")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Prevalence And Predictors Of Opportunistic Infections Among HIV Positive Adults On Antiretroviral Therapy (On-ART) Versus Pre-ART In Addis Ababa, Ethiopia: A Comparative Cross-Sectional Study
Authors Dereje N , Moges K, Nigatu Y , Holland R
Received 4 June 2019
Accepted for publication 12 September 2019
Published 4 October 2019 Volume 2019:11 Pages 229—237
DOI https://doi.org/10.2147/HIV.S218213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Nebiyu Dereje,1 Kalkidan Moges,2 Yemisrach Nigatu,1 Roger Holland2
1Department of Public Health, Myungsung Medical College, Addis Ababa, Ethiopia; 2Department of Medicine, Myungsung Medical College, Addis Ababa, Ethiopia
Correspondence: Nebiyu Dereje
Department of Public Health, Myungsung Medical College, P.O. Box 14972, Addis Ababa, Ethiopia
Tel +251978788638
Email [email protected]
Purpose: Data comparing the burden of the opportunistic infections among the Pre-ART and On-ART HIV-infected patients in Ethiopia are scarce. Therefore, this study aimed to compare the prevalence and predictors of opportunistic infections in Pre-ART and On-ART HIV-infected patients.
Methods: A comparative cross-sectional study was conducted among adult patients infected with HIV and who were on Pre-ART or On-ART and followed up from 2012 to 2016 in Zewditu Memorial Hospital, Addis Ababa. Those patients who were infected with HIV, but not eligible for ART were categorized under Pre-ART follow-up (n=192) and those patients who started taking ART were categorized under the On-ART follow-up group (n=192). Patients were included in the study by using simple random sampling technique from the list of the patients registered in the ART follow-up database. The presence of opportunistic infections along with clinical findings and baseline laboratory data was extracted from the ART follow-up database and the medical records of the patients using a standardized checklist. Factors associated with the development of opportunistic infections were analyzed using multi-variable binary logistic regression analysis.
Results: The overall prevalence of opportunistic infections was found to be 33.6% (95% CI; 28.9–38.5). The prevalence of opportunistic infections among the Pre-ART group (38%) was higher than On-ART group (29.2%) (P-value = 0.04). Pulmonary tuberculosis was the most common opportunistic infection observed in both Pre-ART and On-ART groups. Being in the WHO clinical Stage III (AOR = 2.1; 95% CI 1.1–3.9) or Stage IV (AOR = 3.6; 95% CI 1.7–7.7) were independent predictors for the development of opportunistic infections.
Conclusion: The prevalence of opportunistic infections among the HIV-infected patients who were in Pre-ART was higher than On-ART group. This finding reinforces the need for early initiation of ART for HIV-infected patients irrespective of their CD4 counts.
Keywords: opportunistic infections, Pre-ART, On-ART, HIV, PLWHIV, WHO staging
Introduction
Opportunistic infections are diseases that cause infections in individuals whose immune systems are compromised.1–3 Morbidity and mortality in HIV disease are due to immunosuppression leading to life-threatening opportunistic infections during the natural course of the disease. Severely, immune-compromised HIV patients may develop a variety of opportunistic infections that have a significant impact on their well-being, quality of life, health care costs and their survival.3–5
The advent of antiretroviral therapy (ART) reduces viral replication, increases the number of CD4 lymphocytes and improves their function, re-establishing the defenses of the host and improving chances of survival.3–5 However, it is reported by different studies that there is still high prevalence of opportunistic infections among the HIV-infected patients receiving ART and those in the follow-up. Although, the incidence of opportunistic infections has decreased after the discovery of antiretroviral drugs, they remain an important problem in patients who are unaware of their HIV serologic status, in those not receiving ART, and even in those who are receiving ART due to poor adherence, failure and cross resistance.3,4,6–11 This problem of opportunistic infections in the era of ART was not well studied in Ethiopia. There is a limitation of the studies in comparing the burden of opportunistic infections among those patients taking ART and those not taking ART, but who are on the follow-up. Furthermore, data are scarce on identifying factors associated with the occurrence of the opportunistic infections among the groups of the HIV patients in Ethiopia.9–13
Therefore, this study has compared the burden of opportunistic infections in HIV-infected patients On-ART and Pre-ART, with the aim of assessing the impact of ART on reducing the occurrence of opportunistic infections. Hence, the finding of this study will be used to inform the policy makers and programmers to design appropriate care and control of opportunistic infections among the HIV-infected patients, to maintain a good quality of life and survival.
