Back to Journals » Psychology Research and Behavior Management » Volume 16
Prevalence and Family Determinants of Geriatric Depression Among Elderly People in Elderly Support Groups in Rwanda
Authors Nshimyumuremyi E ![]() , Muziki JD
, Muziki JD ![]() , Harerimana E, Uwera T, Nshimiyimana A, Sebatukura SG, Mutabaruka J
, Harerimana E, Uwera T, Nshimiyimana A, Sebatukura SG, Mutabaruka J
Received 30 January 2023
Accepted for publication 19 April 2023
Published 26 April 2023 Volume 2023:16 Pages 1445—1455
DOI https://doi.org/10.2147/PRBM.S406386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Eric Nshimyumuremyi,1 Jean d’Amour Muziki,1,2 Eugene Harerimana,1 Thaoussi Uwera,3 Augustin Nshimiyimana,1 Siméon Gitimbwa Sebatukura,1 Jean Mutabaruka1
1Department of Clinical Psychology, College of Medicine, and Health Sciences, University of Rwanda, Kigali, Rwanda; 2Department of Tubarerere Mu Muryango (TMM), National Child Development Agency (NCD), Kigali, Rwanda; 3Department of Health Informatics, College of Medicine, and Health Sciences, University of Rwanda, Kigali, Rwanda
Correspondence: Jean d’Amour Muziki, Department of Tubarerere Mu muryango (TMM), National Child Development Agency (NCD), A&P Building, 3rd Floor 18KG Ave Kigali, Kigali, Rwanda, Tel +250788887249, Email [email protected]
Background: The 1994 Tutsi genocide in Rwanda significantly impacted family structure, with many people growing old alone and lacking social bonds and connections with family members. However, little is known about the contribution of the family environment to geriatric depression which was highlighted by WHO as a psychological problem with a 10% to 20% prevalence rate among the elderly worldwide. This study aims to investigate geriatric depression and associated family determinants among the elderly in Rwanda.
Methods: With a community-based cross-sectional study design, we assessed geriatric depression (GD), quality-of-life enjoyment and satisfaction (QLES), family support (FS), loneliness, neglect, and attitude toward grief in a convenience sample of 107 participants (M=72.32, SD=8.79) aged between 60 and 95 years who were recruited from three groups of elderly people supported by the NSINDAGIZA organization in Rwanda. SPSS (version 24) was used for statistical data analysis; differences across various sociodemographic variables were tested for significance by an independent t-test; the relationship between study variables was tested by Pearson correlation analysis; and multiple regression analysis was performed to model the contribution of independent variables to dependent variables.
Results: A total of 64.5% of the elderly scored above the threshold of the normal range of geriatric depression (SDS> 49), with higher symptoms in women than in men. Multiple regression analysis indicated that family support and quality-of-life enjoyment and satisfaction were contributors to geriatric depression in the participants.
Conclusion: Geriatric depression was relatively common in our participants. It is associated with the quality of life and family support received. Hence, adequate family-based interventions are needed to improve the well-being of geriatric people in their respective families.
Keywords: depression, family environment, elderly, Rwanda
Introduction
According to the United Nations, senescence or old age in humans is considered to be 60 or 65 years of age or older.1 The elderly population has grown quickly in recent decades as mortality and fertility rates have decreased and the quality of life has improved.2 The number of persons aged 60 or more was one billion in 2019, and it is predicted to rise to 1.4 billion by 2030 and 2.1 billion by 2050, with low- and middle-income nations accounting for 80% of all older people by 2050.3,4 Senescence is a natural process characterized by the degradation of human body systems and cells, resulting in death.5 It causes significant changes in different domains of individuals, such as physiological (structural and functional losses), sociological (the decline and losses in the values that society bestows on individuals), and psychological (the deterioration of problem-solving abilities, perception, and learning).6
More than 20% of adults over 60 years old are more likely to experience mental health issues.7 Geriatric depression is one of the major mental health issues among the elderly8 and a risk factor for mortality and disability.9 Scholars have revealed that geriatric depression remains undiagnosed in about 50% of the affected population and differs greatly.10,11 It is also well known that geriatric depression is caused by a complex combination of social, psychological, and biological factors.12,13
According to WHO global estimates, elderly people ranging from 10 to 20% have significant symptoms of geriatric depression.14–16 Recent evidence from a systematic review and metanalysis study showed that the prevalence of geriatric depression among elderly people was 31.74%, with a higher rate in developing countries (40.78%) than in developed countries (17.05%).17 Contributing factors for geriatric depression in developing countries are a history of chronic disease, poor social support, older age, marital loss18 poor quality of life, low monthly income, having low educational status, a family history of mental illness, and cognitive impairments,19 but the female population is more likely to suffer than the male population.18 Despite the previous findings, the burden of geriatric depression is not properly addressed due to the insufficient data that directly affects mental health care delivery in different communities all over the world.15,20
Rationale
The 1994 Tutsi genocide in Rwanda significantly impacted family structure, with many people growing old alone. There are presently elderly people with various mental health challenges, including trauma, the stigma associated with older age, abuse, neglect, a low public profile, and a lack of basic needs.21 Although depression was revealed as a seriously disabling mental health issue in post-genocide Rwanda,22–26 social bonds and connections with family members were proven to be protective factors against geriatric depression.27–29 On the other hand, a lack of family bonds and family dysfunction were reported as potential risk factors for geriatric depression.30,31 Considering a need to investigate burden-related family attitudes and behaviours that hinder elderly people’s ability to recover from geriatric depression,32 family determinants of geriatric depression should be explored in sub-Saharan African countries like Rwanda, where the family was negatively affected by the consequences of the genocide against the Tutsi in 199433 to inform policymakers, practitioners, and future researchers.
