")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Prevalence and Predictors of Hypovitaminosis D in Ethiopian HIV-Infected Adults
Authors Belete AM , Tefera AA , Getnet M , Asefa A , Aynalem YA , Shiferaw WS
Received 22 October 2021
Accepted for publication 6 December 2021
Published 22 December 2021 Volume 2021:13 Pages 1101—1109
DOI https://doi.org/10.2147/HIV.S345827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Abebe Muche Belete,1 Alemu Adela Tefera,1 Mekasha Getnet,2 Adisu Asefa,1 Yared Asmare Aynalem,2 Wondimeneh Shibabaw Shiferaw2
1Biomedical Department, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Nursing, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Abebe Muche Belete Email [email protected]
Background: Hypovitaminosis D is associated with bone fracture and cardiovascular disease in patients receiving antiretroviral therapy. Currently, there are few data on the magnitude of hypovitaminosis D in people living with HIV in Sub-Saharan country. Therefore, the present study determines the magnitude of hypovitaminosis D in people living with HIV and its associated factors in Ethiopia.
Methods: A cross-sectional study was conducted among 171 adult people living with HIV at Debre Berhan Specialized Hospital. Serum vitamin D was measured. Multivariate logistic regression analysis and p-value < 0.05 was used to identify the associated factors of hypovitaminosis D.
Results: In the present study, the prevalence of hypovitaminosis D was 129/171 (75.4%), with 11/171 (6.4%) having vitamin D deficiency and 118/171 (69%) having vitamin D insufficiency. Female sex was significantly associated with hypovitaminosis D (AOR: 3.01, 95% CI = 1.381– 6.561, P = 0.006).
Conclusion: Our study found a high burden of hypovitaminosis D among adult people living with HIV on antiretroviral therapy. Female sex was associated with hypovitaminosis D.
Keywords: vitamin D, HIV, antiretroviral therapy, Ethiopia
Background
Hypovitaminosis D is a widespread health problem in the general population as well as in people living with HIV (PLHIV). For example, USA-70.3%,1 New York City-21.2%,2 South-Central United States – 64%,3 Spain – 71.6%,4 and Uganda – 77%.5
Hypovitaminosis D status is a known risk factor for bone fracture and low bone mineral density,6,7 coronary artery disease,8 atherosclerosis,9–11 insulin resistance and type-2 diabetes12 and neurocognitive impairment13 in people living with HIV. Additionally, hypovitamin D status is also associated with tuberculosis.14,15
Possible established risk factors for hypovitaminosis D have been identified in PLHIV individuals. Some of these are common to the general population, whereas others are related to HIV itself. The presence of dark skin,16 female,17 old age,16,17 high body mass index (BMI), black race,16 winter season16 and HAART.18 In particular, Efavirenz treatment has been associated with low vitamin D status.17,19 Besides, longer duration of ART, CD4 count <200/μL and advanced stages of disease were independently associated with hypovitaminosis D status.20
Currently, there are few data on the magnitude of vitamin D status in PLHIV in sub-Saharan Africa. Most studies of vitamin D status with HIV represent populations from developed countries. The treatment disparities combined with differences in demographics, lifestyle, and nutritional status between Ethiopian and Western populations, may make this population more susceptible to hypovitaminosis D. Therefore, the present study will determine the magnitude of hypovitaminosis D in HIV patients and its associated factors in Ethiopia.
Methods and Materials
Study Setting and Design
This study was conducted at Debre Berhan Referral Specialized Hospital (DRSH), Debre Berhan, Ethiopia. The area is characterized by two seasonal climate; a dry season (November–May) and a rainy season (June–September), and ambient temperatures vary from 46°F in December to 69°F in May. A laboratory-based cross-sectional study design was employed among adult people living with HIV on ART, and the study period was from January 1 to 30, 2021.
Study Population and Sample
All Adult PLHIV. A convenient sampling technique was used to include a total of 171 adult PLHIV individuals visiting the selected hospital during the data collection period from January 1 to 30, 2021.
