")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Prevalence and Associated Factors of Human Immune Deficiency Virus and Tuberculosis Co-Infection in Patients Attending Kolla Diba Health Center, Dembia District, Northwest Ethiopia
Authors Asmamaw Dejenie T , Mamo Degu W , Birara Aychiluhm S , Chekol Abebe E , Tiruneh G/Medhin M
Received 16 December 2020
Accepted for publication 29 January 2021
Published 12 February 2021 Volume 2021:13 Pages 191—196
DOI https://doi.org/10.2147/HIV.S282201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Tadesse Asmamaw Dejenie,1 Worku Mamo Degu,2 Setognal Birara Aychiluhm,3 Endeshaw Chekol Abebe,4 Markeshaw Tiruneh G/Medhin1
1Department of Biochemistry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Public Health, College of Medicine and Health Sciences, Samara University, Samara, Ethiopia; 3Carter Center, Atlanta, Ethiopia; 4Department of Biochemistry, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Tadesse Asmamaw Dejenie Tel +251 909045760
Email [email protected]
Background: TB-HIV co-infection is the most common problem of African countries, especially, Sub-Saharan countries including Ethiopia. So this study aimed to assess TB-HIV co-infection with its associated factors in patients with Tuberculosis in Northwest Ethiopia. Although the prevalence of TB-HIV was low, the need for strengthening the health extension program especially in urban dwellers also needed to include TB-HIV testing.
Objective: This study aimed to assess TB-HIV co-infection with its associated factors in patients with Tuberculosis in Northwest Ethiopia.
Methodology: Institutional based cross-sectional study has been done and a total of 638 subjects participated in the study. The data of the study subjects were collected from the tuberculosis logbook using two trained data collectors who were work in the TB DOTS program and by using a well-prepared checklist and SPSS was used for analyzing data.
Results: 9.7% (62/638) of TB patients were found to be co-infected with HIV. Among these 32 (11.4%) were females and 30 (8.4%) were males. More infected individuals were found in urban residents 44 (20%) than rural residents and age groups 30– 40 years 31 (22.5%) are more infected than the other age group. TBforms, age, and residence were associated with HIV/TB co-infection significantly.
Conclusions and Recommendations: Although the prevalence of TB-HIV was low, the need for strengthening the health extension program especially in urban dwellers is needed to include TB-HIV testing. Further surveys involving HIV infected TB patients to strengthen and scale-up for TB and HIV is needed.
Keywords: TB-HIV co-infection, Kolla Diba, Northwest Ethiopia
Background
TB-HIV co-infection is the most common problem of African countries, especially, Sub-Saharan countries including Ethiopia.1 Tuberculosis (TB) is the leading cause of death among adults living with HIV/AIDS. Late diagnosis of TB is a major contributor. HIV decreases the disease protection capability of the individual which increases the chance of infecting with TB. The latent TB can progress to active TB in individuals infected with HIV. This virus can also alter the usual sign/symptom of TB and its connection with TB induces a high magnitude of drug-resistant TB.1 Without HIV infection, the chance of changing to active TB is about 10%. But for those HIV-infected individuals, it can be tenfold. Smear-negative pulmonary TB (PTB) and extrapulmonary TB (EPTB) are the most common problems in HIV co-infected individuals.2
The burden of TB-HIV co-infection is higher in developing countries. In African countries, 82% of TB cases are reported in individuals co-infected with HIV.3,4 In Ethiopia, which is under sub-Saharan African countries, the magnitude of new cases had raised from 55,000 to 100,000 in the last 10 years. The HIV/AIDS pandemic has substantially altered the epidemiology of tuberculosis. The findings of different studies showed that for individuals co-infected with TB and HIV the annual risk of developing active TB is 5–8%.5 In general, the human immunodeficiency virus (HIV) leads to a serious challenge to control tuberculosis (TB).6 The late screening and diagnosis are the major cause of this. Compared to other opportunistic Infections, TB occurs earlier in the course of HIV infection even when the immune system is fairly competent.7 In Ethiopia, the burden of TB/HIV co-infection is increasing and deserves special attention.
Therefore, data about the extent and trends of the dual infection is important for effective prevention and control programs. However, there are limited studies that describe the association between the two diseases in Ethiopia still now.
This study aimed to assess TB-HIV co-infection with its associated factors in patients with Tuberculosis in Northwest Ethiopia.
Methods and Materials
Study Area
The study was done at Kolla Diba health center (the first health center in Ethiopia), Dembia district, which is located in North Gondar, Amhara region. The distance of the study area is 729 km away from Addis Ababa (Capital City of Ethiopia).
Study Design and Period
A cross-sectional document review study was done using the data from November 2018 –December 2019 by reviewing TB registration Logbook reports at Kolla Diba health center and the study was conducted from January 15/2019 to February 30/2019.