With regard to what is known, the majority of trending studies on geriatric depression have focused on improved diagnostic tools;34–37 prevalence;38–41 comprehension of differences in demographic traits (eg, occupation status, gender, age, marital status, health status, and social support);42 and the plausible risk factors.43–45 Consistently, researchers have found that geriatric depression can be influenced by various family factors such as family support,46 quality of life enjoyment and satisfaction,47 loneliness,48 neglect,49 and grief.50 Our study intends to explore the influence of the family environment on geriatric depression symptoms in the Rwandan context.
The rated family-based factors of geriatric depression symptoms are family support, quality of life enjoyment and satisfaction, loneliness, neglect, and grief whilst personal characteristics are age, education, gender, and marital status. Therefore, we hypothesize that (i) there is a high rate of geriatric depression in the study sample; (ii) there is a significant difference in geriatric depression symptoms among participants with different personal characteristics; and (iii) there is an association between geriatric depression and family support, quality of life enjoyment and satisfaction, loneliness, neglect, and grief.
Methods
Study Design, Sample, and Procedures
This study was approved by the Institutional Review Board of the University of Rwanda, CMHS (IRB-CMHS). It adopted a quantitative approach with a community-based cross-sectional study design. A convenience sample of 107 elderly people (20 males and 87 females) was selected from three available groups of elderly people supported by NSINDAGIZA (a Rwandan organization that promotes the rights and welfare of the elderly, especially the most vulnerable older women and men in the country) in Rwanda’s Nyarugenge and Huye Districts. The total number of participants from the three groups was 218 (51 males and 167 females) aged 60 or older, but those eligible were 107. Before selecting the participants, approval was obtained from the director of NSINDAGIZA, who also supported the selection process. Inclusion criteria were to be a Rwandan with permanent residence, supported by NSINDAGIZA organization, aged 60 or older, and ready to participate voluntarily in the study. Participants were excluded from the study if they were unable to communicate, were psychologically distressed by research questionnaires, or were psychologically unstable due to chronic diseases or psychotropic medication.
Before collecting data, participants were informed of the research objectives and ethical guidelines. They, therefore, provided oral informed and accepted consent or written informed consent for their voluntary participation. A trained psychologist was ready to provide appropriate emotional support to the participants who were psychologically distressed by the questionnaires. These participants were then referred to the nearest clinic for further support. Similarly, a trained research assistant collected data from those who were unable to write. Besides, the participants were informed of their right to opt out of the study at any point and that there were no penalties or other impacts for their choice. The study questionnaires were granted for non-commercial use. To ensure the content validity of the Kinyarwanda version, those questionnaires were translated from English to Kinyarwanda and back-translated from Kinyarwanda to English by three psychologists with fluent competence in Kinyarwanda and English. The similarity between the two English versions helped to ensure the content validity of the questionnaires. Furthermore, the reliabilities of the questionnaires were assessed using Cronbach’s alpha coefficients. The alpha values were above 0.7, except the SDS, MNBS, and AAG values ranged between 0.56 and 0.69. Fortunately, these alpha values are between 0.5–0.7, indicating an acceptable level of moderate reliability for those questionnaires.51 Additionally, no missing data were detected in our dataset.
Measurements
The Self-Rating Depression Scale (SDS) consists of 20 items to screen for geriatric depression symptoms “over the past several days” on a 4-point Likert-type scale ranging from 1 (little or none of the time) to 4 (most or all of the time).52 The plausible scores range from 20 through 80, where the score classifications are as follows: normal (<50), mild depression (50 −59), moderate to marked major depression (60–69), and severe to extreme major depression (>70).52 In this study, the Cronbach’s alpha coefficient was 0.67.
The Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-QSF), with 16 items, evaluates life satisfaction over the past week.53 This self-administered questionnaire originating from the general activities scale of 93 items,54 assesses overall enjoyment and satisfaction in different life domains such as daily functioning, economic status, household and leisure activities, medications, mood, work, physical health, sexual life, social and family relationships, and overall well-being. Each item is rated on a 5-point scale from 1 (Very Poor) to 5 (Very Good). Then, scores from the individual items are added together to provide a possible score ranging between 14 and 70, where a higher score indicates better enjoyment and satisfaction with life.53 The first 14 items are summed together to give the total score for further analysis, while the final two (medications and overall life satisfaction) are given separate consideration.53 The Cronbach’s Alpha value was 0.85 in the current sample.
The University of California, Los Angeles Loneliness Scale (UCLA Loneliness Scale) was developed by Russell in 1980 to measure loneliness caused by a discrepancy between the desire for social connection and the actual level of loneliness.55 It is a one-dimensional scale consisting of 20 items, of which 11 are positive and 9 are negative. The respondent is required to rate each item on a four-Likert rating scale, with 4 for “all the time”, 3 for “sometimes”, 2 for “rarely”, and 1 for “never”.55 The overall score runs from 20 to 80, with higher levels denoting more severe symptoms of loneliness.55 The Cronbach’s Alpha coefficient was 0.81 in the current sample.
The family support scale (FSS) for elderly people comprises 20 items to assess perceived support for the following 20 areas: company, daily activities, emotional support, food, happiness, health, help in problem-solving, important decisions, important people, information, love, money, personal needs, personal problems, religious activities, respect, satisfaction, sleep, social events, and treatment.56 Each item is measured on a 4-point Likert scale from 0 (no) to 3 (much).56 The total possible scores fall between 0 and 60, where a higher score reflects greater perceived family support for the elderly.56 In the current sample, the Cronbach’s alpha was 0.94.
The Multidimensional Neglectful Behaviour Scale (MNBS) aims to assess how often four fundamental developmental needs, like physical (clothing, food, medical care, and shelter), emotional (companionship, support, and affection), supervisory (setting limits), and cognitive (explaining things) were neglected for older people when they were growing up.57 It is composed of 8 items assessed on a four-Likert rating scale, from “Strongly Disagree” (1) to “Strongly Agree” (4), where greater experienced neglect is reflected in higher scores.57 Cronbach’s alpha for the current sample was 0.56.
