Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 13
Prevalence and Parental Attitude Toward Nitrous-Oxide and Papoose-Board Use in Two Dental Referral Centers in Saudi Arabia: A Cross-Sectional Study
Authors Sabbagh HJ ![]() , Turkistani JM
, Turkistani JM ![]() , Alotaibi HA, Alsolami AS, Alsulami WE, Abdulgader AA, Bagher SM
, Alotaibi HA, Alsolami AS, Alsulami WE, Abdulgader AA, Bagher SM ![]()
Received 19 September 2021
Accepted for publication 3 December 2021
Published 24 December 2021 Volume 2021:13 Pages 531—539
DOI https://doi.org/10.2147/CCIDE.S340158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Heba J Sabbagh,1 Jihan M Turkistani,2 Hadeel A Alotaibi,3 Abrar S Alsolami,3 Waad E Alsulami,4 Areej A Abdulgader,5 Sara M Bagher1
1Department of Pediatric Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 2King Abdulaziz Medical City, National Guard Health Affairs, Jeddah, Saudi Arabia; 3Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Pediatric Dentistry, Ministry of Health, Jeddah, Saudi Arabia; 5Department of Restorative Dentistry, Princess Noura University, Riyadh, Saudi Arabia
Correspondence: Heba J Sabbagh
Department of Pediatric Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Tel +96655668481
Email [email protected]
Background: Parental preferences and attitudes strongly influence dentists’ choices for managing children’s behavior in clinics. This study aimed to assess parental attitudes toward two behavior management technique (BMTs)—nitrous oxide (N2O) sedation and/or protective passive stabilization by papoose board (PB)—before and after their children received dental treatment at two referral centers in Jeddah, Saudi Arabia.
Methods: Participants were parents of healthy children who required dental treatment under N2O and/or PB over an 18-month period. Before and after dental treatment, parents answered a questionnaire on their attitudes toward BMTs used on their children. Parents were divided into three groups: Group 1 (parents of children who received N2O), Group 2 (parents of children who received PB), and Group 3 (parents of children who received both N2O and PB).
Results: Out of the 132 parents who answered the questionnaire, 106 (80.3%) were in Group 1, 10 (7.6%) in Group 2, and 16 (12.1%) in Group 3. More children of parents with low monthly family incomes were in Group 3 than Group 1 compared to other family-incomes.
Conclusion: Parental attitudes toward N2O and/or PB improved after their children experienced BMTs. The future use of PB alone with their child’s sibling was parents’ least preferred BMT (p = 0.001).
Keywords: attitude, nitrous oxide, papoose board, protective stabilization, sedation
Introduction
One of the most challenging aspects of being a pediatric dentist is managing anxious and fearful children.1 Those children are usually uncooperative and sometimes require more advanced behavior management techniques (BMTs) to provide the proper treatment required and promote positive attitudes toward dental health care.2
The American Academy of Pediatric Dentistry (AAPD) has classified BMTs into two main categories: basic and advanced techniques.2 Basic BMTs include tell-show-do (TSD), distraction, positive reinforcement, voice control, nitrous oxide (N2O), and parental presence/absence.2 However, for some children, basic techniques may be inadequate for managing their behaviors, and more advanced techniques are required. Advanced BMTs include protective stabilization, sedation, and general anesthesia (GA).2
The AAPD defines protective stabilization as restraining a patient’s freedom of movement by either involving others or by the use of a patient stabilization device, such as a papoose board (PB).2 Parents’ acceptance and understanding of BMTs play crucial roles in dentists’ choices, and therefore in the success of the dental treatment provided.3 Nevertheless, different BMTs undergo annual reassessment by the pediatric dental organizations, where some are discouraged. One of the main reasons behind these changes is parental attitude and acceptance,4–7 which highlights the importance of understanding parental attitude to a behavior management technique.
Previous studies have investigated parental attitudes toward different BMTs in hypothetical situations in which parents were asked to rate their level of acceptance after watching videos3,8–10 or PowerPoint presentations11 of different BMTs. Most previous studies reported that TSD was the most accepted BMT,3,8,9,11 while other pharmacological BMTs, including N2O,8,9 GA,11 and physical restraints, were among parents’ least preferred BMTs.3,9 However, a study conducted by Patel et al reported that more parents preferred pharmacological management over protective stabilization,10,12 which indicated a shift in parental preferences among younger generations. Furthermore, a qualitative study that interviewed parents after their children were treated under PB reported different parental opinion that is related to the dentist's communication, explanation and involvement of parents in decision-making.13
Additionally, parents from different populations could have different attitude toward the BMTs that rely on their background and other surrounding factors that might affect their decision.14 A previous study conducted in 1991 and investigated parental attitudes toward PB after the technique was used with their children. The study reported a high level of maternal acceptance, reaching up to 90%.15 Moreover, Peretz et al,16 in 1999 reported that parental acceptance of certain BMTs, such as voice control and sedation, would increase after their children had been treated using those BMTs.16 In Saudi Arabia, Al-Shalan et al reported in 2003 that parental age, child gender, and number of siblings had an influence on parental acceptance of different BMTs used for their children. Further, they reported deficiencies in parental awareness regarding the importance of different BMTs.17
Therefore, assessing the use of different BMTs and parental attitude toward these BMTs are essential in different populations with different cultural background.
The aims of the study include: (Part-1) to assess the prevalence of two behavior management techniques (BMTs) (nitrous oxide (N2O) sedation and protective passive stabilization using a papoose board (PB)); and (Part-2) to compare parental attitudes toward those two BMTs before and after their children received dental treatment under N2O and/or PB at two referral centers in Jeddah, Saudi Arabia.
