Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Prevalence and Risk Factors of Post-Traumatic Stress Disorder in Survivors of a Cohort of Road Accident Victims in Benin: Results of a 12-Month Cross-Sectional Study
Authors Daddah D ![]() , Glèlè Ahanhanzo Y
, Glèlè Ahanhanzo Y ![]() , Kpozehouen A
, Kpozehouen A ![]() , Hounkpe Dos Santos B, Ouendo EM, Levêque A
, Hounkpe Dos Santos B, Ouendo EM, Levêque A
Received 14 January 2022
Accepted for publication 25 March 2022
Published 5 April 2022 Volume 2022:15 Pages 719—731
DOI https://doi.org/10.2147/JMDH.S358395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Donatien Daddah,1,2 Yolaine Glèlè Ahanhanzo,1 Alphonse Kpozehouen,1 Bella Hounkpe Dos Santos,1,2 Edgard-Marius Ouendo,3 Alain Levêque2
1Epidemiology and Biostatistics Department, Regional Institute of Public Health, Ouidah, Benin; 2Center for Research in Epidemiology, Biostatistics and Clinical Research, Public Health School, (Université Libre de Bruxelles), Brussels, Belgium; 3Health Policies and Systems Department, Regional Institute of Public Health, Ouidah, Benin
Correspondence: Donatien Daddah, Epidemiology and Biostatistics Department, Regional Institute of Public Health, P.O. Box 384, Ouidah, Benin, Tel +229 97167245, Email [email protected]
Purpose: Post-traumatic stress disorder (PTSD) is a frequent psychiatric complication in road accident survivors. However, it remains under-explored and is not taken into account in health policies in Benin. The purpose of this study was to determine the prevalence and risk factors of PTSD after a road traffic accident. This will help to improve its diagnosis and management in Benin hospitals.
Materials and Methods: An institution-based cross-sectional study was conducted from November 2020 to January 2021. Consenting victims of road traffic accidents from three hospitals across Benin, aged 18 years and above, living in the south of the country, were administered various questionnaires at 12-month follow-up. Data on PTSD were collected using a pre-tested, structured and standardized post-traumatic stress disorder questionnaire, the PTSD Checklist (specific version) (PCL-S). A logistic regression model was fitted to identify factors associated with PTSD. An adjusted odds ratio (AOR) followed by a 95% confidence interval was calculated to determine the level of significance with a p-value less than 0.05.
Results: Out of 865 patients in the cohort eligible for the 12-month follow-up, 734 (85%) participated in the study. The prevalence of PTSD was 26.43% (95% CI: 23.36– 29.75). Factors associated with PTSD on multivariate analysis were female gender (adjusted odds ratio (AOR) = 2.14, 95% CI: 1.38– 3.33), hospitalization (AOR = 1.87, 95% CI 1.21– 2.89), negative impact of the accident on income (AOR = 4.22, 95% CI: 2.16– 8.25), and no return to work (AOR = 3.17, 95% CI: 1.99– 5.06).
Conclusion: The prevalence of PTSD is high in road accident survivors in Benin. The results of this study highlight the need for early diagnosis and a multidisciplinary approach to the management of PTSD patients in Benin’s hospitals.
Keywords: PTSD, prevalence, risk factors, road accident survivors
Introduction
Road accidents, in addition to their fatal consequences, are the cause of significant morbidity with social, professional, economic, physical and psychological impacts.1–10 According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), post-traumatic stress disorder (PTSD) is diagnosed in people who have experienced traumatic events.11 Around the world, it is one of the most frequent and debilitating psychiatric disorders following an event such as a road accident, terrorist attack, nuclear accident or natural catastrophe (flood, hurricane, earthquake).12–19 The World Health Organization (WHO) Global Burden of Disease Survey estimates that mental illnesses, including stress-related disorders, will be the second leading cause of disability around the world by 2020.9,20 It is a public health problem that contributes to poverty, unemployment, insecurity of living conditions and changes to social networks, and is strongly associated with a low quality of life.21
Several studies have been conducted on PTSD and other psychiatric disorders after a road accident, with varying prevalence depending on the context.6,22,23 Studies conducted in Ethiopia have reported prevalence among road accident survivors ranging from 15 to 47%.16,24–27 Several other studies have been conducted worldwide on PTSD and have identified prevalence ranging from 13.3% to 48.2%.10,28–30
This prevalence also varies according to the time elapsed between the accident and the time of the evaluation. One study found prevalence of at least one psychiatric disorder including PTSD of 48.2%, 52.5% and 49.3%, at 6, 12 and 24 months respectively after an accident. Over 42% of patients had unstable diagnostic patterns between follow-up periods.31
A variety of factors contribute to the occurrence of PTSD and extensive research in different countries, including East Africa, has also revealed wide variability in the factors associated with PTSD among patients. The main factors identified in the literature as significantly associated with PTSD were female gender, lack of social support, divorce, pre-traumatic depressive symptoms, personal or family history of mental illness, common mental disorders, severity of injury, history of near misses, use of psychiatric medication, anxiety, depression and history of a road accident, among others.7,16,25–27,32
Despite the rich literature on PTSD worldwide, it has been little studied by researchers in West Africa and particularly in Benin. The management of road traffic injuries is limited to the management of physical problems rather than the holistic management of survivors’ health problems.
