Back to Journals » Orthopedic Research and Reviews » Volume 18
Prevalence and Demographic Associations of Ligamentum Flavum Hypertrophy in Lumbar Spinal Stenosis
Authors Tawhid MH ![]() , Durrani NA
, Durrani NA ![]() , Rahimi HM, Khabir A, Pirzad AF, Khurassani MH, Niazi AUR
, Rahimi HM, Khabir A, Pirzad AF, Khurassani MH, Niazi AUR
Received 18 April 2026
Accepted for publication 2 June 2026
Published 4 June 2026 Volume 2026:18 614519
DOI https://doi.org/10.2147/ORR.S614519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qian Chen
Mohammad Homayun Tawhid,1,2 Naseer Ahmad Durrani,2 Hashmatullah Mawlana Rahimi,1 Abdulkhabir Khabir,1 Ahmad Fawad Pirzad,1 Mohammad Haroon Khurassani,3 Aziz-ur-Rahman Niazi2
1Neurosurgery Department, Aliabad University Hospital, Kabul University of Medical Sciences, Kabul, Afghanistan; 2Department of Public Health, Faculty of Medicine, Afghan International Islamic University, Kabul, Afghanistan; 3Department of Ophthalmology, NOOR Eye Hospital, Kabul, Afghanistan
Correspondence: Mohammad Homayun Tawhid, Neurosurgery Department, Aliabad University Hospital, Kabul University of Medical Sciences, Kabul, 1006, Afghanistan, Tel +93700208688, Email [email protected]; [email protected]
Background: The ligamentum flavum (LF) is a posterolateral ligament of the spinal canal. Ligamentum flavum hypertrophy (LFH) is a principal degenerative determinant of lumbar spinal stenosis (LSS), causing reduction of canal and foraminal space and thereby promoting nerve roots compression. LFH prevalence and severity increase with advancing age, rendering it a key factor in the clinical presentation and surgical approaches.
Objective: This study aims to determine the prevalence of LFH in patients undergoing surgical decompression for LSS.
Methods: This cross-sectional study was conducted in the Department of Neurosurgery at Aliabad University Hospital and included all patients diagnosed with LSS (per surgical protocols and/or MRI reports) from January to December 2025. The association between age, gender, and LFH was also tested using a chi-square test in SPSS 26.0.
Results: Of 239 patients with LSS, 128 (53.6%) were males and 111 (46.4%) were females. LFH was present in 102 (42.7%) patients, including 64 (50.0%) males and 38 (34.2%) females; with a significant association between LFH and male sex (p = 0.014). LFH prevalence increases markedly with age (21– 30 years: 18.5%; 61– 70 years: 93.9%; p=0.001). Anatomically, LFH was most frequent at L4–L5 (40.2%) and L3–L4 (18.6%).
Conclusion: LFH represents a major pathological component of LSS, with prevalence increasing progressively with age. LFH was more frequent in male patients and was most commonly localized to L3 to L5. Accordingly, standardized preoperative cautions for LFH should be considered to support the selection of the surgical approach.
Keywords: ligamentum flavum hypertrophy, low back pain, lumbar disc herniation, lumbar spine stenosis
Introduction
Lumbar spinal stenosis (LSS) is one of the most common spinal disorders in the elderly population and represents one of the leading indications for spinal surgery. Ligamentum Flavum Hypertrophy (LFH) is a major contributor to acquired LSS. The Ligamentum Flavum (LF) is an important anatomical structure that covers the posterolateral portion of the spinal canal. It tends to increase with age.1,2 Its thickness is from 3.5 to 6 mm.3 LFH, which plays a significant role in LSS and nerve roots compression, has considerable clinical importance. A thickness of 4 mm or greater is generally considered hypertrophic, and surgical intervention is often required.4,5 The pathology of LSS involves degenerative changes in the facet joints and hypertrophy of the LF. These changes are usually irreversible and frequently necessitate surgical intervention.6 Patients with LSS typically present with low back pain, lower limb weakness, and neurogenic claudication. Both LFH and Lumbar Disc Herniation (LDH) contribute to the reduction of spinal canal space and compression of the thecal sac and nerve roots. Even in the absence of disc herniation or osteophyte formation, LFH alone may lead to canal stenosis and clinical symptoms.7
The first report of LFH was published in 1881 by the German neurologist Dr. Hermann Oppenheim, who described it as a cause of myeloradiculopathy.8 Recent advances in spinal instrumentation and full-endoscopic surgical techniques have led to favorable clinical outcomes in the treatment of spinal pathologies.9 Patients who do not respond to conservative treatment require surgical intervention. Traditional surgical techniques focus on complete decompression and may be associated with complications.10
The prevalence of LFH increases over time and with advancing age; patients aged 60 years and older had higher rates of LFH. The degenerative alteration occurs as a result of aging or mechanical instability, and LFH is a key factor in acquired LSS.4,11,12 Studies in Egypt show that LFH was responsible for LSS in 24.5% of patients, and was more prevalent with increasing age, observed in 32.9% of participants. No significant differences in LFH were noted between males and females.7,13 In Japan, among patients aged over 65 years with LSS, approximately 51% had LFH.6 The Israeli data indicate that LFH is independent of gender and increases with age at all levels.1 Serbian and Egyptian data indicate that the prevalence of LSS is more frequent at the vertebral level of L4/L5, with a secondary peak at L3/L4.13,14
Accurate identification of the primary pathological driver of LSS is essential to select a targeted decompressive surgery strategy. In many surgical settings in Afghanistan, procedures are frequently performed without systematic etiologic assessment. This nonselective practice is associated with persistent symptoms, higher rates of reoperation, and more frequent postoperative complications. This study aims to determine the prevalence of LFH in patients undergoing surgical decompression for LSS, with particular attention to patients’ age, gender, and the specific lumbar vertebral level.
