")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Prevalence and Risk Factors of Diabetic Nephropathy Among Saudi Type-1 Diabetic Patients in Taif City, Saudi Arabia
Authors Al-Zahrani N , AlSwat HK, AlQarni AM , Alzahrani SS , Boubshait LA, Alassaf LA , Alsalman Z
Received 25 August 2023
Accepted for publication 26 October 2023
Published 9 November 2023 Volume 2023:16 Pages 3609—3616
DOI https://doi.org/10.2147/DMSO.S432700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Antonio Brunetti
Noura Al-Zahrani,1 Hameed Khoshaiban AlSwat,2 Amani M AlQarni,3 Saleh Sadan Alzahrani,4 Leila A Boubshait,5 Lujain A Alassaf,6 Zaenb Alsalman7
1Department of Medicine, Hera General Hospital, Ministry of Health, Makkah, Saudi Arabia; 2Pediatric Endocrinologist, Endocrine Diabetic Center, King Abdulaziz Specialist Hospital, Taif, Saudi Arabia; 3Family and Community medicine department, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 4Medical Intern, Ibn Sina National College, Jeddah, Saudi Arabia; 5Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 6Clinical Insights, Clinical Excellence, Saudi Center for National Health Insurance, Riyadh, Saudi Arabia; 7Department of Family and Community Medicine, College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia
Correspondence: Amani M AlQarni, Family and community medicine department, King Fahd Hospital of the University, Imam Abdulrahman bin Faisal University, Dammam, 34212, Saudi Arabia, Tel +966133333766 ; +966 59 177 5751, Email [email protected]
Purpose: We investigated the prevalence and associated risk factors of DNP in T1DM patients in Taif city, Saudi Arabia, where the renal diseases are prevalent. The incidence of diabetic nephropathy (DNP) is increasing in Saudi Arabia, and the country is also ranked 4th in terms of the number of diagnosed type-1 diabetes (T1DM) patients.
Patients and Methods: The retrospective cohort study was conducted with type-1 diabetes patients registered at King Abdulaziz Specialist Hospital in Taif, Saudi Arabia. A total of 198 patients (aged > 18 years), had T1DM for more than 5 years with documented albuminuria; albumin-creatinine ratio (ACR) ≥ 30 mg/g creatinine in two of three urine samples or estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2, were included in the study. Patients’ demographic and laboratory data were collected from medical records. A regression analysis model was used to identify risk factors for DNP. Statistical significance was set at P < 0.05.
Results: The overall prevalence of DNP was 23.7% in our study group, with 8% having low eGFR alone, 20.71% having positive ACR and 6.22% having both positive ACR and low eGFR. A statistically significant correlation between DNP and risk factors was found for uncontrolled and longer duration of T1DM, elevated ACR, and hypertension (P < 0.05). No statistical significance was found for age, sex, or body mass index (BMI).
Conclusion: The prevalence of DNP in T1DM patients in Taif city was higher (23.7%) than the pooled average prevalence in Saudi Arabia (20.59%). Patients’ education regarding glycemic and blood pressure control could reduce the burden.
Keywords: type-1 diabetes mellitus, diabetic nephropathy, renal diseases, risk factors, prevalence, Saudi Arabia
Introduction
Diabetes Mellitus type-1 (T1DM) is a serious chronic health condition worldwide, with increasing pervasiveness seen in children and in youth.1 It is defined as an autoimmune disease that targets pancreatic β-cells and causes a permanent absolute insulin deficit.2,3 Globally, the burden of T1DM is vast. In 2021, approximately 8 million people worldwide had T1DM; 18% of them were in age group under 20, 64% were ages 20–59 and 19% were at age 60 or above. It is predicted to increase in prevalence by 60–107% from 2021 to 2040.2,4
Saudi Arabia is ranked as the 8th country among top ten countries in the world with high incidence rates of T1DM in youth and children and 4th country in terms of the number of diagnosed diabetic patients.5
T1DM is usually associated with poor quality of life, serious long-term sequelae, and a shorter life span.2,3 The predominant complication of T1DM is diabetic kidney disease (DKD),5 which can progress to chronic kidney disease (CKD), End-Stage Renal Disease (ESRD), and cardiovascular events.3,6 The clinical diagnosis of DKD begins when a patient has albuminuria, a reduced estimated glomerular filtration rate (eGFR), or both.
