Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence and Predictors of Multi-Drug Resistant Organisms Among Ambulatory Cancer Patients with Urinary Tract Infections
Authors AbuSara A ![]() , Tayyeb N, Matalka L, Almomani B, Abaza H
, Tayyeb N, Matalka L, Almomani B, Abaza H ![]() , Nazer L
, Nazer L
Received 4 September 2022
Accepted for publication 16 December 2022
Published 3 February 2023 Volume 2023:16 Pages 747—753
DOI https://doi.org/10.2147/IDR.S388680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Aseel AbuSara,1 Nabiha Tayyeb,1 Lujain Matalka,1 Bayan Almomani,2 Haneen Abaza,3 Lama Nazer1
1Department of Pharmacy, King Hussein Cancer Center, Amman, Jordan; 2Department of Microbiology, King Hussein Cancer Center, Amman, Jordan; 3Office of Scientific Affairs and Research, King Hussein Cancer Center, Amman, Jordan
Correspondence: Aseel AbuSara, Department of Pharmacy, King Hussein Cancer Center, Queen Rania Al-Abdallah Street, P.O.Box 1269, Amman, 1191, Jordan, Tel + 962-6 5300460, Email [email protected]
Purpose: Urinary tract infections (UTIs) are among the most common community-acquired infections in patients with cancer. Though the prevalence of multi-drug resistant organisms (MDROs) has increased, there are limited studies on MDROs among ambulatory cancer patients with UTIs. Therefore, we aimed to evaluate the prevalence and predictors of MDROs in this patient population.
Patients and Methods: A retrospective study of adult cancer patients treated for bacterial UTIs in the ambulatory setting at King Hussein Cancer Center. The medical laboratory’s system was used to identify positive urine cultures taken in the ambulatory setting, between Aug 2020 and March 2021. UTIs were defined as a positive urine culture along with the initiation of antibiotics empirically or as definitive therapy. Patient characteristics, as well as the type and sensitivity of the bacterial organisms, were recorded. MDROs were defined as intrinsic or acquired non-susceptibility to at least one agent in three or more antimicrobial categories. Logistic regression was used to identify predictors that were independently associated with MDROs.
Results: A total of 376 patients had UTIs that met the inclusion criteria; mean age 60.5± 15.1 (SD) years and 330 (87.8%) had solid tumors. Gram-negative bacteria was recorded in the majority of UTIs (n = 368, 97.9%), the most common being Escherichia-coli (n = 220, 59.8%) and Klebsiella-pneumonia (n = 68, 18.5%). MDROs were recorded in 226 (60.1%) of urine cultures, with the majority being extended-spectrum-beta-lactamase producing organisms (n = 142, 62.8%). The only significant predictor was having had a UTI with MDRO within the past 6 months (OR 5.6, 95% CI 2.1– 15.2).
Conclusion: More than half of the positive urine cultures of cancer patients treated for UTIs in the ambulatory setting were MDROs. A subsequent UTI due to MDROs is more likely to occur in patients who had a UTI with an MDRO within the past 6 months.
Keywords: cancer, neoplasms, ambulatory care, urinary tract infections, drug resistance
Introduction
Urinary tract infections (UTIs) are among the most common community-acquired infections in patients with and without cancer.1–3 UTIs are associated with significant morbidity and mortality, and this burden has increased with the emergence of multi-drug resistant organisms (MDROs).4–8 MDROs are organisms that are resistant to one or more classes of antimicrobial agents.9 In a large study of over 17,000 patients, about one-fourth of the bacterial cultures were caused by MDROs.2 In a cross-sectional study of an oncology Center in Nepal, Shrestha et al reported that 89% of UTIs were caused by multi-drug-resistant strains and of the 73 studied culture-positive samples, only two samples were sensitive to all the antibiotics being tested.10
Over the past years, with the availability of newer treatment modalities, cancer patients are increasingly being treated in the outpatient setting.11 Ambulatory patients are at a lower risk of developing UTIs than hospitalized patients especially those caused by MDROs. On the other hand, it has been reported that resistance patterns of UTIs in the ambulatory setting is changing and that the prevalence of MDROs is increasing, but there is limited data evaluating cancer patients.12,13
Several studies described UTIs and risk factors for MDROs, but only a few of them focused on cancer patients; additionally, those studies either combined results of both outpatient and inpatient settings or included only hospitalized patients and/or all age group.4,10,14 Therefore, we aimed to evaluate the prevalence and predictors of MDROs in a cohort of adult cancer patients treated for UTIs in the ambulatory setting at a comprehensive cancer center.