Many studies have shown that PTSD is associated with important economic and social factors in victims, such as unemployment and low household income.6,25,33–38
We hypothesize that PTSD is related to the adverse economic impact of the road accident on the victim.
This study aims to determine the prevalence and risk factors of PTSD after a road traffic accident. This could contribute to better screening and integrated management of PTSD in hospitals in Benin.
Materials and Methods
Study Settings and Period
This is a cross-sectional study conducted at approximately 12 months after the accident among survivors of a hospital-based cohort of road traffic accident victims called the “TraumAR Cohort”. This cohort was set up in Benin as part of a Multidisciplinary Research for the Prevention of Road Accidents project (ReMPARt). The initial data collection took place in five reference hospitals that treated road accident injuries. These were: (i) the Centre National Hospitalier Hubert Koutoukou Maga, the only national referral hospital for road accidents and all other diseases in Benin, (ii) the Centre Hospitalier Departemental Oueme-Plateau, an intermediate level hospital in the health system of Benin and a referral center for several other hospitals in the region, (iii) the Hopital de Zone de Menontin, a peripheral level hospital in the health system, which frequently treats victims of road accidents, (iv) the Centre Hospitalier Departemental Borgou-Alibori, an intermediate level hospital in the health system and the largest in the northern region of Benin. It is the main referral center for all hospitals in this region of Benin and (v) the district level hospital called Hopital de Zone de Boko. These hospitals are located throughout the country.
Baseline data were collected from July 2019 to January 2020 by direct administration of the questionnaire to patients or to one of their parents if they were unable to answer. Medical records were also used to collect baseline medical data.
After the baseline collection, patients were then followed up twice: the first at approximately 6 months after the accident with a questionnaire administered via telephone and the second at approximately 12 months after the accident, with physical examination and face-to-face administration of different questionnaires, in a care setting, including the PTSD screening questionnaire.
Study Population
The study population was consenting survivors of road traffic accidents living in southern Benin, aged 18 years and above, admitted 12 months previously to the three selected hospitals in the south of the country. Patients recruited from the other two hospitals in the north were not included in the study due to lockdown measures imposed during the COVID-19 pandemic, which limited travel to certain regions of the country.
Sampling
An exhaustive recruitment of all individuals meeting the selection criteria was performed. A total of 865 patients in the cohort were eligible for 12-month follow-up.
Data Collection and Measurements
Data collection on PTSD was carried out only at the 12-month follow-up at three sites by teams of two, one of which was a nurse trained in data collection using the questionnaire interview technique. Collection team were supervised by a medical epidemiologist responsible for data quality control. All eligible subjects in the cohort were contacted in advance by telephone to make an appointment. For those who could not travel to the collection site, an appointment for a home visit was made.
During this collection, the patients were given a clinical examination, with the administration of a tool that examined the psychological state of the patients.
These tools were pre-tested at the district hospital of Ouidah on a sample of patients not included in this study. The tool used to screen for post-traumatic stress disorder was the specific version of the checklist (PCL-S). This is a standardized self-report PTSD scale consisting of 17 items that correspond to the main symptoms of PTSD in the Diagnostic and Statistical Manual of Mental Disorders DSM-IV.11 This tool included Likert-scale response options ranging from 1 “not at all” to 5 “extremely” according to the intensity and frequency of symptoms during the previous month. The 17 items were grouped into 3 clusters corresponding to the 3 main syndromes of PTSD: intrusion (items 1 to 5: total score 5 to 25); avoidance (items 6 to 12: total score 7 to 35) and hyperstimulation (items 13 to 17: total score 5 to 25). The total PTSD symptom severity score ranging from 17 to 85 was obtained by adding together the scores for each item.39 A cut-off score of 34 was used for the diagnosis of PTSD.
The dependent variable was post-traumatic stress disorder in survivors of traffic accidents at 12-months.
The independent variables studied were: i) sociodemographic data: age (18–24; 25–35; 36–45; 46 and over), sex, marital status (single, married/with a partner, divorced/separated), professional status (employed, in training, unemployed), Body Mass Index (BMI); ii) clinical and lifestyle characteristics: history of chronic disease (psychiatry, heart disease), history of road accidents, drug, alcohol, and tobacco consumption; iii) road accident-related characteristics: type of road user (pedestrian, motorcyclist, other), driver of the vehicle, pattern of traumatic injury (head, upper limbs, thorax/abdomen, lower limbs), severity of injury as measured by the Abbreviated Injury Scale (AIS), hospitalization, means of transport to the hospital (ambulance, 2–3 wheeled vehicle, private vehicle, on foot), collected at baseline; and iv) economic impacts of the accident: negative impact on income and not returning to work, which were collected at 12-month follow-up.
