")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Prevalence and Associated Factors of PTSD Symptoms After the COVID-19 Epidemic Outbreak in an Online Survey in China: The Age and Gender Differences Matter
Authors Mao J, Wang C, Teng C, Wang M, Zhou S, Zhao K, Ye X, Wang Y
Received 24 November 2021
Accepted for publication 17 March 2022
Published 5 April 2022 Volume 2022:18 Pages 761—771
DOI https://doi.org/10.2147/NDT.S351042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yuping Ning
Jiankai Mao,1,* Chaoyue Wang,2,3,* Chao Teng,4,* Mengpu Wang,2,3 Siyao Zhou,2 Ke Zhao,2 Xiangming Ye,5 Yijia Wang6
1Tongde Hospital of Zhejiang Province, Hangzhou, People’s Republic of China; 2Department of Psychiatry, School of Mental Health, Wenzhou Medical University, Wenzhou, People’s Republic of China; 3The Affiliated Kangning Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China; 4The 4th Clinical College of Zhejiang Chinese Medicine University, Hangzhou, People’s Republic of China; 5Zhejiang Provincial People’s Hospital, Hangzhou, People’s Republic of China; 6Wenzhou Seventh People’s Hospital, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangming Ye; Yijia Wang, Email [email protected]; [email protected]
Introduction: The COVID-19 is a highly contagious disease belonging to the family of coronaviruses which can affect a great deal of people shortly. As a devastating event in the world, many people suffer the PTSD from this severe disease. The aim of study is to explore the prevalence and severity of post-traumatic stress disorder (PTSD) symptoms, and discuss the possible factors among the general public in China after the COVID-19 epidemic outbreak.
Methods: This is a cross-sectional study. We used the self-designed demographic questionnaire and the Posttraumatic Stress Checklist-Civilian Version (PCL-C) of Chinese version as our screening tools to investigate 4872 subjects living in the communities in China from Nov. 8th, 2020 to Dec. 8th, 2020.
Results: Finally, we received 3705 effective respondents. The response rates of the questionnaire can reach 76.97 percentage. Peculiarly, the prevalence of PTSD mild and severe symptoms after the COVID-19 epidemic outbreak was 53.2%. Mild PTSD symptoms accounted for 24.9%, and severe PTSD symptoms (scores above 38) accounted for 28.3%. PCL-C mean scores were 41.4± 14.7. The females accounted for 67.7% of the total samples. Participants’ mean age was 30.5± 11.2 years old. The PCL-C gross scores of females were all higher than males in four subject groups. Meantime, gender and age made differences not only in total PCL-C points but also in the four aspects of PCL-C (P< 0.001). The middle-aged group (ages from 45 to 60) got the lowest scores among the four groups.
Conclusion: COVID-19 brought tremendous psychological pressure on the public in many ways, including people’s work, social contact, study, and daily life. Results of our research discover that symptoms of the PTSD are severe, including the re-experiencing, avoidance/numbing, flashbacks, and hyper-arousal. Actions should be taken at society level to prevent and protect individuals from PTSD suffering. Special attention should be paid to females and young people. Further studies should be conducted to explore the dynamic and other risk and protection factors to prevent PTSD.
Keywords: COVID-19, post-traumatic stress symptoms, mental health, age, female
Introduction
The COVID-19 is a highly contagious disease belonging to the family of coronaviruses, which infects many people in a short time due to its person-to-person transmission characteristics.1 COVID-19 has brought huge and numerous casualties. Since the outbreak of COVID-19 in China from December 2019, more than 100 thousand people were infected by this coronavirus. Unfortunately, the COVID-19 has resulted in at least 4 thousand deaths in China.2 Moreover, the number of confirmed cases worldwide has reached 134,384,056. The enormous figures exert overwhelming pressure on governments and medical workers, and the general public, the infected patients of course, even greater.3
The COVID-19 has affected not only the public’s physical health but also their mental health. Up to now, it has become the most urgent and fatal threat and burden in the world.4 Citizens were isolated at home in the initial phase of the COVID-19 outbreak in China, especially in Wuhan. They stayed alone or only lived with their families during their quarantines.5,6 Therefore, they could not communicate with their friends and work that they used to do. They felt lonely, afraid, worried, anxious, and stressed due to social isolation.7 They could not sleep well or even fall asleep.
In general, Post-traumatic stress disorder (PTSD) often follows traumatic events which easily happen in the survivors after devastating blows, serious diseases, and unbearable occurrences8. PTSD symptoms usually include typical patterns of sustained trauma, avoidance of related stimulants, flashbacks of traumatic memories, hyper-arousal, and emotional anesthesia. Clinicians generally make an appropriate diagnosis by referring to the Diagnostic and Statistical Manual of Mental Disorders (DSM) or the International Statistical Classification of Diseases (ICD) based on the symptoms presented by patients. A recent study indicated that avoidance of thoughts and reminders, hypervigilance, overreacted startle response, intrusive thoughts, flashbacks, detachment, and self-destructive behavior were in the network of PTSD symptoms related to COVID-19.9
The PTSD symptoms caused by the previous epidemic was an vital reference in our study. A study demonstrated that 17.3% of health care workers had significant mental symptoms during the SARS epidemic.10 More than 40% of SARS survivors reported experiencing PTSD symptoms at one time after the epidemic outbreak.11,12 Meantime, individuals isolated and in hospitals were more likely to develop high levels of PTSD symptoms than those who were free to go out and do what they love.13 Sun et al explored the severity and prevalence of PTSD and risk factors among Chinese during the COVID-19 one month after the outbreak, and the results showed that the prevalence of PTSD in the Chinese public population was 4.6%. And the study suggested that gender, contact history in epidemic areas, population classification, and subjective sleep quality can be used as predictors of PTSD.14 A study focusing on the nurses demonstrated that the COVID-19 generated more severe trauma on the nurse who got a close to the patients infected by the new coronavirus.15 Another study concentrating on the young adults in America revealed that different degrees of bad mood could be seen among the respondent.16 In China, the number of these researches focusing on the PTSD in community during the COVID-19 pandemic was relatively small. And rarely research could involve the analysis of the differences in various dimensions of PTSD symptoms. Therefore, there were no targeted measures in intervention and treatment. This was mostly due to the lack of a comprehensive understanding of this phenomenon. Health Care Professionals (HCPs) should pay more attention to the occurrence and prevalence of PTSD symptoms about COVID-19 from the lessons of SARS. The Chinese government had taken actions and measurements, including medicine, psychological treatments, and so on, in no time to take control of the epidemic.17,18
The epidemic of the COVID-19 cannot disappear in a short time. Through the analysis of the epidemiology of PTSD under the novel coronavirus epidemic, we aim to find different characteristics of symptoms in different groups. In other words, the special symptoms correspond to the special population. Considering this regularity, we can adjust more effective intervention to alleviate and prevent the occurrence of these mental problems caused by the COVID-19. Furthermore, the people’s psychological protection could be enhanced exceedingly. It is worthwhile to explore the factors that contribute to PTSD symptoms in different people, considering both long-term and short-term effects.