Materials and Methods
This was a retrospective study conducted at King Hussein Cancer Center (KHCC), a comprehensive cancer teaching hospital in Amman, Jordan, that treats patients with all types of malignancies in the inpatient and outpatient settings. The study was approved by the Institutional Review Board, with a waiver of informed consent because of the retrospective nature of the study. The research was performed in compliance with the Declaration of Helsinki principles. All patient identifiers were coded and the patient data was handled with confidentiality.
We included adult cancer patients (≥18 years old) who were treated for UTIs in the ambulatory setting, between August 2020 and March 2021. The medical laboratory system was utilized to identify all positive urine cultures obtained during the study period. Cultures with fungal infections and those taken upon or during hospitalization were excluded. UTIs were defined as a positive urine culture along with antibiotics initiated empirically or as definitive therapy. For patients with multiple positive urine cultures, only the first one was included in the analysis to avoid the risk of including duplicate data.
At our institution, the urine specimen and cultures are processed as follows: a urine specimen is collected into a clean, sterile container and transported to the microbiology laboratory. Processing of specimens is typically done within 2 hours of collection. The urine specimen is then mixed prior to inoculation and a disposable calibrated loop is inserted vertically in the urine specimen for exact quantity. A loopful of sample is delivered to the agar plate. The plate is then streaked down the center and then cross-streaked at a 90° angle to the inoculum. The plate is examined after appropriate incubation time; once an organism is identified, susceptibility testing is performed, as appropriate.
For susceptibility testing, the disc diffusion test (Kirby Bauer) was used for the following organisms: Enterobacterales, Pseudomonas aeruginosa, Acinetobacter species, Stenotrophomonas maltophilia, Staphylococcus species and Enterococcus species while the E-test was used for the following organisms: Carbapenem-resistant enterobacterales (CRE), multi-drug resistant Escherichia coli, Klebsiella species (for meropenem, imipenem, and tigecycline), vancomycin resistant enterococcus (for vancomycin) and Staphylococcus species (for vancomycin and teicoplanin).
Patient characteristics, as well as the type and sensitivity of the bacterial organisms, were recorded. MDROs were defined as those with an intrinsic or acquired non-susceptibility to at least one agent in three or more antimicrobial categories, including penicillins, cephalosporins, aminoglycosides, monobactam, carbapenems, and fluoroquinolones.9 Patients with at least one MDRO in the urine culture were labeled to have MDRO UTI.
The hospital-based electronic patient records system was used to collect the patients’ characteristics, cancer diagnosis, co-morbidities, the presence of an indwelling urinary catheter or nephrostomy, as well as the laboratory readings including urine analysis, type of bacterial organisms in the culture, neutrophils, and platelets count. Other data including the history of previous hospitalization or ICU admission, use of chemotherapy, steroids, and antibiotics in the past three months, and the 30- and 90-days’ mortality were also collected.
Statistical Analysis
Categorical data were reported as counts and percentages while continuous data was reported as means and standard deviations (SD). The normality of the sample was tested using the Shapiro–Wilk test (P > 0.05), which indicated that it was not normally distributed. The characteristics of the patients and the cultures were compared between patients who developed MDROs and those who did not, using Pearson Chi-Square & Fisher’s Exact Tests for categorical variables and the Mann–Whitney U-test for continuous variables. The variables with P<0.1 in bivariate analyses were selected as candidate independent variables for a backward stepwise logistic regression analysis to identify predictors significantly and independently associated with the development of MDROs. All statistical analyses were performed using IBM SPSS V.28.0, and the P-value at level ≤0.05 (two-tailed) was considered significant.