Materials and Methods
Participants
This prospective cross-sectional study was conducted in the pediatric dental clinics at King Abdulaziz University Hospital (KAUH) and King Abdulaziz Medical City (KAMC), in Jeddah, Saudi Arabia; which are the two main referral centers that provide dental treatment for their pediatric dental patients under N2O and/or PB. The study was carried out between January 2018 and June 2019.
Sample size was calculated using OpenEpi online calculator with 80% power, 108 parents are required to analyze the proportions in a population of 800 with a 25% exposure.
All healthy two to-12-year-old children receiving dental treatment by a pediatric dentist during the study period in one of the included centers were eligible. Parents of children who received only N2O “Group I”; received only PB “Group II”; and received both N2O and PB “Group III” were identified (see Figure 1).
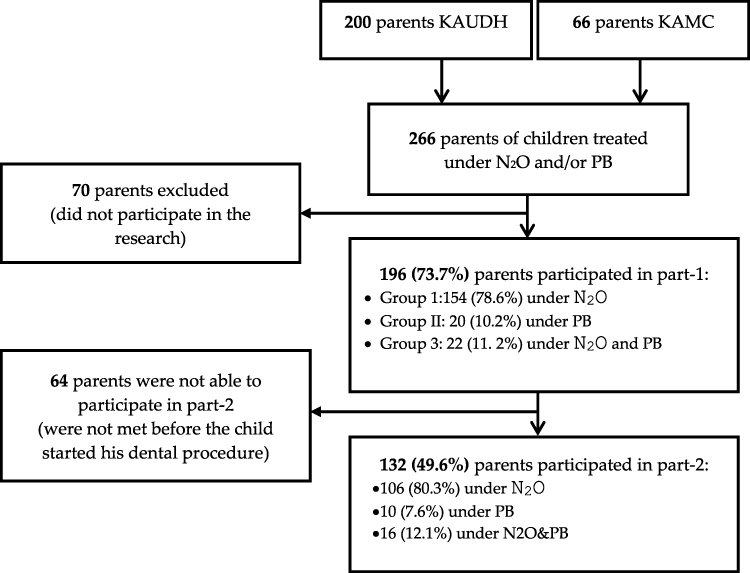 |
Figure 1 Sample flow chart. Abbreviations: KAUDH, King Abdulaziz University Faculty of Dentistry; KAMC, King Abdulaziz Medical City; N2O, nitrous oxide; PB, papoose board. |
Inclusion criteria included parents of healthy two to-12-year-old children that required dental treatment under N2O and/or PB because of their behavior. Parents of children with mental or physical disabilities were excluded from the study. Some additional inclusion for part-2 of the study were that the data collector needs to reach the patients’ parents before their children starts their dental procedure and that parents were with no previous experience of N2O or PB. If the data collector failed to reach the parents before their children started their dental treatment under the N2O or/and PB, they were excluded from part-2 of the study.
Procedure
Ethical approval obtained from the Research Ethics Committee at KAUDH (086-10-17). Eligible subjects were approached by one of the trained dentists, and the aim and methodology of the study were presented. If they agreed, an Arabic consent form was signed by the participating parents.
For part-1 of the study, healthy 2–12-years-old children who received dental treatment under N2O and/or PB during the study period were compared to the total treated children in the same included centers to assess the prevalence.
The Validated Arabic questionnaire was constructed based on two previously published articles15,18 and was modified according to the evaluation of two experts in the field. Then, for face validity, 10 representative parents were interviewed and asked to report whether they faced any difficulty understanding or answering any of the asked questions, and the questions were modified accordingly. Cronbach’s α was used to assess the reliability of the questionnaire and was calculated to be 0.769.
The questionnaire comprised two sections; Section-1: included child’s sociodemographic data. The monthly family income was divided into four groups based on the overall monthly income, where a monthly income of less than 7000 Saudi Riyals (SR) was considered low; 7000 to 10,000 SR was middle; 10,000 to 16,000 SR was high, and more than 16,000 SR was very high. In addition, it included number of siblings and the reason for using the BMT. Section-2 of the questionnaire included three questions. The first two questions evaluated parental attitude toward the BMT/s before and after their children received dental treatment under N2O and/or PB. The third question was regarding parents’ future preferences for using the experienced BMTs with the child’s siblings, when needed. Parents answered the questions by selecting one of three choices of three levels Likert scale (Agree/Neutral/Disagree).
Section-1 of the questionnaire was answered by all the subjects, while Section-2 was answered by only parents who were reached before their children started their dental treatment under N2O and/or PB. If the trained data collector failed to interview parents before their children’s dental treatment under the selected BMT, or they had a previous experience, they were excluded from part-2 of the questionnaire. The questionnaire is presented in Supplementary Material 1.
Dental treatment done during the use of N2O and/or PB in this study were procedures that are considered painful, according to Ghanei et al.19 All of included children were injected with anesthesia that is considered the main cause of pain in pediatric dental patients; followed by restoration, extraction, pulp therapy, or stainless-steel crown.19
N2O and PB Use Protocol at KAUDH and KAMC
The protocol for patient selection and techniques for using N2O and/or PB at both KAUDH and KAMC were performed according to AAPD guidelines.5 This includes, using N2O when the child is fearful, or anxious, and using PB when the child has uncontrolled movement that might jeopardize the safety of the child or anyone surrounding him, if the child requires urgent treatment, if the child history of cooperation is rapidly changed from uncooperative to cooperative and uncooperative child who required minimal treatment and sedation or general anesthesia is not possible or contraindicated.