Analysis
Data were processed and analyzed using Stata 15 software. Quantitative variables were presented as a mean (standard deviation) after checking for normality. Qualitative data were presented as a percentage. The prevalence of PTSD was calculated with its 95% confidence interval. Factors associated with PTSD 12 months after the accident were identified by performing a univariate analysis and subsequently a multivariate analysis. The univariate analysis consisted of cross tabulating the dependent variable with each of the independent variables, using simple logistic regression. Thus, all covariates were examined for inclusion in the multivariate analysis using a threshold of p < 0.1. The multivariate analysis consisted of multiple logistic regression using a top-down stepwise strategy. Variables with p value greater than 0.05 were removed one-by-one from the initial model. Co-linearity between variables was sought. The final results were presented as Adjusted Odd Ratios (AOR) with the 95% confidence interval. The goodness-of-fit (Hosmer and Lemeshow) and specification tests (linktest) of the final model were also performed.
Results
Socio-Demographic Characteristics
Out of the 865 eligible patients in the cohort, 734 (85%) responded to the 12-month follow-up.
Most patients were over 25 years old (n = 602, 82.02%). They were predominantly male (n = 543, 73.98%) and married or with a partner (n = 497, 69.80%). Their mean age and body mass index were 38.04 (SD=12.38) years and 24.04 (SD=3.76) kg/m2 respectively (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Road Accident Survivors Followed at 12 Months, Benin, 2020–2021 |
Clinical and Lifestyle Characteristics
In 24.86% of the cases, the survivors had a history of chronic disease (psychiatric or cardiovascular), 7.65% reported habitual drug or tobacco use, and 68.47% reported habitual alcohol use (Table 2).
 |
Table 2 Clinical and Lifestyle Characteristics of Road Accident Survivors Followed at 12 Months, Benin, 2020–2021 |
Characteristics Related to the Road Accident
The patients were mostly motorcyclists (n = 605, 83.10%) and drivers of the vehicle involved in the accident (n = 475, 75.52%). Injuries were mostly located in the thorax or abdomen (n = 497, 67.71%). The proportion of severe injuries, according to the AIS severity score, was 13.48% at 12 months in road accident survivors and the main means of transport to the hospital l was ambulance (n = 287, 39.53%) (Table 3).
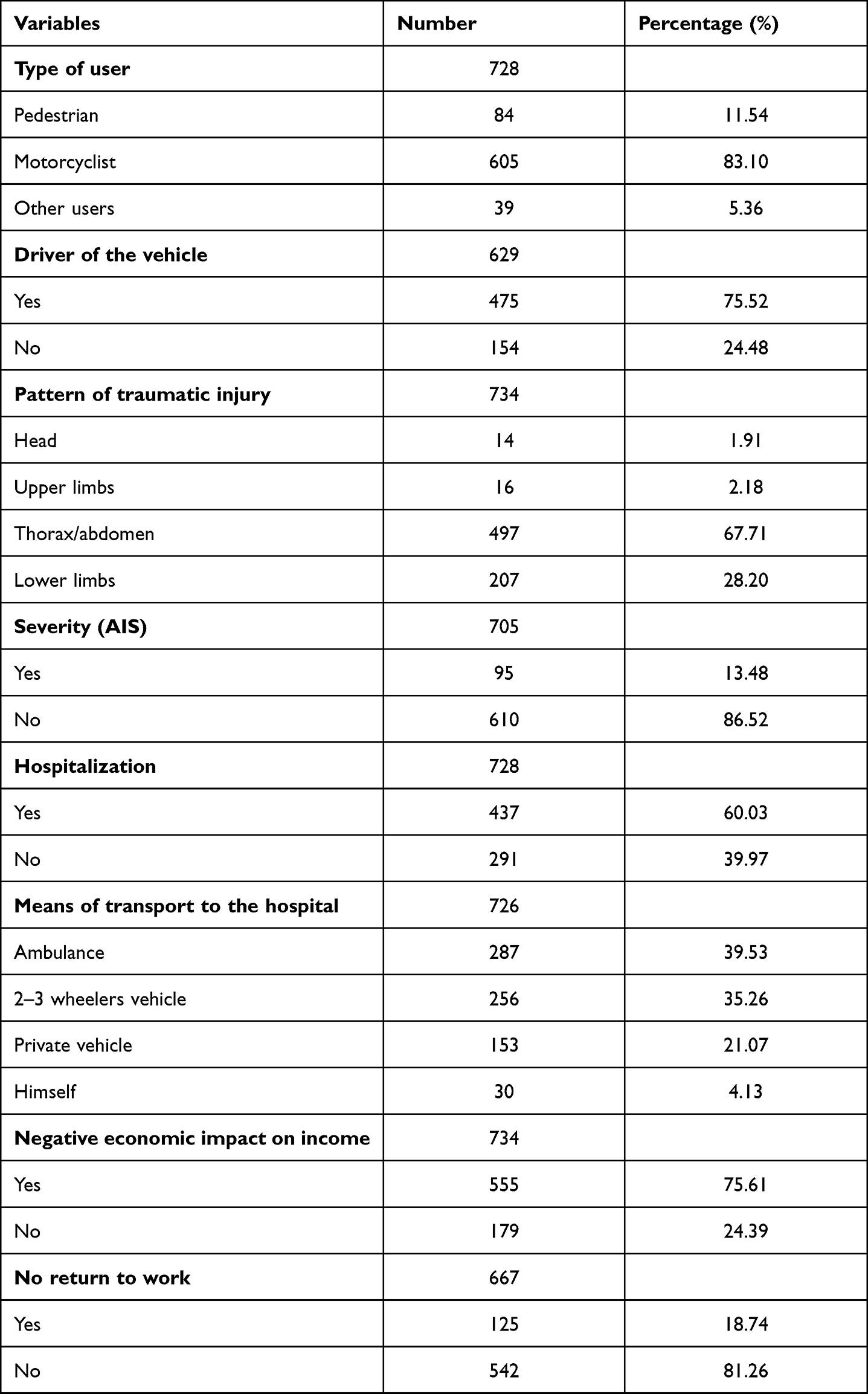 |
Table 3 Road Accident Characteristics and their Economic Impact on Survivors at 12 Months, Benin, 2020–2021 |
Economic Impact of the Accident
Road accident survivors reported in 75.61% of cases that it had a negative impact on their income and 18.74% of survivors in employment before the crash had not yet returned to work 12 months after the accident (Table 3).
