Back to Journals » Patient Preference and Adherence » Volume 17
Prevalence and Modifiable Factors for Holistic Non-Adherence in Renal Transplant Patients: A Cross-Sectional Study
Authors Torres-Gutiérrez M, Burgos-Camacho V, Caamaño-Jaraba JP, Lozano-Suárez N ![]() , García-López A
, García-López A ![]() , Girón-Luque F
, Girón-Luque F
Received 29 April 2023
Accepted for publication 12 August 2023
Published 6 September 2023 Volume 2023:17 Pages 2201—2213
DOI https://doi.org/10.2147/PPA.S419324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Manuel Torres-Gutiérrez,1 Viviana Burgos-Camacho,1 Jessica Paola Caamaño-Jaraba,1 Nicolás Lozano-Suárez,2 Andrea García-López,2 Fernando Girón-Luque2,3
1Department of Mental Health, Colombiana de Trasplantes, Bogotá, Colombia; 2Department of Transplant Research, Colombiana de Trasplantes, Bogotá, Colombia; 3Department of Transplant Surgery, Colombiana de Trasplantes, Bogotá, Colombia
Correspondence: Andrea García-López, Transplant Research, Colombiana de Trasplantes, Av Carrera, 30 No. 47 A-74, Bogota, 111311, Colombia, Email [email protected]
Introduction: In renal transplant recipients, compliance with medical therapy is vital. Non-adherence is considered a risk factor for worst outcomes in kidney recipients, with attributed outcomes of 64% for graft loss and 80% for late acute rejection. Most literature defines adherence as self-based immunosuppression compliance but does not consider other relevant factors such as consult and procedure compliance. Therefore, this study aims to describe adherence prevalence in kidney transplant recipients and the factors related to non-adherence.
Methods: This cross-sectional study included 1030 renal transplant patients followed by Colombiana de Trasplantes between January 2019 and July 2021. Sociodemographic and clinical variables were obtained based on clinical records. The mental-health group diagnosed holistic adherence in a semi-structured interview. The diagnosis considered medication intake failure, frequency and number of failures to medical controls or other procedures, suspicious non-adherence behaviors, and serum levels of immunosuppressants. A bivariate followed a descriptive analysis, and a forward logistic regression was performed for non-adherence.
Results: Patients had a median of 47 years, and 58.1% were male. Non-adherence was presented in 30.7% of patients. The non-adherence patients were younger, with a higher prevalence of males, single, divided transplant care, had a longer time after transplantation, psychopathological diagnosis, and more reinforcement education by only nursing. Older age and multidisciplinary reinforcement education were protective factors. On the other hand, poor social support, psychopathology diagnosis, and longer time after transplant presented as non-adherence risk factors.
Conclusion: Holistic non-adherence was diagnosed in approximately one-third of renal transplant recipients. Its definition included more than just medication non-compliance and could identify more non-adherent patients. Notably, there is a need to consider the related factors in the health follow-up and encourage future research in modifiable factor interventions aiming to increase adherence and achieve better outcomes for renal transplant patients.
Keywords: treatment adherence and compliance, kidney transplantation, patient compliance, social support, patient education, mental health, psychopathology
Introduction
Kidney transplantation has been considered the best treatment for chronic kidney disease stage 4 or 5.1,2 In 2021, Colombia contributed with 606 (0.55%)3 of the 109,215 kidney transplants that were performed worldwide.3,4 In the Colombian population, at the fifth year posttransplant, approximately 11.6% of kidney transplant recipients will have a graft loss,5 and it is well-described worldwide that medium- and long-term outcomes are vastly influenced by adherence to treatment.6,7 Attributed outcomes for non-adherence have been described as high as 64% for graft loss8 and 80% for late acute rejection, according to global literature.9 Consequently, it is essential to understand and describe non-adherence in renal transplant recipients in order to improve their outcomes.
The World Health Organization considers adherence goes beyond taking prescribed pharmaceuticals and defines it as
The extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.10
Meichenbaum and Turk also considered adherence as the set of specific behaviors of the patient in relation to all aspects of his treatment and not only the correct taking of his medication.11 But this wide definition is poorly used in kidney transplant recipients, defined mainly as compliance with the immunosuppression therapy and leaving behind other patient behaviors. Therefore, immunosuppression non-adherence in renal transplant recipients presents between 2 and 67% upon its definition and measurement.6
Many factors have been related to immunosuppression non-adherence, such as younger age, poor social support, cognitive impairment, and intrinsic religiosity.12–15 Moreover, previous research has found modifiable risk factors associated with immunosuppression adherence, such as health beliefs, self-beliefs, and self-efficacy.16,17 However, these factors are limited to immunosuppression non-adherence, not with a complete understanding of adherence. Also, these results are based on relatively small samples. Therefore, we estimated non-adherence prevalence and associated factors from a wide approach, including a large sample of Colombiana de Trasplantes and its network center patients. These results may enable us to improve our population’s adherence and outcomes for kidney transplant recipients.
Materials and Methods
An analytical, cross-sectional study was conducted, including all kidney transplant recipients followed by Colombiana de Trasplantes (network of 4 centers: Bogotá, Barranquilla, Rionegro, and Armenia) between January 2019 and July 2021. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology statement.18
Population and Sample
A non-randomized convenience sample was performed without prior sample size calculation by considering the inclusion of all patients who met the selection criteria. We included all patients in follow-up by Colombiana de Trasplantes after a renal transplant who continue being followed for at least one year after their evaluation. No patients were excluded. A power of 98% was estimated in R studio with the “pwr” package for the sample included (n = 1030) with a 95% confidence and a size effect of 0.39.19 The size effect was calculated with the Cohen formula considering a 50% expected prevalence described by Alba M20 and the obtained prevalence.
Data Collection
Data were collected from the clinical history and a semi-structured interview to determine adherence. A mental health team member conducted this interview with transplant patients (two psychiatrists and one psychologist) physically or virtually. In addition, the same team interviewed all patients in the four centers. This interview explored sociodemographic characteristics, events in the immediate post-transplant period (less than three months), and events related to their behavior in the late post-transplant period (more than three months). At the end of the interview, the mental health professional diagnosed the patient’s behavior as adherent or non-adherent.