As the course of DKD in people with T1DM is unpredictable, it is important to identify its risk factors.7 Poor glycemic control being the primary cause in the development of diabetic nephropathy.6 Other variables include retinopathy, dyslipidemia, hypertension, and male sex have been linked to the development of DKD in T1DM patients.7
Although, both types of diabetes can cause nephropathy, only a small percentage of those with type-2 diabetes develop ESKD.7 As excess protein in the urine is seen in T1DM patients more frequently (15–40%) as compared to T2DM patients.8,9
Diabetes accounts for 44% to 45% of incidence instances of ESKD in the US, making it one of the highest rates in the world.9 Internationally, there is a lot of variation between nations, with incidence rates ranging from 9% in Russia to 49% in Malaysia.9,10 An increased T1DM burden is also seen in other Arab countries, but only few attempts were made to study the disease prevalence, its causes and complications.11,12
Saudi Arabia is among the top ten countries with an increasing incidence of diabetic nephropathy.13,14 A higher frequency of albuminuria is seen in Saudi women.15 Studies revealed that DKD will progress to ESRD in one out of every five Saudi diabetic patients with the females at higher risk than males.16 One study shows that there was 25.1% increase in the CKDs within a span of 10 years in the Kingdom.17
In view of this rapid rise in the burden of diabetes and its comorbidities in the Kingdom, the Ministry of Health (MOH) in Saudi Arabia had approved a “ten-year National Executive Plan” for the control of diabetes.18 The plan included treatment strategies, prevention, and control awareness programs.18
Taif is one of the regions in Saudi Arabia where renal diseases and its risk factors are more prevalent.19,20 In addition, knowledge and awareness regarding CKD and its risk factors are very poor among the general public in the city.19
As T1DM is one of the leading causes of CKDs and a serious health issue in Saudi Arabia,21 we devised the present study to evaluate the prevalence of DKD and its associated risk factors in registered patients with T1DM at King Abdulaziz Specialist Hospital (KASH) in Taif, Saudi Arabia.
This is the first study to address renal complications in type-1 diabetes in one of the regions of Saudi Arabia. This effort may be helpful in providing useful insights to deduce an action plan to recognize the risk factors for DKD and further promote awareness programs in different regions of the country.
Materials and Methods
This was an observational, retrospective cohort study of T1DM patients at KASH in Taif, Saudi Arabia. The number of study participants was evaluated using 16% prevalence of microalbuminuria in Saudi T1DM patients in Jeddah and the total registered T1DM patients at KASH (400 patients).22 An estimated sample size was calculated as 151 patients using Rao soft calculator, with 80% analytical power, 95% confidence level, and 5% margin of error. Patients’ demographic, clinical, and laboratory data were collected from their medical records. The data included patients’ age, gender, BMI, eGFR, ACR, A1C, BP, lipid profile etc.
The prevalence of DKD was calculated based on the American Diabetes Association (ADA) criteria, which uses albuminuria as a urine albumin-creatinine ratio (UACR) ≥30 mg/g creatinine in two of three specimens collected within a 3- to 6-month period, or eGFR <60 mL/min/1.73 m2.23 Also, we referred to some studies that used the same cut-off for eGFR as an indicator of kidney disease.24,25
Exclusion criteria included patients under the age of 18 years, those who had diabetes other than T1DM, those who had T1DM for less than 5 years, or those who did not have two documented urine samples for ACR.
This study was approved by the Directorate of Health Affairs-Taif’s ethics committee and is following the declaration of Helsinki.
