")
Back to Journals » Nature and Science of Sleep » Volume 13
Prevalence and Risk Factors Associated with Insomnia Symptoms Among the Chinese General Public After the Coronavirus Disease 2019 Epidemic Was Initially Controlled
Authors Guo J, Yang L , Xu Y, Zhang C, Luo X, Liu S, Yao L, Bai H, Zong X, Zhang J, Liu Z, Zhang B
Received 23 February 2021
Accepted for publication 12 May 2021
Published 1 June 2021 Volume 2021:13 Pages 703—712
DOI https://doi.org/10.2147/NSS.S307996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Junlong Guo, 1, 2 Lulu Yang, 1, 2 Yan Xu, 1, 2 Chenxi Zhang, 1, 2 Xian Luo, 1, 2 Shuai Liu, 1– 3 Lihua Yao, 4 Hanping Bai, 4 Xiaofen Zong, 4 Jihui Zhang, 5 Zhongchun Liu, 4 Bin Zhang 1, 2
1Department of Psychiatry, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Guangdong Mental Health Center, Guangdong Provincial People’s Hospital, Guangzhou, People’s Republic of China; 3Department of Psychiatry, The Third People’s Hospital of Qinghai Province, Xining, People’s Republic of China; 4Department of Psychiatry, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 5Guangdong-Hong Kong-Macao Greater Bay Area Center for Brain Science and Brain-Inspired Intelligence, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Bin Zhang
Department of Psychiatry, Nanfang Hospital, Southern Medical University, 1838 Guangzhou Avenue North, Guangzhou, 510515, People’s Republic of China
Tel +86-20-62786731
Email [email protected]
Zhongchun Liu
Department of Psychiatry, Renmin Hospital of Wuhan University, 238 Jiefang Road, Wuhan, 430060, People’s Republic of China
Email [email protected]
Introduction: The prevalence rate and related factors of insomnia remained unknown after the COVID-19 epidemic had been under control. Therefore, we conducted this survey to investigate the prevalence rate and related factors of insomnia symptoms in the Chinese general public after the COVID-19 had been initially control.
Methods: An online survey was conducted among Chinese citizens through the JD Health APP. The questionnaire was used for collecting demographic data and self-designed questions related to the COVID-19 outbreak. Insomnia Severity Index, Patient Health Questionnaire-9, Somatic Symptom Scale-8 and Impact of Events Scale-Revised were used for measuring psychological symptoms. To examine the associations of sociodemographic and psychological factors with insomnia symptoms, a binary logistic regression was used.
Results: In total, there were 14,894 eligible participants, and 4601 (30.9%) participants were found to have insomnia symptoms. The regression model revealed that a higher risk of insomnia symptoms was associated with being over the age of 40 years, having history of psychiatric disorders, smoking, having infected friends or colleagues, having depressive or somatic symptoms, experiencing psychological distress and feeling estranged from family members. Meanwhile a lower risk of insomnia symptoms was associated with being female, having closer family relationships, not feeling alienated from others and being satisfied with the available information.
Conclusion: In our study, 30.9% of the participants in the general public reported insomnia symptoms after the COVID-19 epidemic had been initially controlled. When providing precise interventions for insomnia, extra attention should be paid to the individuals who are male, elderly and smokers, and those with psychiatric disorder history, with infected friends or colleagues, with psychological symptoms and with poor social support.
Keywords: insomnia symptoms, prevalence, COVID-19, under control, general public, China
Corrigendum for this paper has been published
Introduction
In December 2019, the novel coronavirus (COVID-19) first broke out in Wuhan, China, causing grave concern among the public.1 To prevent the broader spread of the disease, the Chinese government decided to restrict all the outbound and inbound channels, first in Hubei Province and later in the entire country.2 This preventative action had a remarkable effect, which could be reflected by the fact that there have been no more confirmed cases among local residents since May 24th.3 Within the succeeding 18 days, only one new indigenous confirmed case was reported (on June 6th).4 It was the first time there had been so few new indigenous confirmed cases for so long- even longer than the 2-week incubation of COVID-19. Therefore, it can be stated that the COVID-19 epidemic had been initially controlled in Mainland China in those 18 days. However, a tendency towards the COVID-19 epidemic resurgence started to show up since June 11th.5
COVID-19 caused concern as well as great psychological problems in both regular citizens and healthcare workers. Depression, anxiety, insomnia and acute stress symptoms were all found to be more prevalent among the public during the outbreak.6 More severe symptoms of these mental health problems occurred among the patients confirmed or suspected of having COVID-19, the people with confirmed or suspected family members and friends, and the residents of Hubei Province.6 Quarantine and delays to return to work were also found to be associated with mental health status.6 Another study showed that the prevalence of somatic symptoms also increased in the general population at the peak of the epidemic period compared to the beginning of the outbreak, which was thought to be related to psychological resilience.7 In addition, a high prevalence of sleep problems were observed among the adolescents whose anxiety and depression symptoms were proved to be mediators of social support and insomnia symptoms.8 Furthermore, a systematic review and meta-analysis suggested that a considerable proportion of healthcare workers experienced mood and sleep disturbances during this outbreak.9 Regarding the factors related to insomnia in healthcare workers, Zhang’s study found that insomnia symptoms were associated with education level, isolated environment, the psychological worries about the COVID-19 outbreak, and doctor occupation.10 In regard to the period after the COVID-19 pandemic had been controlled, a longitudinal study showed that fear significantly decreased while depression levels significantly increased over the course of the pandemic.11 However, a contradictory result was reported in another study investigating perinatal women, which showed a decrease in the prevalence of depression, anxiety and insomnia symptoms.12
Although several studies have analyzed the psychological health status in China during the COVID-19 epidemic, most of them focused on each particular population, such as healthcare workers, adolescents and perinatal women. In addition, only few studies have investigated the public mental health situation after the COVID-19 epidemic had been under control rather than the outbreak time. Lastly, to the best of our knowledge, no studies have investigated insomnia after the COVID-19 epidemic had been under control. In view of this gap in knowledge, we conducted this large-sample study to assess insomnia symptoms and to explore the related social psychological factors of insomnia symptoms in the Chinese general public after the epidemic had been initially controlled.