Methods
Study Population
After the COVID-19 pandemic outbreak, we launched an anonymous and voluntary survey in China from 8 November 2020 to 8 December 2020, to find out citizens’ physical and mental health on a public questionnaire platform, whose name is Wenjuanxing (www.wjx.cn). The questionnaire were spread through the chat group in the Wechat application. And the reality of this information was checked by the administrators in every chat group. As a cross-sectional study, we used the Gpower which is an statistical software to calculate the necessary samples.19 The number of our samples is more than the result calculated by the Gpower.
Each subject who was willing to join the research was given electronic informed consent. The study protocol was reviewed and approved by the Local Medical Ethics Committee of the Affiliated Kangning Hospital of Wenzhou Medical University before they started to fill in the questionnaire. Seven members of the ethics committee unanimously approved this study. Participants under 18 years of age were approved by the ethics committee too, and they provided the informed consents along with their parents. And our study complies with the Declaration of Helsinki. Respondents had the option to quit at any time. One important feature about Wenjuanxing was that one account could only answer the questionnaire once.
The inclusion criteria are:1 willing to join in the research;2 never be diagnosed with mental disorders;3 no reading disorder;4 use computer or smartphone independently.
The patients diagnosed with a mental health need to take antipsychotic persistently. However, these effective psychotropic may be suspended by the temporary rules conducted by the local administrators. So some of them will relapse. Similarly, many people with chronic diseases-hypertension, diabetes, stroke, Parkinson’s disease Chronic obstructive pulmonary disease-also need oral medicine to maintain their own healthy condition. The disruption of these critical medicine will develop a anxiety in these people regardless of the COVID-19. So we exclude the people with any physical or mental disorder. The rest of the samples can be identified as healthy people most of who are from the community. There are a great deal of people who are eligible. This screening process will not restrict the variance given the purpose of this study.
The exclusion criteria are:1 had other neurological or mental disorders;2 had been diagnosed with severe physical illness, such as heart disease, diabetes, organic brain disease, or others;3 having difficulty in using computer or smartphone;4 complete the survey less than 2 mins or more than 30 mins, so that the respondents who did not concentrate while completing the questionnaire would be excluded;5 submit the incomplete information.
The Questionnaire of PTSD
The questionnaire has two components: one is the general information focused on demographic characteristics (age, gender, nationality), the other is the Posttraumatic Stress Checklist-Civilian Version (PCL-C). We use PCL-C to evaluate the participants’ current mental health status and the prevalence and severity of PTSD symptoms.
The PCL-C is a 17-item self-report measure, which can be finished within 5–10 minutes. We use the Chinese version of this scale. The Chinese version of the questionnaire was formulated by Yang X and his colleagues in 2007 which was proved great consistency and convergent validity.20 So far, it has been one of the most universal PTSD screening tools in current medical researches. It can not only be used for screening the interviewees’ PTSD symptoms in the past month but also be used for diagnosis and monitoring the changes of participants’ PTSD symptoms based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and PTSD criteria B, C, D.21–23 The scale consists of 4 dimensions: intrusive re-experiencing symptoms (items: 1,2,3,4,5), avoidance/numbing symptoms (items: 6,7,8), social function impairments (items: 9,10,11,12,13,14,15) and alarm responses/hyper-arousal (items: 16,17).
The PCL-C is a 5-Likert scale from 1 (not at all) to 5 (extremely), which indicates how much one is plagued by problems and experiences about stressful life events that occurred in the past month. A symptom was considered present when a participant assessed an item as moderately, quite a bit, and extremely (3,4 or 5).24 Participants rate every item based on their conditions and eventually fulfill the scale quickly. Its total scores range from 17 to 85. Higher scores represent higher effects, with scores of 38 or higher being regarded as probable PTSD.25,26 The scores below 38 are deemed as symptom absent; the scores above 38 can be divided into two conditions: mild symptom (38–49) and severe symptom (50–85).The Chinese version of PCL has been well-validated and widely used in Chinese samples. The scale has good internal and test-retest reliability and validity, the Cronbach’α was 0.915.24,27
Statistical Analyses
All statistical analyses were performed with SPSS 22 for Windows 7. Our study focused on the direct and indirect effects of the prevalence and severity of PTSD symptoms by PCL-C. Two independent samples t-test were performed to analyze demographic statistics. The p-value of less than 0.05 was considered statistical difference.
Results
The Demographic Characteristics (Table 1)
Table 1 depicts the demographic characteristics of the anonymous survey. Ultimately, we received 4872 responses, after filtering the collected data and eliminating the incomplete data, we reserved 3705 questionnaires. The response rate reached 76%. The Cronbach’α was 0.9 in our experimental samples.