The most recent A1C values were obtained from patient records. Then, the patients were classified according to ADA guidelines, which consider A1C <7.0% to be the level for optimal control. A1C level greater than 9.0% indicates poor control of diabetes.23
Regarding lipid profiles, patients were classified based on the following measures: total cholesterol (normal = <200 mg/dL, borderline high = 200–239 mg/dL, high = ≥240 mg/dL), LDL cholesterol (optimal = <100 mg/dL, near optimal = 100–129 mg/dL, borderline high = 139–159 mg/dL, high = ≥160 mg/dL), and triglycerides (normal = <150 mg/dL, borderline high = 150–199 mg/dL, high = ≥200 mg/dL).24 Patients’ Body Mass Index (BMI) was recorded using the formula = weight in kilograms divided by the square of height in meters and categorized according to the United States Centers for Disease Control and Prevention (CDC) (Underweight = BMI less than 18.5; normal weight, BMI 18.5 to <25; Overweight = BMI 25.0 to <30; and obese, BMI = ≥30.0).25
Blood pressure reading was obtained from the medical record, and patients with average SBP ≥140 mm Hg were defined to have high systolic blood pressure, and those with average DBP ≥90 mm Hg were defined to have high diastolic blood pressure.26
Data Analysis
Data analysis was performed using the “Statistical Package for the Social Sciences” (SPSS) version 23, and descriptive analysis was performed using frequencies, percentages, means, and standard deviations. Furthermore, a regression analysis model was used to identify risk factors for DKD. Statistical significance was set at P < 0.05.
Results
Table 1 presents the demographic and laboratory data of the number (N) of the study participants. The study included 198 participants. The mean age of the study population was 26.863±8.15. Most of them were females (59%) in which nearly half (48%) were overweight or obese. The average duration of diabetes in the sample was approximately 11 and a half years. With regard to cholesterol levels, more than half of our population was found to have “above optimal” or “borderline high” LDL (low-density lipoprotein), and the average cholesterol level was found to be 182.44 mg/dL.
 |
Table 1 Participants’ Demographic and Laboratory Data (N = 198) |
The prevalence of DKD was determined to be 23.7% in the sample, with 8% having low eGFR alone, 20.71% having positive ACR, and 6.22% having both positive ACR and low eGFR.
Regression Analysis of Risk Factors
