")
Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence and Genetype Distribution of Human Papillomavirus in Women with Condyloma Acuminatum in Henan Province, Central China
Authors Chen G , Gao L, Zheng P , Liu Y, Li P, Liu H
Received 25 May 2023
Accepted for publication 20 July 2023
Published 28 July 2023 Volume 2023:16 Pages 4919—4928
DOI https://doi.org/10.2147/IDR.S418783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Guanghui Chen, Lan Gao, Peiming Zheng, Yanhong Liu, Pan Li, Huifang Liu
Department of Clinical Laboratory, Henan Provincial People′s Hospital, People’s Hospital of Zhengzhou University, People’s Hospital of Henan University, Zhengzhou, People’s Republic of China
Correspondence: Guanghui Chen, Department of Clinical Laboratory, Henan Provincial People′s Hospital, People’s Hospital of Zhengzhou University, People’s Hospital of Henan University, No. 7 Weiwu Road Jinshui District, Zhengzhou, 450003, People’s Republic of China, Email [email protected]
Purpose: This study aims to analyze the distribution of human papillomavirus (HPV) genotypes and the associations of demographic characteristics with HPV infection among women with condyloma acuminatum (CA) in Henan Province of China.
Methods: From January 2019 to October 2022, 702 women with CA were sampled for HPV subtypes and surveyed by questionnaire at Henan Provincial People′s Hospital. The HPV genotype was tested by flow-through hybridization after polymerase chain reaction (PCR).
Results: The location of warts was mainly vulva. The age of the subjects was mainly distributed in the 20– 29-year-old, followed by 30– 39-year-old. The most common subtypes were HPV 6 (43.59%), 11 (24.93%), 16 (11.82%), 52 (7.83%), 58 (7.55%), 51 (7.26%), 61 (5.70%), 39 (5.56%), 18 (5.13%), and 54 (4.70%), our results also suggested that HPV 6 and 11 were the dominant genotypes in each age group. The infection of low-risk HPV (LR-HPV) (74.50%) and single HPV (47.01%) were the main categories. In terms of educational level, women with senior high school or above were inclined to infect single and pure-LR HPV. Unmarried status, sometimes or never condom use increased the chances of multiple, pure high-risk (HR) and mixed HPV infections. Women with multiple sex partners were more likely to cause multiple and mixed HPV infections.
Conclusion: Our experimental data on the prevalence and subtype distribution of HPV in women with CA could provide valuable reference for preventing CA in Henan Province. The application of the nine-valent vaccine provides a broad prospect for female CA prevention.
Keywords: human papillomaviruses, condyloma acuminatum, genetype distribution, prevalence, central China
Introduction
As one of the most common venereal disease, condyloma acuminatum (CA) is an epidermal hyperplasia of the urogenital organs and perianal skin, which is caused by the infection of human papillomavirus (HPV). The appearance of CA is obviously papillary and can be diagnosed by observing its special appearance.1 The annual incidence of CA (including new and recurrent) ranged from 160 to 289 per 100,000, with a median of 194.5 per 100,000.2 The treatment for CA is generally classified into surgical and medical therapies at present.
So far, more than 200 different HPV subtypes have been identified, approximately 40 of which are capable of infecting the urogenital mucosal epithelium.3 Based on carcinogenicity, HPV subtypes can be divided into high-risk HPV (HR-HPV) and low-risk HPV (LR-HPV).4 HR-HPV genotypes are known as oncogenic and mainly include HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 82.5 LR-HPV genotypes generally only cause benign lesions and mainly include HPV 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81.6
Geographical variations in HPV genotypes have been reported, even within the same country.7,8 Due to the vast size of China, it is possible that the distribution of HPV genotypes varies across different regions. The distribution of HPV genotypes in CA varies with geographical location, while demographic factors (such as age, education level, marital status, etc.) may influence the type of HPV infection.
Females with CA tend to suffer greater psychological impact than males,9 which is the reason we are specifically working on the HPV genotypes among females with CA. In addition, there are few studies on HPV genotype distribution and clinical and demographic characteristics of patients with CA in Henan Province, a large agricultural region in Central China with a population of nearly 100 million. Therefore, it is necessary to gain a deeper understanding of the distribution of HPV genotypes and clinical and demographic characteristics of female CA patients in Central China, as this information can provide valuable insights for preventing CA in females.