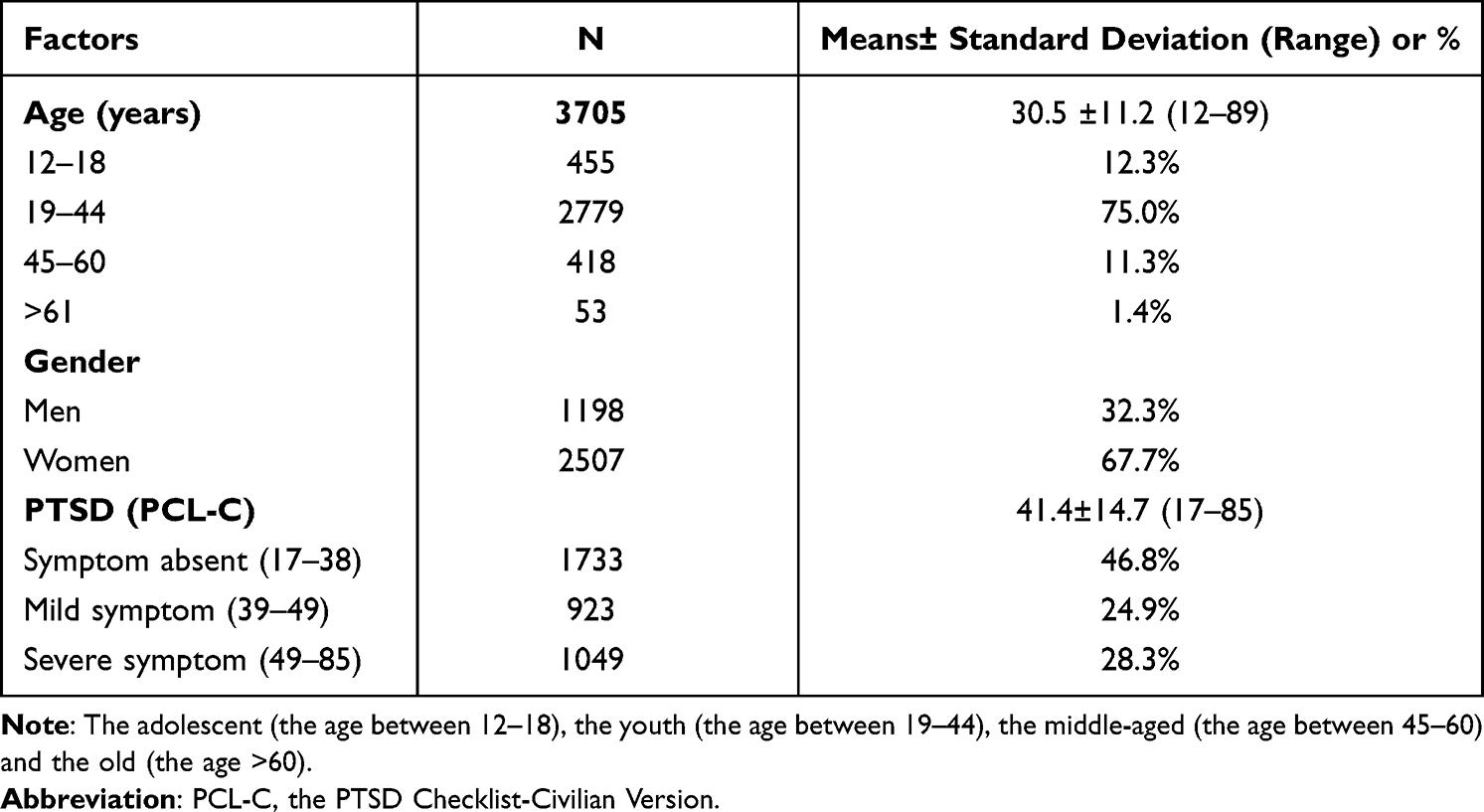 |
Table 1 Demographic Characteristics of the Participants (N=3705) |
The age was divided into 4 groups: adolescent, youth, the middle-aged and the old. Among them, the youth made up the majority.As for gender, the proportion of females is about twice that of males. The PCL-C mean scores were 41.4±14.7. Considering the severity of the symptoms, the proportion of mild and severe symptoms was almost equal. More detailed information could be seen from Table 1.
Gender Matters Across Different Age Groups (Table 2 and Figure 1)
We used the two independent samples t-test in this section. Subjects’ mean age was 30.5±11.2 years old. The ages ranged from 12 to 89. In general, the PCL-C scores of females were higher than males. There were significant gender differences in the adolescent group and the youth group, as indicated in Figure 1. Female subjects all had remarkably higher total PCL-C scores than male subjects in these two groups (p<0.001). This phenomenon could be seen in the other two groups. However, there were no significant gender differences in the middle-aged and the old groups.