Methods
Study Design and Samples
The survey was cross-sectional and was conducted online among Chinese citizens, using the convenience sampling method. It was launched on June 5th, 2020, after the COVID-19 epidemic had been controlled in all of Mainland China for nearly 2 weeks, and it ended on June 7th, 2020. The survey link was posted on JD Health APP, a large e-commerce and information service platform that has over 70 million users and provides online health products and services in China. All the APP users can obtain access to the survey, but each account can only submit the survey once. Before it started, the purpose and significance of the survey were briefly introduced to all participants, and participant consent was required to continue. The survey was allowed to proceed only if all the questions were answered before the final submission, and then the data were recorded and stored on the APP automatically. A string would be generated and recorded automatically by the APP system to replace each user’s name, ensuring confidentiality in the further data handling. Participants who met the following criteria were qualified: (1) could read a questionnaire written in Chinese, (2) JD Health APP users, and (3) volunteered for the survey. The exclusion criteria consisted of (1) being unable to understand the questionnaire and (2) being under 18 years old. The study was approved by the Ethics Committee of Nanfang Hospital of Southern Medical University. To guarantee the respondents’ privacy, the survey was conducted anonymously. The study was conducted in accordance with the Declaration of Helsinki.
Measures
Demographic data were collected. Self-designed questions related to the impact of COVID-19 epidemic, such as infection status, the perceived feelings on changes of relationship and satisfaction of available information, were asked in the survey. We also administered the Insomnia Severity Index, the Patient Health Questionnaire-9, the Somatic Symptom Scale-8, and the Impact of Events Scale-Revised.
To detect the symptoms and cases of insomnia, the Insomnia Severity Index (ISI) was used. ISI is a reliable and valid instrument to quantify perceived insomnia severity.13 The total scores of ISI ranges from 0 to 28, with each item rated on a 0–4 scale. Higher scores indicate more severe insomnia symptoms.14 The score of ≥8 is considered to indicate symptoms of insomnia.15
The Patient Health Questionnaire-9 (PHQ-9) was included to assess depressive symptoms. The total score can be categorized into five severity levels: normal (0–4), mild depression (5–9), moderate depression (10–14), moderate to severe depression (15–19) and severe depression (20–27).16,17 Previous study had proved a great reliability and validity of the PHQ-9 among the Chinese general population.17
For the evaluation of psychological distress in response to COVID-19, the Impact of Events Scale-Revised (IES-R) was performed.18 It is a five-point Likert scale for which the total scores can be categorized into four different levels: subclinical (0–8), mild (9–25), moderate (26–43) and severe (44–88). The great reliability and validity were observed in the Chinese version of IES-R.19
The Somatic Symptom Scale–8 (SSS-8), composed of 8 items, was used for assessing the somatic symptom burden over the past 7 days. The sum of the scores ranges from 0 to 32, which can be categorized into five different levels: none to minimal (0–3), low (4–7), medium (8–11), high (12–15) or very high (16–32) physical symptoms.20 Matsudaira’s study had confirmed the validity and internal consistency of SSS-8.21
Statistical Analysis
The categorical variables are presented as frequencies and percentages. Descriptive statistical analyses were performed by using the Chi-square test. Post-hoc analyses were performed on multiple category data by Bonferroni correction. To examine the associations among the demographic factors, epidemic-related factors and psychological factors with insomnia symptoms, a binary logistic regression was used. The regression model was adjusted for gender and age by using the enter method while other factors were analyzed by using the forward likelihood ratio method. The sensitivity analyses were conducted to determine the influence of the different cut-off score on the findings.15,22 All the analyses were two-tailed with an alpha level set at P < 0.05 and were conducted by using SPSS Analytics software v.22.0.