Methods And Materials
Study Setting, Design And Population
A comparative cross-sectional study was conducted among adult patients (>18 years) infected with HIV; who were on Pre-ART or On-ART follow-up from 2012 to 2016 in Zewditu Memorial Hospital. The hospital is located in Addis Ababa, the capital city of Ethiopia. The city has a population of 3,384,569 according to the 2007 population census, with annual growth rate of 3.8%. Zewditu Memorial Hospital is one of the prominent public hospitals in the city and the first ART service delivering facility since 2003 and has grown to become the largest HIV care and treatment center in the country. The ART clinic of the hospital currently delivers comprehensive HIV/AIDS services in the following areas: HIV counseling and testing, provision of ART (adult and pediatric), provision of co-trimoxazole and isoniazid prophylaxis, palliative care, TB/HIV treatment, sexually transmitted infections diagnosis and treatment, post-exposure prophylaxis for HIV, pre-cervical cancer evaluation and treatment, nutritional assessment and support, youth counseling support, pharmacy and data management services.
Sample Size And Sampling Procedures
A two-population proportion formula was used to estimate the sample size. The assumptions used were with a power of 80%, the proportion of opportunistic infections On-ART and Pre-ART groups were 9.1% and 67.2%, respectively, was taken from a research report conducted in Ethiopia.12 Then, the sample size determined was 384 samples (192 patients on Pre-ART and 192 patients On-ART).
There were a total of 2586 adult people living with HIV who were enrolled in the follow-up at Zewditu Memorial Hospital ART Clinic from Jan 2012 to Dec 2016. From which, 263 people were below the age of 15 years old and thus excluded. From the remaining 2323 adults who were in follow-up in the ART clinic, 459 patients were Pre-ART and 1864 patients were On-ART. Then, by using simple random sampling technique; a computer-based random number generating using the patient’s registry as a sampling frame, a total number of 384 patients were selected to be included in the study (Figure 1).
 |
Figure 1 Sampling procedures. |
Data Collection Tools And Procedures
Prior to the start of data collection, ethical clearance was obtained from the institutional review board of Myungsung Medical College and the Addis Ababa Regional Health Bureau.
According to the Federal Ministry of Health HIV ART follow-up guideline,5,13 HIV patients were expected to visit the ART follow-up clinic at least once a month. Those patients who are infected with HIV but not eligible for ART were categorized under pre-ART follow-up and those patients whose HIV status is confirmed and started ART were categorized under the ART follow-up. In either category and at every visit, data related to the patient’s demographic information, clinical condition, medical history, opportunistic infection diagnosis, adherence to ART, Isoniazid and/or cotrimoxazole prophylaxis use, any other treatment given and side effects would be registered in the standardized case report format. Therefore, data were extracted for our study from the ART follow-up database and medical records of the patients by using a standardized checklist, which was adapted from the Federal Ministry of Health HIV ART follow-up guidelines.13 The contents of the checklist include: socio-demographic characteristics (sex, age, residence, marital status, occupational status, educational status), ART and chemoprophylaxis-related information (ARV drug treatment, drug adherence, treatment regimen, Isoniazid and/or cotrimoxazole prophylaxis treatment and its adherence), laboratory-related information (CD4+ Count, hemoglobin value), opportunistic infections diagnoses, clinical information (i.e., WHO clinical staging), functional status of the patient (working, ambulatory or bedridden).5,13
Data extraction was carried out by trained female clinical nurses who were familiar with the ART follow-up unit. Data extractors were trained on objectives of the study, how to keep confidentiality of information, the contents of the checklist and the process of data extraction. On the days of data extraction, the principal investigator supervised the data extraction process by checking consistency and completeness of the data.
