")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Prevalence and Determinants of Pre-Cancerous Cervical Lesion and Human Papillomavirus Among HIV-Infected and HIV-Uninfected Women in North-West Ethiopia: A Comparative Retrospective Cross-Sectional Study
Authors Kiros M , Mesfin Belay D , Getu S , Hailemichael W , Esmael A , Andualem H , Geteneh A
Received 14 March 2021
Accepted for publication 28 May 2021
Published 29 June 2021 Volume 2021:13 Pages 719—725
DOI https://doi.org/10.2147/HIV.S310905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Mulugeta Kiros,1 Demeke Mesfin Belay,2 Sisay Getu,1 Wasihun Hailemichael,1 Ahmed Esmael,3 Henok Andualem,1 Alene Geteneh4
1Department of Medical Laboratory Sciences, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Nursing, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Medical Laboratory Sciences, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 4Department of Medical Laboratory Sciences, College of Health Sciences, Woldia University, Woldia, Ethiopia
Correspondence: Mulugeta Kiros Email [email protected]
Background: The poor socio-economic status, underdeveloped health care system, and the high HIV/AIDS burden have potentially increased the incidence of cervical cancer in sub-Saharan Africa (SSA) including Ethiopia. Studies on the magnitude of pre-cancerous cervical lesion and human papillomavirus (HPV) among HIV-infected women are still limited, particularly in the current study setting. Thus, we determined the prevalence of pre-cancerous cervical lesion and HPV among HIV-infected women in comparison with HIV-uninfected women at Debre Tabor Comprehensive Specialized Hospital (DTCSH), North-West Ethiopia.
Methods: Hospital-based comparative retrospective cross-sectional study was conducted among 546 women from July 2018 to January 2020 at DTCSH. All records during the study period were collected using a structured checklist. Epi data version 4.02 and SPSS version 25.0 were used for data entry and analysis, respectively.
Results: The overall prevalence of pre-cancerous cervical lesion among 546 women was 8.8%. The prevalence of pre-cancerous cervical lesion was comparable between HIV-infected (9.3%) and HIV-uninfected women (8.6%) (p = 0.859). Age > 45 years old, widowed marital status, multiparous (women ≥ 5 childbirths), and educational status were independent contributing factors of a pre-cancerous cervical lesion. Regarding HPV prevalence, among 109 screened women, 7 (6.4%) were positive for both HPV 16 and 18 strains.
Conclusion: HIV infection was not statistically correlated with the magnitude of pre-cancerous cervical lesion (p = 0.859). Women in the study setting developed pre-cancerous cervical lesions irrespective of their HIV status. Hence, we recommend routine screening of women for pre-cancerous cervical lesion and HPV infection regardless of their HIV status for early management and prevention of associated morbidity and/or mortality.
Keywords: pre-cancerous cervical lesion, VIA, OncoE6 test, HPV, HIV status, Ethiopia
Introduction
Cervical cancer (CC) is the fourth most common cancer among women following breast cancer, colorectal cancer, and lung cancer in the globe.1 Similarly, recent reports have indicated that CC is the leading cause of cancer-related death in low and middle-income countries.1,2 The incidence of the disease in this region, particularly, in sub-Saharan Africa (SSA) is increasing over time. The poor socio-economic status, less accessible and underdeveloped health care system, and the high HIV/AIDS burden in sub-Saharan Africa (SSA) have been potentially increased the incidence of CC in the region.3 Due to this increment of CC incidence, women in this region are more affected with greater morbidity and mortality rates relative to other regions of the world.4
According to World Health Organization (WHO) estimation, CC is expected to kill over 443,000 women by 2030, and the majority (more than 98% of deaths) are believed to occur in developing countries (mainly in SSA).3 These alarming estimations would pose a challenge in achieving the sustainable development goals and is a call for developing preventive action like routine screening and consecutive treatment of cases to diminish the upcoming effect. The current recommended CC screening method in resource-limited settings like SSA is a visual inspection of the cervix using acetic acid (VIA).5 Besides, using rapid, easy to use, and low-cost molecular tests; such as the OncoE6 test that directly detects the elevated levels of the E6 oncoprotein of Human Papilloma Virus (HPV) types 16 and 18 can be used as a preferred screening test than previous screening method.6
According to the previous reports, CC is the second-top deadly cancer among Ethiopian women.7,8 In 2016 alone, an estimated 718,500 people were living with HIV, women have accounted for the 60% of all HIV infections (about 433,763 women were living with HIV).9 These number of women are at increased risk of acquiring human papillomavirus infection, pre-cancerous cervical lesion, and even having an invasive CC compared with uninfected women.10,11 Despite this concern, previous studies in Ethiopia were more focused on knowledge, attitude, and practices of CC screening while studies on the magnitude of pre-cancerous cervical lesion among the at-risk population (HIV infected) relative to the general population were seen as limited. Specifically, in the current study setting, no study was reported regarding pre-cancerous cervical lesion and HPV. Thus, this study determined the prevalence of pre-cancerous cervical lesion among HIV-infected women in comparison with HIV-uninfected women at Debre Tabor Comprehensive Specialized Hospital (DTCSH), North-West Ethiopia.