Results
Characteristics of the Subjects and Prevalence of Insomnia Symptoms
A total sample of 14,999 participants was finally obtained, and 105 (0.7%) of the initial respondents were excluded prior to the data analysis since their age was under 18. Tables 1 and 2 show the characteristics of the eligible participants and the differences between the insomnia symptom and non-insomnia symptom groups in terms of demographic data, COVID-19 epidemic-related questions and psychological status. Based on their ISI score (ISI ≥8), 4601 participants (30.9%) were found to have symptoms of insomnia. In addition, 6277 (42.1%) participants, 6501 (43.6%) participants and 8635 (58%) participants were found to have depressive symptoms (PHQ-9 ≥5), somatic symptoms (SSS-8 ≥4) and psychological distress (ISE-R≥9), respectively. The sensitivity analyses showed that the results obtained by using the cut-off scores of ≥8 were roughly consistent with that by using the cut-off scores of ≥10. (Shown in STables 1 and 2 in Supplement)
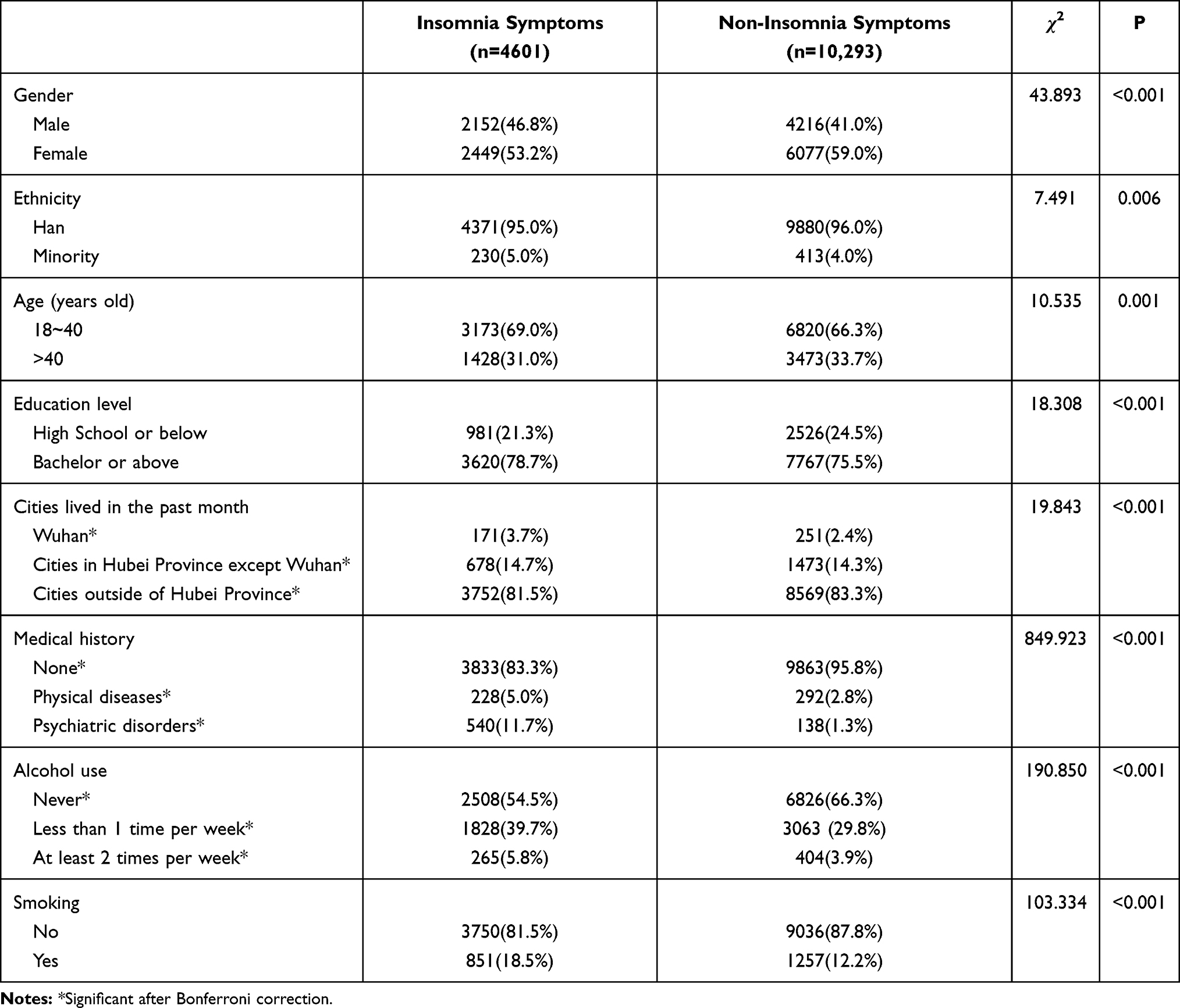 |