For KAMC, an additional Departmental Policy and Procedure is followed for dental treatment of children using N2O sedation on a prescheduled sedation appointment. The child must be sent to the Pre-Anesthesia Clinic for medical assessment and clearance by an anesthesiologist. Once the child is fit for N2O sedation, the pediatric dentist can pursue any planned dental procedure using N2O technique. Furthermore, on the day of the appointment, fasting status or NPO (ie, nothing by mouth) must be confirmed by the treating pediatric dentist in addition to clearance from any recent upper respiratory tract infection.
The selected BMT/s is/are then introduced to the children and parents using a positive approach. Communication with parents and children was established, and the PB was described to children as a “colorful chair” that keeps you warm through rapping and tiding it around you, and as “a shield” that protects you from harming yourself during dental treatment. Additionally, a brief verbal explanation including the rationale and implementation method of the selected BMT/s was provided. The children were continuously monitored throughout the procedure. Finally, parents were asked to sign an Arabic consent form before their children received dental treatment under the selected BMT/s. Parents have the freewill to refuse or accept the proposed BMT/s. Moreover, they were allowed to be present in the clinic during their children’s dental treatment under the selected BMT/s.
Statistical Analysis
Statistical analysis was performed using SPSS version 20. Descriptive statistics were displayed as frequencies and percentages for categorical variables or means and standard deviations (SD) for continuous variables. Chi-square tests were used with p < 0.05 and adjusted using post-hoc Bonferroni correction when assessing parental preference for N2O and/or PB. Additionally, a binary regression analysis was performed to assess significant relationships between predictors (child age, gender and parental socioeconomic status [education and monthly family income]) and child treatment under N2O alone (Group I) or PB with or without N2O (Group II and group III) as a dependent variable.
Results