Prevalence and Factors Associated with PTSD
Out of the 734 road accident survivors followed up at 12 months, 194 met the definition of PTSD, a prevalence of 26.43% (95% Confidence Interval [CI] = 23.36–29.75).
In univariate analysis, compared to subjects aged 18 to 24 years, patients aged 25 to 35 years had a higher risk of PTSD (OR = 2.17, 95% CI 1.28–3.68) followed by those aged 36 to 45 years (OR = 1.77, 95% CI 1.03–3.04). Similarly, female (OR = 1.83, 95% CI 1.28–2.61) and married/ with a partner subjects (OR = 1.68, 95% CI 1.10–2.58) had an increased risk of developing PTSD than male and single survivors respectively. Injuries to the upper limbs were more strongly associated with PTSD than injuries to other parts of the body (OR = 4.47, 95% CI 1.59–12.53). In addition, hospitalized patients were more likely to develop PTSD than non-hospitalized patients (OR = 2.26, 95% CI 1.54–3.32). It was also noted that patients transported to hospitals by ambulance were more likely to develop PTSD than those admitted to the hospital by other means (OR = 2.02, 95% CI 1.36–3.00). Finally, the negative impact of the accident on income and not returning to work since the accident were also significantly associated with PTSD (OR = 6.18, 95% CI 3.42–11.17) (Table 4).
 |
Table 4 Factors Associated with PTSD in Road Accident Survivors Followed at 12 Months, Benin, 2020–2021: Univariate Analysis |
Multivariate analysis showed that female gender, patient hospitalization, negative impact on income, and not returning to work were predictors of PTSD in the final model.
After adjustment for other variables, the probability of PTSD occurrence was higher in female than in male patient (AOR = 2.14; 95% CI: 1.38–3.33) (p = 0.001). Similarly, hospitalization of the patient increased the probability of PTSD occurrence (AOR = 1.87; 95% CI: 1.21–2.89) (p = 0.005). Furthermore, the negative impact of the accident on the patient’s income was associated with the occurrence of PTSD in survivors (AOR = 4.22; 95% CI: 2.16–8.25) (p < 0.001). Finally, not returning to work was also a predictor of PTSD (AOR = 3.17; 95% CI: 1.99–5.06) (p < 0.001) (Table 5).
 |
Table 5 Factors Associated with PTSD in Road Accident Survivors Followed at 12 Months, Benin, 2020–2021: Final Model |
The model was adequate, p = 0.462 (Hosmer and Lemeshow), and specific, p=0.000 (linktest).
Discussion
The present study aimed to determine the prevalence and factors associated with the occurrence of post-traumatic stress disorder (PTSD) at approximately 12 months in road accident survivors in Benin.
Results showed that the prevalence of PTSD was 26.43%. The associated factors were female gender, hospitalization of the survivor after the accident, not having returned to work at the 12-month follow-up, and negative impact of the accident on the survivor’s income.