Main Outcome
The diagnosis of adherence or non-adherence was a clinical holistic impression by a mental health team member that considered aspects such as pharmaceutical intake failure and its frequency, number of failures to medical controls, failure to other procedures (hospitalization, biopsies, laboratories), presence of suspicious non-adherence behaviors and serum levels of immunosuppressants. Table 1 elaborates on the postulated definitions of adherence, and Appendix 1 presents the semi-structured interview.
 |
Table 1 Definitions of Adherence, Non-Adherence, and Subtypes |
Variables
Sociodemographic and clinical variables were included to characterize the patients and explore associated factors to non-adherence. The sociodemographic variables considered were gender, age, and marital status. Clinical aspects related to the transplant procedure included transplant care, number of transplants, and type of donor. Factors related to transplant follow-up were reinforcement education in the first months, early anxiogenic events, and after-transplant follow-up time. Variable definitions are presented in Appendix 2.
Statistical Analysis
A descriptive analysis of the variables was performed according to their nature and distribution. Comparison of the adherence and non-adherence groups was evaluated using the chi-square test between categorical variables and Student’s t-test or Mann–Whitney U-test between quantitative variables according to their distribution. Results were considered statistically significant when the p-value was less than 0.05. A logistic regression was performed to determine associated factors to non-adherence. We calculated crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) to identify independent risk factors. For the multivariate analysis, we identified the variables with significant differences in the bivariate analysis and those clinically relevant. Variable selection was performed using a forward method. The inclusion of each variable was determined by statistical significance in ANOVA (analysis of variance) and chi-square tests compared to the previous model; once all variables were included, we sought the most parsimonious model. Any variable that changes the estimates by 10% was considered a cofounder and was controlled by its inclusion in the logistic regression.21,22 A complete or full model was also made, including all bivariate significant and clinically relevant variables. The final or reduced model was assessed with the Hosmer–Lemeshow test and Nagelkerke’s R2 (Pseudo-R-square).23,24 Multicollinearity was evaluated using the Variance Inflation Factor (VIF). Any variable with a VIF greater than five was considered highly correlated and excluded from the model.25 A sub-analysis by transplant group was conducted because patients transplanted by other groups did not receive the same adherence training and reinforcement as the kidney recipients of Colombiana de Trasplantes, particularly during the pre-transplant and early post-transplant periods. Analyses were performed using R software version 4.2.2.26
Ethical Statement
This study complied with International Ethical Guidelines by the Council for International Organizations of Medical Sciences (CIOMS) and the World Health Organization (WHO),27 the Declaration of Helsinki,28 and national ethical guidelines. All the kidneys were donated voluntarily with written informed consent in accordance with the Declaration of Istanbul.29 The Ethics Committee waived the research informed consent as the study was classified as with-out-risk by Colombian Resolution 8430.30 The analysis and presented results were anonymized, ensuring patient data confidentiality. The study only began after approval of the Ethics Committee.
Results
A total of 1030 patients were attended by Colombiana de Trasplantes during the study period. They had a median age of 47 years (IQR 36–58), 58.5% (n = 603) were men, 56.4% (n = 581) had a stable marital union and 30.9% (n = 319) were single. On the other hand, more than a third of patients had a diagnosis of psychopathology, in which affective, personality and adaptive disorders prevailed (Table 2).
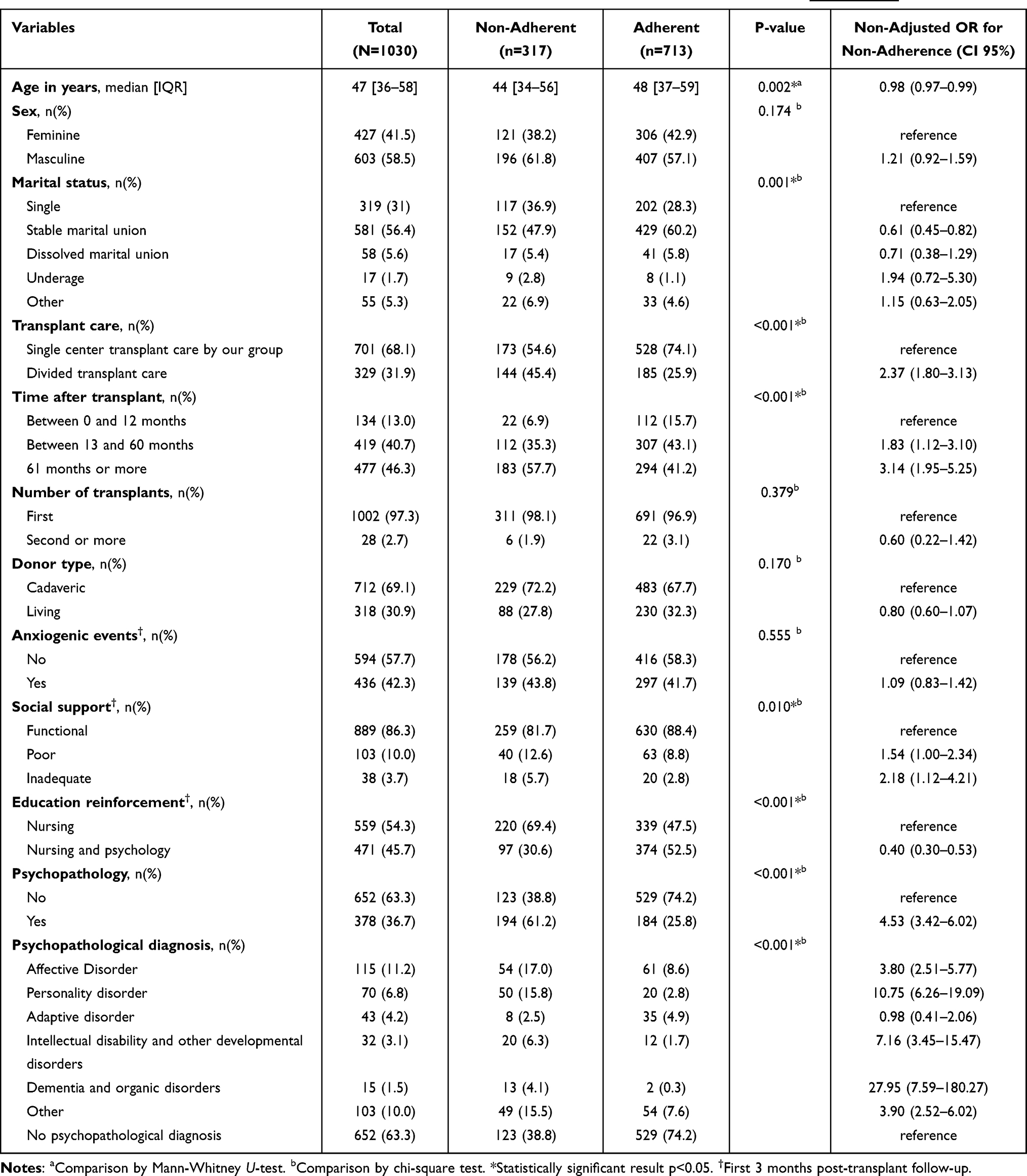 |
Table 2 Characterization of Adherent and Non-Adherent Patients. Definitions for Each Variable are in Appendix 2 |
Our surgical team transplanted and followed 68.1% (n = 701) of patients; the remaining patients were operated by other transplant groups and referred to our center (divided transplant care). Most of them of a deceased donor (69.1%) and only few patients (2.7%) were retransplanted (second or more transplant). In the first three post-transplant follow-up months, the majority of patients had a functional social support (86.3%), less than a half had an education reinforcement by psychology and nursing (45.7%), and 42.3% presented early anxiogenic events.