A total of 266 (200 from KAUH and 66 from KAMC) children were treated under N2O and/or PB compared to 1903 children (850 from KAUH and 1053 from KAMC) visiting pediatric dental clinics for dental treatment during the study period (18-month). This gave an estimated frequency of 13.98% for using N2O and/or PB at both centers together; 23.52% at KAUH and 6.27% at KAMC.
Out of the total number of children treated under N2O and/or PB, 196 (73.7% response rate) agreed to participate in part-1 of the research: 154 (78.6%) were treated under N2O (Group I); 20 (10.2%) were treated under PB (Group II); and 22 (11. 2%) were treated under both N2O and PB (Group III) (see Figure 1). The mean (±SD) age of the children was 8.35 ±2.3. Although there were more females in Group I (88 (57.1%)) and Group II (14 (70.0%)) compared to males (66 (42.9%) and 6 (30.0%) respectively), the difference was not statistically significant (P=0.325). The most common reason for using N2O and/or PB was behavioral problems (85 (64.4%)), while multiple cavities were the reason for 41 (31.1%) children as presented in Table 1.
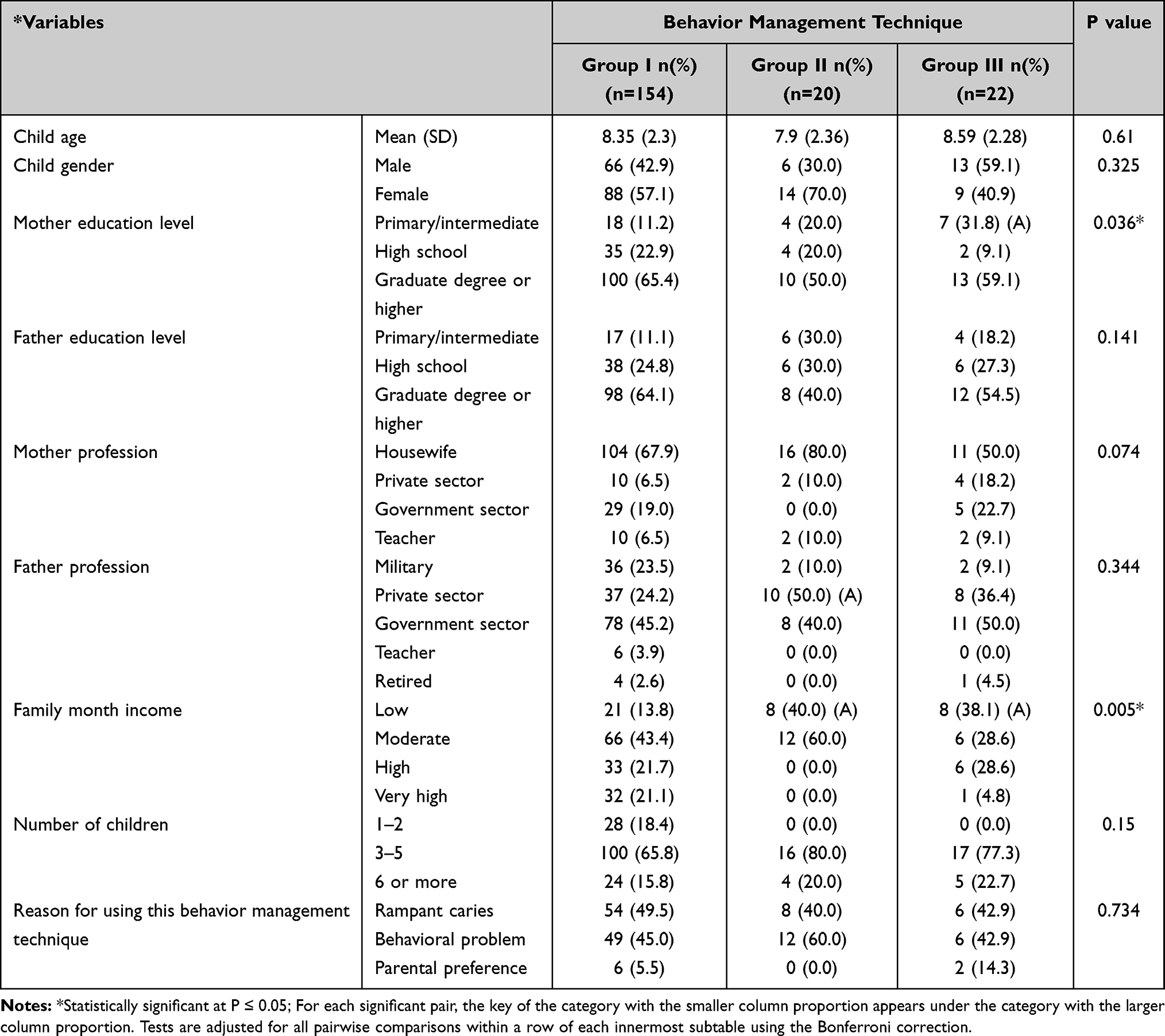 |
Table 1 Distribution of the Sample According to Type of Behavior Management Techniques Used and Sociodemographic Variables (N=196) |
Regarding socioeconomic status variables, 100 (65.4%) of the mothers and 98 (64.1%) of the fathers had received a bachelor’s degree or higher; 74 (69.8%) of the mothers were housewives and 53 (40.2%) of the families had a moderate family monthly income. None of the children in Group II were from families with high to very high family monthly incomes. Monthly family income and maternal education were statistically significantly related to the type of BMT used (P=0.005 and 0.036 respectively). When conducting Bonferroni corrections to adjust chi-square tests for family monthly income groups, there were statistically significantly more children of parents with a low family monthly income in Group II and III, compared to Group I. In addition, there were statistically significantly more children of mothers with primary/intermediate education treated with N2O and PB compared to those treated with N2O alone as presented in Table 1.
When assessing factors related to children in Group I compared to those in Group II and III grouped together as a dependent factor in binary regression, those with middle and high family monthly income were statistically significantly more treated under N2O compared to low family income (P=0.005, OR: 25.46 and 95% CI: 2.69 to 24.4 and P=0.029, OR: 10.197 and 95% CI: 1.26 to 82.34 respectively) (see Table 2).