Results
Out of 1059 screened positive urine cultures, a total of 376 cultures for 376 patients were included. The mean age for the patients was 60.5 years ±15.1 and 62.2% of the patients were females (n = 234). Among the cohort included, solid tumors (n = 330, 87.8%) were more prevalent than hematological malignancies (n = 46, 12.2%), and about half of the included patients had metastatic disease (n = 170, 45.2%). The majority of the patients’ urine samples were collected through midstream catch (n = 358, 95.2%). Table 1 outlines the characteristics of the patients included in the study, in addition to the results of the urine analysis.
 |
Table 1 Characteristics and Outcomes of Patients with and without Multi Drug Resistant Organisms (MDRO) |
The majority of urine samples included a single bacterial organism (n = 339, 90.2%), while the remaining samples included two or three organisms. Gram-negative bacteria represented the majority of the isolated organisms (n = 368, 88.7%), with the most common being Escherichia coli (n = 220, 59.8%) and Klebsiella pneumonia (n = 68, 18.5%). On the other hand, Gram-positive bacteria represented 11.3% of the UTIs, with the most common being Enterococcus faecalis (n = 18, 38.3%) and Coagulase-negative Staphylococcus species (n = 10, 21.3%). Table 2 outlines the type of organisms reported in the urine cultures.
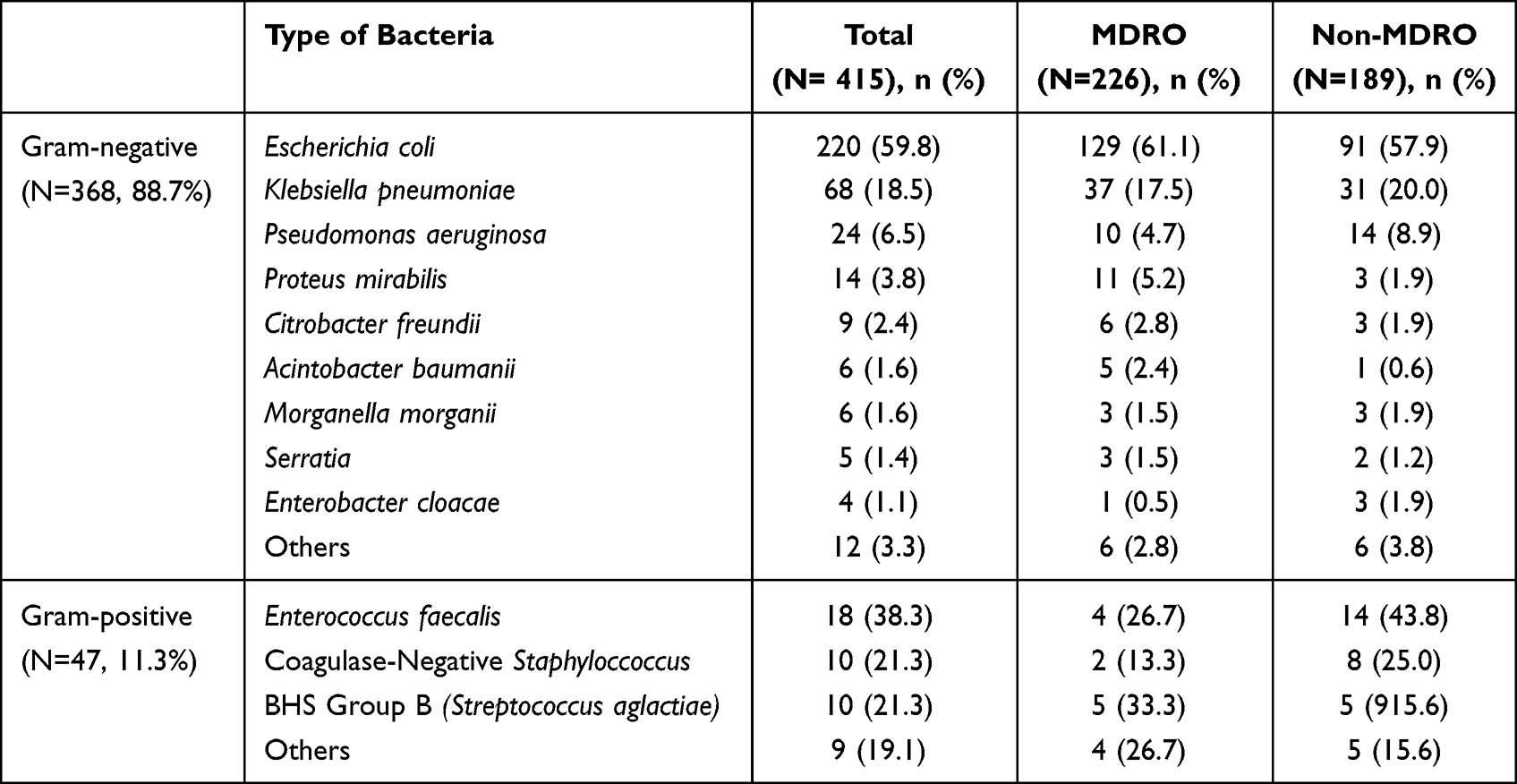 |
Table 2 Bacterial Profile of Urine Cultures |
Among the included patients, 202 (53.7%) had at least one MDRO identified in their urine cultures, of which the majority were extended-spectrum-beta-lactamase-producing organisms (ESBL) (n = 142, 62.8%). Other types of MDROs included carbapenem-resistant Pseudomonas aeruginosa, (n = 8, 3.6%), methicillin-resistant Staphylococcus aureus (n = 3, 1.3%) and carbapenem-resistant Enterobacterales (n = 2, 0.9%).