Source Population
All TB patients that were registered from TB room in the logbook form in Kolla Diba health center from 2018– 2019.
Study Population
TB patients who were tested for HIV registered from November 2018 to December 2019.
Sample Size and Sampling Method
A sample size of 638 TB patients that were registered in the logbook and tested for HIV from February 2018 to December 2019 was participated in the study by using a consecutive sampling technique.
Study Variables
Dependent Variable
- HIV co-infection
Independent Variable
- Age
- sex
- Weight
- Residence (urban/rural),
- Type of Tuberculosis,
- TB category
Eligibility Criteria
- All cases registered in the TB clinic logbook from February 2018-December 2019 and tested for HIV were included in the study.
Data Collection Tool and Procedure
The data collection tool (checklist) was prepared based on the variables found in the patient record book, and then data was collected by using the checklist tool by reviewing patient history.
Data Quality Control and Management
The data was maintained using a data collection tool which is adapted from the national standard. Close supervision during the data collection period was done by the principal investigator and using well-trained data collectors (two clinical nurses) who work in TB room classes. Data were managed using a statistical package (SPSS) and were cleaned and coded in line with previous literature.
Data Analysis and Management
The data were checked, cleared, coded, and entered into Statistical Package for the Social Sciences (SPSS) for analysis. The data was presented by using tables, graphs, and charts. Proportions and summary statistics such as mean, the standard deviation was calculated for variables. The determinant factors were identified using binary logistic regression. The univariate was first checked, and then variables that were significant at a p-value of <0.05 were used for multivariable analysis.
Ethical Consideration
The study was based on the Declaration of Helsinki. Collaboration letter for data collection was obtained from North Gondar Zonal Health Department with protocol number 1996/05/18. The study protocol was approved by North Gondar Zonal Health Department. Informed consent was obtained from the participants before sample collection. Patient identifiers like the name of patients were not used during the entire work process and data were not used for other purposes.
Results
Socio-Demographic Characteristics of Study Subjects
A total of 638 TB patients have participated in the study. Among these 357 (56%) were males and 281 (44%) were females. The mean (±SD) age of respondents enrolled in the study was 31.7 ±17.7 years. Nearly more than half of the study participant 421 (66%) were residing in rural while 217 (34%) were from the urban setting (Table 1)
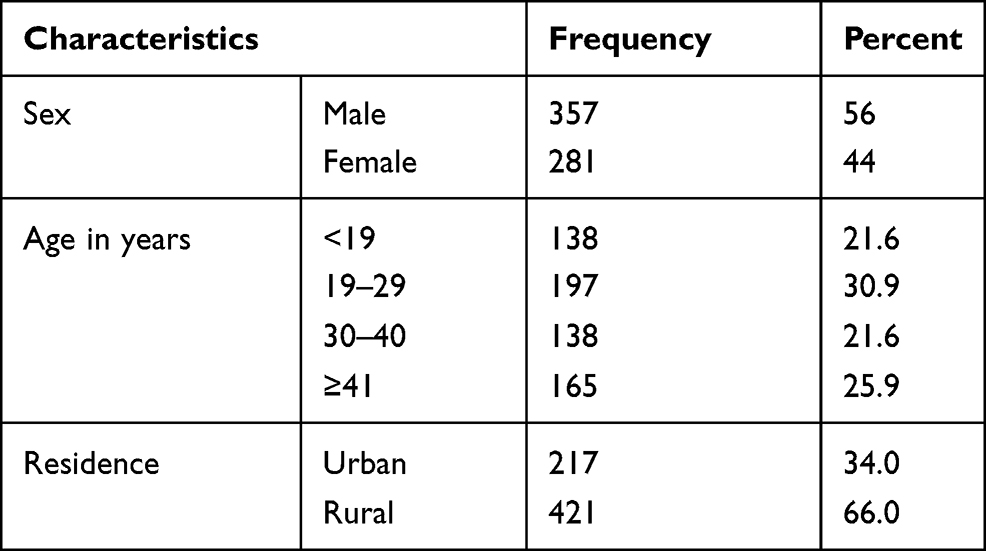 |
Table 1 Socio-Demographic Characteristics of the Study Participants; Kolla Diba Health Center, Gondar, Ethiopia, 2018–2019 |
Clinical Feature of the Study Participants
During intensive anti-tuberculosis treatment, the mean initial weight was found to be 42.7 Kg (SD± 12.1). Concerning with type of tuberculosis majority of tuberculosis cases, 268 (42%) were extra-pulmonary TB, and the rest pulmonary smear-negative TB and Smear positive pulmonary TB are 240 (37.6%) and 130 (20.4%) respectively. Regarding with type of tuberculosis category, almost all the study participants 628 (98.2%) were new TB in case of treatment outcome, majority of the 68.3% (436) were treatment completed, 14.7% (94) were cured and 63 (90.9) transfer out. But 27 (4.2%) of them were died (Table 2).