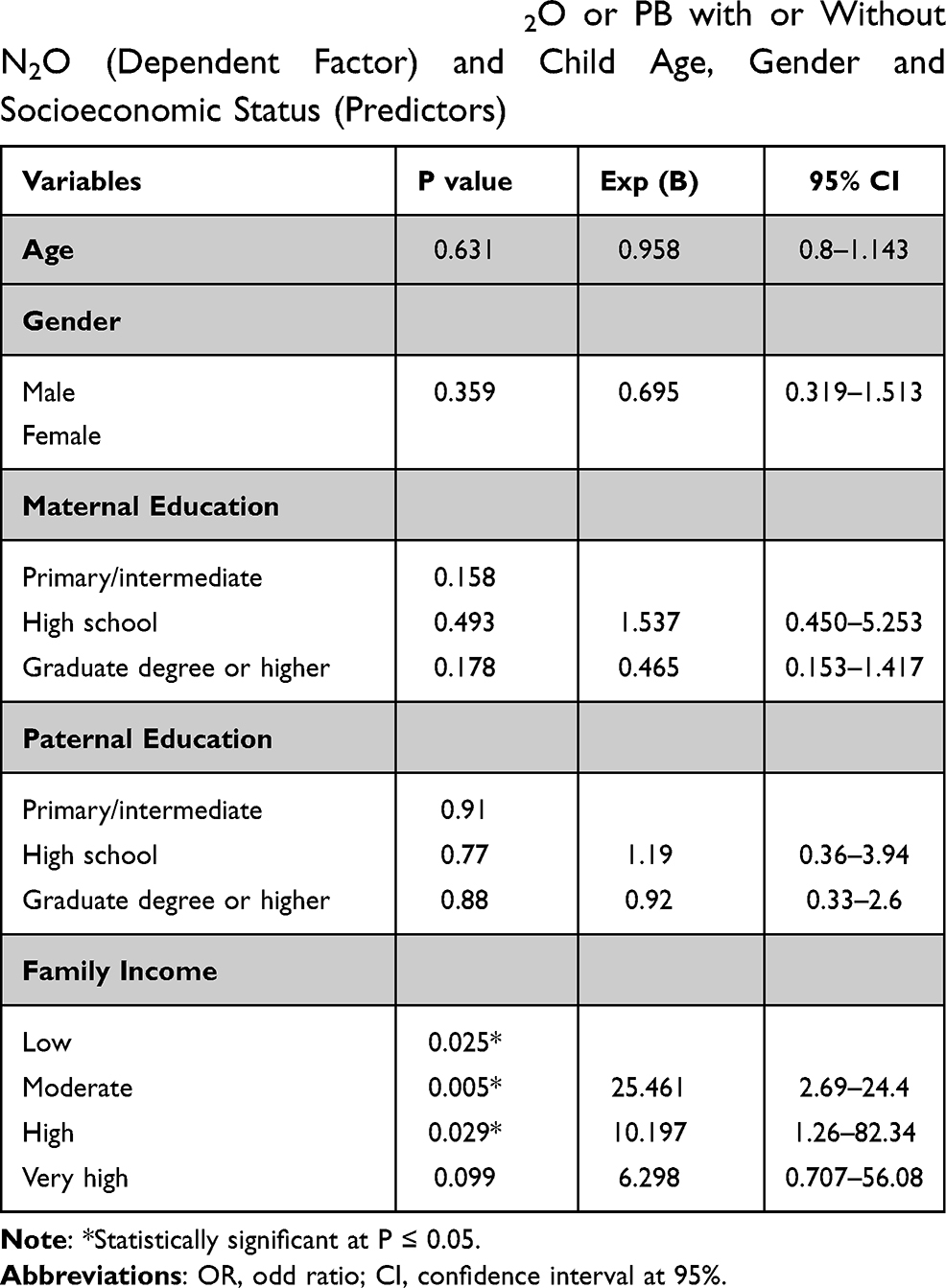 |
Table 2 Binary Regression Analysis Showing the Relationship Between Children Treated with N2O or PB with or Without N2O (Dependent Factor) and Child Age, Gender and Socioeconomic Status (Predictors) |
Out of the 196 children participating in Section-1 of the questionnaire, 64 parents were excluded from Section-2 (attitude questionnaire) because the trained data collector failed to interview parents before their children receive dental treatment under N2O and/or PB. Therefore, a total of only 132 parents participated in part-2 of the study (response rate = 49.62%). The mean (±SD) age of the children was 8.3 ±2.16, and 79 (59.8%) were female.
Before children received dental treatment under N2O and/or PB, 64 (60.4%) in Group I, 4 (40%) in Group II, and 12 (75%) in Group III of the parents reported no struggle and were more comfortable in selecting the BMTs, with no significant differences between the three groups (p=0.205). However, after treatment, more parents were comfortable in selecting the BMTs (102 (96.2%) in Group I, 10 (100%) in Group II, and 13 (81.2%) in Group III) (see Table 3). Nevertheless, after conducting Bonferroni corrections to adjust chi-square tests for the three groups, there were statistically significantly more parents comfortable in selecting N2O for their children (Group I), compared to N2O with PB (Group III). Moreover, 83 (62.9%) of the parents reported they would prefer N2O and/or PB for their other children, if they needed dental treatment. However, the use of PB alone with a sibling was statistically significantly less preferred by parents, compared to N2O with or without PB (P=0.001; Table 4).
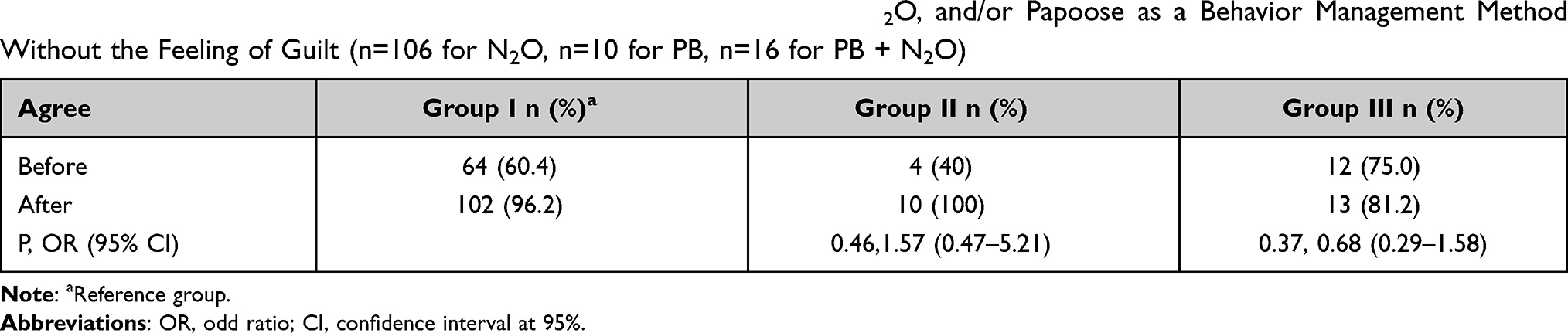 |
Table 3 Parental Agreement That They Were Comfortable in Using N2O, and/or Papoose as a Behavior Management Method Without the Feeling of Guilt (n=106 for N2O, n=10 for PB, n=16 for PB + N2O) |
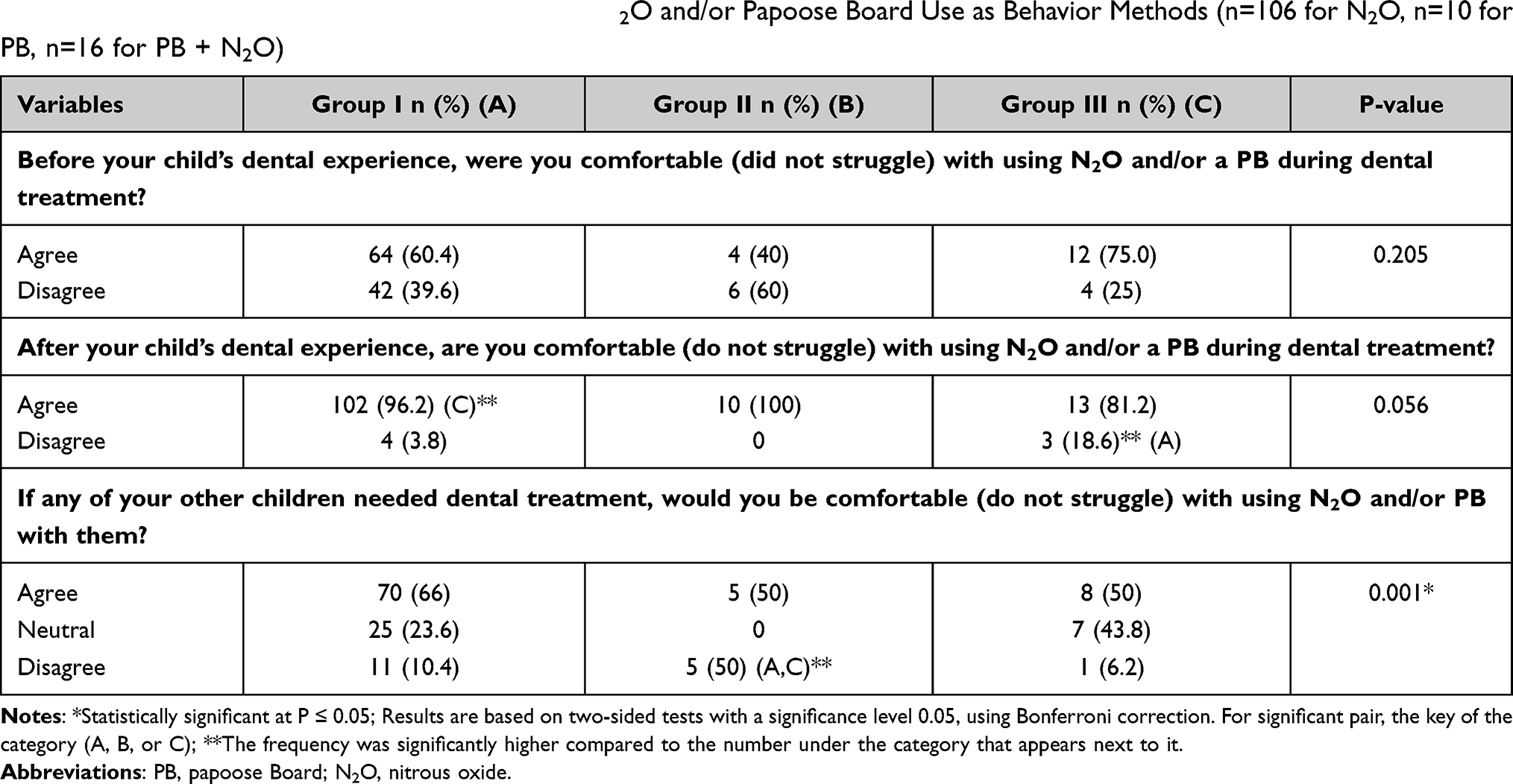 |
Table 4 Comparison of Parental Attitudes Between N2O and/or Papoose Board Use as Behavior Methods (n=106 for N2O, n=10 for PB, n=16 for PB + N2O) |
Discussion