The Adult Attitude to Grief (AAG) scale assesses the level of vulnerability in grief.58 It comprises 9 items with five response options, ranging from 4 for strongly agree to 0 for strongly disagree.58 All items are summed to get the total score, where a score greater than 24 indicates severe vulnerability to grief, one ranging between 21 and 23 indicates higher vulnerability, and a score below 20 indicates lower vulnerability to grief.58 In the current sample, Cronbach’s alpha was 0.69.
Statistical Analysis
Data analysis was carried out in line with the study hypotheses and objectives, using IBM SPSS version 24. In the first step, descriptive statistics were performed to verify the reliability of the standardized scales, means, and standard deviations of the study variables and further determine the frequencies of sociodemographic variables and clinical symptoms of geriatric depression based on cut-off scores. In the second step, skewness and kurtosis were used to determine whether the study variables were normally distributed. However, non-normally distributed samples were identified because the kurtosis was greater than 2 for dependent variable. This means that the estimation of values for parametric tests was not possible with our data.59 Fortunately, there are estimation techniques other than normal theory, such as bootstrapping, an alluring estimation technique that requires few assumptions and deals with non-normally distributed data.60–63 Hence, a bootstrapped independent t-test, correlation, and multiple linear regressions with 5000 bootstrap samples were used to make the right decision on the use of predicting analysis for determinants of geriatric depression. It helped to calculate statistical significance using 95% confidence intervals. In this case, when the 95% confidence interval does not include 0, this indicates that there is statistically significant result.
Results
Characteristics of the Study Participants
As presented in Table 1, the study sample was composed of 107 elderly people (M=72.32, SD=8.79) aged between 60 and 95 years, predominantly more females (81.3%) than males (18.7%). Over half of the sample (67.3%) did not have any partner, while a small part of the sample (32.7%) was revealed to be in partnership. About 57.9% of the participants attended formal school, allowing them to be able to read and write. However, 42.1% of them cannot write or read because of not attending formal school.
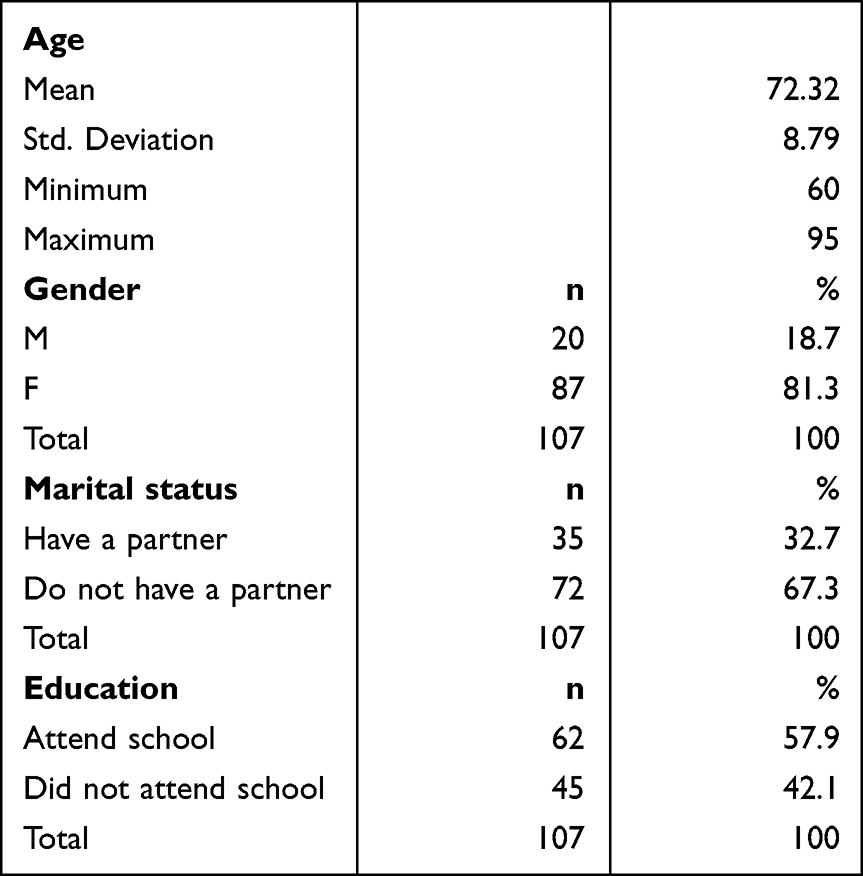 |
Table 1 Analysis of Socio-Demographic Characteristics of the Participants |
Descriptive Analysis of Study Variables
Geriatric depression (GD), family support (FS), quality of life enjoyment and satisfaction (QLESQ), loneliness, neglect, and grief underwent skewness and kurtosis screening to assess the normality of the scale’s distribution. Following an argument by George and Mallery stating that skewness and kurtosis values should range between −2 and +2,64 study findings showed that all variables were in the normal range except geriatric depression, which violated the kurtosis requirements (Table 2). Consequently, using the bootstrapping technique was a suitable solution for further analysis.60–63
 |
Table 2 Descriptive Analysis of Study Variables |
Rate of Geriatric Depression Among the Participants
Table 3 provides estimates of the prevalence of participants’ geriatric depression based on various cut-off values for the Self-Rating Depression Scale (SDS) total scores. Overall, 64.5% of the participants had significant symptoms of geriatric depression. Table 3 shows that only 35.5% of the participants were in the normal range, 52.3% had mild symptoms, and 12.2% had moderate symptoms. However, no cases of severe depression were highlighted by the analysis.
 |
Table 3 Distribution of Symptoms of Geriatric Depression Among the Participants |
However, identified geriatric symptoms are not equally distributed across different sociodemographic variables. Results from an independent t-test show that there were no statistically significant differences in geriatric depression symptoms between the participants who have partners and those who do not have partners (t (156) = 0.025, p = 0.91), or between participants who attended school and those who did not attend school (t (156) = −1.33, p = 0.19), but there were statistically significant differences in geriatric depression symptoms between females and males (t(105) =−3.05, p = 0.007), with more symptoms in the female group (M=51.5; SD=8.15) than in the male group (M=45.9; SD=7.27). Results from the independent t-test are presented in Table 4.
