")
Back to Journals » International Journal of General Medicine » Volume 16
Prevalence and Knowledge of Respiratory Symptoms Among the General Public in the Southern Area of Najran, Saudi Arabia: A Cross-Sectional Health Survey Study
Authors Alyami MH , Naser AY , Alyami HS, Algahtani TS, Alyami AH, Alsalem SA, Almansour AH, Alswar HS, Alhareth AMA
Received 21 April 2023
Accepted for publication 31 August 2023
Published 7 September 2023 Volume 2023:16 Pages 4077—4090
DOI https://doi.org/10.2147/IJGM.S418152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammad H Alyami,1 Abdallah Y Naser,2 Hamad S Alyami,1 Thamer S Algahtani,1 Abdullah H Alyami,3 Saleh A Alsalem,3 Abdullah H Almansour,3 Hadi S Alswar,3 Ali M Al Alhareth3
1Department of Pharmaceutics, College of Pharmacy, Najran University, Najran, Saudi Arabia; 2Department of Applied Pharmaceutics and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan; 3Directorate of Health Affairs Najran, Ministry of Health, Najran, Saudi Arabia
Correspondence: Mohammad H Alyami, Department of Pharmaceutics, College of Pharmacy, Najran University, Najran, 11001, Saudi Arabia, Tel +966 565022774, Email [email protected] Abdallah Y Naser, Department of Applied Pharmaceutics and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan, Tel +962 795285555, Email [email protected]
Objective: To investigate the knowledge, prevalence of chronic respiratory disorders, and utilization of their medications among the adults at Najran region, Saudi Arabia.
Methods: An online cross-sectional survey was carried out in Najran region, Saudi Arabia. A self-administered questionnaire was distributed among a random sample of the general population, aged 18 or above between March and December 2022. The survey instrument included questions regarding history and exposure, physician diagnosed-disorders, respiratory symptoms, allergy, use of medications and possible risk-related factors.
Results: This research had a total of 712 individuals. Nearly one-third of the participants in the survey (n = 218; 30.6%) said that they or a member of their family suffer from respiratory ailments. The majority of research participants (n = 167; 76.8%) identified asthma as their primary respiratory condition. A total of 32.0% of participants (n = 70) reported dealing with dust or chemicals such as paints, fertilizers, and cleaning products on a daily basis at work or at home. Around 62.0% of the participants (n = 134) said that exposure to gases, fragrances, and other such substances negatively impacts their health. Almost 78.0% (n = 169) of them indicated that summer weather affects their health, whereas 63.0% (n = 138) reported that winter cold affects their health. Participants aged 41– 50 years were 38.0% less likely to have CRDs compared to others (p < 0.05).
Conclusion: This study is among the first few studies that explored the knowledge, prevalence of chronic respiratory disorders, and utilization of their medications among the adults at Najran region, Saudi Arabia. In the southern area of Najran, respiratory symptoms are frequent among the inhabitants of Saudi Arabia. More research is required to discover avoidable risk factors and create countermeasures for them. It is recommended that healthcare personnel increase their efforts to educate their patients about respiratory illness prevention methods.
Keywords: diseases, respiratory, Saudi Arabia, symptoms
Introduction
Chronic respiratory disorders (CRDs), which affect the airways and other respiratory structures, are among the primary causes of morbidity and mortality globally.1,2 Asthma, chronic obstructive pulmonary disease (COPD), and occupational lung disorders are the most prevalent respiratory illnesses.1
Several disease types are major contributors to the growing worldwide incidence of noncommunicable diseases (NCDs). In order to reduce the burden of CRDs and work toward a world where everyone can breathe easily, the WHO Global Alliance against CRDs was founded.3
There are many possible risk factors for CRDs, including the use of biomass fuels, which exposes at least 2 billion people to harmful side effects, outdoor air pollution, which affects 1 billion people, and smoking, which affects an almost equal number of people through second hand smoke.4 An estimated 4 million individuals die early because CRDs each year.1
Although work-related respiratory circumstances are a well-established risk factor, it is difficult to quantify their magnitude. Based on the few studies that have been conducted, it is estimated that work-related exposures to respiratory conditions are responsible for about 2 million work-related deaths each year.5,6 Additionally, older age is linked to a number of structural changes in the airways, which increases vulnerability to disease processes. For example, following acute respiratory infections, older persons are at risk to develop pneumonia. Importantly, age-related lung alterations are exacerbated by the impacts of heart and lung disorders, particularly those induced by the harmful consequences of smoking.2,7