Materials and Methods
Study Setting
This cross-sectional study was conducted in the Department of Neurosurgery, Aliabad University Hospital, Kabul, Afghanistan, from January to December 2025.
Target Population
The target population of this study includes all patients who undergo a surgical operation for LSS at the Neurosurgery Service of Aliabad University Hospital.
Sampling
Using a census sampling method, all patients diagnosed with LSS (surgical protocols and/or MRI reports), who were admitted to the Department of Neurosurgery during the study period, and aged >20 years, were included in the study. On the other hand, patients with spinal infection, spine trauma, spinal cord tumor, or congenital deformity, as well as those with previous LSS surgery, were excluded from the study.
Data Collection
Data of LSS and LFH obtained from patients’ files (surgical protocols and/ or MRI reports). Cases were included in the study if LSS or LFH were documented on the MRI report “Accordance with the radiologist’s written report, which was based on measurements obtained from axial images” or identified during the lumbar spine surgery “Intraoperatively, midline and bilateral ligamentum flavum hypertrophy was measured using calibrated instruments”. LF thickness of 4 mm or greater was considered as LFH.3
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 26.0. Descriptive statistics summarized demographic characteristics of the study participants. Continuous variables were categorized by grouping. Categorical variables were presented as frequencies and percentages. A chi-square test was used to assess the association between age and gender, with LFH.
Ethical Considerations
This study complies with the declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board of Kabul University of Medical Sciences (Protocol ID and ethical approval number: 27, Date of review: 25.12.2024). In addition, the study supervisor has approved the proposal before submission. Informed consent was obtained from study participants before their inclusion in the study. Privacy and confidentiality of participants and their data were strictly maintained throughout the study.
Results
Of the 239 patients diagnosed with LSS based on surgical findings and/or MRI reports, 102 patients (42.7%) were found to have LFH, while 137 (57.3%) did not exhibit LFH.
Among the patients with LSS, 128 (53.6%) were male and 111 (46.4%) were female. LFH was present in 64 males (50.0%) and 38 females (34.2%). A statistically significant association between LFH and male gender was observed (p = 0.014) (Table 1).
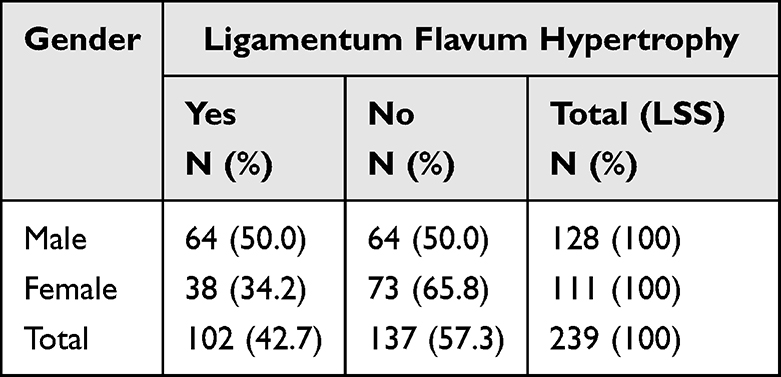 |
Table 1 Ligamentum Flavum Hypertrophy in Patients with Lumbar Spine Stenosis; Participants’ Gender |
An important finding of this study was that the proportions of both LSS and LFH increased with advancing age. In the 21–30 and 31–40-year age groups, 5 of 27 (18.5%) and 15 of 60 (25.0%) patients with LSS had LFH, respectively. By contrast, in the 51–60 and 61–70-year age groups, 33 of 48 (68.8%) and 31 of 33 (93.9%) patients with LSS exhibited LFH, respectively. A statistically significant association between LFH and increased age was observed (p = 0.001) (Table 2).