Materials and Methods
Study Population
The study population was comprised of women who attended gynecology, dermatology, or urology department and were diagnosed as CA from January 2019 to October 2022 in Henan Provincial People′s Hospital. The diagnosis of CA referred to the Guideline for the Diagnosis and Treatment of Condyloma Acuminatum (2014 edition) and the Guideline for the Clinical Management of Anogenital Warts in China (2021 edition).10
The women in the study had to conform to the following inclusion criteria: ① newly diagnosed with CA, not a recurrence; ② not diagnosed with cervical lesions previously; ③ resided in Henan Province; ④ no treated for CA currently; ⑤ had not recently taken antiviral drugs; ⑥ agreed to undergo HPV testing and questionnaire survey.
A total of 746 women were invited to participate in this study. Forty-four women refused to take the questionnaire due to concern of privacy or time consumption, and eventually 702 women were enrolled in this study.
Ethical Statement
This study was approved by the Ethics Committee of Henan Provincial People’s Hospital. All the specimens and clinical information of the participants were obtained according to protocols approved by the Ethics Committee, and informed consent was obtained from the study participants or legal guardians of the minor participants prior to study commencement. Patient information was managed in strict accordance with the Declaration of Helsinki.
Specimen Collection
Exfoliated cells from wart tissue were collected using a disposable cytobrush for HPV genotyping by an experienced gynecologist, dermatologist, or urologist before treatment. For patients with more than one wart, exfoliated cells were collected from each wart. After collection, the exfoliated cells were immediately placed in a sterile tube containing 3.5 mL sample preservation solution and stored at 4°C until processing.
HPV DNA Extraction, PCR Amplication, and Genotyping
DNA was obtained from damaged cells using the DNA Mag-Ax Kit (HybriBio Ltd.) via an automatic nucleic acid extractor (HBNP-4801A, HybriBio Ltd.). By amplifying the β-globin gene as an internal control, the quality of the extracted DNA was confirmed. In addition, positive and negative quality control products were extracted during the whole process as the control group. According to the manufacturer’s protocols, the extracted DNA was amplified with the PCR kit (HybriBio Ltd.), and then HPV genotyping was performed with the HPV Genotyping Kit (HybriBio Ltd.). Eventually, 37 HPV genotypes could be detected, including 18 HR-HPV types (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82) and 19 LR-HPV types (6, 11, 34, 40, 42, 43, 44, 54, 55, 57, 61, 67, 69, 70, 71, 72, 81, 83, and 84).
Statistical Analysis
Statistical analysis was performed by SPSS version 23.0 (IBM, Armonk, NY, USA). The difference between two groups was compared using chi-square test. Unconditional logistic regression was used for odds ratios (ORs) with 95% confidence intervals (CIs). All the P values were 2-sided, and a P < 0.05 was considered statistically significant.
Results
Clinical and Demographic Characteristics of the Subjects
A total of 702 women with CA aged 13–70 years were enrolled in this study. The mean age was 29.5 ± 10.5 years. The clinical characteristics are described in Table 1. The location of warts was mainly vulva (91.88%), and there were 11 females with more than one body part of warts (3 females with vulva+vagina, 2 females with vulva+cervix, 2 females with vulva+crissum, 1 female with vagina+cervix, 3 females with vulva+vagina+cervix). The majority of population were aged 20–29 years, followed by 30–39 years. There were more women who attended senior high school or above (64.67%) and were married (59.69%). In addition, there were 28 women in pregnancy. Nearly one-third of the women had two or more sexual partners in the past year, and only 7.55% used a condom every time.