Inclusion and Exclusion Criteria
All Adult PLHIV aged ≥18 years old and treated with ART for at least 6 months were included in the study. Study participants with mental health problems, hearing impairments or any other serious health problems and those patients who would not be able to provide the appropriate information and pregnant women were excluded.
Study Variables
Independent Variables
Age, sex, smoking status, alcohol use, physical exercise, CD4 count, duration on HAART, duration of HIV-infection since first diagnosis, anthropometric indicators, use of corticosteroid, multivitamin take, Crhons ds, suns cream use, sun exposure, use of tanning booth, comorbidities, diarrhea in the past 2 week, Rheumatoid arthritis, and HBV/HCV coinfection.
Dependent Variable
Serum vitamin D status.
Operational Definition
Alcoholic beverage drinkers: Individuals were classified as follows: those drinking on average one or more drink(s) daily; those drinking 4 to 6 drinks weekly; those drinking 1 to 3 drinks weekly; and those drinking less than one drink weekly. (One drink is defined as one bottle of beer, one glass of wine or one shot of liquor).
No drinkers: Individuals who are not currently drinking, and have never drunk alcoholic beverages at all.
Adherence rate is measured based on missed doses per month. The percentage of ARV taken is used as a criterion to classify drug adherence (Good is defined as ≥95% of doses taken as prescribed, Fair defined as 85–94% of doses taken, and poor defined as <85% of doses taken).
Other medications: Participants were taking additional medication other than ART.
Comorbidities were defined as medical conditions clinically diagnosed and present at the time of data collection.
Data Collection and Procedure
Participant age, sex, date of the first HIV-sero positive test, last CD4+ cell count, and any viral load determinations were obtained from the participant’s hospital card. Questionnaire-driven interviews were performed by a trained nurse at the DRSH HIV clinic. Self-reported personal and familial history of heart fracture, kidney disease, diabetes, and self-reported alcohol and cigarette use were recorded.
First, the questionnaire was written in English and then translated to Amharic language. The questionnaire was retranslated into English by an expert to ensure its consistency. A half day of training was given to two senior nurses and laboratory technologists about the objective, methodology and ethical issues of the study. Two nurses collected data using a structured questionnaire and a checklist, and two laboratory technologists determined serum vitamin D levels. Pretest was done on 5% of the sample to check the validity of the questionnaire and the checklist. In addition, the completeness of the data was checked daily by the principal investigator.
Anthropometric Measurements
Body weight and height were measured. Weight was measured using a Tanita scale; patients were fully dressed, without heavy clothing or shoes, and height was determined without shoes using a portable stadiometer. Weight to the nearest 100 g and height to the nearest 1 mm were measured. Body mass index (BMI) was calculated by dividing weight (kg) by height (m2).21
Blood Sample Collection and Analysis
For determination of serum vitamin D, after overnight fasting, 5 mL venous blood samples were collected by phlebotomy laboratory technologist under aseptic conditions. A serum sample was immediately separated from the collected venous blood after the blood sample clotted and was centrifuged at 1000–2000 g for 10 minutes. The separated serum was transferred to a Nunc tube and kept frozen at −20°C until processed. Then, serum vitamin D was determined using ichroma vitamin D, which is a fluorescence immunoassay for the quantitative determination of total 25(OH) D2/D3 level and reported in ng/mL. Quality control was done. Vitamin D deficiency was defined as a 25(OH) D level of 20 ng/mL or less, insufficiency as 21–29 ng/mL, and sufficiency as 30 ng/mL or more. Hypovitaminosis D was defined as vitamin D insufficiency or deficiency (<30 ng/mL).22
Data Processing and Analysis
Data was checked, cleaned, and entered into Epi-data software version 4.2, and then exported to SPSS version 25.0 software for analysis. The results of the descriptive statistics were expressed as frequency and percentage. Univariate logistic regression was performed to examine the association of independent variables with hypovitaminosis D for all study participants using crude odds ratios (ORs) with 95% confidence intervals (CI). Those independent variables with a p-value <0.2 in univariate analysis were included in the multivariable logistic regression models. P-value <0.05 on multivariable logistic regression was considered as a statistically significant association.