Methods
Study Design and Setting
A hospital-based comparative retrospective cross-sectional study was conducted at DTCSH from July 2018 to January 2020. DTCSH is found in Debra Tabor town, South Gondar Zone, and is 667 km from Addis Ababa (the capital city of Ethiopia) and 102 km from Bahir Dar (the capital city of Amhara regional state). It was established by the Italian missionaries in 1941 and is now offering services for more than 2.3 million people. This study has reviewed back the participant’s medical records for socio-demographics, HIV status, history of sexually transmitted infections (STI), pre-cancerous cervical lesion screening by VIA, and OncoE6 test during the study period. The OncoE6 test kit used was directed against the high-risk HPV strains 16 and 18.
Eligibility Criteria
All women who had VIA and HIV screening test results along with complete socio-demographic data during the study period were included.
Data Collection Tool and Techniques
Data were extracted from the medical records of admitted women through a structured checklist adapted from medical records, registration books, and previous works of literature. The checklist includes socio-demographics, HIV status, history of STI, pre-cancerous cervical lesion screening by VIA, and confirmation with OncoE6 from July 2018 to January 2020, 2020.
Data Quality Control
Data extraction was conducted using a pre-tested structural review checklist. Data collection was performed by two trained medical professionals under the principal investigator’s supervision. The clarity and completeness of data were checked daily by the principal investigator.
Statistical Analysis
The socio-demographic and clinical data recorded by the review checklist were checked for completeness and double entered into Epi data version 4.02 and exported to SPSS version 25.0 for analysis. Descriptive statistics such as mean and proportions were used to characterize the variables. The difference in characteristics among participants enrolled was determined using a chi-square test for categorical variables. Differences were statistically significant if p < 0.05 at 95% confidence interval (CI). Both bivariable and multivariable binary logistic regression models were used to identify the predictors of the outcomes variables.
Ethical Consideration
Waiver of consent for this study was obtained from DTCSH. Besides, the medical record identification information (name and card number) was not included in the study to maintain the confidentiality of the women, and data collected from the chart were kept strictly confidential and used only for the study purpose. This study was approved by the DTCSH research ethics committee, and the study protocol was following the Declaration of Helsinki.
Results
Socio-Demographic and Clinical Characteristics
Out of 943 screened women in the hospital during the study period, 397 women were excluded for different reasons (unknown HIV status, incomplete socio-demographic and clinical data, and women who undergo a hysterectomy). Hence a total of 546 women were included in the study. Among the 546 eligible participants, the number of HIV-negative and HIV-positive women were 417 (76.4%) and 129 (23.6%), respectively. The majority of the study participants were rural residents (60%). More than half of the study participants; 352 (64.5%), were in the age group of 30–45 years old. The mean age of the study participants was 36.96 ± 8.6 years old. Among women screened for pre-cancerous cervical lesion, around 326 (59.7%) of them had given birth at least once with a mean parity of 3.08 ± 2.3 SD (Table 1.).