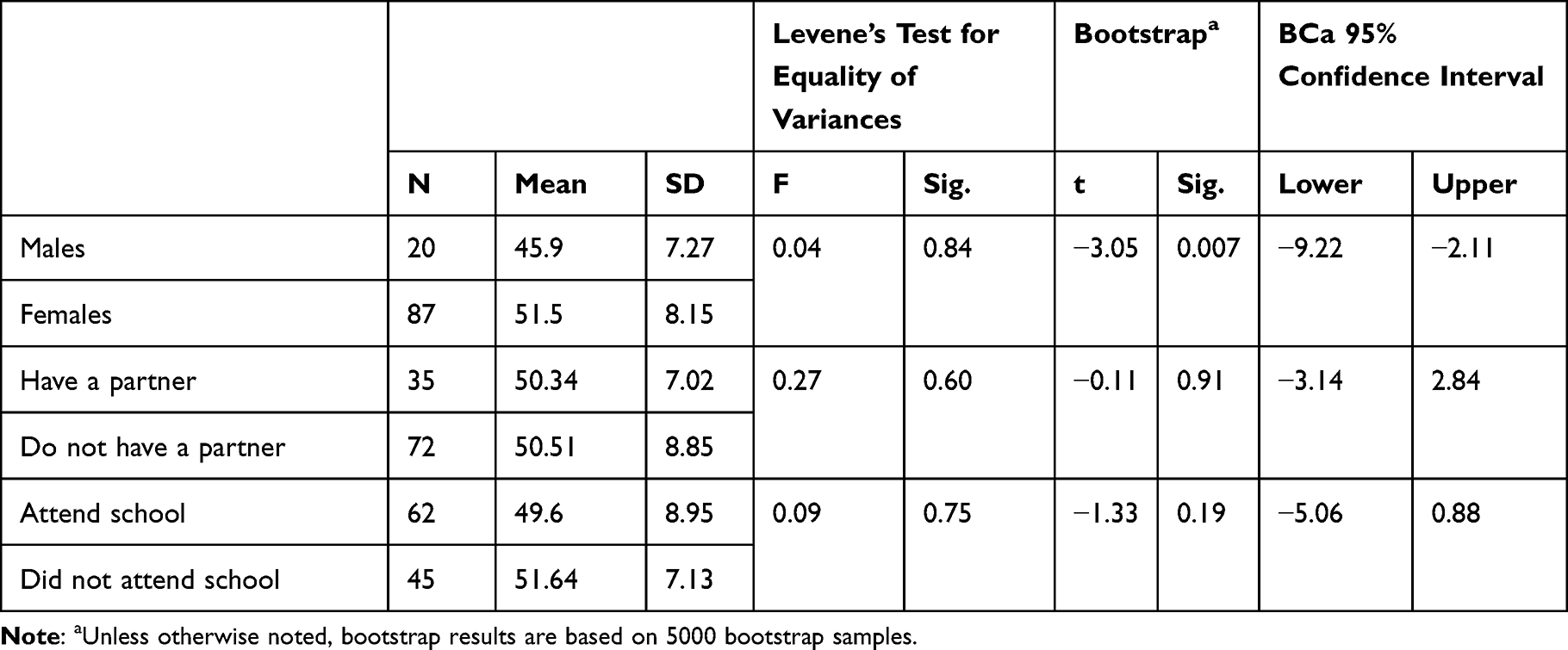 |
Table 4 Results from Independent Samples Test |
Bivariate Correlation Analyses
Results from bivariate correlation analyses are presented in Table 5. Given that some of the variables are not normally distributed, the bootstrapped confidence intervals were more concerning than the significance of Pearson correlations, because the distribution of scores cannot alter the bootstrapped confidence intervals, but it might have an impact on the significance value.65 The lower and upper boundary values are included in these confidence intervals, which are referred to as BCa 95% Confidence Intervals (CI).
 |
Table 5 Correlation Between GD, FS, QLESQ, LNSS, NGLCT, and Grief (N=107): Bootstrapc |
For our five correlation coefficients, GD is negatively correlated with FS (BCa 95% CI: −0.43, −0.10) and QLESQ (BCa 95% CI: −0.47, −0.09), but it is not correlated with loneliness (BCa 95% CI: −0.15, 0.26), neglect (BCa 95% CI: −0.10, 0.20), and grief (BCa 95% CI: −0.40, 0.16). These results support a plausible association between the dependent variable, geriatric depression (GD), and the independent variables, FS and QLESQ.