 |
Table 1 Clinical and Demographic Characteristics in 702 Women with CA |
Prevalence and Genotype Distribution of HPV
Table 2 lists the detection results of HPV genotypes. Except for HPV 57 and 72, the remaining 35 of the 37 HPV genotypes were found, including 17 LR-HPV genotypes (6, 11, 34, 40, 42, 43, 44, 54, 55, 61, 67, 69, 70, 71, 81, 83, and 84) and 18 HR-HPV genotypes (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82). The overall rate of HPV infection was 88.18% (619/702). The top ten prevalent genotypes were HPV 6 (43.59%), 11 (24.93%), 16 (11.82%), 52 (7.83%), 58 (7.55%), 51 (7.26%), 61 (5.70%), 39 (5.56%), 18 (5.13%), and 54 (4.70%). HPV 6 was the most common LR-HPV, and HPV 16 was the most common HR-HPV. HPV 6/11 were detected in 66.24% (465/702) of all patients, accounting for 75.12% (465/619) of HPV-positive patients. The detection rate of LR-HPV was higher than that of HR-HPV (χ2 = 116.700, P < 0.001).
 |
Table 2 Distribution of HPV Genotypes Among 702 Women with CA |
Category Distribution of HPV Infection
As shown in Table 3, the infection rate of single HPV genotype (47.01%, 330/702) was slightly higher than that of multiple HPV genotypes (41.17%, 289/702) (χ2 = 4.857, P < 0.05). Double infections were the predominant category of multiple infections. Single infection was mainly LR-HPV, while multiple infections were mainly mixed with LR and HR HPV. As a whole, pure-LR HPV infections (41.88%, 294/702, including single and multiple LR-HPV infections) were the dominant infection form, followed by mixed HPV infections (32.61%, 229/702, including HR-HPV and LR-HPV mixed infections).
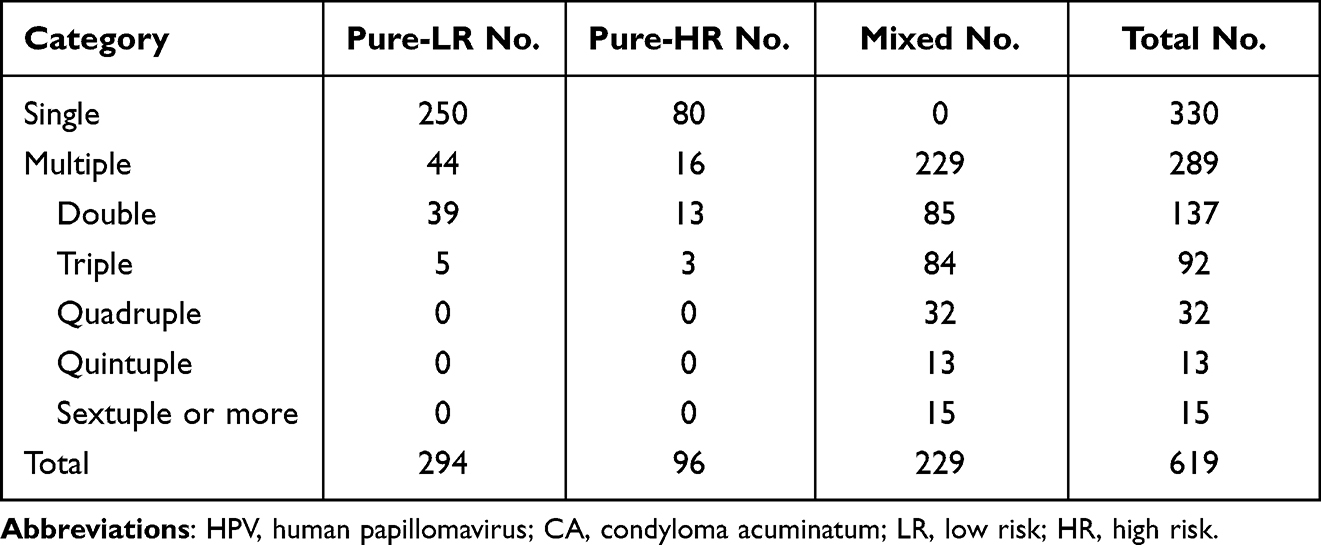 |
Table 3 Category Distribution of HPV Infection Among 619 HPV-Positive Women with CA |
Prevalence and Genotype Distribution of HPV Grouped by Age
Table 4 shows that HPV 6 and 11 were the dominant genotypes in each age group. The prevalence of single and multiple HPV infections in each age group is displayed in Figure 1. The prevalence was different between single and multiple HPV infections in the 13–19-year-old (χ2 = 12.367, P < 0.001) and 30–39-year-old (χ2 = 25.405, P < 0.001) groups. The prevalence of pure-LR, pure-HR, and mixed HPV infections in each age group is displayed in Figure 2. There was a significant difference among pure-LR, pure-HR, and mixed HPV infections in each age group except the 60–70-year-old group, whereas no difference existed between pure-LR and mixed HPV infections in the 20–29-year-old group, nor between pure-HR and mixed HPV infections in the 30–39-year-old group.