Prevalence of Post-Traumatic Stress Disorder
The prevalence of PTSD was 26.43%, which is close to the 26.7% and 22.8% observed by Iteke et al and Yohannes et al respectively in road accident survivors.10,25 Nevertheless, it is higher than the 12.6% observed by Alenko et al33,40 These authors used another PTSD screening tool, the Trauma Screening Questionnaire (TSQ). In addition, the collection was limited to the group of male drivers of public transport vehicles. In other studies, Bedaso et al and Kim et al found a similarly low prevalence of 15.4% and 5.6% respectively.17,24 Although Bedaso et al used the PCLS tool in hospital-recruited road accident survivors, the difference in prevalence may be due to the fact that the assessment was performed within only one month after the road accident.24 In the Kim et al study, this difference could be related to the tool used for the assessment of PTSD. This tool was the Korean version of the Composite International Diagnostic Interview (K-CIDI 2.1).17 A WHO survey found a low prevalence of PTSD of 2.5% among survivors of potentially fatal road accidents.41
The prevalence found in this study is nevertheless lower than that observed in several other studies.26,42–45 This wide variability in PTSD prevalence was found in a meta-analysis conducted by Lin et al who observed prevalence ranging from 6.3% to 58.3%.46
This difference could be due to the 12-month period considered in this study, which is not the case in several other studies that have assessed prevalence at widely varying time periods. In these studies, assessment tools, thresholds for PTSD diagnosis and study design are heterogeneous. Nevertheless, a multicenter survey conducted in 24 countries demonstrated that higher levels of vulnerability in a country is associated with a decreased risk of PTSD in the population. In this research, the highest prevalence was observed in Canada, the Netherlands and Australia, while the lowest was noted in Nigeria, China and Romania.47 We could therefore also note the role of individual and collective resilience of individuals in each country in the face of psychosocial risks. This is also the case in Israel, for example, where the low prevalence of PTSD in a context of recurrent attacks has been explained by certain authors by a process of habituation and adaptation mechanisms developed by the population.18,23
Factors Associated with Post-Traumatic Stress Disorder
The results show that women were at greater risk for PTSD than men. This excess risk for women is consistent in most of the studies found in the literature.1,7,10,25,26,42,48 However, Sadat et al found no association between PTSD and the gender of survivors.30 The vulnerability of the patients in this study could be explained by the fact that in Benin there is no mechanism for financial support or psychological support for road accident survivors. They are often forced to sell valuables to cover expenses, which can cause emotional damage and distress in these survivors. This situation is exacerbated in Benin context when the patient is a woman, as she plays a central role in the household and society with important responsibilities towards children, husbands and the family in general. Some authors have linked this to women having a lower capacity to cope.12 Still others have justified it by women adapting poorly, interpreting trauma more negatively than men.49–51
Other risk factors identified were hospitalization, not returning to work, and negative economic impact of the accident on income. Our hypothesis that PTSD is related to a negative economic impact of the traffic accident on the victim is thus verified. Similar results have been found by other authors in survivors with severe initial injuries as well as in hospitalized patients.45,52 In addition, some authors had noted that perceived social deprivation and loss of professional activity due to the accident were risk factors for PTSD.52,53
Having little financial or social support is therefore an important factor in the development of PTSD.25,26,33–38 Some authors have also identified factors with a psychological impact, such as divorce, was as being significantly associated with PTSD.45 A study conducted at 12 months on the ESPARR cohort in the Rhône region found that subjects from lower socio-economic backgrounds experience many difficulties after an accident, particularly in returning to work. The authors concluded that it would be very important to better take into account and treat PTSD.5 These results could be explained by the financial vulnerability of underpaid patients without a culture of healthcare provision or alternative mechanisms to cover the costs of care.
Strengths and Limitations
The cross-sectional design of the study may have only partially captured temporal relationships. This does not however invalidate the study.
Social desirability and recall biases could have interfered with survivors’ decisions when the questionnaire was administered. Individuals without PTSD symptoms may have less recall of a previous exposure than those with PTSD symptoms.
Another limitation of this study is that some pre-injury factors were not collected, and the DSM-IV tool used for collection is an older version compared to the DSM-V. However, the tool has been validated and has good internal consistency. Another strength of this study is that the collection was performed by trained health professionals under the supervision of medical epidemiologists. Finally, the study is original in Benin and used a relatively representative sample.
Conclusion
The high prevalence of PTSD demonstrates that road accidents have a large impact on the mental health of survivors in Benin.
Female gender, hospitalization after the accident, not having returned to work, and negative impact of the accident on the survivor’s income were significantly associated with PTSD at 12 months.
Early diagnosis of patients at risk of PTSD and a multidisciplinary approach to the management of PTSD patients, involving trauma specialists, psychologists, and psychiatrists could improve survivors’ health.