Significant Family Determinants of Geriatric Depression Among the Participants
Our dependent variable (GD), as mentioned in the descriptive analysis section, is significantly kurtotic, making bootstrapping an attractive and viable estimation technique since it does not require normally distributed data. It was shown in Table 6 that both independent variables, namely FS (b = −0.10, p < 0.05, BCa95% CI: −0.186 and −0.020) and QLESQ (b = −0.19, p < 0.05, BCa95% CI: −0.364 and −0.022) were found to be statistically significant contributors to geriatric depression in the participants. It was also noted that the variables’ 95% lower- and upper-bound confidence intervals were negative in value, indicating a statistically significant effect. These findings revealed that a lower level of FS and QLESQ among the participants predicted the symptoms of geriatric depression.
 |
Table 6 Results from Multiple Regressions Analysis: Bootstrapa |
Discussion
The results of this study showed that 64.5% of the participants are identified as meeting the criteria for geriatric depression. This rate is higher than the one recently observed in developing countries (40.78%) and developed countries (17.05%).17 This difference can be explained by the fact that low-income countries are immoderately affected by mental disorders,66 with depression as a major cause of disease burden, especially in older people.67
Additionally, results indicate that female participants are more vulnerable to geriatric depression than men. This finding is consistent with previous cross-sectional studies.68,69 Consistently, theories hold that women are more likely than men to develop more symptoms of depression due to the effect of the menstrual cycle and time surrounding menopause,70 the socialization effect that requires girls to be more caring while boys are required to be more independent,71,72 society’s undervaluation of women’s roles and responsibilities,73 the use of ruminative coping style which leads to the development of depressive symptoms,74 and stressful life events encountered by more women than men.7,75 In addition, women are more likely than males to develop internalizing disorders (such as depression and anxiety), but men are more likely to exhibit externalizing problems (ie, violence, substance abuse).76–79
Further, geriatric depression was negatively associated with family support. This means that a decrease in perceived social support may be linked to an increase in geriatric depression. A recent integrative literature review conducted by Vilas showed that the lack of family support is associated with geriatric depression in elderly people.80 Similarly, numerous studies have demonstrated that geriatric depression symptoms decrease significantly with increased support from spouses, children, or other potential family members.46,81,82 Finally, a significant negative association was also observed between geriatric depression and quality of life enjoyment and satisfaction. That is, a lack of enjoyment and satisfaction in one’s life leads to geriatric depression in the elderly. Consistently, geriatric depression and low quality of life enjoyment were recently observed in a sample of elderly people.83 Other scholars found that a lower level of quality-of-life enjoyment among elderly people was significantly associated with a higher level of geriatric depression symptoms.83–86
Strength and Study Implications
The primary strength of the study is that it was conducted in a country where there are few studies, especially on the psychosocial well-being of the elderly. In addition, the study showed a high prevalence of symptoms of geriatric depression in the study sample, with females more vulnerable than males. This study revealed that lower levels of family support and quality of life enjoyment and satisfaction were associated with increased symptoms of geriatric depression. The results imply that family support and quality of life should be improved to prevent geriatric depression in the elderly by focusing specifically on women. Another implication of the findings is that, in close collaboration with policymakers and decision-makers, family members should be encouraged and supported to plan and implement family-based interventions targeting improving the well-being of elderly people in their respective families. The reason for this is that observed geriatric depression can be mitigated or caused by quality of life and family support.
Limitations
The first limitation is that our study explored family determinants. The contribution of community factors and co-morbidity should also be investigated in this sample for advanced support. The second limitation is methodological because a cross-sectional study design was adopted. With this design, data concerning the rate, comprehension of differences in demographic traits, and family determinants were highlighted, but the direct cause-effect relationship was not assessed. Therefore, a similar study with a longitudinal study design is needed to test the cause-and-effect relationship. The third limitation, the self-Rating Depression Scale (SDS) is commonly used for adult people and not exclusively for geriatric. Finally, family determinants such as intimate partner violence and perceived poverty that might be plausible determinants should also be assessed.
Conclusion
Geriatric depression was relatively common in our participants. It can be mitigated or generated by the quality of life and family support received. Hence, adequate family-based interventions are needed to improve the well-being of geriatric people in their respective families.
Data Sharing Statement
Based on a reasonable request, the corresponding author can provide the data that supports the study’s conclusions.
Ethics and Consent
The ethical consent was approved by the Institutional Review Board of the University of Rwanda, CMHS (IRB-CMHS). We confirm that participants provided written informed consent for their voluntary participation. The principles set forth in the Helsinki Declaration were also observed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scherbov S, Sanderson W. Measures of population ageing. World Popul Ageing. 2019;2020:13–24.
2. Bujang MA, Muneer A, Hamid A, et al. Mortality rates by specific age group and gender in Malaysia: trend of 16 years. J Heal Informatics Dev Ctries. 2012;6(2):521–529.
3. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11. doi:10.1016/j.maturitas.2020.05.018
4. World Health Organization. Multisectoral action for a life course approach to healthy ageing: draft global strategy and plan of action on ageing and health. Sixty-ninth World Health Assembly; 2016:1–37. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_17-en.pdf.
5. Özel F, Yildirim Y, Fadiloǧ Ç. Huzurevinde yaşayan yaşlilarda aǧri yönetimi [Pain management in the elderly living in nursing homes]. Agri. 2014;26(2):57–64. doi:10.5505/agri.2014.41103
6. Samanci Tekin Ç, Kara F. Dunyada VeTurkiye De Yaslilik. J Int Sci Res. 2018;3(1):219–229.
7. Hamilton JL, Stange JP, Abramson LY, Alloy LB. Stress and the development of cognitive vulnerabilities to depression explain sex differences in depressive symptoms during adolescence. Clin Psychol Sci. 2015;3(5):702–714. doi:10.1177/2167702614545479
8. Moss K, Scogin F, Di Napoli E, Presnell A. A self-help behavioral activation treatment for geriatric depressive symptoms. Aging Ment Heal. 2012;16(5):625–635. doi:10.1080/13607863.2011.651435
9. Blazer D, Hybels C, Pieper C. The association of depression and mortality in elderly persons. J Gerontol a Biol Sci Med Sci. 2001;56(8):M505–9. doi:10.1093/gerona/56.8.M505
10. Demyttenaere K, Bruffaerts R, Posada-Villa J, et al. For treatment of mental disorders in the world health organization. JAMA. 2004;291(21):2581–2590.