Data Management And Analysis
In this study, people living with HIV and who developed either of herpes zoster infection, candidiasis, cryptococcal meningitis, chronic diarrhea, encephalopathy, herpes simplex, Pneumocystis jiroveci pneumonia, pneumonia, pulmonary tuberculosis, extra-pulmonary tuberculosis, intestinal parasitosis, toxoplasmosis, or upper respiratory tract infections were considered as having opportunistic infections.
The functional status of the patients was categorized as working, if able to perform usual work in or out of the house, harvest, go to school; ambulatory, if able to perform activities to daily living; and bedridden, if not able to perform activities of daily living. The ART adherence was categorized as “good” if the patient misses three or less doses, “fair” if the patient misses three to eight doses and “poor” if the patient misses more than eight doses per month.13
Data were cleaned, entered and analyzed by using SPSS version 20 software. Descriptive analysis including frequency distribution and percentage was made to describe socio-demographic and clinical characteristics and to determine the magnitude of the relative burden of opportunistic infections in the two groups, On-ART and Pre-ART. The prevalence of the opportunistic infections was described with percentage and 95% confidence interval. The difference in the prevalence of opportunistic infections among the two groups was analyzed by using Chi-square test. Bivariate analysis was carried out to determine the association of each independent variable (sex, age, marital status, functional status, received prophylaxis, CD4 count, WHO clinical stage) with the dependent variable (presence of opportunistic infection). The statistically significant difference was considered at p-value <0.05 at 95% confidence interval. Multi-variable binary logistic regression analysis was carried out to identify predictors of developing opportunistic infections in both groups. Variables which had p-value <0.25 in the bivariate analysis were considered in the multi-variable analysis and odds ratio was used to ascertain the strength of associations between the variables.
Results
Socio-Demographic Characteristics
Sample data from three hundred eighty-four (384) patients were analyzed. Majority of them 206 (53.6%) were females and in the age group of 35–44 years (40%). Approximately, one out of ten of the patients were bed-ridden during the diagnosis of the opportunistic infections. In the bivariate analysis, being in the 35–44 years age category and being bedridden have shown statistically significant association with the development of opportunistic infections (p-value <0.05) (Table 1).
 |
Table 1 Socio-Demographic Characteristics And Its Association With Opportunistic Infections Among Pre-ART And On-ART HIV-Infected Patients On Follow-Up In Zewditu Memorial Hospital, Addis Ababa, Ethiopia |
Baseline Clinical Characteristics Of HIV-Infected Patients
As noted in Table 2, the majority of the HIV-infected patients in both groups, 54.7% and 36.5% in Pre-ART and On-ART, respectively, were in the Stage I of WHO clinical staging. Whereas, only 8.8% of the Pre-ART and 14.6% of the On-ART patients were in the Stage IV of WHO clinical staging. There was a statistically significant difference in the occurrence of opportunistic infections among the WHO stages, at which the occurrence of opportunistic infections was higher in Stage III and IV as compared to Stage I (P-value < 0.01).
 |
Table 2 Baseline Clinical Characteristics And Its Association With Opportunistic Infections Among HIV-Infected Patients In Pre-ART And On-ART In Zewditu Memorial Hospital, Addis Ababa, Ethiopia |
About half (45.8%) of the HIV-infected patients in Pre-ART and one-thirds of the HIV-infected patients On-ART had a CD4 cell count of more than 500 cells/mm3. A substantial proportion of the HIV-infected patients in Pre-ART and On-ART (19.8% and 33.3%, respectively) had a CD4 cell count less than 200 cells/mm3. Statistically, significant difference was not seen on the occurrence of opportunistic infections among the CD4 count categories.
Majority of HIV-infected patients who were On-ART (62.5%) and about one-third of the HIV-infected patients in the Pre-ART (37.5%) have received co-trimoxazole and/or isoniazid prophylaxis. However, statistically significant difference was not seen on the occurrence of opportunistic infections among those who took co-trimoxazole and/or isoniazid prophylaxis and those who did not take the prophylaxis.