Table 1 Comparisons Between Insomnia Symptoms and Non-Insomnia Symptoms Individuals on Demographic Data. (N=14,894) |
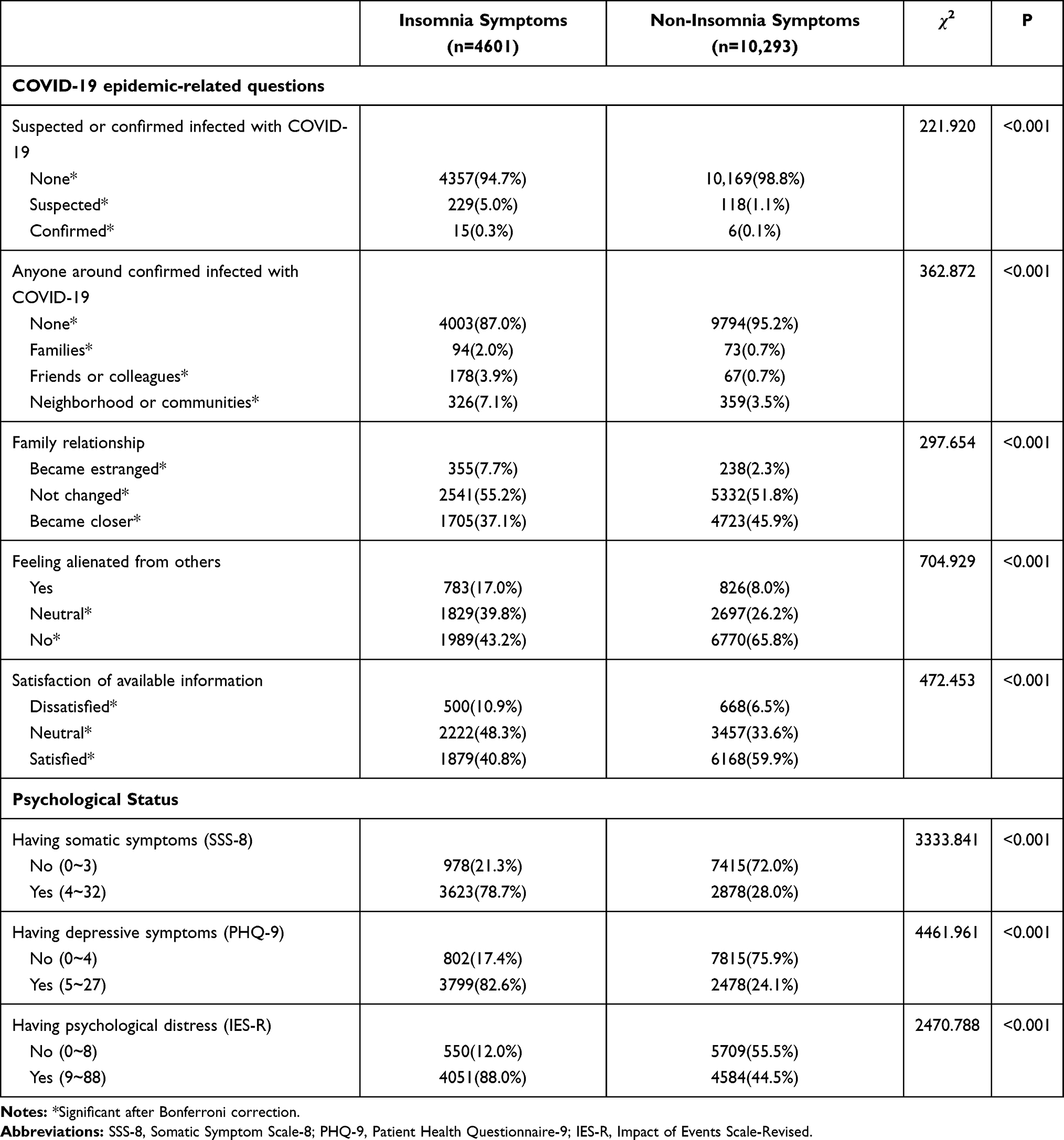 |
Table 2 Comparisons Between Insomnia Symptoms and Non-Insomnia Symptoms Individuals on COVID-19 Related Data and Psychological Status. (N=14,894) |
The participants with insomnia symptoms (ISI ≥8) were likely to be in the 18-to-40-year-old age range, be of minority ethnicity, have bachelor’s degree or above, live in Wuhan, have medical history of psychiatric disorders, drink alcohol at least 2 times per week, smoke, be confirmed to have been infected with COVID-19, have infected friends or colleagues, become estranged from their family, feel alienated from others, be dissatisfied with the available information, have somatic symptoms, have depressive symptoms and experience psychological distress when compared with those without insomnia symptoms. However, female participants displayed a lower risk for insomnia symptoms. (Shown in Tables 1 and 2) The results of the unadjusted regression analysis of the related variables are presented in STable 3 in the Supplement.