According to the Forum of International Respiratory Societies (FIRS), the five most significant lung illnesses globally in terms of prevalence are pneumonia, asthma, COPD, lung cancer, and tuberculosis.8 Although there is no known cure for chronic respiratory diseases, there are a number of treatments that can help manage symptoms, improve patients’ quality of life, and help deter unfavourable outcomes (such as exacerbations) that are linked to significant morbidity, increased healthcare utilization, disability, and mortality risk.9–14
Furthermore, CRDs treatment costs are rising worldwide. For example, in 2019, the estimated spend on CRDs therapy was €380 billion in 28 European countries. This estimate includes direct primary and admissions, the assessed value of lost disability-adjusted life years, a minimum of €42 billion for lost productivity, and a minimum €55 billion for direct primary and inpatient healthcare.1
In 2019, the age-standardised prevalence rate of COPD in Saudi Arabia was 2053.04 (1918.06–2194.29) cases per 100,000.15 According to a previous study by Alomary et al in Saudi Arabia, the prevalence of asthma is estimated to be around 14.0%.16
Among patients with respiratory illnesses in Saudi Arabia, asthma, COPD, and pneumonia were the most prevalent reasons for hospitalization, while hypertension and diabetes represented the most often related conditions.17 According to recent studies, the frequency and incidence of various respiratory disease as COPD, asthma in Saudi Arabia have been continuously increasing between 1990 and 2019.1 Despite the fact that COPD morbidity and mortality rates have been declining, they remain greater in males and the elderly.15,18,19
The Najran region in Saudi Arabia has distinct qualities that set it apart from other regions within the kingdom. These distinguishing features mostly pertain to its geography, climate, and potential health-related problems. Najran is situated in the southwestern region of the Kingdom of Saudi Arabia. The region undergoes elevated temperatures and limited precipitation, hence contributing to the dry climate prevalent in the desert ecosystem. Dust storms and sandstorms are frequently seen phenomena in dry regions, and their occurrence can have significant ramifications for respiratory health. The confluence of dry climatic conditions, occurrences of dust storms, and various other environmental elements has the ability to exert an influence on persons who suffer from asthma or other respiratory diseases. Hence, the current study aims to investigate the knowledge, prevalence of CRDs, and utilization of their medications among the adults at Najran region, Saudi Arabia.
Methods
Study Design
An online cross-sectional survey was carried out in Najran region, Saudi Arabia. A self-administered questionnaire was distributed among a random sample of the general population, aged 18 or above between March and December 2022.
Participants’ Recruitment and Sampling Procedure
The inclusion criteria for this study are adults aged 18 years and above and currently living in Najran region, Saudi Arabia. There were no gender-based criteria for exclusion. The study sample was gathered using a convenience sampling technique. This study included voluntary participants who met the inclusion criteria and were deemed eligible. On the first page of the questionnaire, patients were presented with an informed consent form and given the option to continue or withdraw from the study. To ensure that the patients comprehended the significance of their participation, the study’s objectives were presented in detail. The inclusion criteria were specified in the study’s invitation letter. Participants were asked to participate only if they meet the inclusion criteria. The URL to the survey was disseminated on social media platforms (Facebook, Instagram, and Snapchat) to invite interested individuals to participate.
Study Instrument
The study instrument was developed based on extensive literature review.20–22 The survey instrument included questions regarding history (family history of respiratory diseases, type of respiratory diseases, years of suffering or progression of the disease, tests that were done during the diagnosis, comorbidities) and exposure (whether they deal with dust or chemicals such as paints, fertilizers and cleaning tools on a regular basis at work or at home, whether they expose to fumes, perfumes, or the like affect their, whether the weather change in summer affects their health (dust), whether the cold weather in winter affects their health, whether they live near or have direct contact with animals?), physician diagnosed-disorders, respiratory symptoms (whether they experienced any wheezing at any time during the last 12 months while breathing, whether wheezing happen with or without a cold, whether they wake up because of experiencing shortness of breath or chest tightness, whether they complain from runny nose, or eye redness and itching), allergy profile (whether they suffer from seasonal allergies and whether they have had an allergy test before?), whether they refer to a hospital or a specialist doctor for their condition? And use of medications (whether they take medication for asthma, allergies, or other respiratory diseases, adherence to medications, type of medications, and whether they take any traditional or herbal medicine to treat any kind of respiratory disease), and participants knowledge (possible causes of the spread of respiratory diseases and high-risk population to be affected by respiratory diseases).