 |
Table 4 Prevalence and Genotype Distribution of HPV in Each Age Group |
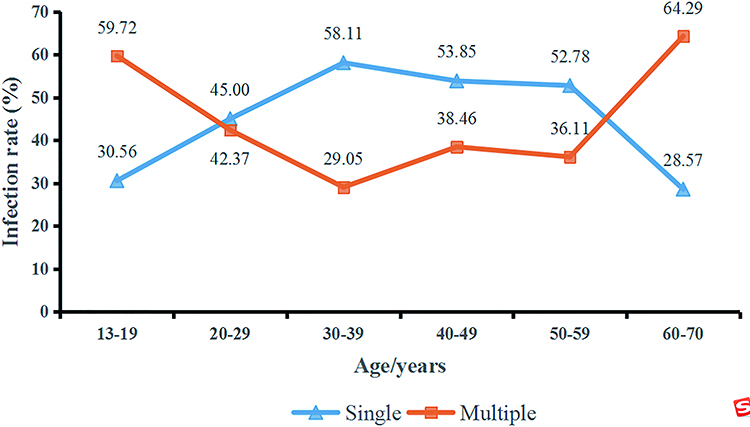 |
Figure 1 Prevalence of single and multiple HPV infections in each age group (13–19 years or 30–39 years, single vs multiple, P < 0.001). Abbreviation: HPV, human papillomavirus. |
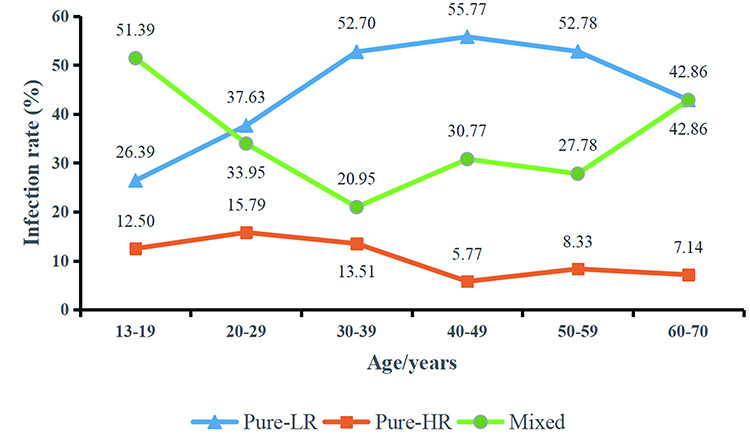 |
Figure 2 Prevalence of pure-LR, pure-HR, and mixed HPV infections in each age group. Abbreviations: LR, low risk; HR, high risk; HPV, human papillomavirus. |
Associations of Demographic Characteristics with HPV Infection
Table 5 summarizes the associations of demographic characteristics with the category of HPV infection. Women aged 20–59 years were more likely to infect single HPV, and women aged 20–70 years were more likely to suffer pure-LR HPV infection. Women with senior high school or above were inclined to suffer single and pure-LR HPV infection. Unmarried status, sometimes or never condom use increased the chances of multiple, pure-HR and mixed HPV infections. Multiple sex partners in the past year increased the chances of multiple and mixed HPV infections.
 |
Table 5 Associations of Demographic Characteristics with the Category of HPV Infection in 702 Women with CA |
Discussion
Condyloma Acuminatum (also referred to as genital warts or anogenital warts) is one of the most commonly reported sexually transmitted diseases due to the infection with some types of HPV. It is a benign lesion, but it results in direct medical costs and a substantial psychological impact on patients, especially women. Nevertheless, researches on the epidemiology of HPV infection in women with CA were quite rare in Henan Province, located in central China. In this study, we evaluated the distribution of HPV genotypes and clinical and demographic characteristics of female CA patients in Henan Province.