The variables used as risk factors in our study were age, duration of diabetes, body mass index (BMI), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, systolic blood pressure (SBP), diastolic blood pressure, A1C (glycated hemoglobin), albumin-creatinine ratio (ACR), and sex.
Risk Factors of Low eGFR
Table 2 shows the regression analysis of the variables associated with eGFR. In the univariate model, the risk of DKD increased 1.014 times per each unit increase in LDL (OR = 1.014; 95% CI: 1.001–1.028; p = 0.032). Furthermore, the duration of type-1 diabetes and ACR were significantly associated with an increased risk of DKD (p < 0.05). In the multivariate model, after adjustment for significant covariates, LDL was no longer significant (p = 0.066), but T1DM duration and ACR remained significantly associated. It is worth mentioning that for each additional year of living with diabetes, the risk of developing DKD increased by approximately 1.1 times (OR = 1.122; 95% CI: (1.041–1.210); p = 0.003).
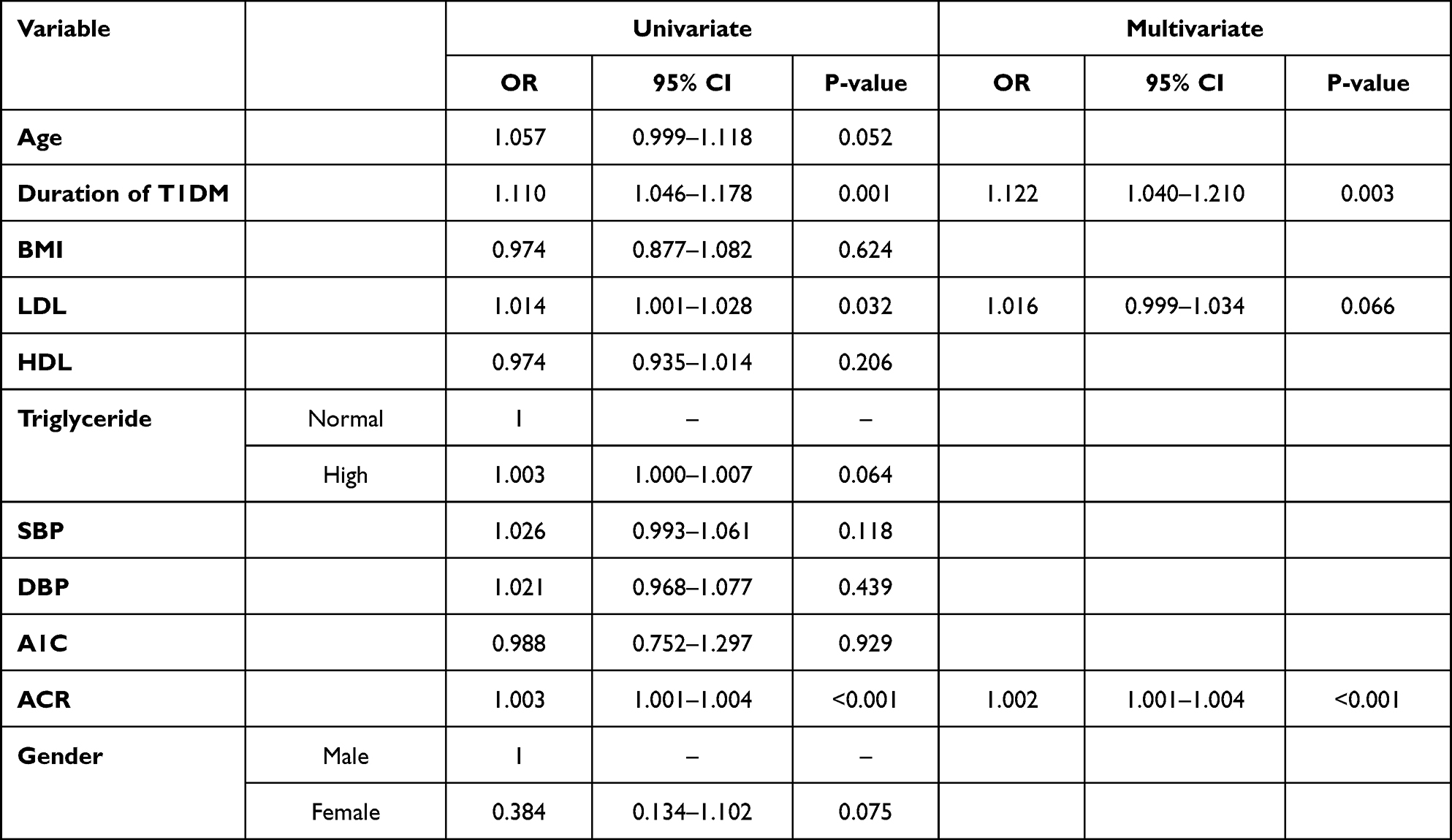 |
Table 2 Regression Analysis for Risk Factors of Low eGFR |
Risk Factors of Elevated ACR
ACR was used as an indicator of kidney disease (Table 3). In the univariate model, sex, duration of diabetes, LDL, triglycerides, systolic blood pressure (SBP), diastolic blood pressure (DBP), and A1C were all associated with DKD (p < 0.05). However, after adjusting for potential confounders in the multivariate model, only systolic blood pressure, eGFR and A1C remained significantly associated with DKD.
 |
Table 3 Regression Analysis for Risk Factors of ACR |
The risk of DKD would increase by 1.046 times for every millimeter increase in SBP (OR = 1.046; 95% CI: 1.007–1.086; p = 0.019).
Moreover, in our study group, the patients with elevated levels of A1C showed a substantially increased risk of developing DKD (OR = 1.323; 95% CI: 1.073–1.633 p = 0.009). Additionally, eGFR <60 was significantly associated with a lower risk of DKD (OR = 0.977; 95% CI: 0.959–0.995, p = 0.011).
Risk Factors of Both Elevated ACR and Low eGFR
Finally, the risk of DKD was tested using both ACR and eGFR as indicators (Table 4). After adjusting for significant variables in the multivariate model, duration of diabetes, high triglyceride levels, and systolic blood pressure were significantly associated with our main outcome variables. For each year increase in diabetes and for each unit increase in the T1DM duration, triglyceride level, and systolic blood pressure, the risk of DKD would increase by slightly over 1 (OR = 1.205, 95% CI: 1.085–1.338, p = 0.001), (OR = 1.012, 95% CI: 1.004–1.019, p = 0.002), and (OR = 1.066, 95% CI: 1.003–1.132, p = 0.039), respectively.