Abbreviations
K-CIDI, The Korean version of the Composite International Diagnostic Interview; WHO, World Health Organization; PCLS, Post Traumatic Stress Disorder Checklist (specific version); ReMPARt, Multidisciplinary Research for the Prevention of Road Accidents; PTSD, Post-Traumatic Stress Disorder; SD, Standard Deviation; TSQ, Trauma Screening Questionnaire.
Ethics Approval
This study is part of a doctoral thesis. Due to the absence of an ethics committee at the Regional Institute of Public Health (IRSP) in Ouidah, the study protocol was submitted and approved by the Ethics Committee of the University of Parakou (Benin), one of the three ethics committees in Benin, under the reference 0182/CLERB-UP/P/SP/R/SA. At recruitment and follow-up, participants were informed of the purpose of the study and of their right to agree or not to participate in the study without compromising their right to care. They could also withdraw from the study at any time. Participation in the cohort was conditional on the patient or a relative signing a free and informed consent form. Patient privacy and confidentiality were respected at all stages of this study, and data were treated as confidential. The present study complies with the Declaration of Helsinki.
Acknowledgments
We thank the patients of the TraumAR cohort who freely agreed to participate in the 12-month follow-up, the investigators, the focal points, and the staff of the hospitals involved.
Disclosure
The authors report no conflicts of interest for this study/work.
References
1. Hasselberg M, Kirsebom M, Bäckström J, Berg HY, Rissanen R. I did NOT feel like this at all before the accident: do men and women report different health and life consequences of a road traffic injury? Inj Prev. 2019;25(4):307–312. doi:10.1136/injuryprev-2017-042673
2. Waszkowska M, Merecz D. [Psychological effects of road accidents: a challenge for public health]. Med Pr. 2006;57(5):479–484. Polish.
3. Mayou R, Bryant B. Consequences of road traffic accidents for different types of road user. Injury. 2003;34(3):197–202. doi:10.1016/S0020-1383(02)00285-1
4. Pélissier C, Fort E, Fontana L, Hours M. Medical and socio-occupational predictive factors of psychological distress 5 years after a road accident: a prospective study. Soc Psychiatry Psychiatr Epidemiol. 2020;55(3):371–383. doi:10.1007/s00127-019-01780-0
5. Nhac-Vu H-T, Hours M, Chossegros L, et al. Prognosis of outcome in adult survivors of road accidents in France: one-year follow-up in the ESPARR cohort. Traffic Inj Prev. 2014;15(2):138–147. doi:10.1080/15389588.2013.804180
6. Heron-Delaney M, Kenardy J, Charlton E, Matsuoka Y. A systematic review of predictors of posttraumatic stress disorder (PTSD) for adult road traffic crash survivors. Injury. 2013;44(11):1413–1422. doi:10.1016/j.injury.2013.07.011
7. Mosaku K. Predictors of posttraumatic stress in patients admitted to a trauma unit following Road Traffic Accident (RTA). J Psychiatry. 2014;17:121.
8. Matthews LR. Work potential of road accident survivors with post-traumatic stress disorder. Behav Res Ther. 2005;43(4):475–483. doi:10.1016/j.brat.2004.03.008
9. Kalia M. Assessing the economic impact of stress[mdash]The modern day hidden epidemic. Metabolism. 2002;51(6,Part B):49–53. doi:10.1053/meta.2002.33193
10. Iteke O, Bakare MO, Agomoh AO, Uwakwe R, Onwukwe JU. Road traffic accidents and posttraumatic stress disorder in an orthopedic setting in South-Eastern Nigeria: a controlled study. Scand J Trauma Resusc Emerg Med. 2011;19(1):39. doi:10.1186/1757-7241-19-39
11. Bell CC. DSM-IV: diagnostic and statistical manual of mental disorders. JAMA. 1994;272(10):828–829. doi:10.1001/jama.1994.03520100096046
12. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27(1):78–91. doi:10.1093/epirev/mxi003
13. Haagsma JA, Polinder S, Olff M, Toet H, Bonsel GJ, van Beeck EF. Posttraumatic stress symptoms and health-related quality of life: a two year follow up study of injury treated at the emergency department. BMC Psychiatry. 2012;12(1):1. doi:10.1186/1471-244X-12-1
14. Hourani L, Williams J, Bray RM, Wilk JE, Hoge CW. Gender differences in posttraumatic stress disorder and help seeking in the U.S. army. J Womens Health. 2016;25(1):22–31. doi:10.1089/jwh.2014.5078
15. Qi W, Gevonden M, Shalev A. Prevention of post-traumatic stress disorder after trauma: current evidence and future directions. Curr Psychiatry Rep. 2016;18(2):20. doi:10.1007/s11920-015-0655-0
16. Saberi HR, Abbasian H, Kashani MM, Esfahani AH. Post-traumatic stress disorder: a neglected health concern among commercial motor vehicle drivers. Int J Occup Environ Med. 2013;4(4):185–194.