In our study, thirty-five different HPV genotypes were detected. The most common HPV genotypes were HPV 6 (43.59%) and 11 (24.93%), and HPV 6/11 were detected in 66.24% of all patients, accounting for 75.12% of HPV-positive patients. Moreover, HPV 6 and 11 were the main genotypes in each age group. It has been reported that more than 90% of CA patients are caused by the low-risk HPV types 6 and 11,11,12 which was higher than that in our study. The difference may be explained by the size and characteristics of the study populations, and different sensitivities of HPV genotyping methods. HPV 16 was confirmed to be the most prevalent HR-HPV genotype and the third most prevalent HPV genotype after HPV 6 and 11 in this study. From a multi-center study, HPV 6, 11, and 16 were the three most common genotypes among genital wart cases (including male and female) in China.13 In addition, HR-HPV 52 and 58 were the fourth and fifth most prevalent genotypes in this study. Previous data has confirmed that HPV 52 and 58 were more prevalent than HPV-18 in Chinese women,14,15 which was different from the results of women in western countries.16
HPV 6, 11, 52, 16, and 58 have been identified as the top five prevalent HPV genotypes causing female genital warts in Beijing and Xi’an,17,18 which is similar to our study except the order of HPV 16 and 52 and may be explained by the geographical proximity. In Shandong Province, which also lies near Henan, the top five prevalent HPV genotypes of CA were HPV 6, 11, 16, 42, and 52 (including male and female).19 This finding is similar to our study except for the fourth and fifth positions, which may be attributed to gender differences in the study population. In Guangzhou, located in southern China, the top five prevalent HPV genotypes of female CA were HPV 6, 52, 11, 16, and 53,20 which is different from our study and may be due to geographical difference. In this study, there were six HR-HPV genotypes in the top ten prevalent genotypes, so we should pay more attention to prevent CA patients infected with HR-HPV from cancerization. The nine-valent vaccine (which targets for HPV 6, 11, 16, 18, 31, 33, 45, 52, and 58) could better protect women from CA in this region but could not cover all of the HPV subtypes that we most commonly detected.
In this study, the infection rate of single HPV genotype was higher than that of multiple HPV genotypes and double infections were the predominant category of multiple infections, similar to some other reports.13,17,20 The results of this study indicated that 41.17% of women with CA had multiple HPV genotype infections, which is significantly higher than that reported by Chang et al.13 The high infection rate of multiple HPV genotypes among women with CA in Henan Province should be taken seriously, because multiple HPV infections were associated with an increased risk of HPV persistence and might make CA become more severe and worse prognosis.6,21,22 The pure-LR HPV infections were the dominant form of infection in our study, indicating that CA was mainly caused by LR-HPV, which is in line with most studies.6,13,17,19
The most common location of warts in women was the vulva in our study (91.88%), consistent with the report from a retrospective analysis.23 The majority of our subjects were aged 20–29 years, followed by 30–39 years, indicating that the majority of CA were young women, in agreement with some relevant studies.2,13,17–19,23 Sexually active young women have the highest infection rate of HPV, although most women will be infected at least once in their lifetime. The high rate of HPV infection in young women increase the risk of CA. Besides, there were 26 cases under the age of 18 in our study, which propose an issue with legal and sexual abuse about children and adolescents. The 28 pregnant women with CA in this study should also be concerned. During pregnancy, the size of genital warts tends to increase, which can bring some problems to the therapeutic management; on the other hand, vaginal delivery can expose newborns to the risk of HPV infection.24,25
We also found that women aged over 20 years or with senior high school or above were more likely to infect single and pure-LR HPV infection. Unmarried status, sometimes or never condom use were inclined to suffer multiple, pure-HR and mixed HPV infections. Multiple sex partners in the past year increased the chances of multiple and mixed HPV infections. Many studies have confirmed that the most common risk factor for HPV infection and clinical sequelae in both men and women was the high number of sexual partners.19,26,27 In addition, there was a higher proportion of women who attended senior high school or above and married, consistent with previous reports.9,13
This study provided the prevalence and genotype distribution of HPV and the associations of demographic characteristics with HPV infection among women with CA in Henan Province of China. But there were also several limitations in our study. First, the demographic characteristics of the subjects were incomplete, and some information was not collected, such as occupation, income and sexual style. Second, high recurrence rate is an important problem of CA, but it was not included in this study, so the relationship between HPV genotypes and the recurrence of CA should be carried out in the future study. Thirdly, although patients with previously diagnoses as cervical lesions were excluded, some patients with undetected cervical lesions might be included in study population. This might lead to biases in the results and conclusion, such as an increase in the proportion of HR-HPV.