11. Coyle JT, Pine DS, Charney DS, et al. Depression and bipolar support alliance consensus statement on the unmet needs in diagnosis and treatment of mood disorders in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2003;42:1494–1503. doi:10.1097/00004583-200312000-00017
12. Suwanmanee S, Nanthamongkolchai S, Munsawaengsub C, Taechaboonsermsak P. Factors Influencing the Mental Health of the Elderly in Songkhla, Thailand. Thailand J Med Assoc Thai. 2012;95(6):S8–15.
13. Sidik SM, Rampal L, Afifi M. Physical and mental health problems of the elderly in a rural community of Sepang, Selangor. Malaysian J Med Sci. 2004;11(1):52–59.
14. World Health Organization. The mental health of older adults: fact Sheet. World Health Organization Media Centre; 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults.
15. Steel Z, Marnane C, Iranpour C, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol. 2014;43(2):476–493. doi:10.1093/ije/dyu038
16. Mitchell AJ, Subramaniam H. Reviews and overviews prognosis of depression in old age compared to middle age: a systematic review of comparative studies. Psychiatry Interpers Biol Process. 2005;2005:1588–1601.
17. Zenebe Y, Akele B, W/Selassie M, Necho M. Prevalence and determinants of depression among old age: a systematic review and meta-analysis. Ann Gen Psychiatry. 2021;20(1):1–19. doi:10.1186/s12991-021-00375-x
18. Mulat N, Gutema H, Wassie GT, Allen K-A. Prevalence of depression and associated factors among elderly people in Womberma District, north-west, Ethiopia. BMC Psychiatry. 2021;21:1–9. doi:10.1186/s12888-020-02964-8
19. Anbesaw T, Fekadu B. Depression and associated factors among older adults in Bahir Dar city administration, Northwest Ethiopia, 2020: cross-sectional study. PLoS One. 2022;17:1–14. doi:10.1371/journal.pone.0273345
20. Bitew T. Prevalence and risk factors of depression in Ethiopia: a review. Ethiop J Health Sci. 2014;24(2):161–169. doi:10.4314/ejhs.v24i2.9
21. Davis F, Emmanuel Murangira MD. Ageing In Rwanda: challenges and opportunities for church, state and nation. International NGO; 2020. Available from: https://reliefweb.int/sites/reliefweb.int/files/resources/Ageingin.Rwanda.finalversion_original.pdf.
22. Sebera F, Dedeken P, Garrez I, et al. Association of depression and epilepsy in Rwanda: a prospective longitudinal study. Epilepsy Behav. 2023;138:108993. doi:10.1016/j.yebeh.2022.108993
23. Kayiteshonga Y, Sezibera V, Mugabo L, Iyamuremye JD. Prevalence of mental disorders, associated co-morbidities, health care knowledge and service utilization in Rwanda – towards a blueprint for promoting mental health care services in low- and middle-income countries? BMC Public Health. 2022;22(1):1–13. doi:10.1186/s12889-022-14165-x
24. Mutuyimana C, Cassady C, Sezibera V, Nsabimana E. Prevalence and correlates of depression among rural and urban Rwandan mothers and their daughters 26 years after the 1994 genocide against the Tutsi. Eur J Psychotraumatol. 2021;12(1). doi:10.1080/20008198.2021.2005345
25. Mukangabire P, Moreland P, Kanazayire C, et al. Prevalence and Factors Related to Depression among Adolescents Living with HIV/AIDS, in Gasabo District, Rwanda. Rwanda J Med Heal Sci. 2021;4(1):37–52. doi:10.4314/rjmhs.v4i1.4
26. Bolton P, Neugebauer R, Ndogoni L. Prevalence of depression in rural Rwanda based on symptom and functional criteria. J Nerv Ment Dis. 2002;190(9):631–637. doi:10.1097/00005053-200209000-00009
27. Thipprakmas R. Social protective factors in depression among the elderly: the role of family, social and community supports. J Heal Cent. 2021;15(37):339–351.
28. Lyberg A, Holm AL, Lassenius E, Berggren I, Severinsson E. Older persons’ experiences of depressive ill-health and family support. Nurs Res Pract. 2013;2013:1–8. doi:10.1155/2013/837529
29. Taqui AM, Itrat A, Qidwai W, Qadri Z. Depression in the elderly: does family system play a role? A cross-sectional study. BMC Psychiatry. 2007;7:1–12. doi:10.1186/1471-244X-7-57
30. Quashie NT, Andrade FCD. Family status and later-life depression among older adults in urban Latin America and the Caribbean. Ageing Soc. 2020;40(2):233–261. doi:10.1017/S0144686X18000879
31. Li L, Reinhardt JD, Pennycott A, Li Y, Chen Q. Prevalence of and risk factors for depression among older persons 6 months after the Lushan earthquake in china: a cross-sectional survey. Front Psychiatry. 2020;11:1–11. doi:10.3389/fpsyt.2020.00001
32. Martire LM, Schulz R, Reynolds CF, Morse JQ, Butters MA, Hinrichsen GA. Impact of close family members on older adults’ early response to depression treatment. Psychol Aging. 2008;23(2):447–452. doi:10.1037/0882-7974.23.2.447
33. Berckmoes LH, Eichelsheim V, Rutayisire T, Richters A, Hola B. How legacies of genocide are transmitted in the family environment: a qualitative study of two generations in Rwanda. Societies. 2017;7(3):1–18. doi:10.3390/soc7030024