This study was designed to understand the prevalence and parental attitudes toward two used BMTs for children. Previous studies reported limited parental acceptance toward the BMTs used in this study, especially PB.3,20 However, parents who participated in our study reported more positive attitudes toward these BMTs after their children experienced them during dental treatment.
The prevalence of children who were treated under N2O and/or PB at KAUH (23.54%), and at KAMC (6.27%) is lower than what was reported in former studies21–23 (80%). Similarly, Baakdah et al reported that 3% of children 18 years or less treated in KAMC experienced N2O sedation.24
Although recent studies reported changes in parental acceptance of BMTs,3,25 no recent reports on the prevalence of children receiving dental treatment under N2O and/or PB have been found in the literature.
Several factors contribute to the lower prevalence of children treated with N2O at KAMC. Following the hospital Departmental Policy and Procedure by sending the children to Pre-Anesthesia Clinic for clearance is an extra step that is not present at KAUDH. This step requires that a pre-determined date for the N2O should be scheduled according to availability of limited sedation slot, which constraint the use of N2O as BMT for providing dental treatment to candidate children. Furthermore, on the day of the N2O appointment, the child may present to the appointment with upper respiratory infection symptoms or not committed to the NPO requirement leading to more frequent cancellation rate.
Previous studies were conducted using various scales and methods to evaluate parental acceptance toward BMTs used in pediatric dentistry. In 2005, Eaton et al evaluated parental preferences for different BMTs, including N2O and active restraints, by asking them to answer a questionnaire after watching a video.3 The most acceptable technique when used separately was found to be TSD, and then N2O; while PB was the least acceptable. In 2019, Desai et al also evaluated parental preferences for different BMTs after showing them a video of different BMTs, and parents reported low acceptance of both N2O&PB.20 Nevertheless, one of the few studies that assessed parental attitudes toward PB after their first experience reported a high rate of parental acceptance, reaching over 90%.15 These findings are similar to our study that showed more positive parental attitudes toward N2O and/or PB after their children experienced these BMTs during dental treatment.