Conclusion
In conclusion, the most prevalent genotypes of CA were HPV 6, 11, 16, 52, 58, 51, 61, 39, 18, and 54 in Henan Province, central China. LR-HPV infection and single HPV infection were the main infections. Women with senior high school or above were inclined to suffer single and pure-LR HPV infection. Unmarried status, sometimes or never condom use increased multiple, pure-HR and mixed HPV infections. Multiple sex partners increased multiple and mixed HPV infections. To understand the epidemiological characteristics of HPV infection, it is very important to formulate prevention and control strategies for CA. The application of the nine-valent vaccine provides a broad prospect for female CA prevention.
Acknowledgments
We thank the participants for contributing their data for this study. We acknowledge the gynecologists, dermatologists, and urologists in our hospital for their support and assistance on the data and specimen collections.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Nature Science Foundation of China (81802094).
Disclosure
The authors report that there is no conflict of interest in this work.
References
1. Leslie SW, Sajjad H, Kumar S. Genital Warts. Treasure Island (FL): StatPearls Publishing; 2023. PMID:28722914.
2. Patel H, Wagner M, Singhal P, Kothari S. Systematic review of the incidence and prevalence of genital warts. BMC Infect Dis. 2013;13:39. doi:10.1186/1471-2334-13-39
3. Ranjeva SL, Baskerville EB, Dukic V, et al. Recurring infection with ecologically distinct HPV types can explain high prevalence and diversity. Proc Natl Acad Sci USA. 2017;114:13573–13578. doi:10.1073/pnas.1714712114
4. Wang X, Huang X, Zhang Y. Involvement of human papillomaviruses in cervical cancer. Front Microbiol. 2018;9:2896. doi:10.3389/fmicb.2018.02896
5. Manini I, Montomoli E. Epidemiology and prevention of human papillomavirus. Ann Ig. 2018;30:28–32. doi:10.7416/ai.2018.2231
6. Cong X, Sun R, Zhang X, Wang Y, Wang L, Yu Y. Correlation of human papillomavirus types with clinical features of patients with condyloma acuminatum in China. Int J Dermatol. 2016;55:775–780. doi:10.1111/ijd.12964
7. Guan P, Howell-Jones R, Li N, et al. Human papillomavirus types in 115,789 HPV-positive women: a meta-analysis from cervical infection to cancer. Int J Cancer. 2012;131:2349–2359. doi:10.1002/ijc.27485
8. Wang R, Guo XL, Wisman GB, et al. Nationwide prevalence of human papillomavirus infection and viral genotype distribution in 37 cities in China. BMC Infect Dis. 2015;15:257. doi:10.1186/s12879-015-0998-5
9. Qi SZ, Wang SM, Shi JF, et al. Human papillomavirus-related psychosocial impact of patients with genital warts in China: a hospital-based cross-sectional study. BMC Public Health. 2014;14:739. doi:10.1186/1471-2458-14-739
10. Lacey CJ, Woodhall SC, Wikstrom A, Ross J. 2012 European guideline for the management of anogenital warts. J Eur Acad Dermatol Venereol. 2013;27:e263–70. doi:10.1111/j.1468-3083.2012.04493.x
11. Garland SM, Steben M, Sings HL, et al. Natural history of genital warts: analysis of the placebo arm of 2 randomized Phase III trials of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine. J Infect Dis. 2009;199:805–814. doi:10.1086/597071