Result
General Characteristics of Study Participants
One hundred and seventy-one adult people living with HIV participated in this study. Out of this, 107/171 (62.6%) were female and 90/171 (52.6%) of the study participants fall in the age group between 31 and 43 years. The duration of HIV since the first diagnosis greater than 7 year is 102/171 (59.6%), years on HAART > 6 years is 124/171 (72.5%). Most of the study participants taking TDF/3TC/DTG-based regimen 110/171 (64.3%) and 131/171 (76.6%) had undetectable viral load. In the present study, we collect independent variables that may contribute to hypovitaminosis D in the body. Accordingly, we found 34/171 (19.9%) of the study participants use suns cream, and 45/171 (26.3%) use of tanning booth (Table 1).
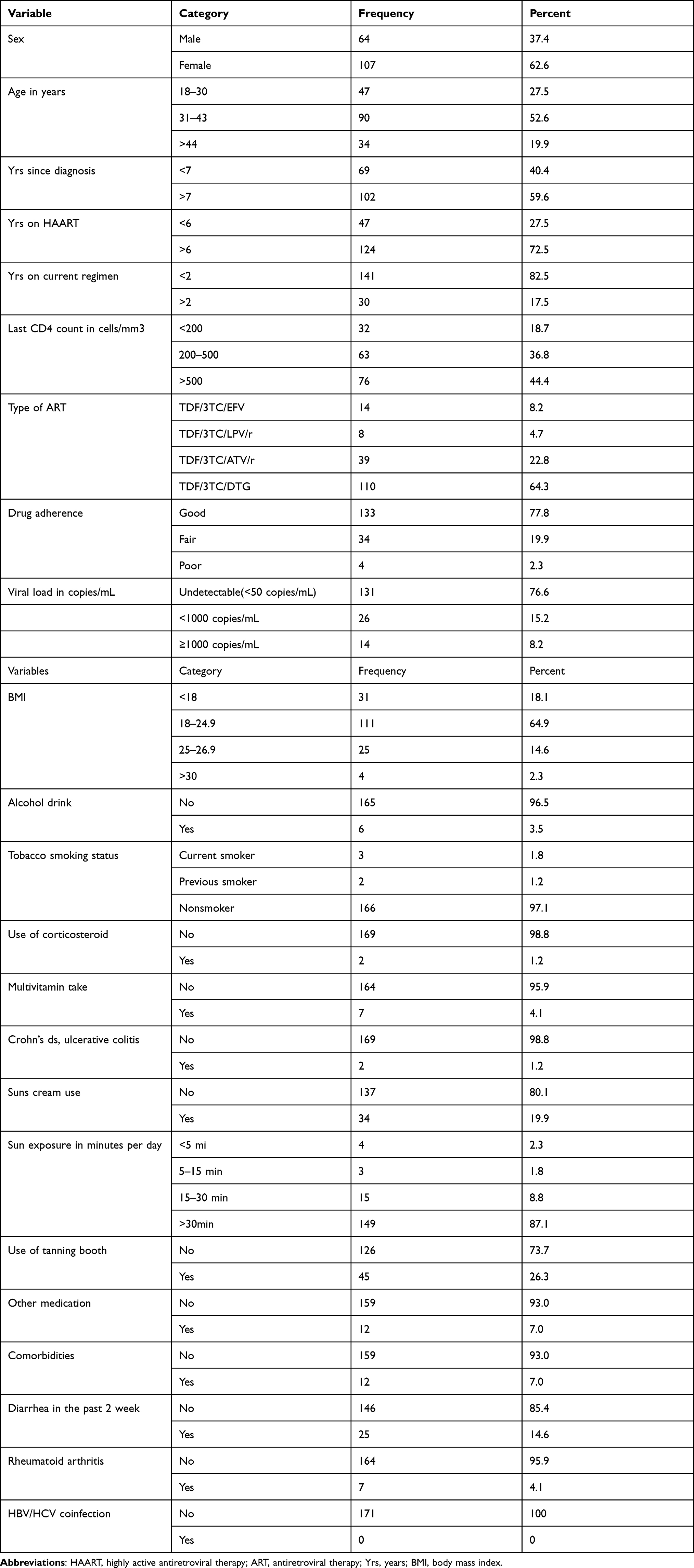 |
Table 1 General Characteristics of Study Participants at HIV Clinic of DBSH, Debre Berhan, Ethiopia, 2021 |
Prevalence of Hypovitaminosis D and Its Associated Factors
The prevalence of hypovitaminosis D was 129/171 (75.4%), with 11/171 (6.4%) having vitamin D deficiency and 118/171 (69%) having vitamin D insufficiency.