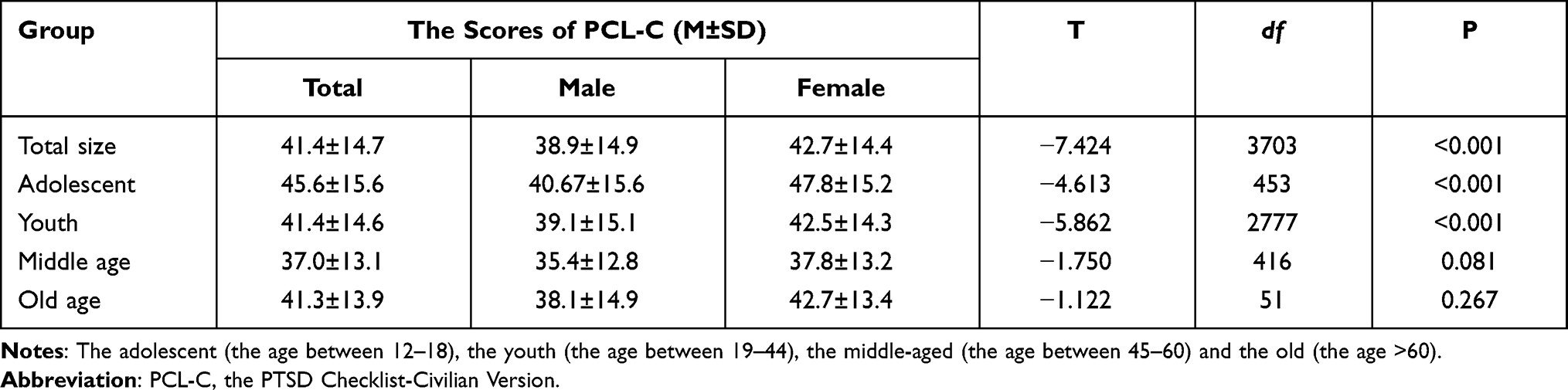 |
Table 2 The Gender Difference of the Scores of PCL-C in Different Groups |
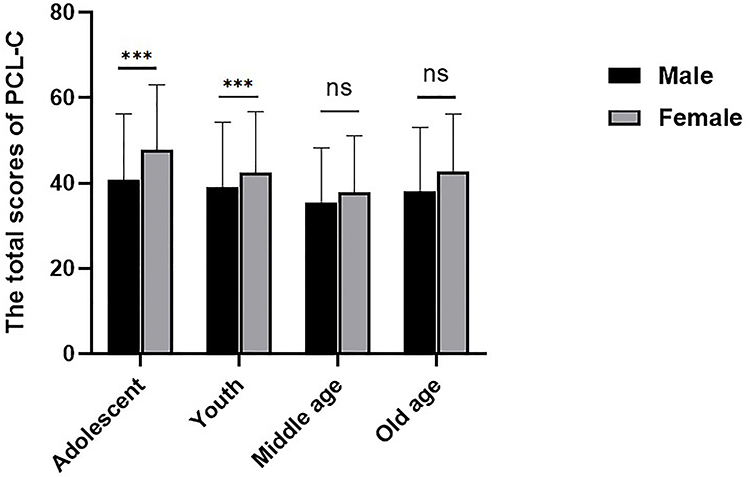 |
Figure 1 The gender difference in different age groups. Abbreviation: PCL-C, the PTSD Checklist-Civilian Version. Notes: Two independent samples t-test was used. The adolescent (the age between 12–18), the youth (the age between 19–44), the middle-aged (the age between 45–60) and the old (the age >60). ***p<0.001. |
Gender and Age Matter in the 4 Dimensions of PCL-C (Table 3A and B and Figure 2)
The two independent samples t-test was used in this section. As mentioned in the methods, the PLC-C consist with four aspects. The results were shown in Table 3A and B and Figure 2, female respondents all had higher scores than male respondents across 4 dimensions. In the adolescent and youth groups, the difference was statistically significant in all aspects of PCL-C (p<0.001), except for the adolescent group in the dimension of alarm responses (p<0.05). The middle-aged group only in the avoidance symptoms aspect was statistically significant (p<0.01). And the old group only in the dimension of alarm response was significant (p<0.05), other aspects were non-significant. Meanwhile, the middle-aged group also had lower scores than adolescents, young people, and the elderly in all 3 aspects, except the dimension of alarm response. The 3 line charts (the scores of intrusive reexperience, avoidance, and social function impairment aspects) run very similar, but the old-aged group of alarm response dimension runs differently. Our data including the total scores and the four aspects scores in every group all fit a normal distribution. However, in the senior group, we find some modestly low scores in the male respondents, compared to female respondents. It may result from the distribution of the data, the senior group makes up a lower proportion. There are more detailed information in the Table 3A and B.
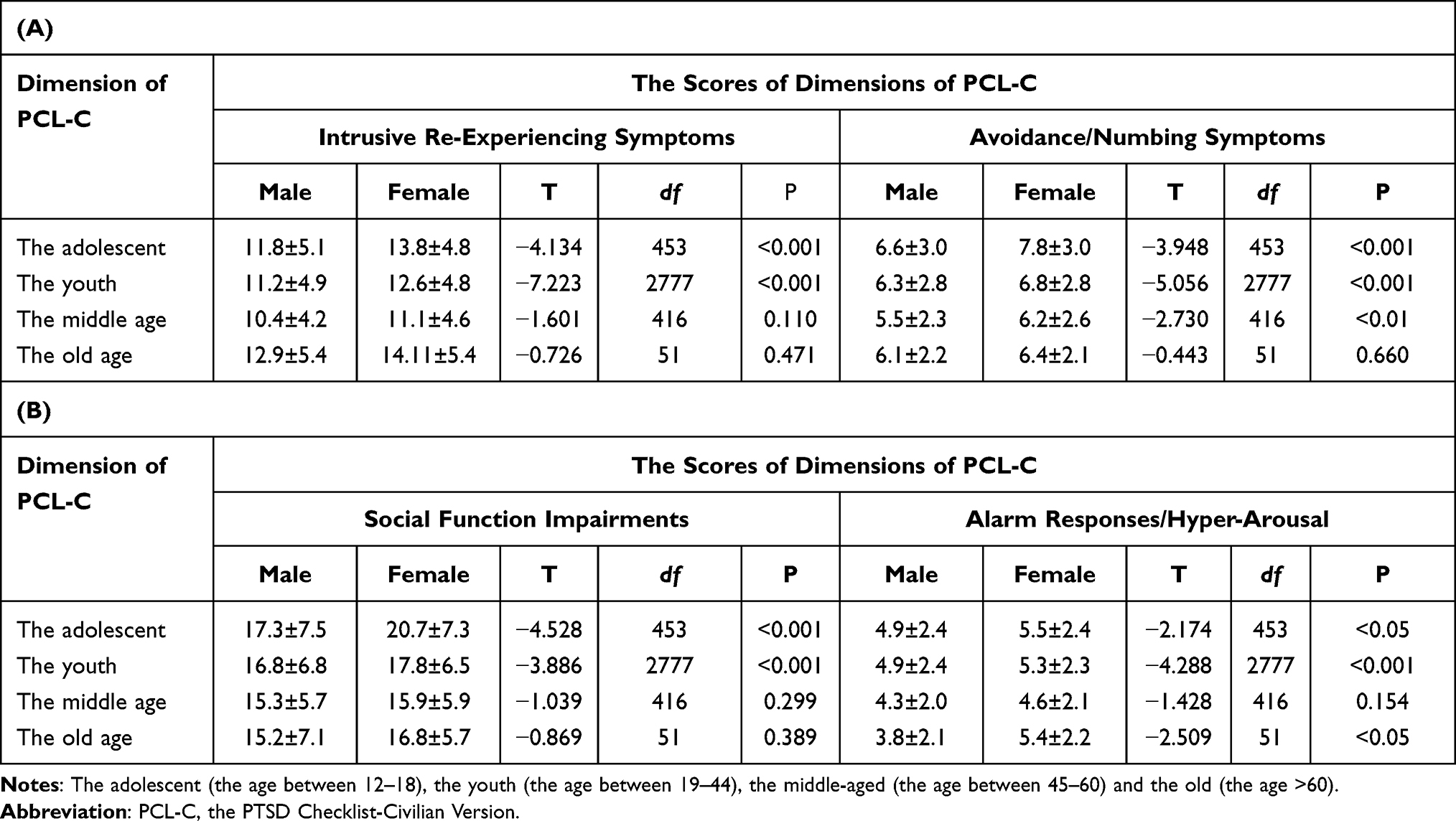 |
Table 3 The Age and Gender Differences in 4 Dimensions of PCL-C |
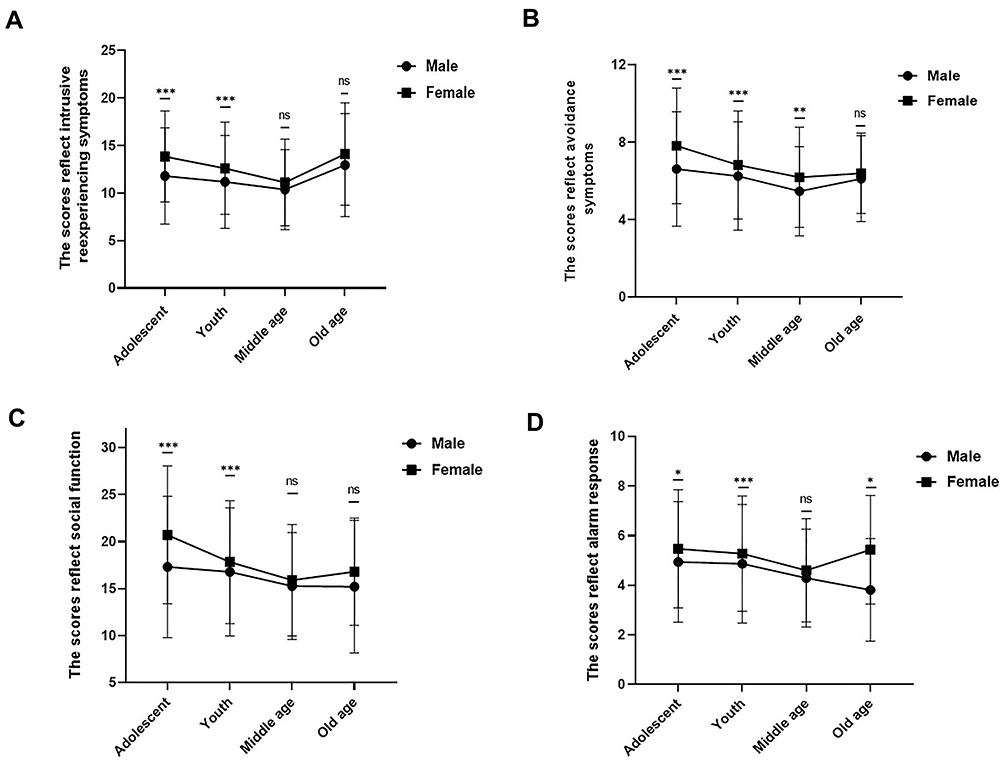 |