12. Ball SL, Winder DM, Vaughan K, et al. Analyses of human papillomavirus genotypes and viral loads in anogenital warts. J Med Virol. 2011;83:1345–1350. doi:10.1002/jmv.22111
13. Chang L, Ci P, Shi J, et al. Distribution of genital wart human papillomavirus genotypes in China: a multi-center study. J Med Virol. 2013;85:1765–1774. doi:10.1002/jmv.23646
14. Wu EQ, Liu B, Cui JF, et al. Prevalence of type-specific human papillomavirus and pap results in Chinese women: a multi-center, population-based cross-sectional study. Cancer Causes Control. 2013;24:795–803. doi:10.1007/s10552-013-0162-8
15. Zeng Z, Yang H, Li Z, et al. Prevalence and genotype distribution of HPV infection in China: analysis of 51,345 HPV genotyping results from China’s largest CAP certified laboratory. J Cancer. 2016;7:1037–1043. doi:10.7150/jca.14971
16. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. Volume 100 B. A review of human carcinogens. IARC Monogr Eval Carcinog Risks Hum. 2012;100:1–441.
17. Ma L, Lu S, Jiang YW, Li M, Cong X, Cao YT. Distribution of human papillomavirus genotypes (2014–2016) in women with genital warts at a sexually transmitted disease clinic in Beijing, China. Future Virol. 2018;13:111–117. doi:10.2217/fvl-2017-0097
18. Zhu C, Wang Y, Mao W, Zhang H, Ma J. Prevalence and distribution of HPV types in genital warts in Xi’an, China: a prospective study. BMJ Open. 2019;9:e023897. doi:10.1136/bmjopen-2018-023897
19. Yuan H, Li R, Lv J, et al. Epidemiology of human papillomavirus on condyloma acuminatum in Shandong Province, China. Hum Vaccin Immunother. 2023;19:2170662. doi:10.1080/21645515.2023.2170662
20. Yang X, Li Y, Tang Y, et al. Cervical HPV infection in Guangzhou, China: an epidemiological study of 198,111 women from 2015 to 2021. Emerg Microbes Infect. 2023;12:e2176009. doi:10.1080/22221751.2023.2176009
21. Oyervides-Muñoz MA, Pérez-Maya AA, Sánchez-Domínguez CN, et al. Multiple HPV infections and viral load association in persistent cervical lesions in Mexican women. Viruses. 2020;12:380. doi:10.3390/v12040380
22. Pista A, Oliveira A, Verdasca N, Ribeiro F. Single and multiple human papillomavirus infections in cervical abnormalities in Portuguese women. Clin Microbiol Infect. 2011;17:941–946. doi:10.1111/j.1469-0691.2010.03387.x
23. Clanner-Engelshofen BM, Marsela E, Engelsberger N, et al. Condylomata acuminata: a retrospective analysis on clinical characteristics and treatment options. Heliyon. 2020;6:e03547. doi:10.1016/j.heliyon.2020.e03547
24. Wilkerson EC, Van Acker MM, Bloom BS, Goldberg DJ. Utilization of laser therapy during pregnancy: a systematic review of the maternal and fetal effects reported from 1960 to 2017. Dermatologica. 2019;45:818–828. doi:10.1097/DSS.0000000000001912
25. Sugai S, Nishijima K, Enomoto T. Management of condyloma acuminata in pregnancy: a review. Sex Transm Dis. 2021;48:403–409. doi:10.1097/OLQ.0000000000001322
26. Chelimo C, Wouldes TA, Cameron LD, Elwood J. Risk factors for and prevention of human papillomavirus (HPV), genital warts and cervical cancer. J Infect Dis. 2013;66:207–217. doi:10.1016/j.jinf.2012.10.024
27. Giuliano AR, Anic G, Nyitray AG. Epidemiology and pathology of HPV disease in males. Gynecol Oncol. 2010;117:S15–9. doi:10.1016/j.ygyno.2010.01.026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.