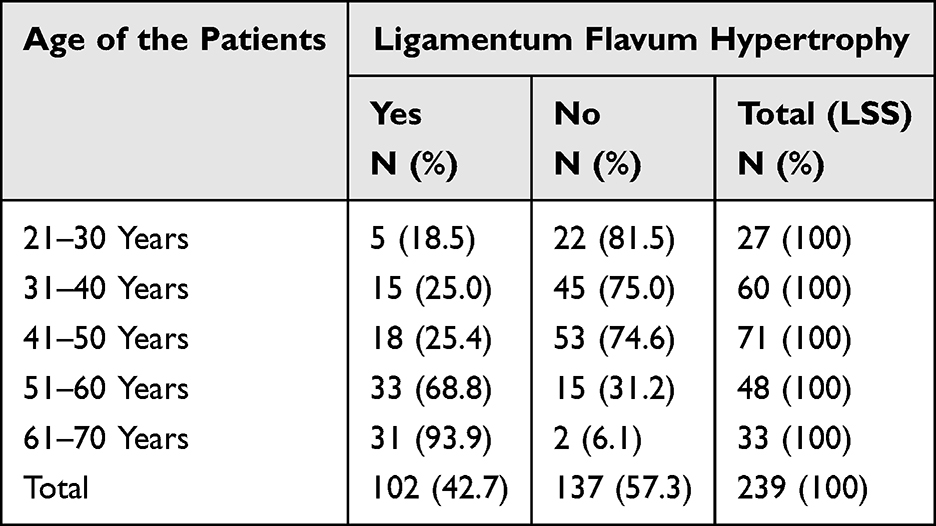 |
Table 2 Frequency and Percentage of Patients’ Age, and Its Association with LFH and LSS |
The highest incidence of LSS occurred at the L4–L5 level (87 patients; 36.4%), followed by L3–L4 (45 patients; 18.8%) and L5–S1 (37 patients; 15.5%). LFH at these same levels was observed in 41 patients (40.2%), 19 patients (18.6%), and 11 patients (10.8%), respectively (Table 3).
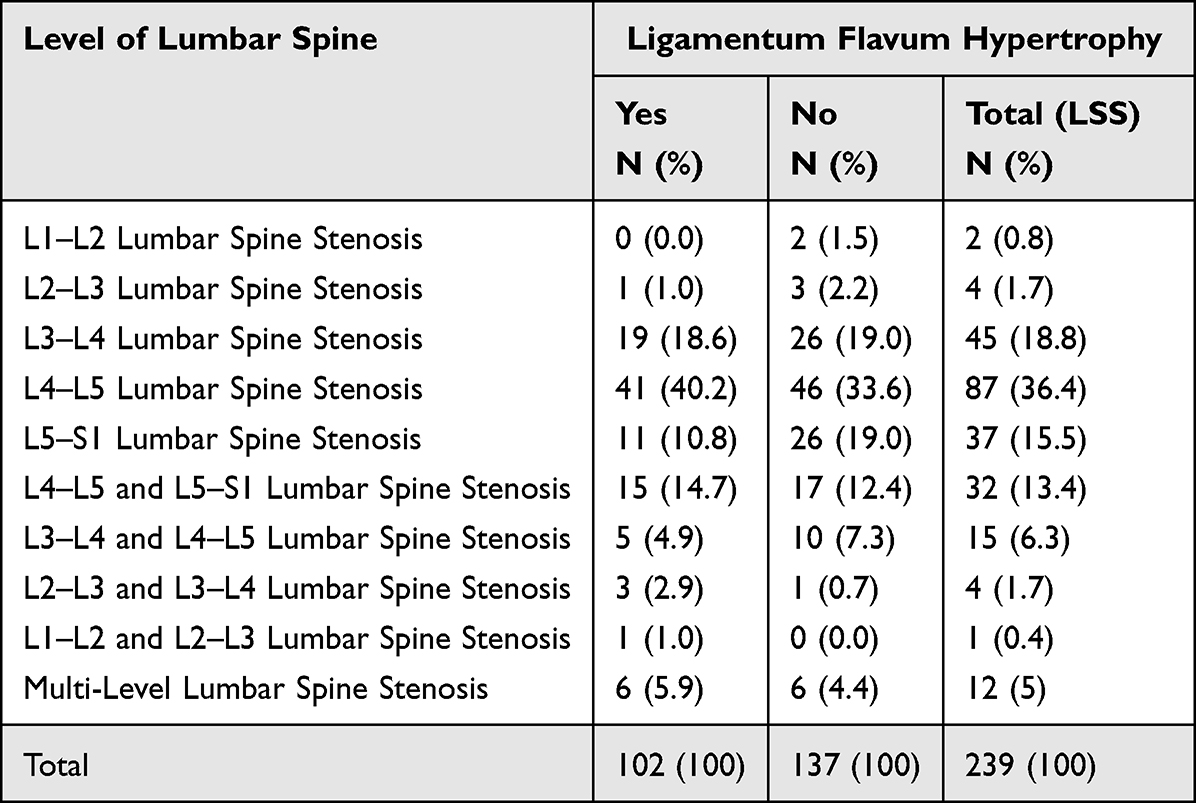 |
Table 3 Prevalence of LFH, LSS, and Their Association with the Lumbar Spine Level |
Discussion
This study aimed to determine the prevalence of LFH among patients with LSS and to assess its associations with age, sex, and lumbar spine level. This is the first investigation of its kind in Afghanistan and provides important and actionable findings for selecting surgical approaches for LSS and preventing anticipated operative complications.