The high parental acceptance rate reported in this study could also be attributed to the fact that all the participants in this study were parents of children who received dental treatment under N2O and/or PB and had never experienced the selected BMTs before this study. In 1984, Fields et al reported that parents usually tend to accept the use of physical restraints, N2O and GA as BMTs on their children if it is for an emergency treatment, while they tend to disagree with their use during normal dental visits.26
Another explanation could be that all participants received a brief verbal explanation including the rationale and implementation of the selected BMTs. A study was conducted to assess parents’ knowledge of and attitudes toward the use of N2O as a BMT for their children and reported that two-thirds of the parents would accept N2O sedation if recommended by a dentist treating their children.27 Additionally, in 1991, Lawrence et al reported an improvement in parental acceptance of BMTs after they received a complete explanation of all types of BMTs, compared to parents who did not receive any explanations.28
As for factors that could influence parental acceptance of N2O and/or PB, previous studies reported no relationship between BMTs and socioeconomic status or age.3,29 In comparison to our study, none of the children from families with high monthly incomes received dental treatment under PB alone. This is comparable to a study conducted by Havelka et al, in which they reported that parents with low socioeconomic status tended to accept PB more than parents with high socioeconomic status.30 The authors explained this as an effect of other variables related to the study population; however, in the present study, dental treatment was provided for free at the included centers. Therefore, financial factors might not have directly affected parental preference. A statistically significant relationship between monthly family income and both parenting styles and children’s behaviors was reported by some previous studies, which might help to explain our findings.31–33
There are some limitations to the present study. First, the number of subjects for the use of PB alone was limited, due to the availability of cases. As PB is rarely used alone and only with selected cases according to AAPD guidelines,2 this could explain the 100% parental preference toward this BMT once their child experienced it. Although the data presented for PB should be considered a preliminary finding, it is important to report, as there is no recently published data that discusses parental attitudes and preferences toward PB, especially in Saudi Arabia.
Further, this study included two centers; however, these two centers are the main centers that provide N2O and PB for their pediatric dental patients and serve different types of population categories. Accordingly, we claim that the prevalence and outcome of Section-1 of the questionnaire could be generalized on the included population. Nevertheless, the response rate of Section-2 of the questionnaire limits its generalization. However, when calculating the sample size according to our results, using OpenEpi online calculator with 80% power, 108 parents are required to analyze the proportions in a population of 800 with a 25% exposure. Fortunately, the number of parents included in this study was “196” in part-1 and “132” in part-2, which exceeded the required calculated number. In addition, when looking at the sample distribution according to their socioeconomic status and gender, the sample of part-2 covers a similar distribution of included subgroups as part-1 of the study.
Future cohort studies with larger sample sizes are recommended to suggest the best methods for using these BMTs, with more definition and specification of the patient’s behavior, parental style and acceptance. In addition, the relationship between the type of dental treatment carried out to the patient and parental acceptance and preference to the BMTs used need to further analyzed.
This study’s clinical significance is that it helps directing the pediatric dentist on the selection of BMT by elaborating and assessing parental preference.
Conclusions
The frequency of N2O and/or PB use at two referral centers in Saudi Arabia was 14.36%. Parental attitudes toward N2O sedation and/or PB as BMTs improved after parents experienced BMTs with their children.
Data Sharing Statement
Data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Written informed consent was obtained from all participants’ guardians, and ethical approval was obtained from the ethics committee of KAUFD (086-10-17).
Consent for Publication
Written informed consent for publication was obtained from the participant’s guardian and approved by the KAUFD ethical committee. A copy of the consent form is available for review by the Editor of this journal if requested from the corresponding author.
Acknowledgment
We would like to acknowledge Rawaa Abduljabbar who participated in data entry. We would also like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elango I, Baweja D, Shivaprakash P. Parental acceptance of pediatric behavior management techniques: a comparative study. J Indian Soc Pedod Prev Dent. 2012;30(3):195–200. doi:10.4103/0970-4388.105010
2. American Academy of Pediatric Dentistry. Use of nitrous oxide for pediatric dental patients. The Reference Manual of Pediatric Dentistry; 2019–2020:293–298.
3. Eaton JJ, McTigue DJ, Fields HW, Beck M. Attitudes of contemporary parents toward behavior management techniques used in pediatric dentistry. Pediatr Dent. 2005;27(2):107–113.
4. American Academy of Pediatric Dentistry. Behavior Guidance for the Pediatric Dental Patient. The Reference Manual of Pediatric Dentistry. Chicago, Ill: American Academy of Pediatric Dentistry; 2020.
5. American Academy of Pediatric Dentistry. Use of Nitrous Oxide for Pediatric Dental Patients. The Reference Manual of Pediatric Dentistry. Chicago, Ill: American Academy of Pediatric Dentistry; 2020.
6. Roberts JF, Curzon ME, Koch G, Martens LC. Review: behaviour management techniques in paediatric dentistry. Eur Arch Paediatr Dent. 2010;11(4):166–174. doi:10.1007/BF03262738
7. Roberts JF, Curzon MEJ, Koch G, Martens LC. Behaviour management techniques in paediatric dentistry. Eur Arch Paediatr Dent. 2010;11:166–174.
8. Alammouri M. The attitude of parents toward behavior management techniques in pediatric dentistry. J Clin Pediatr Dent. 2006;30:310–313. doi:10.17796/jcpd.30.4.m73568r0t74962m3
9. Muhammad S, Shyama M, Al-Mutawa SA. Parental attitude toward behavioral management techniques in dental practice with schoolchildren in Kuwait. Med Principles Pract. 2011;20(4):350–355. doi:10.1159/000323758
10. Patel M, McTigue DJ, Thikkurissy S, Fields HW. Parental attitudes toward advanced behavior guidance techniques used in pediatric dentistry. Pediatr Dent. 2016;38(1):30–36.