The holistic non-adherence was diagnosed in 30.8% (n = 317) and immunosuppression non-adherence in 25.9% (n = 267) kidney recipients.
Comparison Between Adherent and Non-Adherent Patients
Non-adherent patients were younger (44 vs 48 years, p 0.002), with a higher proportion of single and underage patients (p 0.001), and with more psychopathological diagnoses (61.2% vs 25.8%, p < 0.001). Non-adherents were more commonly transplanted by other transplant groups (45.4% vs 25.9%, p < 0.001). In the first months after transplantation, non-adherent patients had higher rates of poor and inadequate social support (p 0.009), and reinforcement education was primarily given by nursing (69.4% vs 47.5%, p < 0.001) (Table 2). Non-adherent patients were grouped by subtype and compared by sex in Figure 1. The most common subtype was invulnerable (48.3%) and apathetic (17%). The comparison between subtypes is presented in Table S1 (Appendix 3). Definitions for each non-adherence subtype are presented in Table 1 and deepened in Appendix 2.
 |
Figure 1 Graphic representation of non-adherence subtypes by sex. (A) Non-adherence subtypes in total population. (B) Non-adherence subtypes in women. (C) Non-adherence subtypes in men. |
Crude Model
We found that older age performed as a protector factor with 0.98 OR (CI 0.97–0.99). Being male increased 21% the risk of non-adherence (OR 1.21, CI 0.92–1.59), and stable marital union decreased by 39% compared to being single (OR 0.61, CI 0.45–0.82). When we analyzed the marital status by sex, we found that in women there was no significant change between being single or in a marital union, but for men being in a marital union decreased 49% the risk for non-adherence (OR 0.51, CI 0.35–0.76). Patients transplanted by other transplant groups had twice the risk for non-adherence (OR 2.37, CI 1.80–3.13). On the other hand, being retransplanted or transplanted from a living donor did not have an association with adherence or non-adherence. The remaining un-adjusted ORs are presented in Table 2.
Adjusted Model
For the multivariate model, the results of the full and reduced logistic regression model are presented in Table 3. In the reduced model, age evidenced a 3% reduction in the risk of non-adherence for each year increase (OR 0.97, CI 0.96–0.98). In the first three months after transplantation, having inadequate social support increased two times the risk of non-adherence (OR 2.31, CI 1.07–4.99), and poor social support also increased the risk (OR 2.09, CI 1.26–3.46) both compared to functional social support. Joint reinforcement education by psychology and nursing behaved as a protective factor reducing the probability of non-adherence by 64% (OR 0.36, CI 0.25–0.51). Psychopathology was a risk factor for non-adherence, especially dementia, personality disorder, and developmental disorders or intellectual disability, with ORs of 49.53, 11.56 and 5.50, respectively. Finally, a post-transplant follow-up time greater than five years presented an OR of 2.38 (CI 1.35–4.36), behaving as a risk factor for non-adherence compared to less than 12 months.
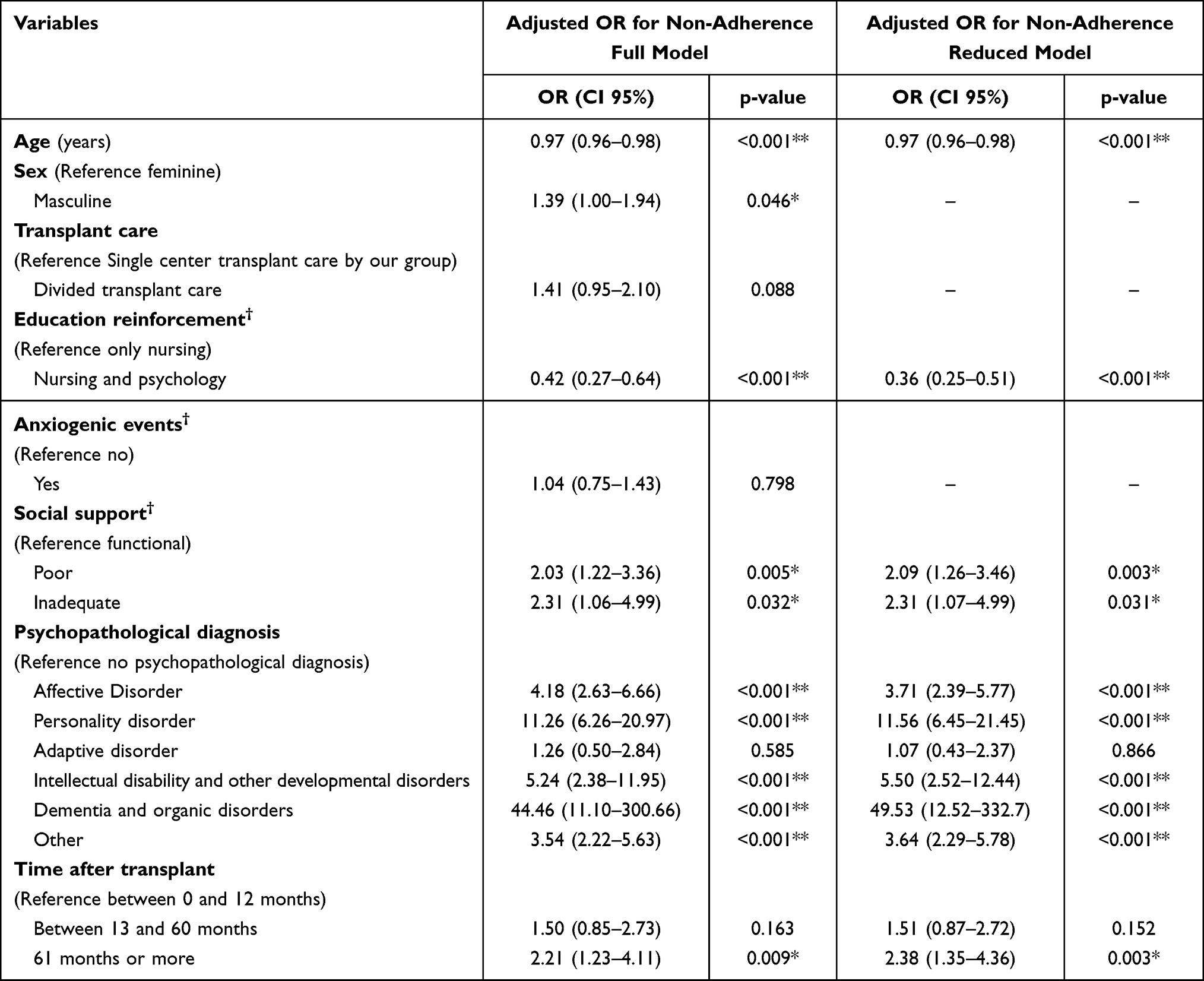 |
Table 3 The Multivariate Model with the Results of the Factors Associated with Non-Adherence. *Statistically Significant p < 0.05 **Very Statistically Significant p < 0.005 †First 3 months post-transplant follow-up. |
According to Bagley SC standards on logistic regression documentation,31 our reduced model had sufficient events per variable (63:1), there was no multicollinearity, Hosmer and Lemeshow test supported the model goodness of fit (p 0.13), and Nagelkerke R2 was 0.294.