Figure 2 The condition of gender and age difference in 4 dimensions of PCL-C. Notes: Two independent samples t-test was used. The adolescent (the age between 12–18), the youth (the age between 19–44), the middle-aged (the age between 45–60) and the old (the age >60). *p<0.05;**p<0.01;***p<0.001. |
Discussion
The prevalence of PTSD symptoms in our study was 53.2%. The emotional and cognitive symptoms is familiar which may cause a kind of suppression among everybody.28,29 Considering some previous experience, it is difficult to separate the share of mental problems that result from the pandemic or other pre-existing factors completely.30
We just focus the symptoms of PTSD and the implication on different persons in this article. Prevalence rates in earlier studies were reported at 7%,31 15.8%,32 and 7.6%,33 respectively. There are another study reporting the prevalence rate less than 7.0%.31 These heterogeneous results may caused by different methods or different periods during the COVID-19 pandemic. The former three studies investigated the immediate impact of the COVID-19 pandemic. But Wang et al reported that during the initial phase of COVID-19, more than half of respondents in China rated as the moderate-to-severe psychological impact.6 The general public might not foresee the infectious disease’s long duration and unexpected changes to society. So they kept an optimistic mind in the wake of the pandemic. The screening tool we selected might increase the false-positive results to some content.
Previous studies have shown that mental health in the general public is affected negatively by the COVID-19 pandemic, and female subjects have more severe and acute PTSD symptoms like anxiety, depression, insomnia than the male in stressful life events and epidemics of infectious diseases, which is consistent with the study.31,34–36 A study focusing the frontline workers draw a similar conclusion that the females are twice as likely as the males to be at risk for potential psychological impairment.37 In terms of the total scores, the result of the present study also suggested that females were more vulnerable to PTSD during the COVID-19 pandemic in the adolescent and the youth groups (the results of the other two groups made no sense).