Among patients who were initiated on empirical antibiotics (n = 326, 87%), the most common were ciprofloxacin (n = 152, 47%), cefixime (n = 45, 14%), levofloxacin (n = 24, 7%) and amoxicillin/clavulanic acid (n = 23, 7%). Other antibiotics were trimethoprim/sulfamethoxazole, cefuroxime, nitrofurantoin, ceftriaxone and ertapenem. The susceptibilities for the most reported antibiotics and among tested isolates were as following: amikacin (97%), ceftazidime-avibactam (97%), ertapenem (97%), meropenem (97%), piperacillin/tazobactam (85%), gentamicin (73%), nitrofurantoin (67%), ciprofloxacin (63%), cefepime (59%), aztreonam (53%), ceftazidime (52%), ceftriaxone (50%), cefixime (45%), ampicillin/sulbactam (39%), trimethoprim-sulfamethoxazole (39%), cefazolin (30%) and ampicillin (14%).
In the bivariate analysis, age, gender, type of malignancy (solid/hematological), type of bacteria (gram-positive or gram-negative), number of previous positive urine cultures, MDROs in urine cultures within the past 6 months, antibiotic use within the past 3 months, and previous hospitalization within the past 3 months were significantly associated with the risk of developing MDRO UTI. However, in the multivariate analysis using logistic stepwise regression, the only significant independent predictor for developing a UTI with an MDRO was having such a diagnosis in the past 6 months (OR 5.632, 95% CI 2.087–15.196). On the other hand, having a UTI due to gram-positive bacteria in the past 6 months was associated with a reduced risk of developing a UTI with an MDRO (OR 0.032, 95% CI 0.003–0.297).
Discussion
In this study, we reported MDROs in the urine cultures of over half of the cancer patients with UTIs treated in the ambulatory setting. To our knowledge, this is the first study evaluating MDROs in a relatively large patient population with UTIs in the ambulatory setting. The findings are a call to action, as this prevalence is higher than that reported in non-cancer and cancer patients.11,14,15 Lee et al reported in non-cancer patients that the prevalence of ESBL-producing Escherichia coli was 12.1% and 23.1% in the outpatient and inpatient settings, respectively.16 This difference could be due to the empiric use of broad-spectrum antibiotics in cancer patients, such as fluoroquinolones, as well as their use as prophylaxis in specific groups.17 Also more than half of the patients in this study with MDRO UTI had recent hospitalization and this was shown to be associated with the emergence of ESBL-producing bacteria.18
In terms of the types of organisms identified in the urine cultures, our findings are consistent with what others have reported in the literature for non-cancer patients.4,19–21 In a systematic review, Tenney et al reported that Escherichia coli was the most common causative organism, ranging from 30 to 100% among the studies that were included in the review.4 In our study, Escherichia coli comprised more than half of the isolates from the urine cultures and this percentage was higher than what was reported by Sime et al, in a similar patient population but it only included females and had a very small number of isolates.14
The majority of patients who received empiric antibiotics were in alignment with what is in literature and recommended by the Infectious Diseases Society of America guidelines. However, the susceptibilities to those antibiotics were reported to be below 70%, which suggests that the majority of the patients were empirically treated with antibiotics to which the pathogens may be resistant. This is unlike what was reported in other studies were the susceptibility rates were higher.10
We also evaluated factors that may predict having MDROs among cancer patients with UTIs in the ambulatory setting. Such information can help clinicians in the choice of the most appropriate empiric therapy for patients. Patients who had an MDRO urine culture within the past 6 months were almost six times at risk of developing an MDRO UTI, when compared to those with non-MDRO urine cultures. Although this factor was not specifically studied in the literature it is generally consistent with what is stated by the Infectious Diseases Society of America guidelines that having a MDR gram-negative urinary isolate within the past 3 months is a risk factor for MDROs.4
Interestingly, unlike what was reported in the literature, our study did not show that urinary catheterization, previous hospitalization, previous antibiotic use, age, previous UTI, and/or male gender are associated with the risk of developing MDRO UTIs.4,22 This could be due to inconsistency in the definition of risk factors and MDRO; however, 4 studies reported in the systematic review had the same definition. In our study, we used the definition that was commonly reported in the literature.4 Another reason could be due to insufficient data due to the nature of the study particularly with catheterization.