17. Kim SE, Kim HR, Park JI, et al. The association between psychiatric disorders and work-related problems among subway drivers in Korea. Ann Occup Environ Med. 2014;26(1):39. doi:10.1186/s40557-014-0039-7
18. Bleich A, Gelkopf M, Solomon Z. Exposure to terrorism, stress-related mental health symptoms, and coping behaviors among a nationally representative sample in Israel. JAMA. 2003;290(5):612–620. doi:10.1001/jama.290.5.612
19. Scott KM, Koenen KC, King A, et al. Post-traumatic stress disorder associated with sexual assault among women in the WHO World Mental Health Surveys. Psychol Med. 2018;48(1):155–167. doi:10.1017/S0033291717001593
20. Lopez AD, Murray CC. The Global Burden of Disease, 1990–2020. Nat Med. 1998;4(11):1241–1243.
21. Akinyemi OO, Owoaje ET, Ige OK, Popoola OA. Comparative study of mental health and quality of life in long-term refugees and host populations in Oru-Ijebu, Southwest Nigeria. BMC Res Notes. 2012;5(1):394. doi:10.1186/1756-0500-5-394
22. Beck JG, Coffey SF. Assessment and treatment of PTSD after a motor vehicle collision: empirical findings and clinical observations. Prof Psychol Res Pr. 2007;38(6):629–639. doi:10.1037/0735-7028.38.6.629
23. Liu H, Petukhova MV, Sampson NA, et al. Association of DSM-IV posttraumatic stress disorder with traumatic experience type and history in the World Health Organization World Mental Health Surveys. JAMA psychiatry. 2017;74(3):270–281. doi:10.1001/jamapsychiatry.2016.3783
24. Bedaso A, Kediro G, Ebrahim J, et al. Prevalence and determinants of post-traumatic stress disorder among road traffic accident survivors: a prospective survey at selected hospitals in southern Ethiopia. BMC Emerg Med. 2020;20(1):52. doi:10.1186/s12873-020-00348-5
25. Yohannes K, Gebeyehu A, Adera T, Ayano G, Fekadu W. Prevalence and correlates of post-traumatic stress disorder among survivors of road traffic accidents in Ethiopia. Int J Ment Health Syst. 2018;12(1):50. doi:10.1186/s13033-018-0229-8
26. Asnakew S, Shumet S, Ginbare W, Legas G, Haile K. Prevalence of post-traumatic stress disorder and associated factors among Koshe landslide survivors, Addis Ababa, Ethiopia: a community-based, cross-sectional study. BMJ Open. 2019;9(6):e028550. doi:10.1136/bmjopen-2018-028550
27. Fekadu W, Mekonen T, Belete H, Belete A, Yohannes K. Incidence of post-traumatic stress disorder after road traffic accident. Front Psychiatry. 2019;10:519. doi:10.3389/fpsyt.2019.00519
28. Ongecha-Owuor FA, Kathuku DM, Othieno CJ, Ndetei DM. Post traumatic stress disorder among motor vehicle accident survivors attending the orthopaedic and trauma clinic at Kenyatta National Hospital, Nairobi. East Afr Med J. 2004;81(7):362–366. doi:10.4314/eamj.v81i7.9192
29. Guest R, Tran Y, Gopinath B, Cameron ID, Craig A. Prevalence and psychometric screening for the detection of major depressive disorder and post-traumatic stress disorder in adults injured in a motor vehicle crash who are engaged in compensation. BMC Psychol. 2018;6(1):4. doi:10.1186/s40359-018-0216-5
30. Sadat Z, Abdi M, Aghajani M. Prevalence of posttraumatic stress disorder and related factors among patients discharged from critical care units in Kashan, Iran. Arch Trauma Res. 2015;4(4):e28466. doi:10.5812/atr.28466
31. Kenardy J, Edmed SL, Shourie S, et al. Changing patterns in the prevalence of posttraumatic stress disorder, major depressive episode and generalized anxiety disorder over 24 months following a road traffic crash: results from the UQ SuPPORT study. J Affect Disord. 2018;236:172–179. doi:10.1016/j.jad.2018.04.090
32. Keane TM, Marshall AD, Taft CT. Posttraumatic stress disorder: etiology, epidemiology, and treatment outcome. Annu Rev Clin Psychol. 2006;2(1):161–197. doi:10.1146/annurev.clinpsy.2.022305.095305
33. Watson P. PTSD as a public mental health priority. Curr Psychiatry Rep. 2019;21(7):61. doi:10.1007/s11920-019-1032-1
34. Sekoni O, Mall S, Christofides N. Prevalence and factors associated with PTSD among female urban slum dwellers in Ibadan, Nigeria: a cross-sectional study. BMC Public Health. 2021;21(1):1546. doi:10.1186/s12889-021-11508-y
35. Auxéméry Y. [Posttraumatic stress disorder (PTSD) as a consequence of the interaction between an individual genetic susceptibility, a traumatogenic event and a social context]. L’Encephale. 2012;38(5):373–380. French. doi:10.1016/j.encep.2011.12.003
36. Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: a meta-analysis. Psychol Bull. 2003;129(1):52–73. doi:10.1037/0033-2909.129.1.52
37. d’Ettorre G, Ceccarelli G, Santinelli L, et al. Post-traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: a systematic review. Int J Environ Res Public Health. 2021;18(2):601. doi:10.3390/ijerph18020601
38. Tirone V, Orlowska D, Lofgreen AM, et al. The association between social support and posttraumatic stress symptoms among survivors of betrayal trauma: a meta-analysis. Eur J Psychotraumatol. 2021;12(1):1883925. doi:10.1080/20008198.2021.1883925
39. Yao S-N, Cottraux J, Note I, Mey-Guillard D, Mollard E, Ventureyra V. Évaluation des états de stress post-traumatique: validation d’une échelle, la PCLS. L’Encephale. 2003;29(3 Pt 1):232–238.