34. Krishnamoorthy Y, Rajaa S, Rehman T. Diagnostic accuracy of various forms of geriatric depression scale for screening of depression among older adults: systematic review and meta-analysis. Arch Gerontol Geriatr. 2020;87:104002. doi:10.1016/j.archger.2019.104002
35. Dias FL, Teixeira AL, Guimarães HC, et al. Accuracy of the 15-item geriatric depression scale (GDS-15) in a community-dwelling oldest-old sample: the pietà study. Trends Psychiatry Psychother. 2017;39(4):276–279. doi:10.1590/2237-6089-2017-0046
36. Sun XY, Li YX, Yu CQ, Li LM. 中文版抑郁量表信效度研究的系统综述 [Reliability and validity of depression scales of Chinese version: a systematic review]. Zhonghua liu Xing Bing xue za zhi. 2017;38(1):110–116. Chinese. doi:10.3760/cma.j.issn.0254-6450.2017.01.021
37. Pocklington C, Gilbody S, Manea L, McMillan D. The diagnostic accuracy of brief versions of the geriatric depression scale: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2016;31(8):837–857. doi:10.1002/gps.4407
38. Pilania M, Yadav V, Bairwa M, et al. Prevalence of depression among the elderly (60 years and above) population in India, 1997–2016: a systematic review and meta-analysis. BMC Public Health. 2019;19(1):1–18. doi:10.1186/s12889-019-7136-z
39. Manandhar K, Risal A, Shrestha O, et al. Prevalence of geriatric depression in the Kavre district, Nepal: findings from a cross sectional community survey. BMC Psychiatry. 2019;19(1):1–9. doi:10.1186/s12888-019-2258-5
40. Ismail Z, Elbayoumi H, Fischer CE, et al. Prevalence of depression in patients with mild cognitive impairment: a systematic review and meta-analysis. JAMA Psychiatry. 2017;74(1):58–67. doi:10.1001/jamapsychiatry.2016.3162
41. Padayachey U, Ramlall S, Chipps J. Depression in older adults: prevalence and risk factors in a primary health care sample. South African Fam Pract. 2017;59(2):61–66. doi:10.1080/20786190.2016.1272250
42. Amha H, Fente W, Sintayehu M, Tesfaye B, Yitayih M. Depression and associated factors among old age population in Dega damot district, North West Ethiopia. A cross-sectional study. J Affect Disord Reports. 2020;2:100034. doi:10.1016/j.jadr.2020.100034
43. Disu TR, Anne NJ, Griffiths MD, Mamun MA. Risk factors of geriatric depression among elderly Bangladeshi people: a pilot interview study. Asian J Psychiatr. 2019;44:163–169. doi:10.1016/j.ajp.2019.07.050
44. Zhao D, Hu C, Chen J, et al. Risk factors of geriatric depression in rural China based on a generalized estimating equation. Int Psychogeriatrics. 2018;30(10):1489–1497. doi:10.1017/S1041610218000030
45. Pramesona BA, Taneepanichskul S. Prevalence and risk factors of depression among Indonesian elderly: a nursing home-based cross-sectional study. Neurol Psychiatry Brain Res. 2018;30:22–27. doi:10.1016/j.npbr.2018.04.004
46. Hung M, Bounsanga J, Voss MW, Crum AB, Chen W, Birmingham WC. The relationship between family support; pain and depression in elderly with arthritis. Psychol Heal Med. 2017;22(1):75–86. doi:10.1080/13548506.2016.1211293
47. Hussenoeder FS, Jentzsch D, Matschinger H, et al. Depression and quality of life in old age: a closer look. Eur J Ageing. 2021;18(1):75–83. doi:10.1007/s10433-020-00573-8
48. Lim YM, Baek J, Lee S, Kim JS. Association between loneliness and depression among community-dwelling older women living alone in south korea: the mediating effects of subjective physical health, resilience, and social support. Int J Environ Res Public Health. 2022;19:15. doi:10.3390/ijerph19159246
49. Dahal M, Dhakal S, Khanal S, Baral K, Mahaseth S. Linkage of depression with elder abuse among institutionalized older persons in Kathmandu Valley, Nepal. Psychiatry J. 2021;2021:1–8. doi:10.1155/2021/5546623
50. Reiland H, Banerjee A, Claesges SA, et al. The influence of depression on the relationship between loneliness and grief trajectories in bereaved older adults. Psychiatry Res Commun. 2021;1(1):100006. doi:10.1016/j.psycom.2021.100006
51. Hinton P, Brownlow C, Mcmurray I, Cozens B. Spss Explained. Oxfordshire, UK: Routledge; 2004.
52. Zung WWK. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
53. Bourion-Bédès S, Schwan R, Laprevote V, Bédès A, Bonnet JL, Baumann C. Differential item functioning (DIF) of SF-12 and Q-LES-Q-SF items among French substance users. Health Qual Life Outcomes. 2015;13(1):1–8. doi:10.1186/s12955-015-0365-7
54. Endicott J, Nee J, Harrison W, Blumenthal R. Quality of life enjoyment and satisfaction questionnaire: a new measure. Psychopharmacol Bull. 1993;29(2):321–326.
55. Russell D, Peplau L, Cutrona CE. Revised UCLA loneliness scale. J Pers Soc Psychol. 1980;39:427–480. doi:10.1037/0022-3514.39.3.472
56. Uddin MA, Bhuiyan AJ. Development of the family support scale (FSS) for elderly people. MOJ Gerontol Geriatr. 2019;4(1):17–20. doi:10.15406/mojgg.2019.04.00170
57. Straus MA, Kinard EM, Williams LM. The multidimentional neglectful behavior scale, form A. Fam Res Lab Univ New Hampsh Durham, NH; 2008. Available from: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.537.4848&rep=rep1&type=pdf.