Majority of the On-ART group HIV-infected patients (84.4%) received first-line regimen Anti-Retro Viral (ARV) Drugs (Tenofovir (TDF), Lamivudine (3TC), Efavirenz (EFV)) and more than three-fourths (86.6%) of the HIV-infected patients’ adherence to ARV drugs were categorized as good and the remaining were categorized as fair.
Prevalence Of Opportunistic Infections
The overall prevalence of opportunistic infections was found to be 33.6% (95% CI; 28.9–38.5). The prevalence of opportunistic infections among the Pre-ART groups was higher than On-ART groups, 38% (95% CI; 34.6–46.1) and 29.2% (95% CI; 20.5–33.2), respectively. Moreover, the difference in the prevalence of opportunistic infections in Pre-ART and On-ART groups was statistically significant (P=0.04). Pulmonary tuberculosis was the commonest opportunistic infection observed in both Pre-ART and On-ART groups (Table 3).
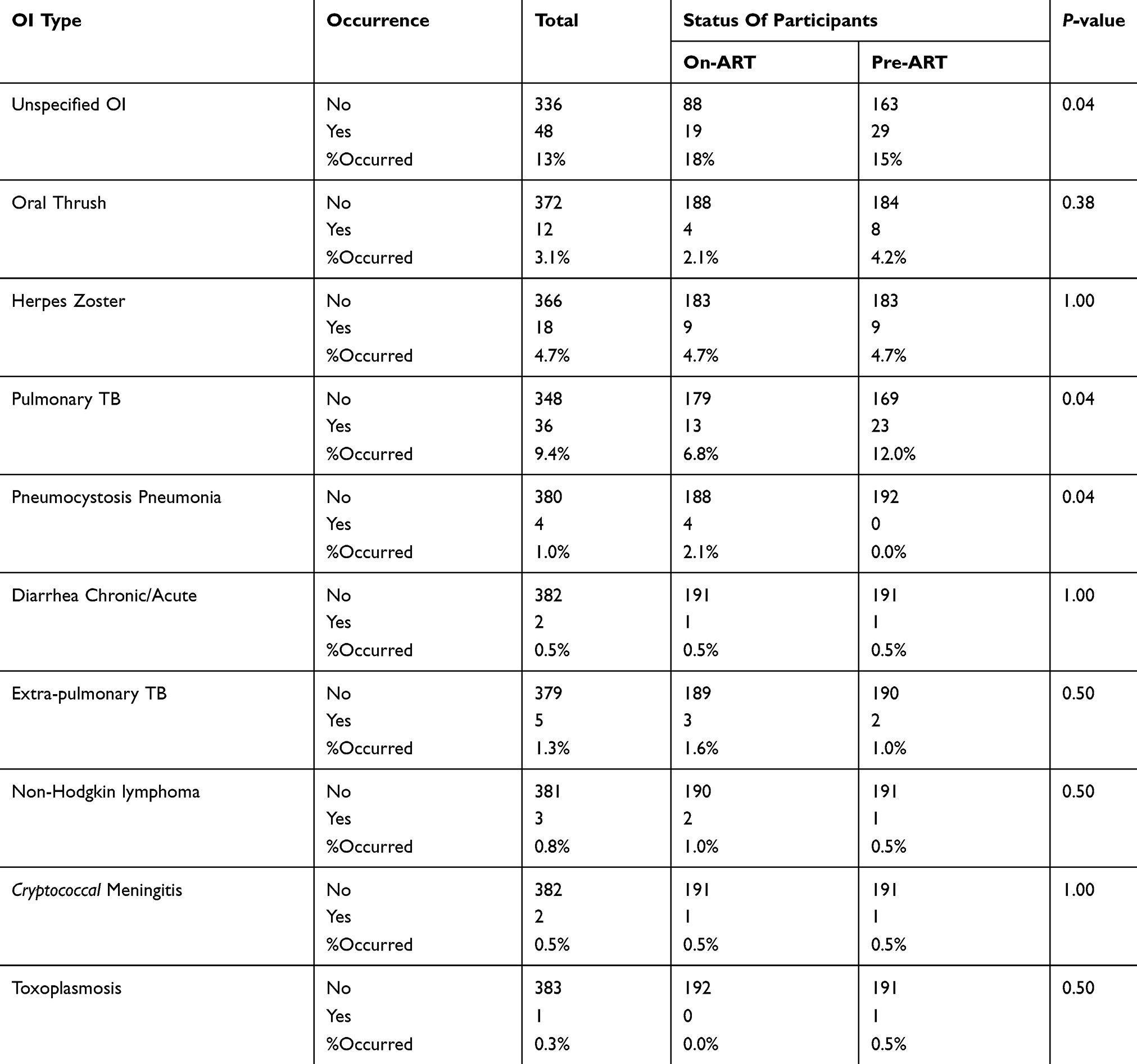 |
Table 3 Prevalence Of Opportunistic Infections Among HIV-Infected Patients In Pre-ART And On-ART In Zewditu Memorial Hospital, Addis Ababa, Ethiopia |
Predictors Of Opportunistic Infections
In the multi-variable binary logistic regression analysis, considering those variables with p-value less than 0.25 in the bivariate analysis, occurrence of opportunistic infections was associated with WHO clinical staging only. Age of the patients, functional status, CD4 count and receiving co-trimoxazole and/or isoniazid prophylaxis therapy were not associated with the occurrence of opportunistic infections (Table 4).
 |
Table 4 Multi-Variable Analysis Showing The Predictors Of Opportunistic Infections Among HIV-Infected Patients In Pre-ART And On-ART In Zewditu Memorial Hospital, Addis Ababa, Ethiopia |
The odds of the occurrence of opportunistic infections among HIV-infected patients who were in the WHO clinical Stage III were two times higher as compared to those who were in the WHO clinical Stage I (AOR = 2.1; 95% CI 1.1–3.9). Similarly, the odds of the occurrence of opportunistic infections among HIV-infected patients who were in the WHO clinical Stage IV were 3.6 times higher as compared to those who were in the WHO clinical Stage I (AOR = 3.6; 95% CI 1.7–7.7).
Discussion