Study Piloting
Two clinical pharmacists from the Najran University Faculty of Pharmacy assessed and checked the questionnaire instrument. They were questioned on the clarity, understandability, and face validity of the questions as well as if any of them were challenging to understand. They were also asked about any inquiries that they considered infuriating or insulting. They mentioned how easy it was to understand and finish the questionnaire. Prior to deploying the questionnaire on a larger scale, an online pilot study was undertaken with a small sample of the general population (40 participants) to gauge understanding, and the findings confirmed that it is simple and easy to understand.
Sample Size
The minimum required sample size was 385 individuals using a 95% confidence interval, a 0.5 standard deviation (SD), and a 5% margin of error.
Statistical Analysis
This study’s data were analyzed using version 27 of the SPSS program. Descriptive statistics were used to present the data for this study. Categorical variables were presented as frequency and percentage. The Chi-Square test of independence was used to examine the statistical difference among participants with CRDs and those without in terms of their demographic characteristics. Binary logistic regression analysis was used to identify risk factors of CRDs. The statistical significance level was assigned as 5.0%.
Results
Participants’ Demographic Characteristics
A total of 712 participants were involved in this study. More than half of them were males (n = 471; 66.2%). Around 38.0% of the participants (n = 268) were aged below 30 years. Around 61.0% (n = 438) of them were married. Almost half of the participants (n = 370; 52.0%) reported that they hold bachelor degree. Almost one-third of the study participants (n = 245; 34.4%) reported that they work outside the healthcare sector. Around 58.0% of the participants (n = 416) reported that work in office-based working settings. For further information on the demographic characteristics of the study participants, refer to Table 1.
 |
Table 1 Participants’ Demographic Characteristics |
Respiratory Diseases History Profile
Around one-third of the study participants (n = 218; 30.6%) reported that either themselves or one of their family members suffer from respiratory diseases. Asthma was the most commonly reported (n = 167; 76.8%) respiratory disease among respiratory disease patients. Almost half of respiratory disease patients (n = 101; 46.3%) reported that they have suffering from their respiratory diseases since more than five years. Only one-quarter of respiratory disease patients (n = 58; 26.8%) reported that have been diagnosed with respiratory disease by licensed physician. Chest x-ray (n = 158; 72.5%) and lungs function test (n = 79; 36.2%) were the most two commonly reported tests performed for respiratory disease patients. Hypertension was the most commonly (n = 21; 9.7%) reported comorbidity among respiratory disease patients. Around one-fifth of the respiratory disease patients (n = 47; 21.5%) reported that they have experienced wheezing during the last 12 months while breathing. Almost half of the respiratory disease patients (n = 114; 52.3%) reported that wheezing happen with or without cold.
Around 67.0% (n = 146) of respiratory disease patients who have respiratory diseases reported that they wake up because of shortness of breath or chest tightness. Almost one-third of respiratory diseases patients reported that they complain from runny nose (n = 73; 33.5%) and eye redness and itching (n = 77; 35.3%). Around two-thirds (n = 149; 68.3%) of respiratory diseases patients reported that they have seasonal allergy and 45.0% (n = 97) of them reported that they have done allergy test before. Around half of respiratory disease patients (n = 116) reported that they refer to a hospital or a specialist doctor for their condition.
A total of 32.0% (n = 70) of respiratory diseases patients reported that they deal with dust or chemicals such as paints, fertilizers and cleaning tools on a regular basis at work or at home. Around 62.0% (n = 134) of respiratory diseases patients reported that exposure to fumes, perfumes, or the like affect their health. Around 78.0% (n = 169) of them reported that weather change in summer affects their health and 63.0% (n = 138) of them reported that cold weather in winter affects their health. Around one-quarter of respiratory disease patients (n = 60) reported that they live near or have direct contact with animals. Almost 26.0% of respiratory disease patients (n = 58) reported that they are either a current smokers of ex-smoker. For further details on patients’ respiratory diseases history profile, refer to Table 2.
 |
Table 2 Patients’ Respiratory Diseases History Profile |
Medications Use and Knowledge About Respiratory Diseases
Table 3 shows respiratory diseases patients’ medications use and knowledge about respiratory diseases. The vast majority of the patients reported that they do not take medications for their respiratory conditions. The most commonly reported medications were inhaled bronchodilators and oral bronchodilators with 38.2% (n = 83) and 24.6% (n = 54), respectively. A total of 18.0% of respiratory disease patients (n = 39) reported that they take traditional or herbal medicine to treat their respiratory disease.
 |
Table 3 Patients” Medications Use and Knowledge About Respiratory Diseases |
When the participants were asked about the population who is at higher risk of developing respiratory diseases, 38.5% of the participants (n = 274) reported that children are at higher risk of developing this type of diseases. The most commonly reported causes of respiratory diseases were air pollution and dust with 50.4% (n = 359) and 48.2% (n = 343), respectively.