Overall, 42.7% of patients with LSS in our study exhibited LFH, a proportion higher than those reported in two Egyptian studies (24.5% and 32.9%).7,13 Similarly, the prevalence of LFH among patients with LSS increases with advancing age, reaching 93.9% at age 61–70, which is comparable to the finding of a Japanese study reporting a prevalence of 51.0% at age 65,6 also this result is consistent with other studies from Israel, Saudi Arabia, Egypt (Two studies), Turkey, and Japan,1,4,7,13,15,16 and collectively indicate a global trend of increasing LFH prevalence with advancing age. The prevalence may be attributable to the more common physically demanding labor among the Afghan population and delayed presentation for medical care. International studies suggest that prolonged engagement in heavy physical labor may accelerate lumbar degeneration and contribute to LSS and LFH.17
Regarding gender distribution, 50.0% of male patients and 34.2% of female patients had LFH, showing a statistically significant association between LFH and male sex (p = 0.014); in other words, LFH was observed more frequently in males than in females. This finding differs from the Egyptian and Turkish studies, which reported no substantial gender-related difference in LFH prevalence.7,15 A plausible explanation for the higher LFH prevalence among males in our sample is the greater exposure to heavy labor and sustained outdoor physical activities.
The highest frequencies of LSS were observed at L4–L5 (36.4%), and L3–L4 (18.8%) Levels; and the highest prevalence of LFH also was observed at the same levels, L4–L5 (40.2%), and L3–L4 (18.6%). These level-specific distributions of LFH are in agreement with studies in Serbia, L4–L5 (50.0%), and L3–L4 (36.7%),14 and in Egypt, L4–L5 (70.8%).13 The Spinal level with LFH, in Turkey, was found more common at L3-L4 and L4-L5, in India at L4-L5, and in Nepal at L5-S1 and L4-L5.18–20 Overall, these findings demonstrate that LFH occurs more frequently at the lower lumbar segments (L3 to L5).
Limitations and Future Directions
This study is limited by its single-center setting and focuses on a single year (2025), which may affect the generalizability of the findings. Future multi-center studies, including correlations with functional outcomes, are recommended to validate and expand these findings.
Conclusion
The findings of this study demonstrate that LFH constitutes a substantial proportion of pathology among patients with LSS and that LFH prevalence increases progressively with advancing age. LFH was more prevalent in male patients, and the highest frequencies were observed at the L3 to L5 levels. Consequently, greater cautions for LFH should be considered to support selection of the surgical approach for LSS.
Acknowledgments
We thank our colleagues in the Department of Neurosurgery for their sincere cooperation in data collection and report writing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
Dr Aziz-ur-Rahman Niazi reports honoraria from َAfghan International Islamic University, outside the submitted work. The authors do not have any other conflicts of interest regarding the data and findings of this study.