In the bivariate logistic regression analysis, female sex, physical exercise, use of sunscreen and use of tanning booth, were significantly associated with hypovitaminosis D (P < 0.05). When these variables were entered and analyzed in a multivariate logistic regression, only female sex was significantly associated with hypovitaminosis D (AOR: 3.01, 95% CI = 1.381–6.561, P = 0.006) (Table 2).
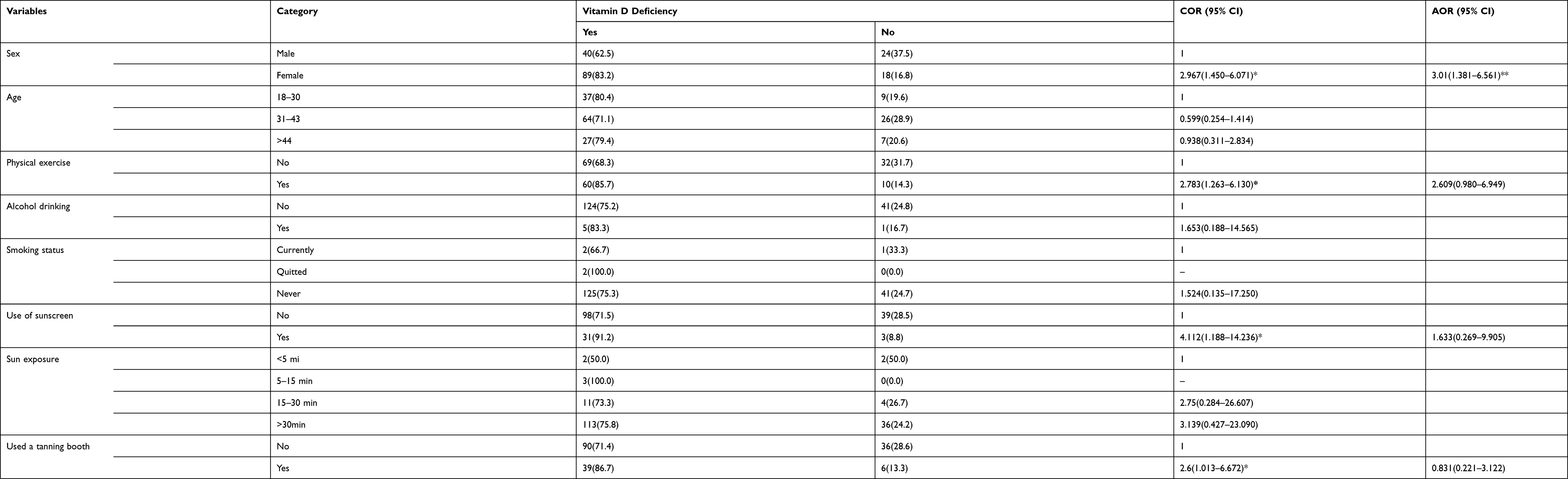 |
Table 2 Bivariate and Multivariate Logistic Regression Analysis of Vitamin D Deficiency with Independent Variables, Adult HIV Patients at DBSH, Debre Berhan, Ethiopia, 2021 |
Discussion
The present study assesses the prevalence of hypovitaminosis D and its associated factor in PLHIV on ART. In this study, hypovitaminosis D was 75.4%. This finding was similar with the findings of a study conducted in USA-70.3%,1 Spain-71.6%,4 Milwaukee-73%,23 Uganda-77%,5 Thailand-71.7%24 and Bangkok-Thailand 70.5%.17 However, the finding was lower than the results of studies done in India-92.63%25 and 89.2%,20 Michigan-95%,26 and France-86%.22 On the other hand, the result of the current study was higher than the finding of a study conducted in New York City-21.2%,2 South-Central United States-64%,3 Southern Australian-39%,27 Italy-47%,28 Latin American and Caribbean-65.7%,29 Kazakhstan- 65.1%,30 and Tanzania-52.8%.31 Additionally, the figure is also higher in non-HIV subjects. For example, a study conducted in Kenya 60%,32 and Cameron 25.8%33 had hypovitaminosis D. The difference observed here might be due to sample size variation, study population and design, and weathers of the study conducted.