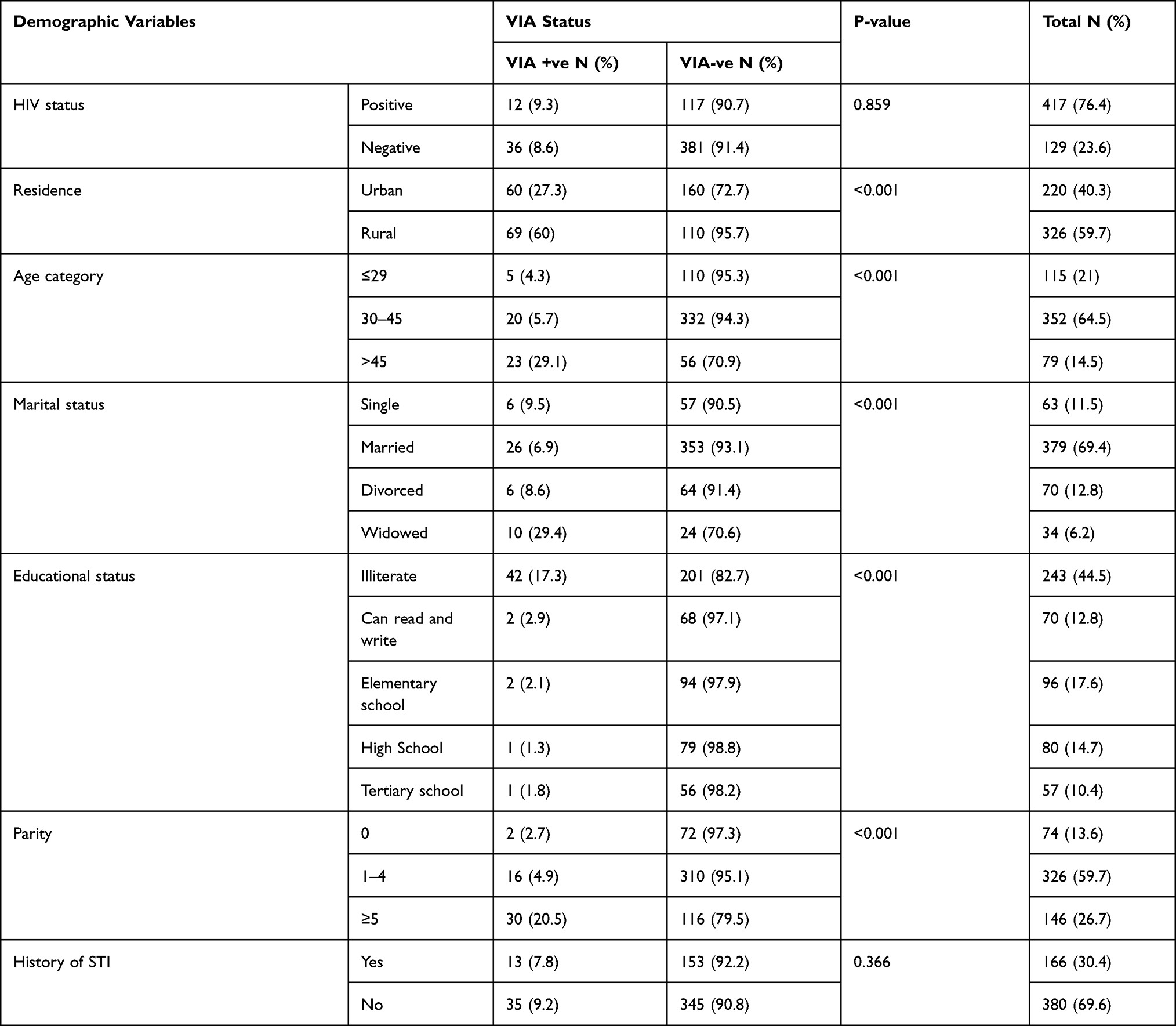 |
Table 1 Comparison of the Prevalence of Pre-Cancerous Cervical Lesion Among HIV-Infected and Non-Infected Women at DTCSH from July 2018 to January 2020, North-West Ethiopia (n=546) |
Prevalence of Pre-Cancerous Cervical Lesion
The prevalence of pre-cancerous cervical lesion among 546 women was 8.8% (95% CI; 8.74, 8.91). The proportions of pre-cancerous cervical lesion were observed to be slightly higher; 9.3% (95% CI; 9.26, 9.44) among HIV-infected women relative to HIV-uninfected 8.6% (95% CI; 8.54, 8.71), though the difference was not statistically significant (P = 0.859) (Table 1).