Participants’ Demographic Characteristics and Their CRDs Status
Table 4 presents the demographic characteristics of the study participants stratified per their CRDs status. Chi-squared test showed that there is no statistically significant difference between participants who have CRD and those who are CRD free (p > 0.05). Binary logistic regression analysis identified that participants aged 41–50 years were 38.0% less likely to have CRDs compared to others (p < 0.05), Table 5.
 |
Table 4 Participants’ Demographic Characteristics and Their CRDs Status |
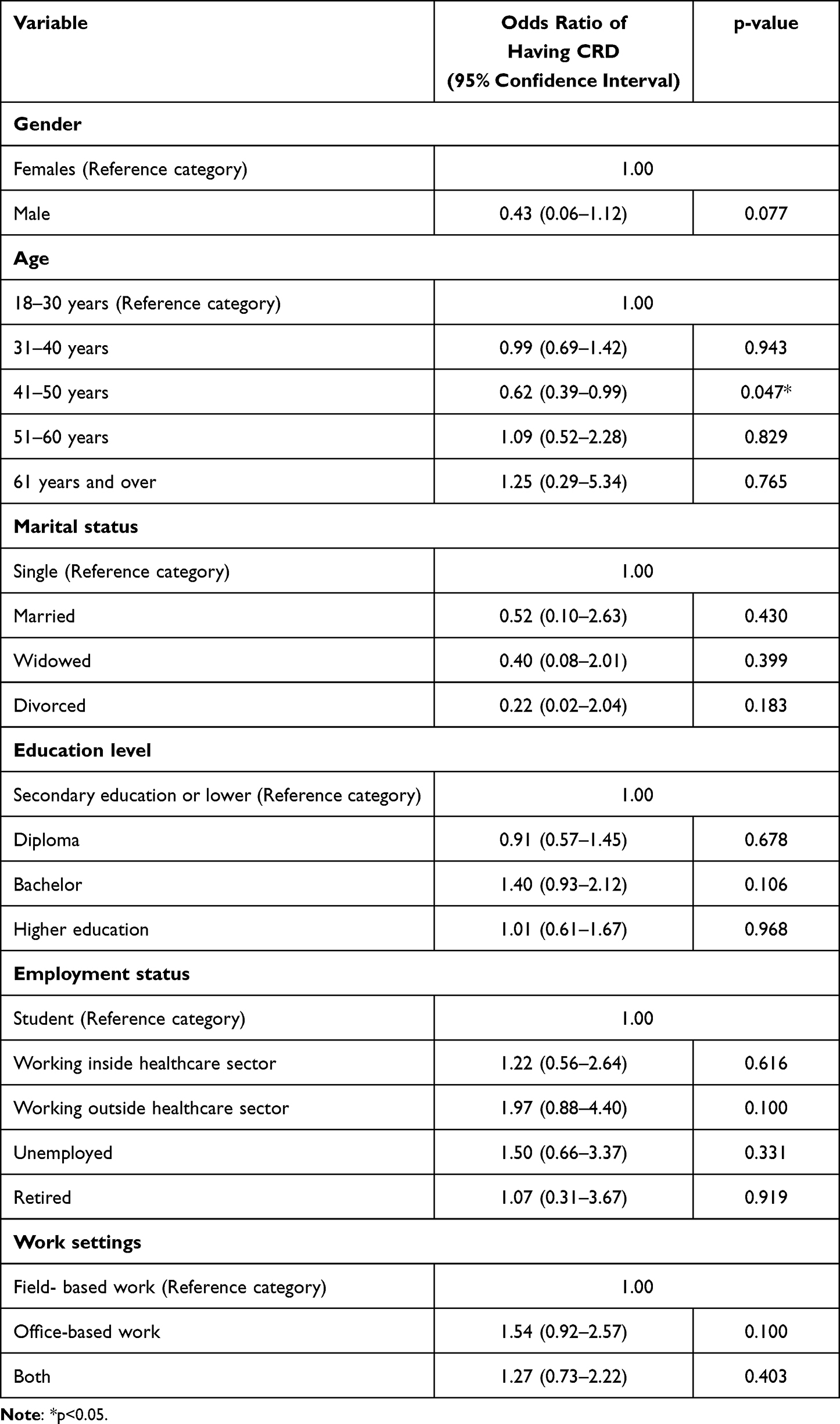 |
Table 5 Binary Logistic Regression Analysis |
Discussion
This study is among the first few studies to investigate the knowledge, prevalence of CRDs, and utilization of their medications among the adults at Najran region, Saudi Arabia. Characterizing respiratory health is essential for comprehending the population’s overall health. A variety of health disorders, including obstructive lung illnesses and heart ailments, may cause shortness of breath or coughing, making respiratory symptoms prevalent.21 The aim of this study was to investigate the knowledge, and prevalence of CRDs and related risk factors among the adults at Najran region, Saudi Arabia. The key findings are: 1) around one-third of the study participants reported that either themselves or one of their family members suffer from respiratory diseases and asthma was the most commonly reported respiratory, 2) chest x-ray and lungs function test were the most two commonly reported tests performed for respiratory disease patients, 3) around one-third of respiratory diseases patients reported that they deal with dust or chemicals such as paints, fertilizers and cleaning tools on a regular basis at work or at home, 4) the majority of them reported that weather change in summer affects their health and reported that cold weather in winter affects their health, 5) the vast majority of the patients reported that they do not take medications for their respiratory conditions, 6) more than one-third of the participants reported that children are at higher risk of developing this type of diseases, and 7) participants aged 41–50 years were 38.0% less likely to have CRDs compared to others.