Our study includes a number of limitations. First those that are related to the retrospective nature of the study such as the recognition of the type of UTIs including upper- or lower UTIs, complicated or uncomplicated UTIs. When collecting data retrospectively from electronic medical records, there is certainly the possibility of not having all the data documented; for example, urinary catheterization was not captured for all the patients. In addition, since it was difficult to accurately assess the clinical condition of the patient due to the retrospective nature of the study, our definition for UTIs was based on the presence of positive urine cultures and the prescribing of antibiotics. We did not include the assessment of other factors such as fever and the presence of urinary symptoms, and instead hypothesized that if the patient was started on antibiotics empirically then it was clinically considered as a true infection. Moreover, this was a single-center study which may impact the generalizability of the findings. Nevertheless, the study presents important findings related to a growing population of immune-compromised patients who are susceptible to infections and the associated complications.
Conclusion
More than half of the positive urine cultures of cancer patients treated for UTIs in the ambulatory setting had MDROs. A subsequent UTI due to MDROs is more likely to occur in patients who had a UTI with an MDRO within the past 6 months.
Data Sharing Statement
The datasets used for the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study’s protocol was approved by King Hussein Cancer Center Institutional Review Board (Reference Number: 21 KHCC 052F). A waiver of informed consent was approved due to the retrospective nature of the study.
Acknowledgments
The authors acknowledge the contribution of Mays Al Qayam in the data collection process.
Funding
This research received funding for a research assistant through King Hussein Cancer Center intramural grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Erdem I, Kara Ali R, Ardic E, et al. Community-acquired lower urinary tract infections: etiology, antimicrobial resistance, and treatment results in female patients. J Glob Infect Dis. 2018;10(3):129–132. doi:10.4103/jgid.jgid_86_17
2. Linhares I, Raposo T, Rodrigues A, et al. Incidence and diversity of antimicrobial multidrug resistance profiles of uropathogenic bacteria. Biomed Res Int. 2015;2015:354084. doi:10.1155/2015/354084
3. Hozzari A, Behzadi P, Kerishchi Khiabani P, et al. Clinical cases, drug resistance, and virulence genes profiling in Uropathogenic Escherichia coli. J Appl Genet. 2020;61(2):265–273. doi:10.1007/s13353-020-00542-y
4. Tenney J, Hudson N, Alnifaidy H, et al. Risk factors for acquiring multidrug-resistant organisms in urinary tract infections: a systematic literature review. Saudi Pharma J. 2018;26(5):678–684. doi:10.1016/j.jsps.2018.02.023
5. Khonsari M, Behzadi P, Foroohi F. The prevalence of type 3 fimbriae in Uropathogenic Escherichia coli isolated from clinical urine samples. Meta Gene. 2021;28:100881. doi:10.1016/j.mgene.2021.100881
6. Behzadi P. Classical chaperone-usher (CU) adhesive fimbriome: uropathogenic Escherichia coli (UPEC) and urinary tract infections (UTIs). Folia Microbiol. 2020;65(1):45–65. doi:10.1007/s12223-019-00719-x
7. Behzadi P, García-Perdomo HA, Karpiński TM, et al. Metallo-ß-lactamases: a review. Mol Biol Rep. 2020;47(8):6281–6294. doi:10.1007/s11033-020-05651-9
8. Sarshar M, Behzadi P, Scribano D, Palamara AT, Ambrosi C. Acinetobacter baumannii: an ancient commensal with weapons of a pathogen. Pathogens. 2021;10(4):387. doi:10.3390/pathogens10040387
9. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
10. Shrestha G, Wei X, Hann K, et al. Bacterial profile and antibiotic resistance among cancer patients with urinary tract infection in a National Tertiary Cancer Hospital of Nepal. Trop Med Infect Dis. 2021;6(2):49. doi:10.3390/tropicalmed6020049
11. Katayama H, Tabata M, Kubo T, et al. Demand for weekend outpatient chemotherapy among patients with cancer in Japan. Support Care Cancer. 2021;29:1287–1291. doi:10.1007/s00520-020-05575-x
12. Walker E, Lyman A, Gupta K, et al. Clinical management of an increasing threat: outpatient urinary tract infections due to multidrug-resistant uropathogens. Clin Infect Dis. 2016;63(7):9605. doi:10.1093/cid/ciw396
13. Behzadi P, Urbán E, Matuz M, et al. The role of gram-negative bacteria in urinary tract infections: current concepts and therapeutic options. Adv Exp Med Biol. 2021;1323:35–69.