Determinants of Pre-Cancerous Cervical Lesion
The age-adjusted model has shown that the occurrence of pre-cancerous cervical lesion was correlated with rural residence; educational status (read and write, elementary school, high school, and tertiary school). Thus, all adjusted models indicated that maternal age greater than 45 years old, widowed marital status, educational status (read and write, elementary school and high school), and parity greater than or equal to 5 were independent contributing factors of the pre-cancerous cervical lesion. Women with age greater than 45 years old (AOR = 0.35, 95% CI: 0.16–0.80) had 65% fewer odds of having pre-cancerous cervical lesion than those women with age ≤ 29 years. Similarly, widowed women (AOR = 3.3, 95% CI: 1.1–10.1) are 3.3 times more likely to have pre-cancerous cervical lesion than married women. Moreover, women who can read and write (AOR = 0.174, 95% CI: 0.04–0.84), had elementary school (AOR = 0.18, 95% CI: 0.04–0.92) and high school (AOR = 0.13, 95% CI: 0.02–1.02) were 82.6%, 82% and 87% less likely to have pre-cancerous cervical lesion as compared to illiterate women. Furthermore, multiparous women (5 or more childbirths) were 6.3 times (AOR = 6.3, 95% CI: 1.07–36.45) more likely to have pre-cancerous cervical lesion than nulliparous women (Table 2).
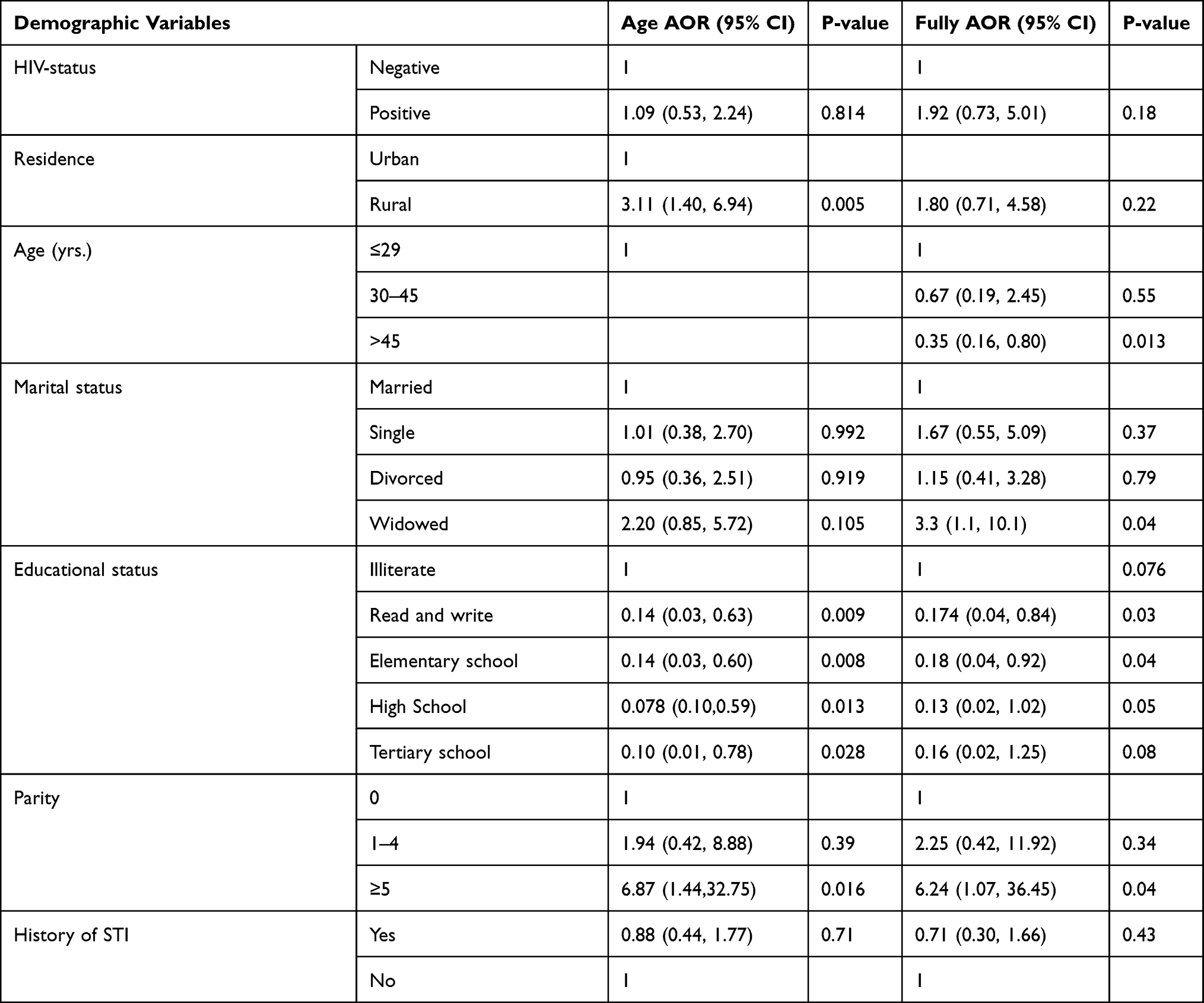 |
Table 2 Bivariate and Multivariate Analysis of Demographic and Clinical Variables with via Test Positivity Among Women Screened for a Pre-Cancerous Cervical Lesion at DTCSH from July 2018 to January 2020, North-West Ethiopia (n=546) |
Prevalence of HPV