This study is aimed to compare the prevalence and predictors of opportunistic infections among HIV-infected patients who were on Pre-ART and On-ART follow-up in Zewditu Memorial Hospital, Addis Ababa, Ethiopia. The principal findings of this study are that one-thirds of the HIV-infected patients developed opportunistic infections in their follow-up time from January 2012 to December 2016; slightly higher prevalence of opportunistic infections were observed among the Pre-ART group as compared to the On-ART group (38% vs 29.2%). This finding of the present study reinforce the need for initiation of ART for all HIV-infected patients irrespective of their CD4 counts, to reduce the burden of opportunistic infections and with ultimate goal of promoting good quality of life. The finding is also consistent with the notion that the introduction of ART is associated with a dramatic effect in the overall reduction of burden of opportunistic infections in people living with HIV.2,6,12,14–16 However, the Ethiopian HIV treatment and care guideline state that initiation of ART should be considered when the CD4 count ≤500 cells/mm3 irrespective of the WHO clinical staging or when the patient is on Stage 3 or Stage 4 of WHO clinical stage irrespective of the CD4 count. If the patient is not eligible for ART, he/she should be seen every three months regularly.13 This guideline is not consistent with the current WHO recommendation to initiate ART for all HIV-infected people irrespective of their CD4 count or clinical stages.5 Our finding also indicated that the burden of OIs was higher among those who did not receive ART as compared to those who were on ART. This finding calls for revision of the Ethiopian HIV care and treatment guideline for the betterment of the quality of life of the HIV-infected survivors and reduction of OI attributed mortality.
The current study’s prevalence of opportunistic infections among the HIV patients taking ART is comparable with the findings from North-West Ethiopia (19.7%)11 and Dessie (17.6%).9 However, it is comparably lower than the study findings from other parts of Ethiopia; Bahirdar (52.4%),17 Eastern Ethiopia (48%)18 and Debremarkos (42.8%).8 Moreover, the prevalence of opportunistic infections among the Pre-ART groups in our study is lower than a study conducted in Uganda, in which the prevalence of opportunistic infections in Pre-ART group was 74.2%.19 The discrepancy might be attributable to the time period of the study, at which the mentioned studies were conducted on and before 2012, when HIV treatment and care were not well organized in Ethiopia. Moreover, the HIV patients in our study were included from one of the pioneers and prominent central hospital for HIV care and treatment, which might have adequate skilled professionals and strict HIV patient follow-up system.