40. Alenko A, Berhanu H, Abera Tareke A, et al. Posttraumatic stress disorder and associated factors among drivers surviving road traffic crashes in Southwest Ethiopia. Neuropsychiatr Dis Treat. 2019;15:3501–3509. doi:10.2147/NDT.S233976
41. Stein DJ, Karam EG, Shahly V, et al. Post-traumatic stress disorder associated with life-threatening motor vehicle collisions in the WHO World Mental Health Surveys. BMC Psychiatry. 2016;16(1):257. doi:10.1186/s12888-016-0957-8
42. Kovacevic J, Miskulin M, Degmecic D, et al. Predictors of mental health outcomes in road traffic accident survivors. J Clin Med. 2020;9(2):309. doi:10.3390/jcm9020309
43. Arora D, Belsiyal CX, Rawat VS. Prevalence and determinants of posttraumatic stress disorder and depression among survivors of motor vehicle accidents from a hilly Indian state. Indian J Psychiatry. 2021;63(3):250–257. doi:10.4103/psychiatry.IndianJPsychiatry_1059_20
44. Wang CH, Tsay SL, Bond AE. Post-traumatic stress disorder, depression, anxiety and quality of life in patients with traffic-related injuries. J Adv Nurs. 2005;52(1):22–30. doi:10.1111/j.1365-2648.2005.03560.x
45. Kovacevic J, Fotez I, Miskulin I, et al. Different patterns of mental health outcomes among road traffic crash survivors: a prospective cohort study. Int J Environ Res Public Health. 2021;18(4):1564. doi:10.3390/ijerph18041564
46. Lin W, Gong L, Xia M, Dai W. Prevalence of posttraumatic stress disorder among road traffic accident survivors: a PRISMA-compliant meta-analysis. Medicine. 2018;97(3):e9693. doi:10.1097/MD.0000000000009693
47. Dückers ML, Alisic E, Brewin CR. A vulnerability paradox in the cross-national prevalence of post-traumatic stress disorder. Br J Psychiatry. 2016;209(4):300–305. doi:10.1192/bjp.bp.115.176628
48. Creamer M, Burgess P, McFarlane AC. Post-traumatic stress disorder: findings from the Australian national survey of mental health and well-being. Psychol Med. 2001;31(7):1237–1247. doi:10.1017/S0033291701004287
49. Muldoon OT. Perceptions of stressful life events in Northern Irish school children: a longitudinal study. J Child Psychol Psychiatry. 2003;44(2):193–201. doi:10.1111/1469-7610.00113
50. Dai W, Kaminga AC, Tan H, et al. Long-term psychological outcomes of flood survivors of hard-hit areas of the 1998 Dongting Lake flood in China: prevalence and risk factors. PLoS One. 2017;12(2):e0171557. doi:10.1371/journal.pone.0171557
51. Dai W, Wang J, Kaminga AC, et al. Predictors of recovery from post-traumatic stress disorder after the dongting lake flood in China: a 13–14 year follow-up study. BMC Psychiatry. 2016;16(1):382. doi:10.1186/s12888-016-1097-x
52. Coronas R, García-Parés G, Viladrich C, Santos JM, Menchón JM. Clinical and sociodemographic variables associated with the onset of posttraumatic stress disorder in road traffic accidents. Depress Anxiety. 2008;25(5):E16–23. doi:10.1002/da.20324
53. Rivière S, Schwoebel V, Lapierre-Duval K, Guinard A, Gardette V, Lang T. Predictors of symptoms of post-traumatic stress disorder after the AZF chemical factory explosion on 21 September 2001, in Toulouse, France. J Epidemiol Community Health. 2008;62(5):455–460. doi:10.1136/jech.2006.057273
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.