On one hand, it depends on biological and physical structure, which coordinating the neuroendocrine and autonomic responses.38 It is common knowledge that women’s menstrual cycle contributes to the fluctuation of body temperature and serum gonadal hormone concentrations due to the presence of ovaries. Consequently, females are more emotional, sentimental and vulnerable to psychological disorders. Notably, It is the luteal phase that has been identified as a period of particular vulnerability to develop posttraumatic stress disorder.39 The females make up more than a half in our study, the effect of the hormone should be taken in account. In addition, 75 percentage of the samples lie in 19–44 years old, this is a youthful group. Simultaneously, estradiol may play an important part in the processes. The lower the estradiol, the stronger symptoms of PTSD, especially intrusive memories.40 That’s why in our study females compared to males in the adolescent and youth groups showed significant differences in the aspect of intrusive re-experiencing symptoms. Women of theses ages are healthier and more energetic in their reproductive organs, which was surprisingly consistent with the results.
The females may survive more PTSD than the males, which can be provided by other researches.41,42 So we should devote more attention on the female when they are being in a depressing atmosphere. Many other reasons should be taken into accounts besides the hormone, one of them is the inflammatory cytokines, especially the tumor necrosis factor α (TNF-α) and its receptor named p55 (sTNF-R p55) and p75 (sTNF-R p75) respectively.43 These cytokines may cause oxidative stress in the brain, leading to a variety of bad emotions. In addition, the C-reactive protein (CRP), interleukin 6 (IL-6) may play a coordinating role with the TNF-α.44 Noteworthy, some probable train can lessen this negative mood.45 In summary, it’s a complex mechanism for this vulnerability mentioned of the females.
A research focusing on the impact of social media exposure on mental health found that more than 80% of 4872 respondents concluded were frequent users of the social media during the COVID-19 pandemic. The proportion of women is up to 83.8 percentage, that is a a very high ratio.46 Neria Y et al found that serious public safety incidents can expand its influence through the social media, leading to anxiety or depression-like emotional experience among the population.47
Given that women usually spend more time on the social media, this negative effects are to be more obvious among them.46 So, females may have more possibilities to get access to the negative contents during the COVID-19 pandemic. We speculated that women may be more easily affected by the new media and presses. Chinese people no matter who was at home in their quarantines at the beginning of the COVID-19 outbreak, were in social isolation and connected to the outside world only by the internet so they receiving a mass of information which may confuse themselves eventually. Studies reported that the news exposure on mainstream media about COVID-19 was markedly associated with depressive symptoms.48
There may be two reasons for the phenomenon: First, the reason of the information overload—that a person obtains too much information from the internet in a short time makes it difficult to screen out the right content quickly. This overloaded information will probably cause the user of the phone to be depressed or anxious. Second, the spread of the pessimistic emotions,47 nobody will be happy when he or she were in a this negative condition.
The middle-aged group (age between 45 to 60 years old) got the lowest scores in the total scores and sub-symptom groups. A investigation conducted in the most serious time revealed that, the senior group has significantly lower social media exposure than the younger.49 There may be various reasons, one of them is a certain percentage of people who have experienced major public safety events in the previous years. Rich experience is very useful to alleviate bad emotion. The consequences were also consistent with a previous study that individuals under 40 years old presented more adverse psychological symptoms during the pandemic.3,50 This suggests that the statistical differences between age and gender may be substantially related to social media exposure.
Moreover, a large number of subjects in the adolescent and young groups were students. Quite a few of them may need to take part in the entrance examination to enter a senior high school or university. They were lonely, panicky, and stressed out in the quarantine due to the inefficient online courses, the delays of school opening and exams. This pressure has been enhanced during the COVID-19 pandemic to a great degree and this effects should be considered as a indirect influence by the COVID-19. Some studies also found that the student status was related to higher scores and levels of PTSD symptoms and depressive symptoms during the COVID-19 pandemic.6,51
Undoubtedly, there are a series of risk factors and resilience factors particularly relevant to mental health when epidemics outbreak, like exposure level, working role, working environment, social support, marital status, age, gender, quarantine, coping styles, and so on.52 Our study merely investigated several factors among them, further studies can be devoted to other relevant risk and resilience factors.
Nowadays, the Chinese government has paid more and more attention to individuals’ mental health. In the wake of the COVID-19, medical teams consisting of a large number of psychiatrists and psychological workers participated in the psychological aid and care of the hardest-hit area, Wuhan. But once the epidemic has got under control, they also left Wuhan immediately.
We find the females and the adolescents are vulnerable to the COVID-19 in our study. It’s a strength among the research focusing on mental health during the COVID-19. That other psychological problems may occur in these kind of persons can be inferred when they are facing different fierce events. Psychological characteristics of these two types of people may overlap, in terms of the role in the society. They may have insufficient strength to take care of themselves independently. With regard to the females, they usually have paid a great deal of attention to the family, including taking care of the seniors or kids. However, as for the adolescents, they are in the growing state and may lack enough calm. Considering these different characteristics, the administrators should give more support to lessen the pressure of the females. Some useful measures which focus on convenience for the seniors or kids who need medicinal treatment could be taken. Moreover, Some counseling services for adolescent mental health should be enhanced through the Internet. Therefore, the subsequent psychological support should keep up and continue to mitigate and relieve the long-term impacts of the COVID-19 epidemic on the general population.
Limitation
The study was a cross-sectional design. It’s better if the study could use more instruments to investigate the prevalence and severity of PTSD symptoms and more aspects of risk factors even though the sample was big enough. Since our research is cross-sectional, it is difficult to precisely demonstrate the relationships between mental health and the COVID-19 pandemic. In addition, this is an online questionnaire, the people who cannot get an access to the Internet may not be fully included. In addition, our sample is self-selected which will introduce a selection bias to some extent. While we have a quantity of persons who complete the questionnaire, that’s a very small percentage of the whole population in China. Because of the algorithm on the Internet, the person who pay attention to the PTSD may reflect more intensively. These features may cause some negative impacts on the conclusion moderately. Moreover, there is only one scale in our research, and no scale for assessing anxiety and depression were included. There are few risk factors included in the statistical analysis, only some possible results can be inferred, lacking of the detailed general demographic variables, such as education level, occupation, living area and type, marital status.