WHO clinical staging is the most significant predictor of opportunistic infections according to the finding of the present study. HIV-infected patients in WHO Stage III and IV were more likely to develop opportunistic infections than those who were in WHO Stage I and II. This finding of the study is consistent with other studies conducted in other parts of Ethiopia, namely; Bahirdar,17 Eastern Ethiopia,18 Arbaminch,12 Gondar11 and Debremarkos.8
Receiving cotrimoxazole and/or isoniazid prophylaxis were not found to be associated with reducing the development of OIs in this study. This might be explained by the absence of data with regard to the adherence and compliance status of patients to the prophylactic drugs. Moreover, other potential factors that can affect the effectiveness of the drugs were not addressed in this study due to the absence of these variables in the database or the patient charts. Therefore, we suggest other prospective longitudinal study which can evaluate the role of prophylaxis in reducing the burden of OIs among the HIV patients.
This study is limited because of the incompleteness of records in specifying the type of opportunistic infections present (13% of opportunistic infections were unspecified). Data on the adherence of ART, cotrimoxazole and/or isoniazid prophylaxis, some patient-related characteristics (e.g., nutritional status, exercise, behavioral factor) were not addressed in this study. Moreover, the baseline data for hemoglobin were not complete and thus excluded from analysis. However, these limitations of the study might not affect the interpretation of the findings with regard to the role of ART on the reduction of the burden of opportunistic infections and still with these limitations of the study, it is possible to reach on the provided conclusion. This is because, the variables missed from the database or the medical chart reviews are expected to be comparable as all the study participants share similar characteristics as all are HIV positive patients.
Conclusions
The prevalence of opportunistic infections among the HIV-infected patients who were in Pre-ART was higher than On-ART groups. This calls for early initiation of ART for HIV-infected patients irrespective of the CD4 counts.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ART, Highly Active Antiretroviral Therapy; HIV, Human immunodeficiency virus; OIs, Opportunistic Infections; PLWHIV, People Living with HIV; WHO, World Health Organization.
Ethics Approval And Consent To Participate
This study was approved by the Institutional Review Board of Myungsung Medical College and Addis Ababa Health Bureau. All participants of the study were informed about the study and they gave their verbal consent to be included in the study. The Institutional Review Board of Myungsung Medical College and Addis Ababa Health Bureau have approved using verbal consent of the participants.
Availability Of Data And Material
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Acknowledgments
The authors would like to thank Myungsung Medical College for funding of this study. The authors are grateful to the data collectors for their contributions.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Podlekareva D, Mocroft A, Dragsted UB, et al. Factors associated with the development of opportunistic infections in HIV-1–infected adults with high CD4 + cell counts: a EuroSIDA study. J Infect Dis. 2006;194(5):633–641. doi:10.1086/506366
2. Iroezindu MO. Prevalence and risk factors for opportunistic infections in HIV patients receiving antiretroviral therapy in a resource-limited setting in Nigeria. J AIDS Clin Res. 2013;01(S3):02. doi: 10.4172/2155-6113
3. Gona P, Van Dyke RB, Williams PL, et al. Incidence of opportunistic and other infections in HIV-infected children in the HAART era. J Am Med Assoc. 2006;296(3):292–300. doi:10.1001/jama.296.3.292
4. Iroezindu M. Disparities in the magnitude of human immunodeficiency virus-related opportunistic infections between high and low/middle-income countries: is highly active antiretroviral therapy changing the trend? Ann Med Health Sci Res. 2016;6(1):4. doi:10.4103/2141-9248.180234
5. WHO. Guidelines Guideline on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for Hiv. World Heal Organ [Internet]; 2015, September:78. Available from: http://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/.