The prevalence of hypovitaminosis D in our study is higher than compared to non-HIV subjects.
In the current study, female sex was significantly associated with hypovitaminosis D. This finding was consistent with other studies.17 Available data also showed that hypovitaminosis D can occur in young women, including those who are pregnant, with higher risk with advancing age in a woman’s lifecycle.34 One possible reason might be that females have more hypovitaminosis D, which is more because of heavily clades with clothes and limited outdoor activity and menopause. However, in contrast to this finding, other studies have not found an association of vitamin D to females.22,28 This discrepancy might be due to demographic difference and most of the study participants in this study were on efavirenz-based regimen.
Our study needs to be interpreted in the light of its limitations. This study is only conducted in only one referral hospital; therefore, data presented here may not be generalizable to all HIV-infected persons in Ethiopia. Additionally, the sample size is also small. Convenient sampling technique brings in bias. Moreover, the study did not include a control group of HIV-uninfected persons which would have provided better insight into the role of HIV infection and antiretroviral drugs on vitamin D levels.
Conclusion
Our study found a high prevalence of hypovitaminosis D among adult PLHIV on ART. Female sex was associated with hypovitaminosis D. A prospective cohort study with long follow-up and large sample size is recommended to pinpoint the prevalence of hypovitaminosis D and its associated factors.
Abbreviations
ART, Anti-Retroviral Therapy; ATV/r, Ritonavir-boosted atazanavir; BMI, Body Mass Index; CD4, Cluster of Differentiation four; DTG, Dolultegravir; DBSH, Debre Berhan Specialized Hospital, EFV, Efavirenz; HAART, Highly Active Anti-Retroviral Therapy; HIV, Human Immune Deficiency Virus; LPV/r, Ritonavir-boosted lopinavir; SPSS, Statistical Package for Social Sciences; PLHIV, People living with HIV.
Data Sharing Statement
The data used to support the findings of this study are included in the article.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the ethical review committee of College of Health Science Debre Berhan University with institutional research ethics review committee number of (IRB protocol: DBU/CHS/MN/SG12/2020). Collaboration letter for data collection was also obtained from Debre Berhan Referral Hospital. The objective of the study was briefly clarified and explained for each participant, before enrolling any of the eligible study participants. Samples and data were collected after informed consent had been obtained from the study participants. To assure confidentiality, a code number was used instead of the participants’ name or identification number. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
First of all, we want to give appreciation to Debre Berhan University, College of Health Science research coordination office for giving us this chance to participate in the research activity. We would like to thank the data collectors, and supervisors who were involved in this study and spent their valuable time responding to our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Debre Berhan University with project Code: GOV/DBU/TH12/CHS/N/03/20. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Dao CN, Patel P, Overton ET, et al. Low vitamin D among HIV-infected adults: prevalence of and risk factors for low vitamin D levels in a cohort of HIV-infected adults and comparison to prevalence among adults in the US general population. Clin Infect Dis. 2011;52(3):396–405. doi:10.1093/cid/ciq158
2. Kim JH, Gandhi V, Psevdos G, Espinoza F, Park J, Sharp V. Evaluation of vitamin D levels among HIV-infected patients in New York city. AIDS Res Hum Retroviruses. 2012;28(3):235–241. doi:10.1089/aid.2011.0040
3. Crutchley RD, Gathe J, Mayberry C, Trieu A, Abughosh S, Garey KW. Risk factors for vitamin D deficiency in HIV-infected patients in the south central United States. AIDS Res Hum Retroviruses. 2012;28(5):454–459. doi:10.1089/aid.2011.0025
4. Cervero M, Agud JL, García-Lacalle C, et al. Prevalence of vitamin D deficiency and its related risk factor in a Spanish cohort of adult HIV-infected patients: effects of antiretroviral therapy. AIDS Res Hum Retroviruses. 2012;28(9):963–971. doi:10.1089/aid.2011.0244
5. Ezeamama AE, Guwatudde D, Wang M, et al. Vitamin-D deficiency impairs CD4+T-cell count recovery rate in HIV-positive adults on highly active antiretroviral therapy: a longitudinal study. Clin Nutr. 2016;35(5):1110–1117. doi:10.1016/j.clnu.2015.08.007