Sub-Analysis by Transplant Group
Non-adherence was found in 24.7% of kidney recipients who received single-center transplant care in Colombiana de Trasplantes and 43.8% in patients who received divided transplant care transplanted by other groups (P < 0.001) (Figure 2). In addition, patients that received divided transplant care were older (46 vs 49 years, p 0.003), with a higher proportion of stable marital union and other civil status patients (p 0.03), greater time after transplant (32% vs 76.9% of more than five years, p < 0.001), less living donor transplants (7.9% vs 15.8%, p < 0.001).
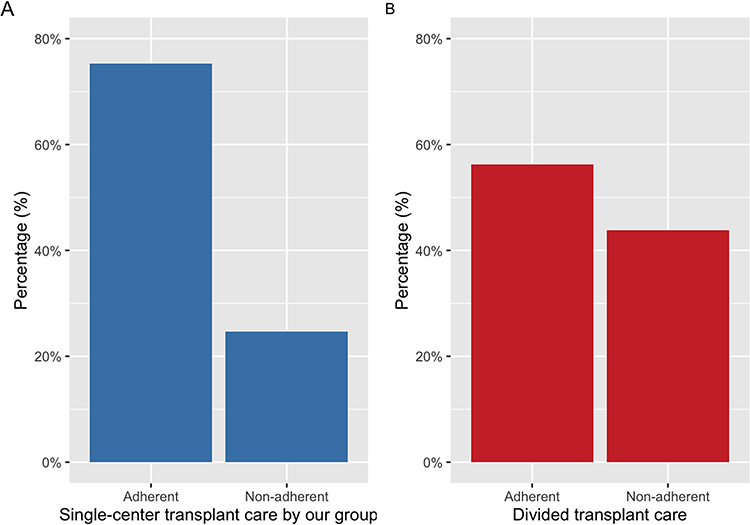 |
Figure 2 Relative frequencies of adherence and non-adherence in (A) patients transplanted and followed by a single center (Colombiana de trasplantes) and (B) patients transplanted by another group and followed by our center. |
The multivariate model in patients transplanted by our group showed that age and education reinforcement by nursing and psychology were protective factors for non-adherence, male sex, psychopathology, five years or more after transplant, and poor and inadequate social support were risk factors for non-adherence. On the other hand, the multivariate model for divided transplant care patients evidenced age and psychopathology as the only associated factors to non-adherence. Further details are presented in Appendix 3 (Tables S2–7).
Discussion
Adherence is a key factor for kidney transplant outcomes.6,7 Therefore, multiple studies have measured it, with a prevalence between 1.6 and 58.7% depending on their highly variable definitions.32 The most widely used definition is immunosuppression compliance, but even in its measuring methods there are essential differences. Data collection involves diverse methods such as electronic monitoring, self-report, pill count, patient interview, physician estimates, and immunosuppression blood levels.32,33 On the other hand, on a literature review of Denhaerynck et al,6 we can acknowledge different immunosuppression non-adherence definitions such as 20% missed of prescribed doses in six months, three or more missed doses in the last month, one or more missed doses in the previous week, taking less than 90% of prescribed doses, less than 80% of a prescribed medication refill, among others. In our study, we evidenced a non-adherence prevalence of 30.8%, self-reported immunosuppression non-compliance of 25.9%, and low immunosuppression blood levels in 15.7% of patients. Considering that non-adherent patients have a higher risk of worse outcomes and may benefit from early intervention, a broader definition of adherence, such as the one used in this study, allows higher non-adherence diagnosis compared to a definition based on self-report immunosuppression compliance and immunosuppression blood levels.
As previously discussed, numerous studies have explored non-adherence-related factors, hoping this understanding may increase adherence and provide better outcomes for renal transplant patients. In our study, age was significantly associated with non-adherence, adherent patients were older than non-adherent, and age presented an OR of 0.97, suggesting that each year of life led to less non-adherence risk. These findings are consistent with Belaiche S systematic review,32 in which recipients under 50 years were considered more non-adherent than those older. Also, Zachcial et al13 reported an age OR of 0.96 (CI 0.94–0.99) for non-adherence, implying fewer problems implementing recommendations with older age. Some authors consider that this adherence deterioration may be caused by increased independence and responsibility to the young person over their medication and management.34 A path to overcome this is establishing a support person outside the medical team who encourages continuous self-care and supervises treatment adherence.34
Another related factor was social support. Non-adherent patients presented higher rates of poor and inadequate social support. Furthermore, in the multivariate analysis, poor and inadequate social support approximately increased twice the non-adherence risk compared to functional support. Our results are consistent with previous evidence that stated that social support is associated with adherence.17,35,36 In fact, Chisholm-Burns M. and collaborators36 described that not only good social support was related to better adherence but that affectionate support was especially associated with increased adherence. It has been theorized that social support acts as a buffer that prevents or alleviates the impact of stressful events.36,37 Therefore, Vyavaharkar and Chisholm-Burns36,38 suggest that greater social support allows better management of stress and more favorable outcomes. These results may be significant by the fact that there is evidence that social support is a modifiable factor,39,40 and its improvement may provide better adherence and outcomes for renal transplant recipients.