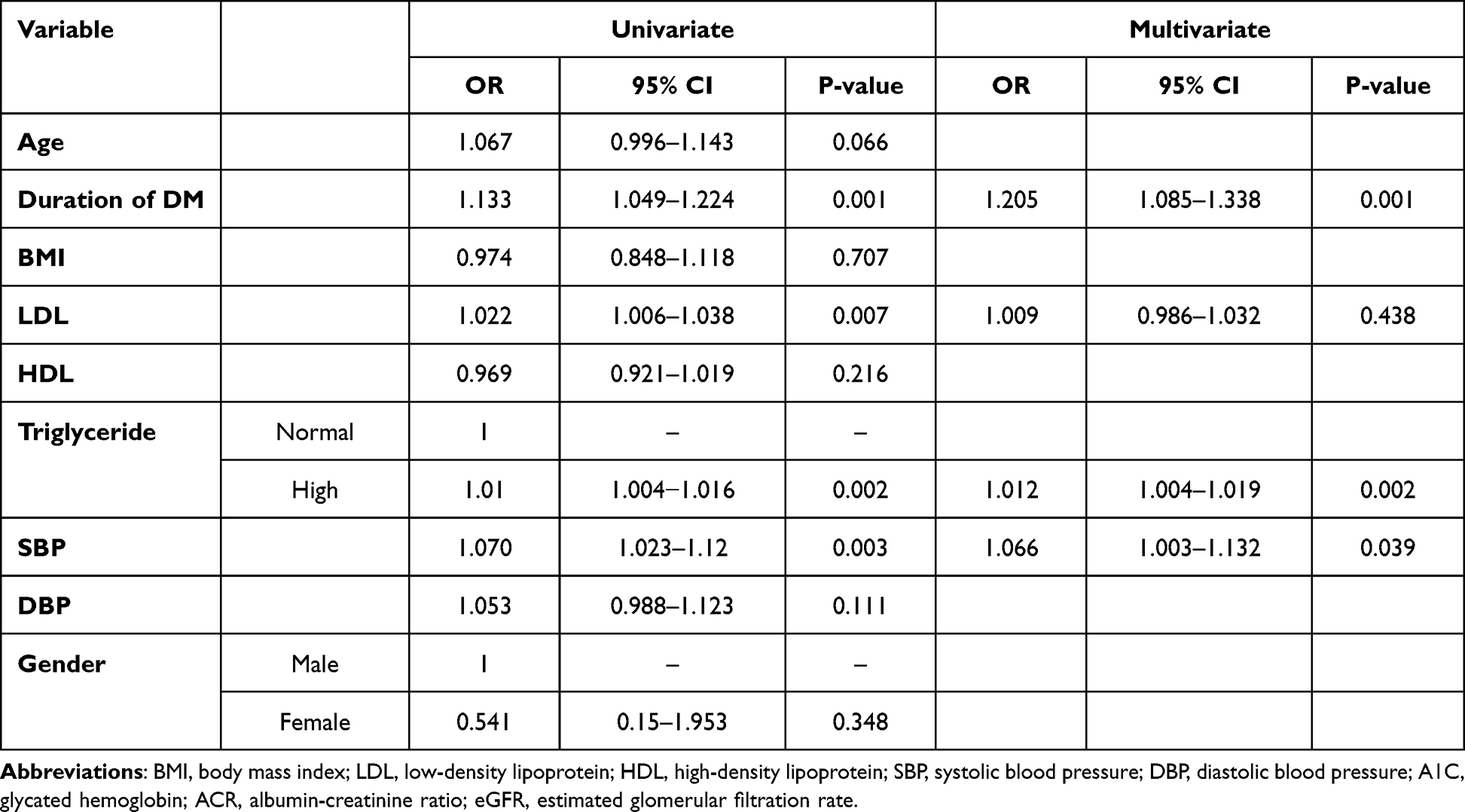 |
Table 4 Regression Analysis for Risk Factors of Both ACR and eGFR |
Discussion
Based on these results, the overall prevalence of DKD was found to be 23.7% in our study group, with 8% having low eGFR alone (<60 mL/min/1.73), 20.71% having positive ACR, and 6.22% having both positive ACR and low eGFR. Although this is regarded as a high prevalence, it is still lower than in other populations, as reported by various studies, such as 50.46% in Oman among Middle Eastern countries, 33% in Yemen,11,27 28.96% (collective average prevalence) in Middle Eastern countries,11 27% in China,13 25% in Republic of Ireland,28 69% in Hail Saudi Arabia,29 and highest in Tanzania (84%).13 The overall collective average prevalence of CKD in diabetic patients in Saudi Arabia was found to be 20.59%.11 Among racial differences, Asian Americans, African Americans and native Americans with type 1 diabetes were found to be more susceptible in developing DN that may progress to more severe complications of DN.30
Notably, the data source is an important factor that may contribute to discrepancies in the results of studies conducted on prevalence. For example, a meta-analysis of the prevalence of CKD in Middle East showed wide variations ranging from 37.32% (95% CI: 32.57–51.07%) to 31.76% (95% CI: 17.27–46.25%) and (21.75%) (95% CI: 1.51–42.0%) in studies using medical files, self-reporting questionnaires, and electronic medical records, respectively.11
With regard to sex, we found no significant sex differences in our study in relation to disease duration or risk factors, although some of the studies reported the DKD prevalence by sex.31 One of the studies reported that male sex is an independent risk factor for DKD and males have 50% higher chance of progression of disease to ESRD as compared to females.32 This can be explained by the absence of hormones estrogen and progesterone, which have a protective effect on kidneys.31 In contrast, high prevalence of DKD in women is supported by some studies, predominantly in DM women of advanced age (>60 years) and non-albuminuric phenotype.15,31
Similarly, no significant difference was found with age in our study groups in relation to risk factors; however, some studies reported the high prevalence of DN in old age33 and children under 12 years of age.34
Furthermore, examining the effect of risk factors on GFR, a longer duration of diabetes and elevated ACR were significantly associated with lower GFR.