6. Saccomanno MF, Ammassari A. Bone disease in HIV infection. Clin Cases Miner Bone Metab. 2011;8(1):33–36.
7. Premaor MO, Compston JE. The hidden burden of fractures in people living with HIV. JBMR Plus (WOA). 2018;2(5):247–256. doi:10.1002/jbm4.10055
8. Lai H, Fishman EK, Gerstenblith G, et al. Vitamin D deficiency is associated with development of subclinical coronary artery disease in HIV-infected African American cocaine users with low Framingham-defined cardiovascular risk. Vasc Health Risk Manag. 2013;9:729–737. doi:10.2147/VHRM.S50537
9. Cheru LT, Saylor CF, Fitch KV, et al. Low vitamin D is associated with coronary atherosclerosis in women with HIV. Antivir Ther. 2019;24(7):505–512. doi:10.3851/IMP3336
10. Calza L, Borderi M, Granozzi B, et al. Vitamin D insufficiency is associated with subclinical atherosclerosis in HIV-1-infected patients on combination antiretroviral therapy. HIV Res Clin Pract. 2019;20(6):131–139. doi:10.1080/25787489.2020.1724749
11. Portilla J, Moreno-Pérez O, Serna-Candel C, et al. Vitamin D insufficiency and subclinical atherosclerosis in non-diabetic males living with HIV. J Int AIDS Soc. 2014;17(1):18945. doi:10.7448/IAS.17.1.18945
12. Alvarez JA, Ashraf A. Role of vitamin D in insulin secretion and insulin sensitivity for glucose homeostasis. Int J Endocrinol. 2010;2010:351385. doi:10.1155/2010/351385
13. Vergori A, Pinnetti C, Lorenzini P, et al. Vitamin D deficiency is associated with neurocognitive impairment in HIV-infected subjects. Infection. 2019;47(6):929–935. doi:10.1007/s15010-019-01313-6
14. Sudfeld CR, Mugusi F, Muhihi A, et al. Efficacy of vitamin D(3) supplementation for the prevention of pulmonary tuberculosis and mortality in HIV: a randomised, double-blind, placebo-controlled trial. Lancet HIV. 2020;7(7):e463–e471. doi:10.1016/S2352-3018(20)30108-9
15. Sudfeld CR, Mugusi F, Aboud S, Nagu TJ, Wang M, Fawzi WW. Efficacy of vitamin D(3) supplementation in reducing incidence of pulmonary tuberculosis and mortality among HIV-infected Tanzanian adults initiating antiretroviral therapy: study protocol for a randomized controlled trial. Trials. 2017;18(1):66. doi:10.1186/s13063-017-1819-5
16. Hidron AI, Hill B, Guest JL, Rimland D. Risk factors for vitamin D deficiency among veterans with and without HIV infection. PLoS One. 2015;10(4):e0124168. doi:10.1371/journal.pone.0124168
17. Avihingsanon A, Kerr SJ, Ramautarsing RA, et al. The association of gender, age, efavirenz use, and hypovitaminosis D among HIV-infected adults living in the tropics. AIDS Res Hum Retroviruses. 2016;32(4):317–324. doi:10.1089/aid.2015.0069
18. Madeddu G, Spanu A, Solinas P, et al. Bone mass loss and vitamin D metabolism impairment in HIV patients receiving highly active antiretroviral therapy. Q J Nucl Med Mol Imaging. 2004;48(1):39–48.