In our study, around one-third of the study participants (30.6%) reported that either themselves or one of their family members suffer from respiratory diseases. Asthma was the most commonly (76.8%) reported respiratory disease among respiratory disease patients. This was confirming the findings of previous study in the USA, which reported that almost 40% of adults reported having at least one moderate or severe respiratory symptom, asthma or COPD.21 Another study in Italy also reported high prevalence of asthma symptoms and COPD diagnosis.23 Similarly, in Pakistan, a previous study reported that 37.5% of the participants reported having at least one respiratory symptom.24 The development of respiratory symptoms is governed by a variety of environmental and behavioral risk factors, the persistence of which results in chronic airway distress and, ultimately, respiratory illnesses.25 There is a lack of consistency on the criteria of respiratory symptoms, resulting in variances in estimates among studies; however, these disparities may also be attributable to cultural differences in reporting respiratory symptoms.26 Taking sex and environmental variables into consideration, research has shown that females are more susceptible to respiratory problems, presumably owing to the use of biomass fuel for cooking or heating in some countries.27 According to spirometry-determined airflow limitation and/or objective evidence of structural or physiological pulmonary dysfunction, COPD is a heterogeneous lung condition characterized by chronic respiratory symptoms (dyspnea, cough, expectoration) brought on by persistent abnormalities of the airways (bronchitis, bronchiolitis), alveoli (emphysema), and/or pulmonary vessels.28 Chronic obstructive pulmonary disease (COPD) is distinguished by the presence of remodeling in both the distal airways and parenchyma, which can be conceptualized as a consequence of impaired regenerative mechanisms.29 According to Morrissey's findings, persons with COPD exhibit distinct gene expression patterns in their endothelium and mesenchymal cells compared to those who are healthy.29 Specifically, the researchers demonstrated that the distal airway multipotent respiratory airway secretory (RAS) cells, which typically have the ability to regenerate alveoli in humans by transforming into alveolar type II epithelial (ATII) pneumocytes cells, undergo an abnormal differentiation process. This results in the buildup of transitioning cells from RAS to ATII in the lungs of individuals with chronic obstructive pulmonary disease (COPD).30 The presence of these cells is likely indicative of an effort to regenerate, which is hindered by a reduced ability to transition from RAS to ATII cells. This ultimately results in the failure of lung regeneration in individuals with COPD.30
In our study, a total of 32.0% of respiratory diseases patients reported that they deal with dust or chemicals such as paints, fertilizers and cleaning tools on a regular basis at work or at home. The increasing exposure of individuals to a poor work environment and air pollution has a negative impact on their airways and general physiology.31 Regular air conditioning usage has been linked to wheezing and shortness of breath in seven studies.16,24,32–36 This, together with the presence of mould in the home, implies that the hot and humid environment of the nation may cause allergens to cause chronic wheezing.37
In our study, around 78.0% of them reported that weather change in summer affects their health and 63.0% of them reported that cold weather in winter affects their health. The seasonal cycle of respiratory virus infections has been extensively acknowledged for decades. Many years have been devoted to examining and debating the processes underpinning the seasonal character of respiratory virus infections. Changes in environmental characteristics and human conduct are the two most important contributors.38,39 The stability and transmission rates of respiratory viruses are affected by temperature and humidity, according to studies. Recent study emphasizes the significance of environmental conditions, particularly temperature and humidity, in influencing the host’s intrinsic, innate, and adaptive immune responses to viral respiratory tract infections.38,40 The modulation of airway defense systems by environmental conditions affects host vulnerability, as well as the survival and transmission of respiratory viruses.40 The contact rates between infected and vulnerable people are influenced by the behaviors of humans.39