Although 546 women were screened for pre-cancerous cervical lesion using VIA, only 109 of them were consecutively screened for HPV using the OncoE6 test due to the limited availability of the kit. Among the 109 women screened, 7 (6.4%; 95% CI = 2.6% – 12. 8%) had a positive Onco E6 test (both for HPV 16 and 18 strains). Two women positive for VIA were tested negative for the HPV Onco E6 test, and this could be due to serotypes other than HPV 16 and 18. As to the HIV status of the OncoE6 screened subjects (109), 26 of them were HIV infected. The incidence of HPV infection among HIV infected and uninfected was 7.7% (2/26) and 6% (5/83), respectively. Hence, HPV infection was found comparable regardless of HIV status in this study (p=0.67).
Discussion
In the current study, HIV-infected women had a higher proportion of pre-cancerous cervical lesion 9.3% (95% CI: 9.26–9.44) relative to HIV-negative women 8.6% (95% CI: 8.54–8.71) (p = 0.859). HIV-infected women`s adherence to highly active antiretroviral treatments might the reason for such comparable findings in the area. This is in line with a similar study from Zambia where it showed that the prevalence of pre-cancerous cervical lesion among HIV infected was higher (25.4%) than uninfected women (23.9%) despite its insignificant association (p>0.05).12 Similarly, a finding from Swaziland investigated that presence of cervical lesion among HIV infected (22.9%) was higher than HIV-negative women (5.7%) (p<0.0001).13 Besides, finding from Tanzania showed that there was a significant discrepancy in the prevalence of pre-cervical cancerous lesion among HIV-infected (71.8%) and uninfected women (27.3%)14 (P< 0.001).