6. Lee CY, Tseng YT, Lin WR, et al. AIDS-related opportunistic illnesses and early initiation of HIV care remain critical in the contemporary HAART era: a retrospective cohort study in Taiwan. BMC Infect Dis. 2018;18(1):1–12. doi:10.1186/s12879-018-3109-6
7. Rubaihayo J, Tumwesigye NM, Konde-Lule J. Trends in prevalence of selected opportunistic infections associated with HIV/AIDS in Uganda. BMC Infect Dis. 2015;15(1):1–15. doi:10.1186/s12879-015-0927-7
8. Moges NA, Kassa GM. Prevalence of opportunistic infections and associated factors among HIV positive patients taking anti-retroviral therapy in DebreMarkos referral hospital, northwest Ethiopia. J AIDS Clin Res. 2014;5(5):1–300. doi:10.4172/2155-6113.1000301
9. Missaye A, Dagnew M, Alemu A, Alemu A. Prevalence of intestinal parasites and associated risk factors among HIV/AIDS patients with pre-ART and on-ART attending dessie hospital ART clinic, Northeast Ethiopia. AIDS Res Ther. 2013;10(1):1–9. doi:10.1186/1742-6405-10-7
10. Tiku S, Tadesse T. Assessment of trends of HIV and its opportunistic infections in Ethiopian police. Ethiop J Heal Dev. 2014;28(3):162–169.
11. Damtie D, Yismaw G, Woldeyohannes D, Anagaw B. Common opportunistic infections and their CD4 cell correlates among HIV-infected patients attending at antiretroviral therapy clinic of Gondar University Hospital, Northwest Ethiopia. BMC Res Notes. 2013;6:1. doi:10.1186/1756-0500-6-534
12. Misker D, Demissie M, Mellie H. Effect of highly active antiretroviral therapy on incidence of opportunistic infections among HIV positive adults in public health facilities of Arba Minch Town, South Ethiopia: retrospective cohort study. J AIDS Clin Res. 2014;5(8):1–6. doi:10.4172/2155-6113.1000330
13. Ministry of Health of Ethiopia. Federal Democratic Republic of Ethiopia Ministry of Health National Guidelines for Comprehensive HIV Prevention, Care and Treatment. 2014:1
14. Low A, Gavriilidis G, Larke N, et al. Incidence of opportunistic infections and the impact of antiretroviral therapy among HIV-infected adults in low- and middle-income countries: a systematic review and meta-analysis. Clin Infect Dis. 2016;62(12):1595–1603. doi:10.1093/cid/ciw125
15. Eyongabane Ako S, Anna Njunda L, Achidi Akum E, et al. Immuno-hematological profile trends of HIV/AIDs patients on ART in the South West region of cameroon: retrospective medical report review for possible stratified follow-up pattern in low income settings. Am J Microbiol Res. 2018;6(2):47–56. doi:10.12691/ajmr-6-2-3
16. Shenoy N, Ramapuram JT, Shenoy A, Ahmed J, Srikant N. Incidence of opportunistic infections among HIV-positive adults on highly active antiretroviral therapy in a Teaching Hospital, India: prospective study. J Int Assoc Provid AIDS Care. 2017;16(3):309–311. doi:10.1177/2325957416686192
17. Abera B, Walle F, Tewabe T, Alem A, Yessin M. ART-naive HIV patients at feleg-hiwot referral Hospital Northwest, Ethiopia. Ethiop J Heal Dev. 2010;24(1):3–8.
18. Mitiku H, Weldegebreal F, Teklemariam Z. Magnitude of opportunistic infections and associated factors in HIV-infected adults on antiretroviral therapy in eastern Ethiopia. HIV/AIDS Res Palliat Care. 2015;7:137–144. doi:10.2147/HIV.S79545
19. Rubaihayo J, Tumwesigye NM, Konde-Lule J, Wamani H, Nakku-Joloba E, Makumbi F. Frequency and distribution patterns of opportunistic infections associated with HIV/AIDS in Uganda. BMC Res Notes. 2016;9(1):1–16. doi:10.1186/s13104-016-1938-1
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.