We evidenced significant differences between marital status in adherent and non-adherent patients, with a non-adjusted odds ratio as a protective risk factor in a stable marital union compared to being single. These results are comparable to those presented by Zachcial et al,13 who described that being in a relationship is a non-significant protective factor against non-adherence, and Couzi et al41 who reported that being single behaves as a significant risk factor for non-adherence. Conversely, another study found higher rates of non-adherence in those in a relationship (married or cohabiting), but a small sample may have limited these results.42
On the other hand, a further analysis by sex and marital status of our data found that a stable marital union was a protective factor in men but not for women. This evidence is similar to the results of Neubert et al,43 which described the recipient’s social support and relationship quality as a predictor of adherence in male transplant, contrary to women’s results, in which only mental quality of life and education level influenced adherence. Scholz et al also established that women’s support for their partners was positively related to adherence intention, but men’s support was slight negatively related.44 This pattern is also described in other pathologies, such as an HIV prospective study that reported being married or in a stable union is a risk factor for non-adherence in females.45 Potential explanations are that women are more empathetic and understand better how to support their male partners.46 Another elucidation may be that the problem is not in the skill to provide support but in their responsiveness to their partner’s changing needs. In stressful experiences, women are better at adapting to their partner’s needs, and men tend to have more negative reactions.47
Our results suggest that reinforcement education by a multidisciplinary team composed of psychology and nursing behaves as a protective factor against non-adherence. Previous research has associated limited health literacy with adverse outcomes and in chronic kidney disease with higher mortality and lower access to transplantation.48,49 Therefore, education is considered an essential aspect of renal transplant treatment. Furthermore, even some authors have described the importance of updated and effective education programs for improving health literacy as a well-known barrier.49–51 Consequently, this multidisciplinary education reinforcement may be a key strategy to improve health literacy and adherence in renal transplant recipients.
A diagnosis of psychopathology was presented in more than a third of the kidney recipients. Likewise, results of the German cohort KTx360 reported that almost 27.5% of kidney transplant patients had a current and a 49.2% a lifetime mental disorder.52 A Korean cohort reported a depression incidence of 18.8 per 1000 person-years.53 It is well described the higher prevalence of significant depression and anxiety in transplant recipients, which could be up to 63% in the first year posttransplant.54–56 This prevalence of psychopathology is even higher than in chronic kidney disease patients (CKD). This was reported in Palmer et al systematic review and meta-analysis that estimated a depression prevalence of 21.4% in CKD and in 25.7% in kidney recipients.57 It has been established that surgery and transplantation can produce great stress and strong emotions in kidney transplant recipients, which can affect personal integrity and identity, allowing psychopathology onset and problems.58–60 Various studies have described the psychological results after kidney transplants, reporting anxiety and depression as the most commonly presented disorders.59,60 However, these studies have also found interpersonal relationship disturbances, emotional coarctation, and cognitive impairment.60–62
In our study, not only psychopathological diagnosis was prevalent but also one of our study’s most significant associations with non-adherence. The non-adjusted odds ratio indicated 4.5 times the risk of non-adherence compared to patients without the diagnosis. In the final logistic regression revealed that dementia, intellectual disability or development disorders, affective and personality disorders behave as risk factors for non-adherence. Only the adaptive disorder did not present an association with non-adherence. Similar to our study, Gelb et al63 reported that adherence can be affected by the psychopathology of the renal recipients.63 Therefore, pre- and post-transplant psychological assessment may be beneficial to screen and treat any psychopathological disturbances, aiming to enhance adherence and patient outcomes.
Time after transplant was also a determinant factor for adherence. Our study suggested that patients with five or more years of post-transplant follow-up presented twice the risk for non-adherence than those with less than a year after transplant. A systematic review reported 11 studies that found time after transplant as a related factor to non-adherence. The systematic review also highlighted the different and not well-established threshold time that increases the risk of non-adherence.32 Moreover, Burkhalter et al64 reported an increase of 20% in the odds for taking non-adherence and 16% in the overall non-adherence for each additional five years since the transplant. These results can be explained by less supervision of the health team and lack of continuous education reinforcement with time.13,65 Also, it could be interpreted as patients that get used to medications over time have a better feeling and less need for treatment perception.13,65,66
The non-adherence of the patients that received divided transplant care versus single-center transplant care by our group was significantly more. Consistently, the non-adjusted OR for divided transplant care was 2.3 times the risk versus single-center transplant care of our group. These findings may have multiple explanations. On one side, it is well described that good relationships with healthcare professionals are facilitators to adherence67–69, and receiving the complete transplant process in the same center may enhance better relations. On the other hand, our institution assessed and reinforced adherence actively in the pretransplant, early posttransplant, and late posttransplant period; likewise, several authors evidenced that adherence programs enhance adherence prevalence and outcomes.70,71
Notably, this study supports the relevance of social support, educational reinforcement, and psychopathology as adherence-modifiable factors in renal transplant recipients.72,73 Similar associated factors have been found in non-adherent CKD patients in pre-dialysis and hemodialysis, including age, social support, depressive symptoms, and marital status.72,73 For this population, there is evidence of the benefits of education and psycho-social interventions in adherence.74,75 In kidney recipients, a meta-analysis from Zhu et al76 confirmed that patients that received adherence interventions had a higher rate of adherence (OR 2.36, CI 95% 122–4.57) than those who did not received them. Some interventions include education, behavioral interventions, pharmacist care, and smartphone reminders. Furthermore, another systematic review conducted by Low et al77 described the increased effectiveness of multidimensional interventions rather than unidimensional, but declared that adherence is a poorly managed problem. Therefore, institutions such as the American Society of Transplantation gave practical recommendations to improve adherence, including educational interventions, cognitive behavioral interventions, and health information technology.78
There are important limitations to disclose. First, the cross-sectional design could limit the quality and quantity of the recollected data. Besides, since the study design, we do not have information on the adherence change across time as a multifactorial process. Second, the definition of adherence may appear widely subjective and could restrain the reproducibility of our methodology in other populations. Also, adherence was obtained mostly from self-reported information, which, on the one hand, is reported to capture more non-adherent patients than other assessment methods,79 but on the other hand, it has the potential to lose precision on recall bias.78 Third, the recollection was mainly in the covid 19 pandemic, which can influence the adherence process. Finally, the generalization of the results may be restricted by the convenience sample methodology. Therefore, there is a need for more extensive studies with heterogenic populations to assess these related factors to adherence. Studies that evaluate interventions are based on the associated factors to non-adherence evidence, in order to find new strategies that could improve adherence and outcomes in renal transplant recipients.