Conclusions
The prevalence and occurrence of PTSD symptoms in China was 53.2% in the research population. And 24.9% among them was mild to moderate and 28.3% was severe. There were age and gender differences across all dimensions of PTSD symptoms about the COVID-19 pandemic. In particular, PTSD symptoms including re-experiencing, avoidance/numbing, flashbacks, and hyper-arousal are more common in females and young people than males and seniors.
We find the females and the adolescents are more vulnerable compared with the males. They may need sufficient support from other members of family or the government. A series of effective psychological interventions should be conducted during devastating events. In addition, the promotion of mental health knowledge are definitely essential to people’s fitness. Further studies could investigate and inspect other factors related to COVID-19 besides age and gender.
Data Availability Statement
These data cannot be public due to privacy.
Ethics Statement
Ethical approval was obtained from the research ethics committee of The Affiliated Kangning Hospital of Wenzhou Medical University. And our study complies with the Declaration of Helsinki. Every patient had to sign informed consent before approving participation in the study. Participants under 18 years of age were approved by the ethics committee too, and they provided the informed consents along with their parents.
Acknowledgment
We are grateful to all participants who made contributions to our study.
Author Contributions
JKM and XMY conceptualized and designed the study. CYW, CT, MPW, SYZ, and KZ recruited the participants and completed the screening assessments. YJW and XMY analyzed the data and performed the statistical analysis. CYW wrote the first draft of the manuscript and helped to complete modifications later. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by no fundings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bchetnia M, Girard C, Duchaine C, Laprise C. The outbreak of the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): a review of the current global status. J Infect Public Health. 2020;13(11):1601–1610. doi:10.1016/j.jiph.2020.07.011
2. COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available from: https://coronavirus.jhu.edu/map.html.
3. Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of COVID-19 in China and associated psychological problems. Asian J Psychiatr. 2020;51:102092. doi:10.1016/j.ajp.2020.102092
4. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
5. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
6. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729.
7. Magson NR, Freeman JYA, Rapee RM, Richardson CE, Oar EL, Fardouly J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J Youth Adolesc. 2021;50(1):44–57. doi:10.1007/s10964-020-01332-9
8. Schelling G. Post-traumatic stress disorder in somatic disease: lessons from critically ill patients. Prog Brain Res. 2008;167:229–237.
9. Jiang W, Ren Z, Yu L, Tan Y, Shi C. A network analysis of post-traumatic stress disorder symptoms and correlates during the COVID-19 pandemic. Front Psychiatry. 2020;11:568037. doi:10.3389/fpsyt.2020.568037
10. Lu YC, Shu BC, Chang YY, Lung FW. The mental health of hospital workers dealing with severe acute respiratory syndrome. Psychother Psychosom. 2006;75(6):370–375. doi:10.1159/000095443
11. Lam MH, Wing YK, Yu MW, et al. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med. 2009;169(22):2142–2147. doi:10.1001/archinternmed.2009.384
12. Mak IW, Chu CM, Pan PC, Yiu MG, Ho SC, Chan VL. Risk factors for chronic post-traumatic stress disorder (PTSD) in SARS survivors. Gen Hosp Psychiatry. 2010;32(6):590–598. doi:10.1016/j.genhosppsych.2010.07.007
13. Wu P, Fang Y, Guan Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry. 2009;54(5):302–311. doi:10.1177/070674370905400504
14. Sun L, Sun Z, Wu L, et al. Prevalence and risk factors for acute posttraumatic stress disorder during the COVID-19 outbreak. J Affect Disord. 2021;283:123–129. doi:10.1016/j.jad.2021.01.050
15. Chen R, Sun C, Chen -J-J, et al. A large-scale survey on trauma, burnout, and posttraumatic growth among nurses during the COVID-19 pandemic. Int J Ment Health Nurs. 2021;30(1):102–116. doi:10.1111/inm.12796
16. Liu CH, Zhang E, Wong GTF, Hyun S, Hahm HC. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for U.S. young adult mental health. Psychiatry Res. 2020;290:113172. doi:10.1016/j.psychres.2020.113172
17. Kang L, Li Y, Hu S, et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry. 2020;7(3):e14. doi:10.1016/S2215-0366(20)30047-X
18. Li J, Long X, Zhang Q, et al. Emerging evidence for neuropsycho-consequences of COVID-19. Curr Neuropharmacol. 2021;19(1):92–96. doi:10.2174/1570159X18666200507085335
19. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
20. Xiaoyun Y, Hongai Y, Qifa L. The research on the reliability and validity of PCL-C and influence factors. Chin J Health Psychol. 2007;15(1):6–9.
21. Silva MA. PCL-C. In: Kreutzer J, DeLuca J, Caplan B, editors. Encyclopedia of Clinical Neuropsychology. Cham: Springer International Publishing; 2017:1–4.