In our study, the vast majority of the patients reported that they do not take medications for their respiratory conditions. A previous study in Poland reported moderate level of adherence to medications among patients with COPD.41 This research found that 74% of patients had sporadic noncompliance and concluded that patients with obstructive lung diseases have moderate medication adherence.41 In addition, they found that the influence of beliefs about medicines on drug adherence is substantial.41 In everyday clinical practice, adherence rates among patients with asthma and COPD often do not surpass 50%.42 Observational studies reflecting real-world clinical practice reveal that adherence rates for patients with chronic obstructive pulmonary disease vary between 10% and 40%.43,44 Asthma patients frequently expressed higher levels of satisfaction with their inhaler devices in comparison to individuals diagnosed with COPD.45
In our study, 38.5% of the participants reported that children are at higher risk of developing this type of diseases. In children under the age of five, lung disorders, including both acute infectious processes and chronic problems, are among the leading causes of mortality.26 Significantly, asthma is the most prevalent chronic illness, affecting around 14% of children worldwide, and its incidence is growing.46 Babies and young children are more prone to this progression of adverse clinical consequences.3
This study has limitations. The cross-sectional study design restricted our ability to determine causality among study variables. The use of convenience sampling technique restricted our ability to have more representative sample and thus limited the generalisability of our study findings. This could be noticed from the demographic distribution of our study participants (only 6.0% of the participants were aged above 50 years). We did not estimate the number of participants who received the study questionnaire, therefore, we are not able to estimate the response rate, which might increase the possibility of non-response bias. Therefore, our findings should be interpreted carefully.
Conclusion
Respiratory symptoms are prevalent among the Saudi population in the southern region of Najran. We did not identify statistically significant association between participants’ demographic characteristics and their CRD status. This highlights the imperative for public health authorities to implement actions. Healthcare facilities in the region may be required to commit resources in order to effectively meet the increased demand for respiratory care. Additionally, there is a necessity for intensified disease surveillance and monitoring efforts. Further studies are warranted to identify preventable risk factors and develop interventions to counteract them. Healthcare professionals are advised to enhance in their educational effort in teaching their patients on respiratory diseases preventive measures.
Data Sharing Statement
All data are available on request from the corresponding authors.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Scientific Research Ethical Committee, Deanship of Scientific Research, at Najran University, Najran, Saudi Arabia (Reference No.:443-41-66963-DS). Informed consent was obtained from all subjects involved in the study. The study was designed and conducted in accordance with the ethical principles that have their origin and comply with in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors are thankful to the Deanship of Scientific Research at Najran University for funding this work, under the General Research Funding program grant code (NU/NRP/MRC/12/38).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR.; GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Schneider JL, Rowe JH, Garcia-de-alba C, Kim CF, Sharpe AH, Haigis MC. The aging lung: physiology, disease, and immunity. Cell. 2021;184(8):1990–2019. doi:10.1016/j.cell.2021.03.005
3. World Health Organization. Chronic respiratory diseases; 2023. Available from: https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_1.
4. Yorgancioglu A, Khaltaev N, Bousquet J, Varghese C. The global alliance against chronic respiratory diseases: journey so far and way ahead. Chin Med J. 2020;133(13):1513–1515. doi:10.1097/CM9.0000000000000851
5. Dalju I, Dessie A, Bogale L, Mekonnen TH. Occupational risk factors associated with respiratory symptoms among tannery workers in Mojo town, Southeast Ethiopia, 2018: a comparative cross-sectional study. Multidiscip Respir Med. 2019;14:1–10. doi:10.4081/mrm.2019.25
6. de Perio MA, Kobayashi M, Wortham JM. Occupational respiratory infections. Clin Chest Med. 2020;41(4):739–751. doi:10.1016/j.ccm.2020.08.003
7. Rojas M, Mora AL, Kapetanaki M, Weathington N, Gladwin M, Eickelberg O. Aging and lung disease. Clinical Impact and cellular and molecular pathways. Ann Am Thorac Soc. 2015;12(12):S222–S227. doi:10.1513/AnnalsATS.201508-484PL