11. Venkataraghavan K, Shah J, Kaur M, Trivedi K, Shah S, Virda M. Pro-activeness of parents in accepting behavior management techniques: a cross-sectional evaluative study. J Clin Diagn Res. 2016;10(7):Zc46–49. doi:10.7860/JCDR/2016/18378.8162
12. Luis de Leon J, Guinot Jimeno F, Bellet Dalmau LJ. Acceptance by Spanish parents of behaviour-management techniques used in paediatric dentistry. Eur Arch Paediatr Dent. 2010;11(4):175–178. doi:10.1007/BF03262739
13. Malik P, Ferraz Dos Santos B, Girard F, Hovey R, Bedos C. Physical constraint in pediatric dentistry: the lived experience of parents. JDR Clin Trans Res. 2021:23800844211041952. doi:10.1177/23800844211041952
14. Al Zoubi L, Schmoeckel JC, Mustafa Ali M, Splieth C. Parental acceptance of advanced behaviour management techniques in paediatric dentistry in families with different cultural background. Eur Arch Paediatr Dent. 2021;22:707–713. doi:10.1007/s40368-021-00607-4
15. Frankel RI. The Papoose Board and mothers’ attitudes following its use. Pediatr Dent. 1991;13(5):284–288.
16. Peretz B, Zadik D. Parents’ attitudes toward behavior management techniques during dental treatment. Pediatr Dent. 1999;21(3):201–204.
17. Al-Shalan TA. Factors affecting Saudi parents’ perception of their children’s first dental visit. J Contemp Dent Pract. 2003;4(4):54–66. doi:10.5005/jcdp-4-4-54
18. Al Zoubi L, Schmoeckel J, Mustafa Ali M, Alkilzy M, Splieth CH. Parental acceptance of advanced behaviour management techniques in normal treatment and in emergency situations used in paediatric dentistry. Eur Arch Paediatr Dent. 2019;20(4):319–323. doi:10.1007/s40368-018-0408-y
19. Ghanei M, Arnrup K, Robertson A. Procedural pain in routine dental care for children: a part of the Swedish BITA study. Eur Arch Paediatr Dent. 2018;19(5):365–372. doi:10.1007/s40368-018-0368-2
20. Desai S, Shah P, Jajoo S, Smita P. Assessment of parental attitude toward different behavior management techniques used in pediatric dentistry. J Indian Soc Pedod Prev Dent. 2019;37(4):350–359. doi:10.4103/JISPPD.JISPPD_138_18
21. Wilson S, Gosnell E. Survey of American Academy of Pediatric Dentistry on nitrous oxide and sedation: 20 years later. Pediatr Dent. 2016;38(5):385–392.
22. Lombardi S, Sheller B, Williams B. Diagnosis and treatment of dental trauma in a children’s hospital. Pediatr Dent. 1998;20(2):112–120.
23. McKnight-Hanes C, Myers DR, Dushku JC, Davis HC. The use of behavior management techniques by dentists across practitioner type, age, and geographic region. Pediatr Dent. 1993;15(4):267–271.
24. Baakdah RA, Turkistani JM, Al-Qarni AM, et al. Pediatric dental treatments with pharmacological and non-pharmacological interventions: a cross sectional study. BMC Oral Health. 2021;21. doi:10.1186/s12903-021-01555-7
25. Chen YP, Hsieh CY, Hsu WT, Wu FY, Shih WY. A 10-year trend of dental treatments under general anesthesia of children in Taipei Veterans General Hospital. J Chin Med Assoc. 2017;80(4):262–268. doi:10.1016/j.jcma.2016.11.001
26. Fields HW, Machen JB, Murphy MG. Acceptability of various behavior management techniques relative to types of dental treatment. Pediatr Dent. 1984;6(4):199–203.
27. Alkandari SA, Almousa F, Abdulwahab M, Boynes SG. Dentists’ and parents’ attitude toward nitrous oxide use in Kuwait. Anesth Prog. 2016;63(1):8–16. doi:10.2344/14-00008.1
28. Lawrence SM, McTigue DJ, Wilson S, Odom JG, Waggoner WF, Fields HW. Parental attitudes toward behavior management techniques used in pediatric dentistry. Pediatr Dent. 1991;13(3):151–155.
29. Boka V, Arapostathis K, Vretos N, Kotsanos N. Parental acceptance of behaviour-management techniques used in paediatric dentistry and its relation to parental dental anxiety and experience. Eur Arch Paediatr Dent. 2014;15(5):333–339. doi:10.1007/s40368-014-0119-y
30. Havelka C, McTigue D, Wilson S, Odom J. The influence of social status and prior explanation on parental attitudes toward behavior management techniques. Pediatr Dent. 1992;14:376.
31. Peisch V, Lafko Breslend N, Jones DJ, MacFarlane M, Forehand R. Young children with behavior disorders in low-income families: the role of clinic observations in the assessment of parenting. Evid-Based Pract Child Adolesc Ment Health. 2017;2(3–4):201–211. doi:10.1080/23794925.2017.1393638
32. Kaiser T, Li J, Pollmann-Schult M, Song AY. Poverty and child behavioral problems: the mediating role of parenting and parental well-being. Int J Environ Res Public Health. 2017;14(9):981. doi:10.3390/ijerph14090981
33. Bor W, Najman JM, Andersen MJ, O’callaghan M, Williams GM, Behrens BC. The relationship between low family income and psychological disturbance in young children: an Australian longitudinal study. Aust N Z J Psychiatry. 1997;31(5):664–675. doi:10.3109/00048679709062679
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.