22. Cadell S, Regehr C, Hemsworth D. Factors contributing to posttraumatic growth: a proposed structural equation model. Am J Orthopsychiatry. 2003;73(3):279–287. doi:10.1037/0002-9432.73.3.279
23. Wu HC, Chou P, Chou FH, et al. Survey of quality of life and related risk factors for a Taiwanese village population 3 years post-earthquake. Aust N Z J Psychiatry. 2006;40(4):355–361. doi:10.1080/j.1440-1614.2006.01802.x
24. Jin Y, Xu J, Liu H, Liu D. Posttraumatic stress disorder and posttraumatic growth among adult survivors of Wenchuan earthquake after 1 year: prevalence and correlates. Arch Psychiatr Nurs. 2014;28(1):67–73. doi:10.1016/j.apnu.2013.10.010
25. Dobie DJ, Kivlahan DR, Maynard C, et al. Screening for post-traumatic stress disorder in female Veteran’s affairs patients: validation of the PTSD checklist. Gen Hosp Psychiatry. 2002;24(6):367–374. doi:10.1016/S0163-8343(02)00207-4
26. Harrington T, Newman E. The psychometric utility of two self-report measures of PTSD among women substance users. Addict Behav. 2007;32(12):2788–2798. doi:10.1016/j.addbeh.2007.04.016
27. Tang W, Hu T, Hu B, et al. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J Affect Disord. 2020;274:1–7. doi:10.1016/j.jad.2020.05.009
28. Rogers JP, Chesney E, Oliver D, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7(7):611–627. doi:10.1016/S2215-0366(20)30203-0
29. Varatharaj A, Thomas N, Ellul MA, et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. Lancet Psychiatry. 2020;7(10):875–882. doi:10.1016/S2215-0366(20)30287-X
30. Magnavita N, Chirico F, Garbarino S, Bragazzi NL, Santacroce E, Zaffina S. SARS/MERS/SARS-CoV-2 outbreaks and burnout syndrome among healthcare workers. An umbrella systematic review. Int J Environ Res Public Health. 2021;18(8):4361.
31. Liu N, Zhang F, Wei C, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. 2020;287:112921. doi:10.1016/j.psychres.2020.112921
32. González-Sanguino C, Ausín B, Castellanos M, et al. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. 2020;87:172–176. doi:10.1016/j.bbi.2020.05.040
33. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a cross-sectional study. Int J Environ Res Public Health. 2020;17(7):2381.
34. Kendler KS, Thornton LM, Prescott CA. Gender differences in the rates of exposure to stressful life events and sensitivity to their depressogenic effects. Am J Psychiatry. 2001;158(4):587–593. doi:10.1176/appi.ajp.158.4.587
35. McLean CP, Anderson ER. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin Psychol Rev. 2009;29(6):496–505. doi:10.1016/j.cpr.2009.05.003
36. Sønderskov KM, Dinesen PT, Santini ZI, Østergaard SD. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. 2020;32(4):226–228. doi:10.1017/neu.2020.15
37. Di Prinzio RR, Bondanini G, De Falco F, et al. Need for psychological support and disability management programs during and after the COVID-19 pandemic in Italy: preliminary findings from a hospital-based occupational health surveillance program. J Health Soc Sci. 2021;6(3):367–378.
38. Goel N, Workman JL, Lee TT, Innala L, Viau V. Sex differences in the HPA axis. Compr Physiol. 2014;4(3):1121–1155.
39. Soni M, Curran VH, Kamboj SK. Identification of a narrow post-ovulatory window of vulnerability to distressing involuntary memories in healthy women. Neurobiol Learn Mem. 2013;104:32–38. doi:10.1016/j.nlm.2013.04.003
40. Wegerer M, Kerschbaum H, Blechert J, Wilhelm FH. Low levels of estradiol are associated with elevated conditioned responding during fear extinction and with intrusive memories in daily life. Neurobiol Learn Mem. 2014;116:145–154. doi:10.1016/j.nlm.2014.10.001
41. MacGregor AJ, Clouser MC, Mayo JA, Galarneau MR. Gender differences in posttraumatic stress disorder among U.S. Navy healthcare personnel. J Womens Health. 2017;26(4):338–344. doi:10.1089/jwh.2014.5130
42. Wesemann U, Zimmermann PL, Bühler A, Willmund GD. Gender differences in hostility and aggression among military healthcare personnel after deployment. J Womens Health. 2017;26(10):1138. doi:10.1089/jwh.2017.6550
43. Himmerich H, Wesemann U, Dalton B, Holdt LM, Teupser D, Willmund GD. Exploring an association between hostility and serum concentrations of TNF-α and its soluble receptors. J Psychosom Res. 2016;91:87–88. doi:10.1016/j.jpsychores.2016.11.001
44. Boisclair Demarble J, Moskowitz DS, Tardif J-C, D’Antono B. The relation between hostility and concurrent levels of inflammation is sex, age, and measure dependent. J Psychosom Res. 2014;76(5):384–393. doi:10.1016/j.jpsychores.2014.02.010
45. Wesemann U, Hadjamu N, Wakili R, et al. Gender differences in anger among hospital medical staff exposed to patients with COVID-19. Health Equity. 2021;5(1):181–184. doi:10.1089/heq.2020.0119
46. Gao J, Zheng P, Jia Y, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. 2020;15(4):e0231924. doi:10.1371/journal.pone.0231924
47. Neria Y, Sullivan GM. Understanding the mental health effects of indirect exposure to mass trauma through the media. JAMA. 2011;306(12):1374–1375. doi:10.1001/jama.2011.1358
48. Olagoke AA, Olagoke OO, Hughes AM. Exposure to coronavirus news on mainstream media: the role of risk perceptions and depression. Br J Health Psychol. 2020;25(4):865–874. doi:10.1111/bjhp.12427
49. Nwachukwu I, Nkire N, Shalaby R, et al. COVID-19 pandemic: age-related differences in measures of stress, anxiety and depression in Canada. Int J Environ Res Public Health. 2020;17:17. doi:10.3390/ijerph17176366
50. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi:10.1016/j.psychres.2020.112954
51. Lei L, Huang X, Zhang S, Yang J, Yang L, Xu M. Comparison of prevalence and associated factors of anxiety and depression among people affected by versus people unaffected by quarantine during the COVID-19 epidemic in Southwestern China. Med Sci Monit. 2020;26:e924609. doi:10.12659/MSM.924609
52. Carmassi C, Foghi C, Dell’Oste V, et al. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res. 2020;292:113312. doi:10.1016/j.psychres.2020.113312
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.