8. The Forum of International Respiratory Societies. Latest News; 2023. Available from: https://www.firsnet.org/.
9. Booth S, Johnson MJ. Improving the quality of life of people with advanced respiratory disease and severe breathlessness. Breathe. 2019;15(3):198–215. doi:10.1183/20734735.0200-2019
10. Caballero MT, Bianchi AM, Nuño A, et al. Mortality associated with acute respiratory infections among children at home. J Infect Dis. 2019;219(3):358–364. doi:10.1093/infdis/jiy517
11. Al Rajeh AM, Naser AY, Siraj R, et al. Acute upper respiratory infections admissions in England and Wales. Medicine. 2023;102(21):e33616. doi:10.1097/MD.0000000000033616
12. Alwafi H, Naser AY, Ashoor DS, et al. Trends in hospital admissions and prescribing due to chronic obstructive pulmonary disease and asthma in England and Wales between 1999 and 2020: an ecological study. BMC Pulm Med. 2023;23(1):49. doi:10.1186/s12890-023-02342-6
13. Naser AY. Hospitalisation profile in England and Wales, 1999 to 2019: an ecological study. BMJ Open. 2023;13(4):e068393. doi:10.1136/bmjopen-2022-068393
14. Naser AY, Mansour MM, Alanazi AFR, et al. Hospital admission trends due to respiratory diseases in England and Wales between 1999 and 2019: an ecologic study. BMC Pulm Med. 2021;21(1):356. doi:10.1186/s12890-021-01736-8
15. Alqahtani JS. Prevalence, incidence, morbidity and mortality rates of COPD in Saudi Arabia: trends in burden of COPD from 1990 to 2019. PLoS One. 2022;17(5):1–12. doi:10.1371/journal.pone.0268772
16. Alomary SA, Al Madani AJ, Althagafi WA, et al. Prevalence of asthma symptoms and associated risk factors among adults in Saudi Arabia: a national survey from global asthma network phase I. World Allergy Organ J. 2022;15(1):1–11. doi:10.1016/j.waojou.2021.100623
17. Alamoudi O. Prevalence of respiratory diseases in hospitalized patients in Saudi Arabia: a 5 years study 1996–2000. Ann Thorac Med. 2006;1(2):76–80. doi:10.4103/1817-1737.27106
18. Al Ghobain M, Al-Hajjaj MS, Wali SO. Prevalence of chronic obstructive pulmonary disease among smokers attending primary healthcare clinics in Saudi Arabia. Ann Saudi Med. 2011;31(2):129–133. doi:10.4103/0256-4947.77485
19. Moradi-Lakeh M, El Bcheraoui C, Daoud F, et al. Prevalence of asthma in Saudi adults: findings from a national household survey, 2013. BMC Pulm Med. 2015;15(1):1–7. doi:10.1186/s12890-015-0080-5
20. Alshahrani ZM. Survey of COPD Knowledge, Skills, and Attitudes Among Saudi Arabian Respiratory Therapists. Georgia state Univeristy; 2021.
21. Pleasants RA, Heidari K, Ohar J, et al. Respiratory Symptoms among US adults: a cross-sectional health survey study. Pulm Ther. 2022;8(3):255–268. doi:10.1007/s41030-022-00194-9
22. Rodrigues da Costa M, Fitzgerald RM, Manzanilla EG, et al. A cross-sectional survey on respiratory disease in a cohort of Irish pig farms. Ir Vet J. 2020;73(1):1–10. doi:10.1186/s13620-020-00176-w
23. Maio S, Baldacci S, Carrozzi L, et al. Respiratory symptoms/diseases prevalence is still increasing: a 25-yr population study. Respir Med. 2016;110:58–65. doi:10.1016/j.rmed.2015.11.006
24. Akhter Z, Razzaq S, Rabbani U, Irfan M, Burney P, Nafees AA. Prevalence of and risk factors for respiratory symptoms in an adult urban population. Int J Tuberc Lung Dis. 2021;25(1):16–22. doi:10.5588/ijtld.20.0057
25. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/S0140-6736(09)61303-9
26. Burney P, Jarvis D, Perez-Padilla R. The global burden of chronic respiratory disease in adults. Int J Tuberc Lung Dis. 2015;19(1):10–20. doi:10.5588/ijtld.14.0446
27. Ramírez-Venegas A, Velázquez-Uncal M, Pérez-Hernández R, et al. Prevalence of COPD and respiratory symptoms associated with biomass smoke exposure in a suburban area. Int J Chron Obstruct Pulmon Dis. 2018;13:1727–1734. doi:10.2147/COPD.S156409
28. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
29. Confalonieri M, Braga L, Salton F, Ruaro B, Confalonieri P. Chronic obstructive pulmonary disease definition: is it time to incorporate the concept of failure of lung regeneration? Am J Respir Crit Care Med. 2023;207(3):366–367. doi:10.1164/rccm.202208-1508LE
30. Basil MC, Cardenas-Diaz FL, Kathiriya JJ, et al. Human distal airways contain a multipotent secretory cell that can regenerate alveoli. Nature. 2022;604(7904):120–126. doi:10.1038/s41586-022-04552-0
31. Chen X, Zhang X, Zhang X. Smog in Our Brains: Gender Differences in the Impact of Exposure to Air Pollution on Cognitive Performance in China. Washington DC, USA: International Food Policy Research Institute; 2017.