Conclusion
This study suggests that a wide definition of non-adherence, including more than immunosuppression compliance, can capture more patients that may benefit from an early diagnosis and treatment. That approximately one-third of kidney transplant recipients are non-adherent. Age, education reinforcement, social support, and psychopathological diagnoses are associated with renal transplant recipient’s adherence. Therefore, these factors should be considered in the health team follow-up and even in prediction tools to target non-adherence risk. Also, to screen and treat psychopathological disorders as a prevalent factor in non-adherent patients. Finally, there is a need for future research to study novel interventions to modifiable factors, such as educational reinforcement and social support, that could improve adherence and outcomes in renal transplant patients.
Acknowledgments
The authors thank Colombiana de Trasplantes for its support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Colombiana de Trasplantes.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Arze Aimaretti L, Arze S. Preemptive renal transplantation - the best treatment option for terminal chronic renal failure. Transplant Proc. 2016;48(2):609–611. doi:10.1016/j.transproceed.2016.02.047
2. Sarier M, Demir M, Goktas S, et al. Results of real-time multiplex polymerase chain reaction assay in renal transplant recipients with sterile pyuria. Transplant Proc. 2017;49(6):1307–1311. doi:10.1016/j.transproceed.2017.02.051
3. Instituto Nacional de Salud de Colombia. Informe anual red donación y trasplantes/Donation and Transplantation Network Annual Report 2021; 2021.
4. World Health Organization, Spanish Transplant Organization. Total kidney transplant - global observatory on donation and transplantation; 2022.Available from: https://www.transplant-observatory.org/data-charts-and-tables/chart/.
5. Pinto-Ramirez J, Garcia-Lopez A, Salcedo-Herrera S, et al. Risk factors for graft loss and death among kidney transplant recipients: a competing risk analysis. PLoS One. 2022;17:e0269990. doi:10.1371/journal.pone.0269990
6. Denhaerynck K, Dobbels F, Cleemput I, et al. Prevalence, consequences, and determinants of nonadherence in adult renal transplant patients: a literature review. Transplant Inter. 2005;18:1121–1133. doi:10.1111/j.1432-2277.2005.00176.x
7. Nevins TE, Matas AJ. Medication noncompliance: another iceberg’s tip. Transplantation. 2004;77:776–778. doi:10.1097/01.TP.0000110409.71847.6F
8. Kiley Deborah J, Lam CS, Pollak R. A study of treatment compliance following kidney transplantation. Transplantation. 1993;55(1):51–56. doi:10.1097/00007890-199301000-00010
9. Rovelli M, Palmeri D, Vossler E, Bartus S, Hull D, Schweizer R. Noncompliance in organ transplant recipients. Transplant Proc. 1989;21(1 Pt 1):833–834.
10. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003:194.
11. Meichenbaum D, Turk DC. Facilitating Treatment Adherence a Practitioner’s Guidebook.
12. Silva AN, Moratelli L, Tavares PL, et al. Self-efficacy beliefs, locus of control, religiosity and non-adherence to immunosuppressive medications in kidney transplant patients. Nephrology. 2016;21(11):938–943. doi:10.1111/nep.12695
13. Zachciał J, Uchmanowicz I, Czapla M, Krajewska M, Banasik M. The association between psychosocial and age-related factors with adherence to immunosuppressive therapies after renal transplantation. J Clin Med. 2022;11(9):2386. doi:10.3390/jcm11092386
14. Scheel JF, Schieber K, Reber S, et al. Psychosocial variables associated with immunosuppressive medication non-adherence after renal transplantation. Front Psychiatry. 2018;9. doi:10.3389/fpsyt.2018.00023
15. Gremigni P, Bacchi F, Turrini C, Cappelli G, Albertazzi A, Bitti PER. Psychological factors associated with medication adherence following renal transplantation. Clin Transplant. 2007;21(6):710–715. doi:10.1111/j.1399-0012.2007.00727.x
16. Heits N, Meer G, Malchow B, et al. Abstract# B1190 quality of life after liver transplantation abstract. Transplantation. 2014;98:825. doi:10.1097/00007890-201407151-02817
17. Butler JA, Peveler RC, Roderick P, Smith PWF, Horne R, Mason JC. Modifiable risk factors for non-adherence to immunosuppressants in renal transplant recipients: a cross-sectional study. Nephrol Dial Transplant. 2004;19(12):3144–3149. doi:10.1093/ndt/gfh505
18. Equator. STROBE checklist for cohort studies. 2018:1–2. Available from: http://www.equator-network.org/reporting-guidelines/strobe/.
19. Ekstrom C, Dalgaard P, Gill J, et al. Pwr: Basic Functions for Power Analysis. CRAN; 2020.
20. Alba M, Camargo A. Adherencia al tratamiento de medicamentos inmunosupresores y su asociación con el rechazo al injerto en pacientes con trasplante renal realizado en Bogotá en Colombiana de Trasplantes en el año 2013 [Adherence to immunosuppressors and its association with graft rejection in patients with renal transplantation performed in Bogotá at Colombiana de Trasplantes in 2013]. Bogotá: Univerisdad Nacional de Colombia; 2017.
21. Maldonado G, Greenland S. Simulation study of confounder-selection strategies. Am J Epidemiol. 1993;138(11):923–936. doi:10.1093/oxfordjournals.aje.a116813
22. Pourhoseingholi MA, Baghestani AR, Vahedi M. How to control confounding effects by statistical analysis. Gastroenterol Hepatol Bed Bench. 2012;5(2):79–83.
23. Hughes G, Choudhury RA, McRoberts N. Summary measures of predictive power associated with logistic regression models of disease risk. Phytopathology. 2019;109(5):712–715. doi:10.1094/PHYTO-09-18-0356-LE
24. Stoltzfus JC. Logistic regression: a brief primer. Acad Emerg Med. 2011;18(10):1099–1104. doi:10.1111/j.1553-2712.2011.01185.x
25. Varady NH, Pareek A, Eckhardt CM, et al. Multivariable regression: understanding one of medicine’s most fundamental statistical tools. Knee Surg Sports Traumatol Arthrosc. 2022;31(1):7–11. doi:10.1007/s00167-022-07215-9
26. RStudio Team. RStudio: Integrated Development Environment for R. Boston, MA; 2022. Available from: http://www.rstudio.com/.
27. Council for International Organizations of Medical Sciences, World Health Organization. International Ethical Guidelines for Health-Related Research Involving Humans. Geneva: Council for International Organizations of Medical Sciences (CIOMS); 2016:122.