Similarly, ACR was most affected by high blood pressure, high A1C and low GFR, and triglycerides in our study group. Among all risk factors, high Hb1Ac was reported as a major contributor of nephropathy in both children and adults with type-1 diabetes33,35 and our results are consistent with these studies.
In summary, the most prominent risk factors identified in our study for the development of DKD in T1DM patients were prolonged and poorly controlled diabetes, poorly uncontrolled blood pressure, and high triglyceride levels. Prolonged and poorly controlled diabetes causes thickening of the glomerular basal membrane and multiplication of mesangial cells, which ultimately results in glomerular damage and albuminuria usually within ten years of the onset of diabetes, with or without hypertension.9 Similarly, increased systolic blood pressure (SBP) also affects GFR and finally causes albuminuria.30
To emphasize, longer duration of diabetes is the most common etiology of CKD in DM patients.34 Our results are also consistent with these findings and can be observed by the low eGFR and elevated A1C levels in our study group.
Conclusion
In the present study, we found a high prevalence of diabetic nephropathy among registered patients with T1DM at King Abdulaziz Specialist Hospital (KASH) in Taif city, Saudi Arabia, compared with the overall prevalence of diabetic kidney disease in the Kingdom.
To the best of our knowledge, this is the first study to address renal complications associated with type-1 diabetes in one region of Saudi Arabia.
As T1DM is a growing problem in Saudi Arabia, further research is needed in other regions of the country to focus on its complications and risk factors.
In this regard, it is important to pay closer attention to hypertension with high A1C levels, as such patients are at a higher risk of developing diabetic kidney diseases and have more chances of progression to chronic kidney disease and end-stage renal disease. Therefore, attempts should be made to control blood pressure and glycemic control to prevent and reduce the risk of complications. This can be achieved by managing modifiable risk factors such as diet, physical activity, compliance with therapeutic plans, strict monitoring and follow-up.
Healthcare providers, awareness programs, and government infrastructure can play a vital role in this regard.