58. Sim J, Machin L, Bartlam B. Identifying vulnerability in grief: psychometric properties of the adult attitude to grief scale. Qual Life Res. 2014;23(4):1211–1220. doi:10.1007/s11136-013-0551-1
59. Kim TK. T test as a parametric statistic. Korean J Anesthesiol. 2015;68(6):540–546. doi:10.4097/kjae.2015.68.6.540
60. Johnston MG, Faulkner C. A bootstrap approach is a superior statistical method for the comparison of non-normal data with differing variances. New Phytol. 2021;230:23–26. doi:10.1111/nph.17159
61. Hosseini S, Latifi S, Kelishadi R. Analysis of factors affecting the body mass index in a national sample of Iranian children and adolescents: bootstrapping regression. Adv Biomed Res. 2017;6(1):152. doi:10.4103/2277-9175.219417
62. Desharnais B, Camirand-Lemyre F, Mireault P, Skinner CD. Determination of confidence intervals in non-normal data: application of the bootstrap to cocaine concentration in femoral blood. J Anal Toxicol. 2015;39(2):113–117. doi:10.1093/jat/bku127
63. Šaltyte Benth J, Dahl FA, Mitic S. Can linear regression model give reliable conclusions about the postoperative recovery? Bootstrap for case study in Mitic et al. Clin Otolaryngol. 2008;33(3):287–289. doi:10.1111/j.1749-4486.2008.01661.x
64. George D, Mallery P. IBM SPSS Statistics 23 Step by Step: A Simple Guide and Reference. New York, NY: Routledge; 2016.
65. Field A. Discovering Statistics Using SPSS: And Sex, and Drugs, and Rock ‘N’ Roll. London: Sage; 2013.
66. World Health Organization. The Global Burden of Disease 2004. Updat World Heal Organ; 2004:146.
67. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):2011–2030. doi:10.1371/journal.pmed.0030442
68. Bhavna S, Kiran B, Tejinder K, Akash N. Prevalence and determinants of geriatric depression in North India: a cross-sectional study. J Fam Med Prim Care. 2020;6(2):169–170.
69. Zou C, Chen S, Shen J, et al. Prevalence and associated factors of depressive symptoms among elderly inpatients of a Chinese tertiary hospital. Clin Interv Aging. 2018;13:1755–1762. doi:10.2147/CIA.S170346
70. Wharton W, Gleason CE, Olson SR, Carlsson CM, Asthana S. Neurobiological underpinnings of the estrogen-mood relationship. Curr Psychiatry Rev. 2012;8(3):247–256. doi:10.2174/157340012800792957
71. Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320–330. doi:10.1016/j.yfrne.2014.05.004
72. Wide J, Mok H, McKenna M, Ogrodniczuk JS. Effect of gender socialization on the presentation of depression among men: a pilot study. Can Fam Physician. 2011;57(2):e74–8.
73. Mayor E. Gender roles and traits in stress and health. Front Psychol. 2015;6:1–7. doi:10.3389/fpsyg.2015.00779
74. Johnson DP, Whisman MA. Gender differences in rumination: a meta-analysis. Pers Individ Dif. 2013;55(4):367–374. doi:10.1016/j.paid.2013.03.019
75. Cohen S, Murphy MLM, Prather A. Ten surprising facts about stressful life events and disease risk. Annu Rev Psychol. 2019;70(1):577–597. doi:10.1146/annurev-psych-010418-102857
76. Smith DT, Mouzon DM, Elliott M. Reviewing the assumptions about men’s mental health: an exploration of the gender binary. Am J Mens Health. 2018;12(1):78–89. doi:10.1177/1557988316630953
77. Kessler RC, Wang PS. The descriptive epidemiology of commonly occurring mental disorders in the United States. Annu Rev Public Health. 2008;29(1):115–129. doi:10.1146/annurev.publhealth.29.020907.090847
78. Jackson DA, King AR. Gender differences in the effects of oppositional behavior on teacher ratings of ADHD symptoms. J Abnorm Child Psychol. 2004;32(2):215–224. doi:10.1023/B:JACP.0000019772.71251.ff
79. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the national comorbidity survey replication-adolescent supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–989. doi:10.1016/j.jaac.2010.05.017
80. Vilas B, Dias B, Rodrigues L, et al. The lack of family support to the institutionalized elderly: an integrative literature review. MOJ Gerontol Ger. 2019;4(6):250–253.
81. Lee J, Kim T, Lee B. The effects of family support and activities of daily living on depression for elderly patients in nursing homes. Indian J Public Heal Res Dev. 2018;9:3.
82. Wang J, Zhao X. Family functioning and social support for older patients with depression in an urban area of Shanghai, China. Arch Gerontol Geriatr. 2012;55(3):574–579. doi:10.1016/j.archger.2012.06.011
83. Jemal K, Hailu D, Tesfa B, Lama T, Kinati T, Mengistu E. Geriatric depression and quality of life in North Shoa Zone, Oromia region: a community cross-sectional study. Ann Gen Psychiatry. 2021;20(1):1–10. doi:10.1186/s12991-021-00357-z
84. Juniarni L, Wulandari SS. The relationship between depression and the quality of life among elderly in nursing home. Int J Caring Sci. 2020;13(3):2048–2053.
85. Cao W, Guo C, Ping W, Tan Z, Guo Y, Zheng J. A community-based study of quality of life and depression among older adults. Int J Environ Res Public Health. 2016;13:7. doi:10.3390/ijerph13070693
86. Akyol Y, Durmuş D, Doǧan C, Bek Y, Cantürk F. Geriatrik populasyonda yaşam kalitesi ve depresif belirti düzeyi. Turkish J Rheumatol. 2010;25(4):165–173. doi:10.5152/tjr.2010.23
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Screening of Depression Among Medical Outpatients Visiting the University Teaching Hospital of Kigali, Rwanda
Gafaranga JP, Bitunguhari L, Mudenge C, Manirakiza F, Kelly B, Gatabazi P
Neuropsychiatric Disease and Treatment 2024, 20:845-854
Published Date: 8 April 2024
Family Functioning, Anxiety and Depression in Chinese Higher Vocational School Students: A Network Analysis
Ye L, Chen S, Chen QW, Luo X
Psychology Research and Behavior Management 2024, 17:4399-4412
Published Date: 25 December 2024