19. Missailidis C, Höijer J, Johansson M, et al. Vitamin D status in well‐controlled caucasian HIV patients in relation to inflammatory and metabolic markers–a cross‐sectional cohort study in Sweden. Scand J Immunol. 2015;82(1):55–62. doi:10.1111/sji.12299
20. Theodorou M, Sersté T, Van Gossum M, Dewit S. Factors associated with vitamin D deficiency in a population of 2044 HIV-infected patients. Clin Nutr. 2014;33(2):274–279. doi:10.1016/j.clnu.2013.04.018
21. World Health Organization. Obesity: preventing and managing the global epidemic; 2000.
22. Allavena C, Delpierre C, Cuzin L, et al. High frequency of vitamin D deficiency in HIV-infected patients: effects of HIV-related factors and antiretroviral drugs. J Antimicrob Chemother. 2012;67(9):2222–2230. doi:10.1093/jac/dks176
23. Bearden A, Abad C, Gangnon R, Sosman JM, Binkley N, Safdar N. Cross-sectional study of vitamin D levels, immunologic and virologic outcomes in HIV-infected adults. J Clin Endocrinol Metab. 2013;98(4):1726–1733. doi:10.1210/jc.2012-4031
24. Wiboonchutikul S, Sungkanuparph S, Kiertiburanakul S, et al. Vitamin D insufficiency and deficiency among HIV-1-infected patients in a tropical setting. J Int Assoc Provid AIDS Care. 2012;11(5):305–310. doi:10.1177/1545109711432142
25. Deshwal R, Arora S. High prevalence of vitamin D deficiency in HIV infected on antiretroviral therapy in a cohort of Indian patients. J Assoc Physicians India. 2019;67(3):42–45.
26. Poowuttikul P, Thomas R, Hart B, Secord E. Vitamin D insufficiency/deficiency in HIV-infected inner city youth. J Int Assoc Provid AIDS Care. 2014;13(5):438–442. doi:10.1177/2325957413495566
27. Klassen KM, Fairley CK, Kimlin MG, Hocking J, Kelsall L, Ebeling PR. Vitamin D deficiency is common in HIV-infected southern Australian adults. Antivir Ther. 2016;21(2):117–125. doi:10.3851/IMP2983
28. Vescini F, Cozzi-Lepri A, Borderi M, et al. Prevalence of hypovitaminosis D and factors associated with vitamin D deficiency and morbidity among HIV-infected patients enrolled in a large Italian cohort. J Acquir Immune Defic Syndr. 2011;58(2):163–172. doi:10.1097/QAI.0b013e31822e57e9
29. Jao J, Freimanis L, Mussi-Pinhata MM, et al. Low vitamin D status among pregnant Latin American and Caribbean women with HIV Infection. Int J Gynaecol Obstet. 2015;130(1):54–58. doi:10.1016/j.ijgo.2015.01.017
30. Nugmanova ZS, Patel N, Akhmetova GM, et al. Relationship between vitamin D and human immunodeficiency virus (HIV) viral load among HIV-infected patients in Kazakhstan. J Infect Dev Ctries. 2015;9(11):1277–1283. doi:10.3855/jidc.6808
31. Sudfeld CR, Wang M, Aboud S, Giovannucci EL, Mugusi FM, Fawzi WW. Vitamin D and HIV progression among Tanzanian adults initiating antiretroviral therapy. PLoS One. 2012;7(6):e40036. doi:10.1371/journal.pone.0040036
32. Kagotho E, Omuse G, Okinda N, Ojwang P. Vitamin D status in healthy black African adults at a tertiary hospital in Nairobi, Kenya: a cross sectional study. BMC Endocr Disord. 2018;18(1):1–7. doi:10.1186/s12902-018-0296-5
33. Tangoh DA, Apinjoh TO, Mahmood Y, et al. Vitamin D status and its associated risk factors among adults in the Southwest region of Cameroon. J Nutr Metab. 2018;2018:1–9. doi:10.1155/2018/4742574
34. Khadilkar SS. The emerging role of vitamin D3 in women’s health. J Obstet Gynaecol India. 2013;63(3):147–150. doi:10.1007/s13224-013-0420-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.