References
1. Janan A, Kamal H, Youssef M, Hila M, Ori H. Ligamentum flavum thickness in normal and stenotic lumbar spines. J Spine. 2010;35(12):1225–6. doi:10.1097/BRS.0b013e3181bfca15
2. Kolte VS, Khambatta S, Ambiye MV. Thickness of the ligamentum flavum: correlation with age and its asymmetry: an magnetic resonance imaging study. Asian Spine J. 2015;9(2):245–253. doi:10.4184/asj.2015.9.2.245
3. Eiman MAM. An Anatomical Study of human lumbar ligamentum flavum. J Neurosci. 2008;13(1):11–16.
4. Albishi W, Alhuqbani MN, Aldosar OA, Aldosari ZA, Alhomaidhi S. A decade-long trends in ligamentum flavum hypertrophy among spinal stenosis patients: a comparative analysis of incedence and patterns. J Orthopaedics. 2025;68:171–174. doi:10.1016/j.jor.2025.05.056
5. Saifuddin A. The Imaging of Lumbar Spinal Stenosis. J Clin Radiol. 2000;55:581–594. doi:10.1053/crad.2000.0223
6. Sakai Y, Wakao N, Matsui H, Osada N. Insulin resistance as a risk factor for flavum hypertrophy in lumbar spinal stenosis. J Spine Surg Related Res. 2024;8(6):583–590. doi:10.22603/ssrr.2024-0025
7. Ali AH, Serhan O, Amier AH, et al. Is there a relationship between low back pain and ligamentum flavum hypertrophy? Eur Rev Med Pharmacol Sci. 2024;28:3822–3827. doi:10.26355/eurrev_202406_36458
8. Mualem W, Liu J, Balu A, Chesney K, Nair N. Biomarkers related to hypertrophy of the ligamentum flavum: a systemic review of the literature. J Neurosurg Spine. 2024;41:33–45. doi:10.3171/2024.2.SPINE23991
9. Yue JJ, Long W. Full endoscopic spinal surgery techniques: advancements, indications, and outcomes. Int J Spine Surg. 2015;9:1–11. doi:10.14444/2017
10. Lui Y, Qi Y, Diaty DM, Zheng G. Treatment of lumbar spinal stenosis secondary to ligamentum hypertrophy using percutaneous endoscopy through interlaminar approach: a retrospective study. J Orthopaedic Surg Res. 2020;15:337. doi:10.1186/s13018-020-01874-5
11. Altun I, Yuksel KZ. Histopathological analysis of ligamentum flavum in lumbar spinal stenosis and disc herniation. Asian Spine J. 2017;11(1):71–74. doi:10.4184/asj.2017.11.1.71
12. Silwal P, Nguyen-Thai AM, Alexander PG, et al. Cellular and molecular mechanism of hypertrophy of ligamentum flavum. J Biomol. 2024;14:1–26.
13. Saadeddin M. Incidence of ligamentum flavum hypertrophy in patients with spinal stenosis. Egyptian Orthopaed J. 2017;52(2):150–152. doi:10.4103/eoj.eoj_35_17
14. Aleksic V, Todorovic J, Miladinovic N, Aleksic N. Ligamentum flavum analysis in patients with lumbar discus hernia and lumbar spinal stenosis. J Scientific Rep. 2023;13:1–10. doi:10.1038/s41598-022-26890-9
15. Altinkaya N, Yildirim T, Demir S, Alkan O. Factors associated with the thickness of the ligamentum flavum, is ligamentum flavum thickness due to hypertrophy or buckling? Spine J. 2011;36(16):1093–1097. doi:10.1097/BRS.0b013e318203e2b5
16. Hiroyuki T, Tsuneo T, Mitsunori Y, Izaya O. The difference in gender affects the pathogenesis of ligamentum flavum hypertrophy. Spine Surg Related Res. 2018;2(4):263–269. doi:10.22603/ssrr.2017-0069
17. Kim SY, Yang MY, Salo S, Sund R, Sirola J. Occupational risk factors for lumbar spinal stenosis: a systematic review. Occup Med J. 2025;75(2):91–98. doi:10.1093/occmed/kqaf005
18. Hamit SK, Ahmet Y, Elmas KA, Soner Y. Effect of ligamentum flavum hypertrophy on lumbar disc herniation with contralateral symptoms and signs: a clinical and morphometric study. Arch Med Sci J. 2010;6(4):617–622.
19. S G, VJ S, Saikrishna G, VK G. Analysis of factors influencing ligamentum flavum thickness in lumbar spine - A radiological study of 1070 disc levels in 214 patients. Clin Neurol Neurosurg J. 2019;182:19–24. doi:10.1016/j.clineuro.2019.04.023
20. Sunita G, Sahana K. Thickness of ligamentum flavum at different levels of lumbosacral spine using magnetic resonance imaging at a tertiary care center. Post Grad Med J Natl Acad Med Sci. 2024;24(4):115–118.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of the Efficacy of Percutaneous Endoscopic Interlaminar Discectomy for Lumbar Disc Herniation with Different Types/Grades of Modic Changes
Shi Z, Li P, Wu W, Jiang Y, Wang Y
Journal of Pain Research 2023, 16:1927-1940
Published Date: 6 June 2023