Finally, we propose our future research that may examine DKD with metabolic syndrome, as its prevalence is also high in DM1, chronic inflammation, and low vitamin D levels.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chiang JL, Maahs DM, Garvvey KC, et al. Type 1 diabetes in children and adolescents: a position statement by the American Diabetes Association. Diabetes Care. 2018;41(9):2026–2044. doi:10.2337/dci18-0023
2. Gregory GA, Robinson TIG, Linklater SE, et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022;10(10):741–760. doi:10.1016/S2213-8587(22)00218-2
3. Mottl AK, Tuttle KR, Bakris GL Diabetic Kidney Dis. Waltham MA: UpToDate Inc. Available from: http://www.uptodate.com.
4. Ogle GD, James S, Dabelea D, et al. Global estimates of incidence of type 1 diabetes in children and adolescents: results from the international diabetes federation atlas, 10th edition. Diabetes Res Clin Pract. 2022;183:109083. doi:10.1016/j.diabres.2021.109083
5. Costacou T, Orchard TJ. Cumulative kidney complication risk by 50 years of type 1 diabetes: the effects of sex, age, and calendar year at onset. Diabetes Care. 2018;41(3):426–433. doi:10.2337/dc17-1118
6. Orchard TJ. Cardiovascular disease in type 1 diabetes: a continuing challenge. Lancet Diabetes Endocrinol. 2021;9(9):548–549. doi:10.1016/S2213-8587(21)00190-X
7. Perkins BA, Bebu I, de Boer IH, et al. Risk factors for kidney disease in type-1 diabetes. Diabetes Care. 2019;42(5):883–890. doi:10.2337/dc18-2062
8. Roy S, Kahn OS, Jafry B, et al. Risk factors and comorbidities associated with diabetic kidney disease. J Prim Care Community Health. 2021;12:1–10. doi:10.1177/21501327211048556
9. Gheith O, Farouk N, Nampoory N, Halim MA, Al-Otaibi T. Diabetic kidney disease: world-wide difference of prevalence and risk factors. J Nephropharmacol. 2016;5(1):49.
10. Selby NM, Taal MW. An updated overview of diabetic nephropathy: diagnosis, prognosis, treatment goals and latest guidelines. Diabetes Obes Metab. 2020;1(S1):3–15. doi:10.1111/dom.14007
11. Naser AY, Alwafi H, Alotaibi B, et al. Prevalence of chronic kidney diseases in patients with diabetes mellitus in the middle east: a systematic review and meta-analysis. Int J Endocrinol. 2021;2021:4572743. doi:10.1155/2021/4572743
12. Abdel-Motal UM, Akila G, Abdelalim EM, et al. Prevalence of nephropathy in type-1 diabetes in the Arab world: a systematic review and meta-analysis. Diabetes Metab Res Rev. 2018;34(7):e3026. doi:10.1002/dmrr.3026
13. Hoogveen EK. The epidemiology of diabetic kidney disease. Kidney Dial. 2022;2(3):433. doi:10.3390/kidneydial2030038
14. Al-Rubeaan K, Siddiqui K, Alghonaim M, Youssef AM, AlNaqeb D. The Saudi Diabetic Kidney disease (Saudi DKD): clinical characteristics and biochemical parameters. Ann Saudi Med. 2018;38(1):46. doi:10.5144/0256-4947.2018.03.01.1010
15. Siddiqui K, Joy SS. Risk factors and management of kidney diseases in Saudi women with diabetes. Curr Womens Health Rev. 2020;16(2):95–101. doi:10.2174/1573404816666200206110002
16. Ahmed HG, Alzayed FSM, Albluwe HKA, et al. Etiology of chronic kidney disease (CKD) in Saudi Arabia. Int J Med Res Health. 2019;8(5):177–182.
17. Top 10 causes of death by rate in 2015. Institute for Health Metrics and Evaluation. Saudi Arabia; 2018. Available from: https://www.healthdata.org/saudi-arabia.
18. Press Report on the MOH’s Efforts Regarding Raising People’s Awareness of Diabetes. MOH Publication; 2013. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/Publications-2013-06-09-004.aspx.