28. 64th World Medical Association General Assembly. Declaration of Helsinki. Fortaleza, Brazil; 2013.
29. Abboud O, Abbud-Filho M, Abdramanov K, et al. The declaration of Istanbul on organ trafficking and transplant tourism. Clin J Am Soc Nephrol. 2008;3(5):1227.
30. Ministerio de Salud y Protección social de Colombia. Resolución número 8430 de 1993/Resolution number 8430 of 1993; 1993:1–19.
31. Bagley SC, White H, Golomb BA. Logistic regression in the medical literature: standards for use and reporting, with particular attention to one medical domain. J Clin Epidemiol. 2001;54:979–985. doi:10.1016/s0895-4356(01)00372-9
32. Belaiche S, Décaudin B, Dharancy S, Noel C, Odou P, Hazzan M. Factors relevant to medication non-adherence in kidney transplant: a systematic review. Int J Clin Pharm. 2017;39(3):582–593. doi:10.1007/s11096-017-0436-4
33. Lieb M, Hepp T, Schiffer M, Opgenoorth M, Erim Y. Accuracy and concordance of measurement methods to assess non-adherence after renal transplantation - A prospective study. BMC Nephrol. 2020;21(1). doi:10.1186/s12882-020-01781-1
34. Bethany JF, Ahna LHP. Adherence in adolescent and young adult kidney transplant recipients. Open Urol Nephrol J. 2014;7(1):133–143. doi:10.2174/1874303X014070100133
35. Lin SY, Fetzer SJ, Lee PC, Chen CH. Predicting adherence to health care recommendations using health promotion behaviours in kidney transplant recipients within 1-5 years post-transplant. J Clin Nurs. 2011;20(23–24):3313–3321. doi:10.1111/j.1365-2702.2011.03757.x
36. Chisholm-Burns MA, Spivey CA, Wilks SE. Social support and immunosuppressant therapy adherence among adult renal transplant recipients. Clin Transplant. 2010;24(3):312–320. doi:10.1111/j.1399-0012.2009.01060.x
37. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
38. Vyavaharkar M, Moneyham L, Tavakoli A, et al. Social support, coping, and medication adherence among hiv-positive women with depression living in rural areas of the Southeastern United States. AIDS Patient Care STDS. 2007;21(9):667–680. doi:10.1089/apc.2006.0131
39. Toseland RW, Rossiter CM, Labrecque MS. The effectiveness of peer-led and professionally led groups to support family caregivers. Gerontologist. 1989;29(4):465–471. doi:10.1093/geront/29.4.465
40. Castelein S, Bruggeman R, van Busschbach JT, et al. The effectiveness of peer support groups in psychosis: a randomized controlled trial. Acta Psychiatr Scand. 2008;118(1):64–72. doi:10.1111/j.1600-0447.2008.01216.x
41. Couzi L, Moulin B, Morin MP, et al. factors predictive of medication nonadherence after renal transplantation. J Transplant. 2013;95(2):326–332. doi:10.1097/TP.0b013e318271d7c1
42. Griva K, Davenport A, Harrison M, Newman SP. Non-Adherence to immunosuppressive medications in kidney transplantation: intent vs. forgetfulness and clinical markers of medication intake. Ann Behav Med. 2012;44(1):85–93. doi:10.1007/s12160-012-9359-4
43. Neubert L, Peters L, Tkachenko D, Zimmermann T. Couples after renal transplantation: impact of sex and relationship quality on adherence in a prospective study. Transplant Proc. 2021;53(5):1599–1605. doi:10.1016/j.transproceed.2021.02.017
44. Scholz U, Klaghofer R, Dux R, et al. Predicting intentions and adherence behavior in the context of organ transplantation: gender differences of provided social support. J Psychosom Res. 2012;72(3):214–219. doi:10.1016/j.jpsychores.2011.10.008
45. de Fatima Bonolo P, Ceccato MGB, Rocha GM, de Assis Acúrcio F, Campos LN, Guimarães MDC. Gender differences in non-adherence among Brazilian patients initiating antiretroviral therapy. Clinics. 2013;68(5):612–620. doi:10.6061/clinics/2013(05)06
46. Thomas G, Fletcher GJO. Mind-reading accuracy in intimate relationships: assessing the roles of the Relationship, the Target, and the Judge. J Pers Soc Psychol. 2003;85(6):1079–1094. doi:10.1037/0022-3514.85.6.1079
47. Neff LA, Karney BR. Gender differences in social support: a question of skill or responsiveness? J Pers Soc Psychol. 2005;88(1):79–90. doi:10.1037/0022-3514.88.1.79
48. Cavanaugh KL, Wingard RL, Hakim RM, et al. Low health literacy associates with increased mortality in ESRD. J Am Soc Nephrol. 2010;21(11):1979–1985. doi:10.1681/ASN.2009111163
49. Young BA. Health literacy in nephrology: why is it important? Am J Kidney Dis. 2013;62:3–6. doi:10.1053/j.ajkd.2013.04.003
50. Urstad KH, Wahl AK, Moum T, Engebretsen E, Andersen MH. Renal recipients’ knowledge and self-efficacy during first year after implementing an evidence based educational intervention as routine care at the transplantation clinic. BMC Nephrol. 2021;22(1):265. doi:10.1186/s12882-021-02468-x
51. Urstad KH, Øyen O, Andersen MH, Moum T, Wahl AK. The effect of an educational intervention for renal recipients: a randomized controlled trial. Clin Transplant. 2012;26(3):E246–E253. doi:10.1111/j.1399-0012.2012.01666.x
52. Birkefeld K, Bauer-Hohmann M, Klewitz F, et al. Prevalence of mental disorders in a German kidney transplant population: results of a KTx360°-Substudy. J Clin Psychol Med Settings. 2022;29(4):963–976. doi:10.1007/s10880-022-09861-0
53. Cho S, Park S, Kim JE, et al. Incidence of depression in kidney transplant recipients in South Korea: a long-term population-based study. Sci Rep. 2022;12(1):1–11. doi:10.1038/s41598-022-20828-x
54. Zalai D, Szeifert L, Novak M. Psychological distress and depression in patients with chronic kidney disease. Semin Dial. 2012;25(4):428–438. doi:10.1111/j.1525-139X.2012.01100.x
55. Dew MA, DiMartini AF. Psychological disorders and distress after adult cardiothoracic transplantation. J Cardiovasc Nurs. 2005;20(Supplement):S51–66. doi:10.1097/00005082-200509001-00007
56. Dew MA, Rosenberger EM, Myaskovsky L, et al. Depression and anxiety as risk factors for morbidity and mortality after organ transplantation. Transplantation. 2015;100(5):988–1003. doi:10.1097/TP.0000000000000901