Factors Associated with Symptoms of Insomnia
The results of the binary logistic regression analysis on insomnia symptom-related factors are shown in Table 3. Female participants were found to have a lower risk of insomnia symptoms than male participants (adjusted OR 0.80, 95% CI 0.72–0.88). Compared with the participants aged 18 to 40 years old, those over 40 years old demonstrated a higher risk of insomnia symptoms (adjusted OR 1.16, 95% CI 1.05–1.28). The participants with medical history of psychiatric disorders also showed a higher risk of insomnia symptoms than those without any medical history (adjusted OR 3.10, 95% CI 2.46–3.90). Besides, the participants who smoked had a higher risk than nonsmokers (adjusted OR 1.41, 95% CI 1.22–1.61). In addition, an elevated risk for symptoms of insomnia was found in the participants with depressive symptoms (adjusted OR 5.35, 95% CI 4.83–5.93), somatic symptoms (adjusted OR 3.43, 95% CI 3.11–3.78) and psychological distress (adjusted OR 3.24, 95% CI 2.89–3.63). Having infected friends or colleagues and feeling estranged from family members were also found to be other risk factors (adjusted ORs 1.70 [95% CI 1.17–2.46] vs 1.46 [95% CI 1.17–1.82]). Nonetheless, a lower risk of insomnia symptoms was associated with having closer family relationships (adjusted OR 0.87, 95% CI 0.79–0.95), not feeling alienated from others (adjusted OR 0.79, 95% CI 0.71–0.87) and being satisfied with the available information (adjusted OR 0.69, 95% CI 0.63–0.76).
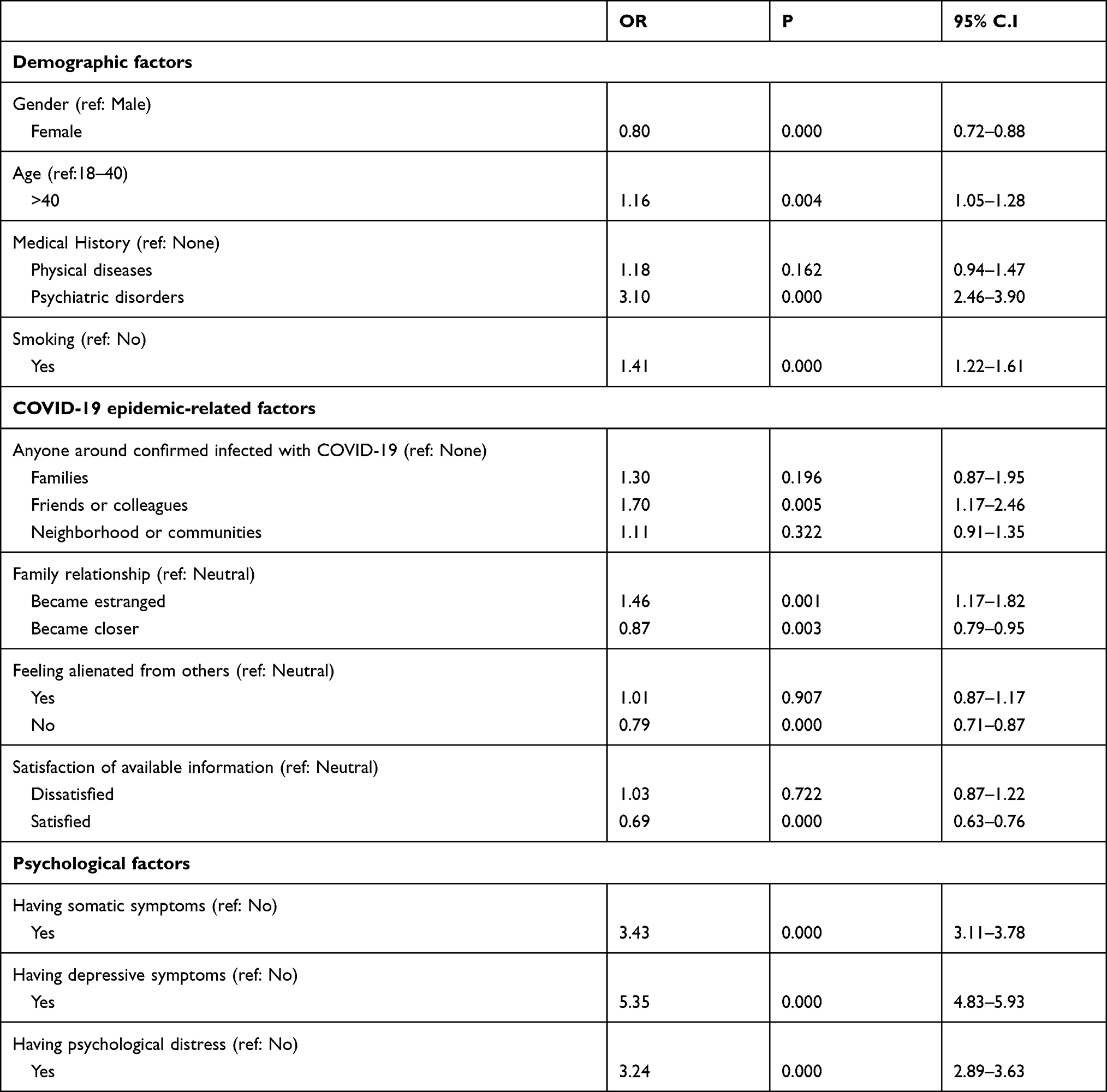 |
Table 3 Binary Logistic Regression Analysis of Insomnia Symptoms-Related Factors |
Discussion
To the best of our knowledge, this is the first study to investigate insomnia symptoms in the general public after the COVID-19 had been initially controlled. Among the large sample of 14,894 valid participants, 30.9% suffered from insomnia symptoms. More psychological problems related to COVID-19 appeared in those with insomnia symptoms. Being male, being older, having medical history of psychiatric disorders, smoking, having somatic symptoms, having depressive symptoms and experiencing psychological distress were all found to be risk factors for insomnia symptoms, while having closer relationships with family, not feeling alienated from others and being satisfied with information about COVID-19 were protective factors.