19. Sultana S, Alquraishi R, Alqarni T, Alnefaie M, Kalakattawi A, Alzahrani R. Risk factors and knowledge assessment of general public for chronic kidney disease in Taif Region, Saudi Arabia. World J Adv Res Rev. 2020;8(1):123–143. doi:10.30574/wjarr.2020.8.1.0373
20. Kajoak S, Bushra W, Elnour H, et al. Study of renal disease during computed tomography in Taif, Saudi Arabia. Med Sci. 2023;27(132):1–9. doi:10.54905/disssi/v27i132/e94ms2823
21. Robert AA, Al-Dawish A, Mujammami M, Al Dawish MA. Type 1 diabetes mellitus in Saudi Arabia: a soaring epidemic. Int J Ped. 2018;9408370. doi:10.1155/2018/9408370
22. Al-Agha AE, Alafif M, Abd-Elhameed IA. Glycemic control, complications and associated diseases in Jeddah Saudi Arabia. Saudi Med J. 2015;36(1):26–31. doi:10.15537/smj.2015.1.9829
23. de Boer IH, Khunti K, Sadusky T, et al. Diabetic management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and kidney disease: improving global outcomes (KIDGO). Diabetes Care. 2022;45(12):3075–3090. doi:10.2337/dci22-0027
24. Nazzal Z, Hamdan Z, Masri D, Abu-Kaf O, Hamad M. Prevalence and risk factors of chronic kidney disease among Palestinian type 2 diabetic patients: a cross-sectional study. BMC Nephrol. 2020;21(1):1–8. doi:10.1186/s12882-020-02138-4
25. Cirillo M, Lombardi C, Chiricone D, Bilancio G, Marcarelli F, De Santo NG. Early identification of kidney disease by eGFR: what is the prevalence of eGFR in the population? J Nephrol. 2008;21:S102–6.
26. James PA, Oparil S, Carter BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
27. Bamashmoos MA, Ganem Y. Diabetic nephropathy and its risk factors in type 2-diabetic patients in Sana’a City, Yemen. World J Med Sci. 2013;9(3):147–152.
28. Majeed MS, Ahmed F, Teeling M. The prevalence of chronic kidney disease and albuminuria in patients with type-1 and type-2 diabetes attending a single centre. Cureus. 2022;14(12):e32248. doi:10.7759/cureus.32248
29. Alghaythi AM, Alsudayri MST, Alshammari F, et al. Prevalence of diabetes among patients with chronic kidney disease in Hail Region. Egypt J Hospital Med. 2018;71(2):2434–2442. doi:10.12816/0045638
30. Giandalia A, Giuffrida AE, Gembillo G, et al. Gender differences in diabetic kidney disease: focus on hormonal, genetic and clinical factors. Int J Mol Sci. 2021;22(11):5808. doi:10.3390/ijms22115808
31. Carrero JJ, Hecking M, Chesnaye NC, Jager KJ. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat Rev Nephrol. 2018;14(3):151–164. doi:10.1038/nrneph.2017.181
32. Damtie S, Biadgo B, Baynes HW, et al. chronic kidney disease and associated risk factors assessment among diabetes mellitus patients at a tertiary hospital, Northwest Ethiopia. Ethiop J Health Sci. 2018;28(6):691–700. doi:10.4314/ejhs.v28i6.3
33. Ahmed H, Elshaikh T, Abdullah M, Wallner M. Early diabetic nephropathy and retinopathy in patients with type 1 diabetes mellitus attending Sudan childhood diabetes centre. J Diabetes Res. 2020;2020:718138. doi:10.1155/2020/7181383
34. Lind M, Pivodic A, Svensson AM, Ólafsdóttir AF, Wedel H, Ludvigsson J. HbA1c level as a risk factor for retinopathy and nephropathy in children and adults with type 1 diabetes: Swedish population- based cohort study. BMJ. 2019;366:l4894. doi:10.1136/bmj.l4894
35. Ku E, McCulloch CE, Mauer M, Gitelman SE, Grimes BA, Hsu CY. Association between blood pressure and adverse renal events in type-1 diabetes. Diabetes Care. 2016;39(12):2218–2224. doi:10.2337/dc16-0857
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.