14. Sime WT, Biazin H, Zeleke TA, et al. Urinary tract infection in cancer patients and antimicrobial susceptibility of isolates in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. PLoS One. 2020;15(12):e0243474. doi:10.1371/journal.pone.0243474
15. Ahmadi M, Ranjbar R, Behzadi P, et al. Virulence factors, antibiotic resistance patterns, and molecular types of clinical isolates of Klebsiella Pneumoniae. Expert Rev Anti Infect Ther. 2022;20(3):463–472. doi:10.1080/14787210.2022.1990040
16. Lee DS, Lee CB, Lee SJ. Prevalence and risk factors for extended spectrum Beta-lactamase-producing uropathogens in patients with urinary tract infection. Korean J Urol. 2010;51(7):492–497. doi:10.4111/kju.2010.51.7.492
17. Nanayakkara AK, Boucher HW, Fowler JVG, et al. Antibiotic resistance in the patient with cancer: escalating challenges and paths forward. CA Cancer J Clin. 2021;71(6):488–504. 11. doi:10.3322/caac.21697
18. Calbo E, Romaní V, Xercavins M, et al. Risk factors for community-onset urinary tract infections due to Escherichia coli harbouring extended-spectrum beta-lactamases. J Antimicrob Chemother. 2006;57(4):780–783. doi:10.1093/jac/dkl035
19. Behzadi P, Behzadi E. The microbial agents of urinary tract infections at central laboratory of Dr. Shariati Hospital, Tehran, Iran. Turk Klin Tip Bilim. 2008;28(4):445–449.
20. Medina M, Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol. 2019;11(11):1756287219832172. doi:10.1177/1756287219832172
21. Sarshar M, Behzadi P, Ambrosi C, et al. FimH and anti-adhesive therapeutics: a disarming strategy against uropathogens. Antibiotics. 2020;9(7):397. doi:10.3390/antibiotics9070397
22. Kalluru S, Eggers S, Barker A, et al. Risk factors for infection with multidrug-resistant organisms in Haryana, India. Am J Infect Control. 2018;46(3):341–345. doi:10.1016/j.ajic.2017.08.021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Socioeconomic Disparity Trends in End-of-Life Care for Cancer and Non-Cancer Patients: Are We Closing the Gap?
Vestergaard AHS, Christiansen CF, Neergaard MA, Valentin JB, Johnsen SP
Clinical Epidemiology 2022, 14:653-664
Published Date: 4 May 2022
Current Advances in Nanocarriers for Cancer Therapy
Zeinali R, Zaeifi D, Zolfaghari-Moghaddam SY, Paul MK, Biazar E
International Journal of Nanomedicine 2025, 20:12217-12262
Published Date: 7 October 2025
Key Nano-Strategies for Cisplatin Resistance in Advancing Anti-Cancer Therapy
Lei SY, Qin H, Liu S, Sheng J
International Journal of Nanomedicine 2025, 20:13255-13292
Published Date: 3 November 2025
KRT17: A Key Driver of Cancer Therapy Resistance and Emerging Therapeutic Target
Hou W
Cancer Management and Research 2025, 17:2705-2717
Published Date: 1 December 2025