The prevalence of insomnia symptoms during the remission period was 30.9% in our study, which is higher than 15.0% during normal times and 20.05% at the beginning of the COVID-19 outbreak.23,24 The prevalence rate in our study was consistent with 29.2% among the Chinese general public during the pandemic period in another study, using the same measurement and cut-off.6 However, it is much higher than 13.9% in another study conducted after the epidemic had been controlled, which may be due to the different measurements used in the two studies.12 The higher prevalence of our finding shows that insomnia symptoms occurred along with the outbreak of COVID-19 and continued to present even after the epidemic had been under control. This finding might indicate that insomnia symptoms tended to become chronic during the whole epidemic period. Many reasons can account for this finding, among which stress is usually considered the primary one.25 The mechanism underlying this insomnia involves stress activating the hypothalamo-pituitary-adrenocortical (HPA) systems, which is incompatible with normal sleep, and the resulting sleep impairment causes further increases in the HPA system. This last effect promotes a vicious circle of stress and insomnia.26 The primary source of stress in this study was clearly derived from the COVID-19 epidemic. According to this finding, the trend in insomnia symptoms becoming chronic may warn us that the stress from COVID-19 lasted from the epidemic outbreak period to the period that the epidemic had been controlled. Thus, understanding and dealing with the stress from COVID-19 may be still necessary for effectively treating insomnia symptoms even after the epidemic had been controlled.
Some demographic factors were found to be associated with insomnia symptoms. Our study surprisingly found that female individuals were less likely to have insomnia symptoms than males, which is contrary to most previous studies.27–29 However, the trend we found was consistent with the result of a recent study conducted during the COVID-19 outbreak period.6 One of the reasons may be attributable to the more frequent risky behaviors during epidemics and a higher infective rate among males.6 Another reason was that male had poorer knowledge about COVID-19 than female,30 resulting in their fear and worry about COVID-19 and hyperarousal. In line with previous studies, the rate of insomnia symptoms rose with age, and insomnia symptoms were more likely to occur in elderly individuals.31,32 The participants aged over 40 in our study suffered more symptoms of insomnia than the youth aged 18 to 40. This phenomenon can be explained by the significant physiological changes in sleep and circadian rhythm across the lifespan.33 In addition, stressful life events or medical conditions, such as respiratory symptoms, physical disability and poor perceived health, also place older adults in an increased risk of insomnia.33 Besides, the smokers in our study had a higher risk of insomnia symptoms than nonsmokers, which is the same as previous findings.34,35 The mechanism is diverse, but the most important mechanism is related to nicotine. This active ingredient is a stimulant that increases alertness, so using it too close to bedtime may affect sleep latency.36 Furthermore, nicotine was believed to increase the risk for snoring and obstructive sleep apnea, ultimately leading to insomnia symptoms.37
Another fact we need to note is that depressive symptoms, somatic symptoms and psychological distress were three important factors that were significantly associated with insomnia symptoms. The same results were observed in a study concerning adolescents.8 The medical history of psychiatric disorders was also found to be a risk factor. This finding is reasonable since insomnia can become secondary to psychiatric disorders or psychological problems, while insomnia may either arouse psychiatric or psychological symptoms. Ohayon has shown that a previous history of a mental disorder is closely related to the severity and chronicity of current insomnia.38 Another study done by Have verified that insomnia was a prevalent problem across different categories of mental disorders, even during the remitted phase.39 Therefore, when intervening in insomnia in the general public, the people with history of mental illness may deserve more attention. It would be necessary to address psychiatric or psychological symptoms to cope with a patient’s insomnia symptoms, although we should reduce their stress at the same time.
As expected, our study showed that the people with better social support (including the support from families and friends) or psychological support (including the satisfaction regarding available information) were at a lower risk of developing symptoms of insomnia. The same evidence was noted by Roberts et al In their study, more severe insomnia at baseline significantly predicted worse parental relationships, lower perceived social support, and more problems with peers one year later.40 Social support is an important resource linked to one’s mental well-being. The people who frequently experience stressful events in their daily life benefit from social support because it contributes to an individual’s capability to cope with negative life experiences and to mitigate the negative impact of stress.41 In other words, ineffective social support may lead to more stress and ultimately result in insomnia.