In this study, the overall prevalence of pre-cancerous cervical lesion among both HIV-infected and uninfected women was found to be 8.8% (95% CI; 8.74–8.91) which is consistent with a previous study from Woldia and Dessie (9.9%), Ethiopia,15 Adwa, Ethiopia (6.7%),16 Jimma, Ethiopia (12.9%),17 Rwanda 5.9%,18 Northern Nigeria (6%),19 but higher to finding in Cameron (3.3%).20 It was also lower than study in southern Ethiopia (22.1%).21 The source of the discrepancy could be due to differences in demographics of the study participants, variation in lesion detection techniques, population immune difference, and a difference in adherence to ART. The prevalence of abnormal cervical lesions by VIA in our study is also much lower than in Kenya; where abnormal VIA among HIV infected was 55.3% very higher compared with 9.3% of our finding. This could be explained by the fact that Kenyan patients were suspected of the cervical lesion and were planned to go through conventional Pap smear, VIA, colposcopy, and biopsy22 as compared to the routine screening in the present study.
In this study, different factors were identified to associate with the pre-cancerous cervical lesion. Accordingly, women age greater than 45 years old tended to have a lower chance of developing pre-cancerous cervical lesion in this study, which is in line with another study from Rwanda that showed older women were similarly less likely to have pre-cancerous cervical lesion.18 In contrast to the current study, a study conducted in Debre Markos and Dessie reported that women aged < 30 years old had a 73% less risk of having a pre-cancerous cervical lesion compared to individuals with age > 30 years old.15 This disagreement in the findings could be due to the difference in the study participants as the compared studies included only HIV-infected women.15 Likewise, widowed women were 3.3 times (95% CI; 1.1–10.1) more likely to have pre-cancerous cervical lesion as compared to married women in our study, which is consistent with the study conducted in Rwanda (AOR= 3.29).18 This could be due to the likelihood of unmarried women having multiple sexual partners that may further increase the risk of having the lesion.23 Concurrent with previous findings in Dessie and Debre Markos,15 the finding of our study also indicated that multiparous women were more likely to have a pre-cancerous cervical lesion.
The recurrent vaginal delivery that can lead to vaginal wall laceration in these women, which in turn is favorable for HPV cross-contamination, might have led to the higher chance of pre-cancerous cervical lesion development relative to other women. On the contrary, finding from Rwanda18 showed that a higher number of children born were not associated with having a higher risk of pre-cancerous cervical lesion. Besides, educational status such as read and write, elementary school, and high school were observed to have less chance of developing pre-cancerous cervical lesion relative to being illiterate. This is in line with a similar study from Southern Ethiopia.24 It is known that education increases the knowledge about the prevention and mode of transmission of the disease, which helps to reduce the risk of acquiring the disease.
Concerning the high-risk HPV infection, 7 (7/109; 6.4%) of the screened women in the current study, were positive for both HPV 16 and 18. As being so, this was lower compared with previous studies from Ethiopia (13.7%),24 Butajira (23.2%) 25, and Gurage (15.8%)26. The relatively higher detection in those above-mentioned studies might be due to their ability to detect multiple genotypes besides HPV 16 and 18, population variation, and difference in the distribution of HPV strains. The OncoE6 test positivity was not supported by VIA positivity indicating that OncoE6 is better at detecting HPV infection early. Regarding the HIV status and HPV positivity, HIV-infected women were observed to have a higher proportion of HPV infection (2/26; 7.7%) than HIV-negative women (5/83; 6%) in this study despite an insignificant p-value. This is in line with a study from Tanzania, which reported HPV infection among HIV infected was higher (71.8%) than those uninfected ones (27.3%)14.
Strength and Limitation of the Study
As a strength, this is the first comparative cross-sectional study in the North-West region of the country. Despite being the first, the retrospective nature of the study has limited the inclusion of some variables like antiretroviral therapy (ART) duration, CD4 count, age of sexual debut, and history of multiple sexual partners, as the data were not available in the chart.
Conclusions
The overall prevalence of pre-cancerous cervical lesion and HPV infection in the current study was 8.8% and 6.4%, respectively. The prevalence of pre-cancerous cervical lesion and HPV infection was not significantly different between HIV-infected and HIV-uninfected women. Hence, women should be screened routinely for pre-cancerous cervical lesion and HPV infections regardless of women’s HIV status. Being widowed and higher parity were independent contributing factors of the pre-cancerous cervical lesion while older maternal age and advance in educational status were protective factors for a pre-cancerous cervical lesion. Therefore, emphasis should be given to women with such risk factors to minimize the burden of the disease in this population. Overall, community mobilization and education programs should be implemented to improve awareness and bring behavioral change.