32. Huang S, Garshick E, Weschler LB, et al. Home environmental and lifestyle factors associated with asthma, rhinitis and wheeze in children in Beijing, China. Environ Pollut. 2020;256:113426. doi:10.1016/j.envpol.2019.113426
33. Larenas-Linnemann D, Romero-Tapia SJ, Virgen C, Mallol J, Baeza Bacab MA, García-Marcos L. Risk factors for wheezing in primary health care settings in the tropics. Ann Allergy Asthma Immunol. 2020;124(2):179–184. doi:10.1016/j.anai.2019.11.008
34. Mészáros D, Burgess J, Walters EH, et al. Domestic airborne pollutants and asthma and respiratory symptoms in middle age. Respirology. 2014;19(3):411–418. doi:10.1111/resp.12245
35. Turner MO, Noertjojo K, Vedal S, Bai T, Crump S, Fitzgerald JM. Risk factors for near-fatal asthma. A case-control study in hospitalized patients with asthma. Am J Respir Crit Care Med. 1998;157:1804–1809. doi:10.1164/ajrccm.157.6.9708092
36. Zuraimi MS, Tham KW, Chew FT, Ooi PL, Koh D. Home air-conditioning, traffic exposure, and asthma and allergic symptoms among preschool children. Pediatr Allergy Immunol. 2011;22:e112–e118. doi:10.1111/j.1399-3038.2010.00992.x
37. Johnston JD, Barney TP, Crandall JH, et al. Prevalence of house dust mite allergens in low-income homes with evaporative coolers in a semiarid climate. Arch Environ Occup Health. 2018;73(1):38–41. doi:10.1080/19338244.2017.1282846
38. Moriyama M, Hugentobler WJ, Iwasaki A. Seasonality of respiratory viral infections. Annu Rev Virol. 2020;7(1):83–101. doi:10.1146/annurev-virology-012420-022445
39. Azziz Baumgartner E, Dao CN, Nasreen S, et al. Seasonality, timing, and climate drivers of influenza activity worldwide. J Infect Dis. 2012;206(6):838–846. doi:10.1093/infdis/jis467
40. Peci A, Winter AL, Li Y, et al. Effects of absolute humidity, relative humidity, temperature, and wind speed on influenza activity in Toronto, Ontario, Canada. Appl Environ Microbiol. 2019;85(6):1–13. doi:10.1128/AEM.02426-18
41. Homętowska H, Świątoniowska-lonc N, Klekowski J, Chabowski M, Jankowska-Polańska B. Treatment adherence in patients with obstructive pulmonary diseases. Int J Environ Res Public Health. 2022;19(18):1–14. doi:10.3390/ijerph191811573
42. Wiśniewski D, Porzezińska M, Gruchała-Niedoszytko M, Niedoszytko M, Słomiński JM, Jassem E. Factors influencing adherence to treatment in COPD patients and its relationship with disease exacerbations. Pneumonol Alergol Pol. 2014;82(2):96–104. doi:10.5603/PiAP.2014.0015
43. Terzano C, Cremonesi G, Girbino G, et al. PRISMA (PRospectIve Study on asthMA control) study group, 1-year prospective real life monitoring of asthma control and quality of life in Italy. Respir Res. 2012;13(1):1–11. doi:10.1186/1465-9921-13-112
44. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
45. Thi HDN, Van GV. The satisfaction and adherence to inhaler devices among patients with chronic obstructive pulmonary disease and asthma at a tertiary hospital in Viet Nam. J Func Vent Pulm. 2021;38:1–78.
46. Pearce N, Aït-Khaled N, Beasley R, et al.; ISAAC Phase Three Study Group. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma And Allergies in Childhood (ISAAC). Thorax. 2007;62(9):758–766. doi:10.1136/thx.2006.070169
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.