In summary, understanding the factors associated with insomnia symptoms could help to provide precise interventions for insomnia in the public. Extra attention should be paid to the people who are male, elderly, and smokers and those with history of a psychiatric disorder. Moreover, maintaining proper interpersonal relationships and improving satisfaction with the available information may help to reduce the risk of insomnia. To accomplish more effective interventions for insomnia, there are some actions that might be emphasized. On the one hand, medical services should be redistributed to ensure the timely treatment for mental health problems, since patients with mental disorders could not receive timely diagnoses, treatment or routine psychiatric care because of the suspended hospital visits during the outbreak period.42 On the other hand, online mental health services, such as hotlines and mobile application platforms, are recommended to be adopted more widely considering the traffic limits and quarantine measures in many areas.43
The strengths of this study are its wide coverage among the Chinese citizens, enormous sample size and special study period. The participants were recruited from different places with multi-demographic and COVID-19 epidemic-related characteristics. Furthermore, to the best of our knowledge, this is the first study conducted to investigate the prevalence of and factors associated with insomnia symptoms systematically after COVID-19 had been initially controlled. We observed that insomnia symptoms among the general public might have trended towards becoming chronic during the entire epidemic period. Our results and findings may be helpful to make political or medical decisions during this new period of the COVID-19 epidemic.
Our study has several limitations. First, this survey was completed online using a convenience sampling method. Only people having logging into their accounts on the JD Health APP could take part in the survey, meaning that the people being less technology literate may not be able to attend the survey. Therefore, the representativeness and the generalizability of the findings might be limited due to the restriction of entering the survey and its sampling method, although this study was geographically extensive and had a large sample size. Second, the total quantity of the APP users having opened the survey link was not recorded in our study, leaving the response rate unknown. Third, all the demographic data or mental health symptoms in the survey were self-reported, which may lead to some bias. Fourth, this was a cross-sectional study, so the associations between mental health symptoms and risk factors could not be considered as causal relationships. Finally, our findings suggested the possibility that insomnia symptoms tended to become chronic. However, further studies, especially follow-up studies, are required to draw these conclusions.
Conclusion
In our study, 30.9% of participants in the Chinese general public reported insomnia symptoms after the COVID-19 epidemic had been initially controlled. When providing precise interventions for insomnia, extra attention should be paid to the individuals who are male, elderly, and smokers and those with psychiatric disorder history, with friends or colleagues infected, with psychological symptoms and with poor social support.
Abbreviations
COVID-19, Corona Virus Disease 2019; ISI, Insomnia Severity Index; PHQ-9, Patient Health Questionnaire-9; SSS-8, Somatic Symptom Scale-8; IES-R, Impact of Events Scale-Revised.
Acknowledgment
We would like to thank all the individuals and organizations that are contributing to this research. Firstly, to Nanfang Hospital of Southern Medical University for the support in the whole process. Secondly, to Renmin Hospital of Wuhan University for their support and participating in the study.
Funding
This study was funded by grant 82071488 from the National Natural Science Foundation of China, grant 2018YFC1314600 from the National Key R&D Program of China, grant 2019Z014 from the President Foundation of Nanfang Hospital, Southern Medical University, and grant CX2018N018 from the Scientific Research Initiation Program of Southern Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
2. National Health Commission of PRC [Website]. Timeline of China releasing information on COVID-19 and advancing international cooperation; 2020. Available from: http://en.nhc.gov.cn/2020-04/06/c_78840.htm.
3. National Health Commission of PRC [Website]. March 25 Daily briefing on novel coronavirus cases in China; 2020. Available from: http://en.nhc.gov.cn/2020-03/25/c_78235.htm.
4. National Health Commission of PRC [Website]. June 7: daily briefing on novel coronavirus cases in China; 2020. Available from: http://en.nhc.gov.cn/2020-06/07/c_80659.htm.
5. National Health Commission of PRC [Website]. June 12: daily briefing on novel coronavirus cases in China; 2020. Available from: http://en.nhc.gov.cn/2020-06/12/c_80731.htm.
6. Shi L, Lu Z, Que J, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the Coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3(7):e2014053. doi:10.1001/jamanetworkopen.2020.14053
7. Ran L, Wang W, Ai M, Kong Y, Chen J, Kuang L. Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: a study of the general population in China at the peak of its epidemic. Soc Sci Med. 2020;262:113261. doi:10.1016/j.socscimed.2020.113261
8. Zhou SJ, Wang LL, Yang R, et al. Sleep problems among Chinese adolescents and young adults during the coronavirus-2019 pandemic. Sleep Med. 2020;74:39–47. doi:10.1016/j.sleep.2020.06.001
9. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
10. Zhang C, Yang L, Liu S, et al. Survey of insomnia and related social psychological factors among medical staff involved in the 2019 novel Coronavirus disease outbreak. Front Psychiatry. 2020;11.
11. Duan H, Yan L, Ding X, Gan Y, Kohn N, Wu J. Impact of the COVID-19 pandemic on mental health in the general Chinese population: changes, predictors and psychosocial correlates. Psychiatry Res. 2020;293:113396. doi:10.1016/j.psychres.2020.113396
12. Zeng X, Li W, Sun H, et al. Mental health outcomes in perinatal women during the remission phase of COVID-19 in China. Front Psychiatry. 2020;11:571876. doi:10.3389/fpsyt.2020.571876
13. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
14. Morin CM, Belleville G, Belanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608.
15. Wong ML, Lau K, Espie CA, Luik AI, Kyle SD, Lau E. Psychometric properties of the Sleep Condition Indicator and Insomnia Severity Index in the evaluation of insomnia disorder. Sleep Med. 2017;33:76–81. doi:10.1016/j.sleep.2016.05.019
16. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
17. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
18. Weiss D. The Impact of Event Scale: Revised. Springer; 2007; 219–238.
19. Wu KK, Chan KS. The development of the Chinese version of Impact of Event Scale - Revised (CIES-R). Soc Psych Psych Epid. 2003;38(2):94–98. doi:10.1007/s00127-003-0611-x
20. Gierk B, Kohlmann S, Kroenke K, et al. The somatic symptom scale–8 (SSS-8). JAMA Intern Med. 2014;174(3):399. doi:10.1001/jamainternmed.2013.12179
21. Matsudaira K, Oka H, Kawaguchi M, et al. Development of a Japanese version of the Somatic Symptom Scale-8: psychometric validity and internal consistency. Gen Hosp Psychiatry. 2017;45:7–11. doi:10.1016/j.genhosppsych.2016.12.002
22. Morin CM, Belleville G, Bélanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608.
23. Cao X, Wang S, Zhong B, et al. The prevalence of insomnia in the general population in China: a meta-analysis. PLoS One. 2017;12(2):e170772.
24. Lin LY, Wang J, Ou-Yang XY, et al. The immediate impact of the 2019 novel coronavirus (COVID-19) outbreak on subjective sleep status. Sleep Med. 2020;77:348–354. doi:10.1016/j.sleep.2020.05.018
25. Morin CM, Rodrigue S, Ivers H. Role of stress, arousal, and coping skills in primary insomnia. Psychosom Med. 2003;65(2):259–267. doi:10.1097/01.PSY.0000030391.09558.A3
26. Åkerstedt T. Psychosocial stress and impaired sleep. Scand J Work Environ Health. 2006;32(6):493–501. doi:10.5271/sjweh.1054
27. Pieh C, Budimir S, Probst T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J Psychosom Res. 2020;136:110186. doi:10.1016/j.jpsychores.2020.110186
28. Fu W, Wang C, Zou L, et al. Psychological health, sleep quality, and coping styles to stress facing the COVID-19 in Wuhan, China. Transl Psychiat. 2020;10(1). doi:10.1038/s41398-020-00913-3.
29. Zhang B, Wing Y. Sex differences in insomnia: a meta-analysis. Sleep (New York, N Y). 2006;29(1):85–93. doi:10.1016/j.explore.2005.10.022
30. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
31. Xiang YT, Ma X, Cai ZJ, et al. The prevalence of insomnia, its sociodemographic and clinical correlates, and treatment in rural and urban regions of Beijing, China: a general population-based survey. Sleep. 2008;31(12):1655–1662. doi:10.1093/sleep/31.12.1655
32. Benbir G, Demir AU, Aksu M, et al. Prevalence of insomnia and its clinical correlates in a general population in Turkey. Psychiat Clin Neuros. 2015;
33. Patel D, Steinberg J, Patel P. Insomnia in the elderly: a review. J Clin Sleep Med. 2018;14(06):1017–1024. doi:10.5664/jcsm.7172
34. Chen L, Steptoe A, Chen Y, Ku P, Lin C. Physical activity, smoking, and the incidence of clinically diagnosed insomnia. Sleep Med. 2017;30:189–194. doi:10.1016/j.sleep.2016.06.040
35. National Institutes of Health. National institutes of health state of the science conference statement on manifestations and management of chronic insomnia in adults, june 13–15, 2005. Sleep. 2005;28(9):1049–1057. doi:10.1093/sleep/28.9.1049
36. Griesar WS, Zajdel DP, Oken BS. Nicotine effects on alertness and spatial attention in non-smokers. Nicotine Tob Res. 2002;4(2):185–194. doi:10.1080/14622200210123617
37. Trenchea M, Deleanu O, Suţa M, Arghir OC. Smoking, snoring and obstructive sleep apnea. Pneumologia. 2013;62(1):52–55.
38. Ohayon MM, Roth T. Place of chronic insomnia in the course of depressive and anxiety disorders. J Psychiatr Res. 2003;37(1):9–15. doi:10.1016/S0022-3956(02)00052-3
39. Ten HM, Penninx B, van Dorsselaer S, Tuithof M, Kleinjan M, de Graaf R. Insomnia among current and remitted common mental disorders and the association with role functioning: results from a general population study. Sleep Med. 2016;25:34–41. doi:10.1016/j.sleep.2016.07.015
40. Roberts RE, Ramsay roberts C, Ger chen I. Impact of insomnia on future functioning of adolescents. J Psychosom Res. 2002;53(1):561–569. doi:10.1016/S0022-3999(02)00446-4
41. Brailovskaia J, Schönfeld P, Zhang XC, et al. Study in Germany, Russia, and China: are resilient and social supported students protected against depression, anxiety, and stress? Psychol Rep. 2017;121(2):265–281. doi:10.1177/0033294117727745
42. Zhou J, Liu L, Xue P, Yang X, Tang X. Mental health response to the COVID-19 outbreak in China. Am J Psychiatry. 2020;177(7):574–575. doi:10.1176/appi.ajp.2020.20030304
43. Li W, Yang Y, Liu ZH, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci. 2020;16(10):1732–1738. doi:10.7150/ijbs.45120
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.