Abbreviations
AOR, adjusted odds ratio; ART, antiretroviral therapy; CC, cervical cancer; CI, confidence interval; DTCSH, Debre Tabor Comprehensive Specialized Hospital; HIV, human immunodeficiency virus; HPV, human papillomavirus; STI, sexually transmitted infections; SSA, sub-Saharan Africa; WHO, World Health Organization.
Acknowledgments
We would like to thank both Debre Tabor University and DTCSH for their support. We would like also to acknowledge all DTCSH staffs who work on the ART clinic and cervical cancer screening unit for their unreserved help during the data collection of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funds for this work.
Disclosure
All authors have declared that they have no conflicts of interest for this work.
References
1. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191–e203. doi:10.1016/S2214-109X(19)30482-6
2. Ferreira MP, Coghill AE, Chaves CB, et al. Outcomes of cervical cancer among HIV-infected and HIV-uninfected women treated at the Brazilian National Institute of Cancer. AIDS. 2017;31(4):523–531. doi:10.1097/QAD.0000000000001367
3. Mboumba Bouassa R-S, Prazuck T, Lethu T, Jenabian M-A, Meye J-F, Bélec L. Cervical cancer in sub-Saharan Africa: a preventable noncommunicable disease. Expert Rev Anti Infect Ther. 2017;15(6):613–627. doi:10.1080/14787210.2017.1322902
4. Jedy-Agba E, Joko WY, Liu B, et al. Trends in cervical cancer incidence in sub-Saharan Africa. British journal of cancer. 2020;123(1):148–154. doi:10.1038/s41416-020-0831-9
5. Huchko MJ, Sneden J, Leslie HH, et al. A comparison of two visual inspection methods for cervical cancer screening among HIV-infected women in Kenya. Bull World Health Organ. 2014;92(3):195–203. doi:10.2471/BLT.13.122051
6. Krings A, Dückelmann AM, Moser L, et al. Performance of OncoE6 cervical test with collection methods enabling self-sampling. BMC Womens Health. 2018;18(1):1–7. doi:10.1186/s12905-018-0559-3
7. Begoihn M, Mathewos A, Aynalem A, et al. Cervical cancer in Ethiopia – predictors of advanced stage and prolonged time to diagnosis. Infect Agent Cancer. 2019;14(1):36. doi:10.1186/s13027-019-0255-4
8. Gemeda EY, Kare BB, Negera DG, et al. Prevalence and predictor of cervical cancer screening service uptake among women aged 25 years and above in Sidama Zone, Southern Ethiopia, Using Health Belief Model. Cancer Control. 2020;27(1):1073274820954460. doi:10.1177/1073274820954460
9. Girum T, Wasie A, Lentiro K, et al. Gender disparity in epidemiological trend of HIV/AIDS infection and treatment in Ethiopia. Arch Public Health. 2018;76(1):51. doi:10.1186/s13690-018-0299-8
10. Leece P, Kendall C, Touchie C, Pottie K, Angel JB, Jaffey J. Cervical cancer screening among HIV-positive women: retrospective cohort study from a tertiary care HIV clinic. Can Fam Physician. 2010;56(12):e425–e31.
11. Dessalegn Mekonnen B. Cervical cancer screening uptake and associated factors among HIV-positive women in Ethiopia: a systematic review and meta-analysis. Adv Prev Med. 2020;2020:7071925. doi:10.1155/2020/7071925
12. Trejo MJ, Lishimpi K, Kalima M, et al. Effects of HIV status on non-metastatic cervical cancer progression among patients in Lusaka, Zambia. Int J Gynecol Cancer. 2020;30(5):613–618. doi:10.1136/ijgc-2019-000987
13. Jolly PE, Mthethwa-Hleta S, Padilla LA, et al. Screening, prevalence, and risk factors for cervical lesions among HIV positive and HIV negative women in Swaziland. BMC Public Health. 2017;17(1):1–8. doi:10.1186/s12889-017-4120-3
14. Chambuso RS, Shadrack S, Lidenge SJ, Mwakibete N, Medeiros RM. Influence of HIV/AIDS on cervical cancer: a retrospective study from Tanzania. Journal of global oncology. 2017;3(1):72–8.