57. Palmer S, Vecchio M, Craig JC, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 2013;84(1):179–191. doi:10.1038/ki.2013.77
58. Kayler LK. Candidate comprehension of key concepts in kidney transplantation. Ann Transplant. 2015;20:124–131. doi:10.12659/AOT.892596
59. Fukunishi I, Aikawa A, Ohara T, Hasegawa A. Psychiatric problems among recipients of kidney transplants: a 10-year follow-up. Transplant Proc. 2002;34(7):2766. doi:10.1016/S0041-1345(02)03401-2
60. de Pasquale C, Luisa Pistorio M, Veroux M, et al. Psychological and psychopathological aspects of kidney transplantation: a systematic review. Front Psychiatry. 2020;11:11. doi:10.3389/fpsyt.2020.00011
61. Gelb S, Shapiro RJ, Hill A, Thornton WL. Cognitive outcome following kidney transplantation. Nephrol Dial Transplant. 2007;23(3):1032–1038. doi:10.1093/ndt/gfm659
62. de Pasquale C, Pistorio ML, Sorbello M, et al. Body Image in Kidney Transplantation. Transplant Proc. 2010;42(4):1123–1126. doi:10.1016/j.transproceed.2010.03.071
63. Pasquale C. Psychopathological aspects of kidney transplantation: efficacy of a multidisciplinary team. World J Transplant. 2014;4(4):267. doi:10.5500/wjt.v4.i4.267
64. Burkhalter H, Wirz-Justice A, Cajochen C, et al. Daytime sleepiness in renal transplant recipients is associated with immunosuppressive non-adherence: a cross-sectional, multi-center study. Clin Transplant. 2014;28(1):58–66. doi:10.1111/ctr.12279
65. Gelb SR, Shapiro RJ, Thornton WJL. Predicting medication adherence and employment status following kidney transplant: the relative utility of traditional and everyday cognitive approaches. Neuropsychology. 2010;24(4):514–526. doi:10.1037/a0018670
66. Ruppar TM, Russell CL. Medication adherence in successful kidney transplant recipients. Prog Transplant. 2009;19(2):167–172. doi:10.1177/152692480901900211
67. Oberlin SR, Parente ST, Pruett TL. Improving medication adherence among kidney transplant recipients: findings from other industries, patient engagement, and behavioral economics—A scoping review. SAGE Open Med. 2016;4:205031211562502. doi:10.1177/2050312115625026
68. Steinberg EA, Moss M, Buchanan CL, Goebel J. Adherence in pediatric kidney transplant recipients: solutions for the system. Pediatr Nephrol. 2018;33:361–372. doi:10.1007/s00467-017-3637-0
69. Arrivillaga-Quintero M. Análisis de las barreras para la adherencia terapéutica en mujeres colombianas con VIH/sida: cuestión de derechos de salud/Analysis of the barriers to therapeutic adherence in Colombian women with HIV/AIDS: a health rights issue. Salud Publica Mex. 2010;52(4):350–356. doi:10.1590/S0036-36342010000400011
70. Varnell CD, Rich KL, Modi AC, Hooper DK, Eckman MH. A cost-effectiveness analysis of adherence promotion strategies to improve rejection rates in adolescent kidney transplant recipients. Am J Kidney Dis. 2022;80(3):330–340. doi:10.1053/j.ajkd.2021.12.013
71. Hooper DK, Varnell CD, Rich K, et al. A medication adherence promotion system to reduce late kidney allograft rejection: a quality improvement study. Am J Kidney Dis. 2022;79(3):335–346. doi:10.1053/j.ajkd.2021.06.021
72. Seng JJB, Tan JY, Yeam CT, Htay H, Foo WYM. Factors affecting medication adherence among pre-dialysis chronic kidney disease patients: a systematic review and meta-analysis of literature. Int Urol Nephrol. 2020;52:903–916. doi:10.1007/s11255-020-02452-8
73. Ghimire S, Castelino RL, Lioufas NM, Peterson GM, Zaidi STR. Nonadherence to medication therapy in haemodialysis patients: a systematic review. PLoS One. 2015;10. doi:10.1371/journal.pone.0144119
74. Kim H, Jeong IS, Cho MK. Effect of treatment adherence improvement program in hemodialysis patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(18):11657. doi:10.3390/ijerph191811657
75. Tao W, Tao X, Wang Y, Bi S. Psycho‐social and educational interventions for enhancing adherence to dialysis in adults with end‐stage renal disease: a meta‐analysis. J Clin Nurs. 2020;29(15–16):2834–2848. doi:10.1111/jocn.15301
76. Zhu Y, Zhou Y, Zhang L, Zhang J, Lin J. Efficacy of interventions for adherence to the immunosuppressive therapy in kidney transplant recipients: a meta-analysis and systematic review. J Investig Med. 2017;65(7):1049–1056. doi:10.1136/jim-2016-000265
77. Low JK, Williams A, Manias E, Crawford K. Interventions to improve medication adherence in adult kidney transplant recipients: a systematic review. Nephrology Dialysis Transplantation. 2015;30(5):752–761. doi:10.1093/ndt/gfu204
78. Myaskovsky L, Jesse MT, Kuntz K, et al. Report from the American society of transplantation psychosocial community of practice adherence task force: real-world options for promoting adherence in adult recipients. Clin Transplant. 2018;32(9):e13353. doi:10.1111/ctr.13353
79. Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and risk factors for nonadherence to the medical regimen after adult solid organ transplantation. Transplantation. 2007;83(7):858–873. doi:10.1097/01.tp.0000258599.65257.a6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of an Auditory Mediated Patient Health Education (PHE) Program on Treatment Compliance and Satisfaction Among Patients Seeking Prosthodontic Care During COVID Pandemic – A Prospective Interventional Study
Sindi AS, Mittal R, Mattoo K, Deep A, Khateeb SU, Algarni YA, Baba SM, Hakami AM
Patient Preference and Adherence 2022, 16:1247-1255
Published Date: 16 May 2022
Mental Health Literacy and Professional Psychological Help-Seeking Attitudes Among Primary Healthcare Workers: The Mediating Role of Social Support and Mental Illness Stigma
He X, Chen S, Zhang Q, He S, Yang L, Ma J
Risk Management and Healthcare Policy 2025, 18:703-718
Published Date: 28 February 2025