma JK, Mølbak K, Barrett TJ, et al. Antimicrobial‐resistant nontyphoidal salmonella is associated with excess bloodstream infections and hospitalizations. J Infect Dis. 2005;191(4):554–561. doi:10.1086/427263
36. Fuche FJ, Sow O, Simon R, Tennant SM, Salmonella Serogroup C, Papasian CJ. Current status of vaccines and why they are needed. Clin Vaccine Immunol. 2016;23(9):737–745. doi:10.1128/CVI.00243-16
37. Tack B, Vanaenrode J, Verbakel JY, Toelen J, Jacobs J. Invasive non-typhoidal Salmonella infections in sub-Saharan Africa: a systematic review on antimicrobial resistance and treatment. BMC Med. 2020;18(1):212. doi:10.1186/s12916-020-01652-4
38. Liang B, Xie Y, He S, et al. Prevalence, serotypes, and drug resistance of nontyphoidal Salmonella among pediatric patients in a tertiary hospital in Guangzhou, China, 2014–2016. J Infect Public Health. 2019;12(2):252–257. doi:10.1016/j.jiph.2018.10.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.