15. Belayneh T, Mitiku H, Weldegebreal F. Precancerous cervical lesion and associated factors among HIV-infected women on ART in Amhara Regional State, Ethiopia: a hospital-based cross-sectional study. Int J Health Sci. 2019;13(3):4–9.
16. Misgina KH, Belay HS, Abraha TH. Prevalence of precancerous cervical lesion and associated factors among women in North Ethiopia. J Public Health Epidemiol. 2017;9(3):46–50. doi:10.5897/JPHE2016.0891
17. Mulissa Z, Alemseged F, Assefa H. Prevalence and factors associated with precancerous cervical lesions among clients screened at family guidance association of Ethiopia, south west area office, jimma model clinic, jimma, 2013. 2014.
18. Makuza JD, Nsanzimana S, Muhimpundu MA, Pace LE, Ntaganira J, Riedel DJ. Prevalence and risk factors for cervical cancer and pre-cancerous lesions in Rwanda. Pan Afr Med J. 2015;22(1). doi:10.11604/pamj.2015.22.26.7116
19. Bakari F, Abdul MA, Ahmed SA. The prevalence and course of preinvasive cervical lesions during pregnancy in a Northern Nigerian Teaching Hospital. Ann Afr Med. 2017;16(2):74. doi:10.4103/aam.aam_35_16
20. Nkfusai NC, Mubah TM, Yankam BM, Tambe TA, Cumber SN. Prevalence of precancerous cervical lesions in women attending Mezam Polyclinic Bamenda, Cameroon. Pan Afr Med J. 2019;32.
21. Gedefaw A, Astatkie A, Tessema GA, Atashili J. The prevalence of precancerous cervical cancer lesion among HIV-infected women in southern Ethiopia: a cross-sectional study. PLoS One. 2013;8(12):e84519. doi:10.1371/journal.pone.0084519
22. Mabeya H, Khozaim K, Liu T, et al. Comparison of conventional cervical cytology versus visual inspection with acetic acid (VIA) among HIV-infected women in western Kenya. J Low Genit Tract Dis. 2012;16(2):92. doi:10.1097/LGT.0b013e3182320f0c
23. Teame H, Addissie A, Ayele W, et al. Factors associated with cervical precancerous lesions among women screened for cervical cancer in Addis Ababa, Ethiopia: a case control study. PLoS One. 2018;13(1):e0191506. doi:10.1371/journal.pone.0191506
24. Teka T, Kote M, Kejela G, Getachew T. Magnitude and factors associated with precervical cancer among screened women in Southern Ethiopia. Adv Public Health. 2019;2019:1–8. doi:10.1155/2019/5049752
25. Ali KE, Mohammed IA, Difabachew MN, Demeke DS, Haile T, Ten Hove R-J, et al. Burden and genotype distribution of high-risk Human Papillomavirus infection and cervical cytology abnormalities at selected obstetrics and gynecology clinics of Addis Ababa, Ethiopia. BMC cancer. Adv Public Health. 2019;19(1):1–9.
26. Teka B, Gizaw M, Ruddies F, Addissie A, Chanyalew Z, Skof AS, et al. Population–based human papillomavirus infection and genotype distribution among women in rural areas of South Central Ethiopia. International Journal of Cancer. 2021;148(3):723–30.
27. Leyh-Bannurah S-R, Prugger C, de Koning MN, Goette H, Lellé RJ. Cervical human papillomavirus prevalence and genotype distribution among hybrid capture 2 positive women 15 to 64 years of age in the Gurage zone, rural Ethiopia. Infectious agents and cancer. 2014;9(1):1–9.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.