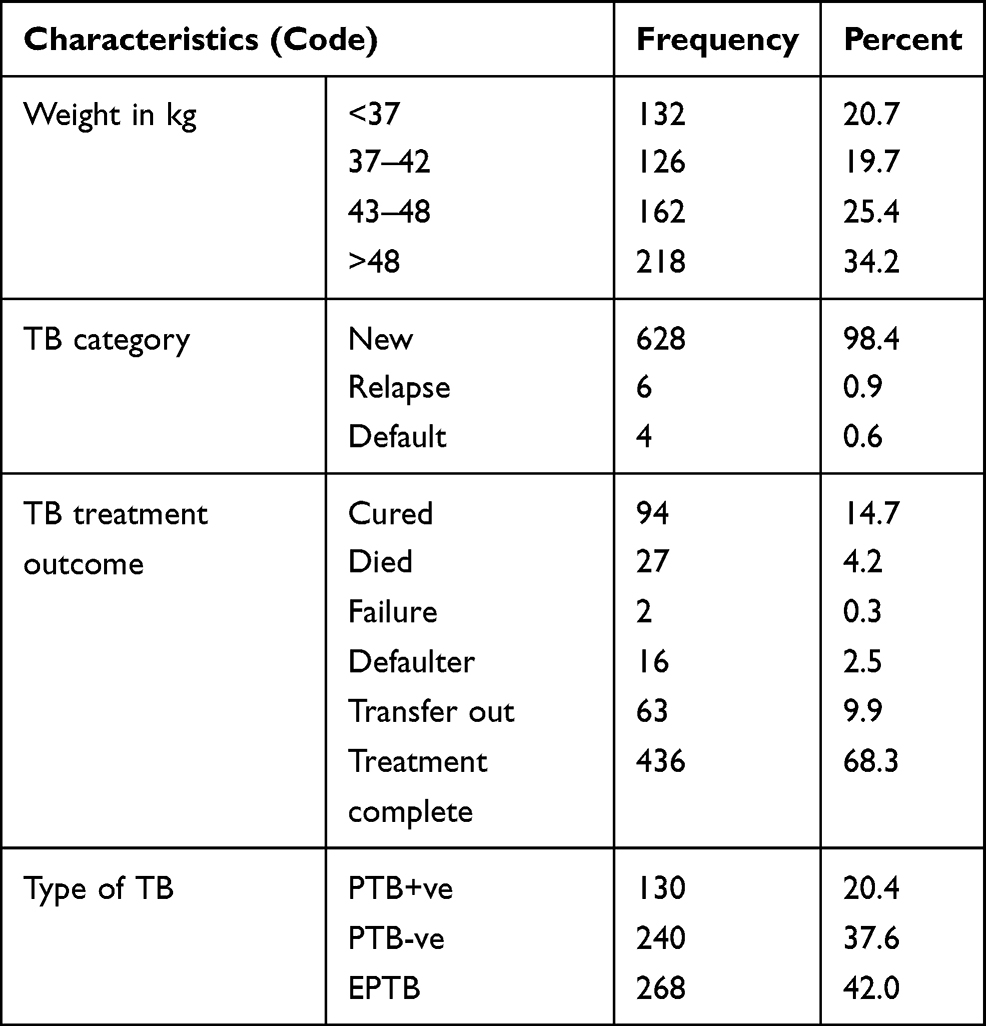 |
Table 2 Frequency Distribution of Clinical Feature for Assessment and Associated Factor of HIV Among TB Patients in Kolladiba Health Center, 2018–2019 |
Prevalence and Its Associated Factors of HIV Infection Among Patients with TB
In a total of 638 study participants prevalence of HIV was 9.7% (62/638) among this study female11.4% (32/281) more affected than males 8.4% (30/357). A higher rate of the virus was observed among urban residents 20% (44/217) than rural residents and age groups 30–40 years 22.5% (31/138) are more infected than the other age group. From this study the TB category result is shown their homogeneity of data due to this it cannot be comparable with HIV status. The associated factors of HIV co-infection in multivariate analysis were Residence AOR 5.19 with 95% CI (2.85–9.46), age group (<19yrs AOR 0.19 with 95% CI (0.04–0.74), and 30–40 AOR 2.87 with 95% CI (1.38–5.96)) and smear-positive pulmonary TB at AOR 2.09 with 95% CI (1.08–4.04) are associated with HIV co-infection with P<0.05 (Table 3).
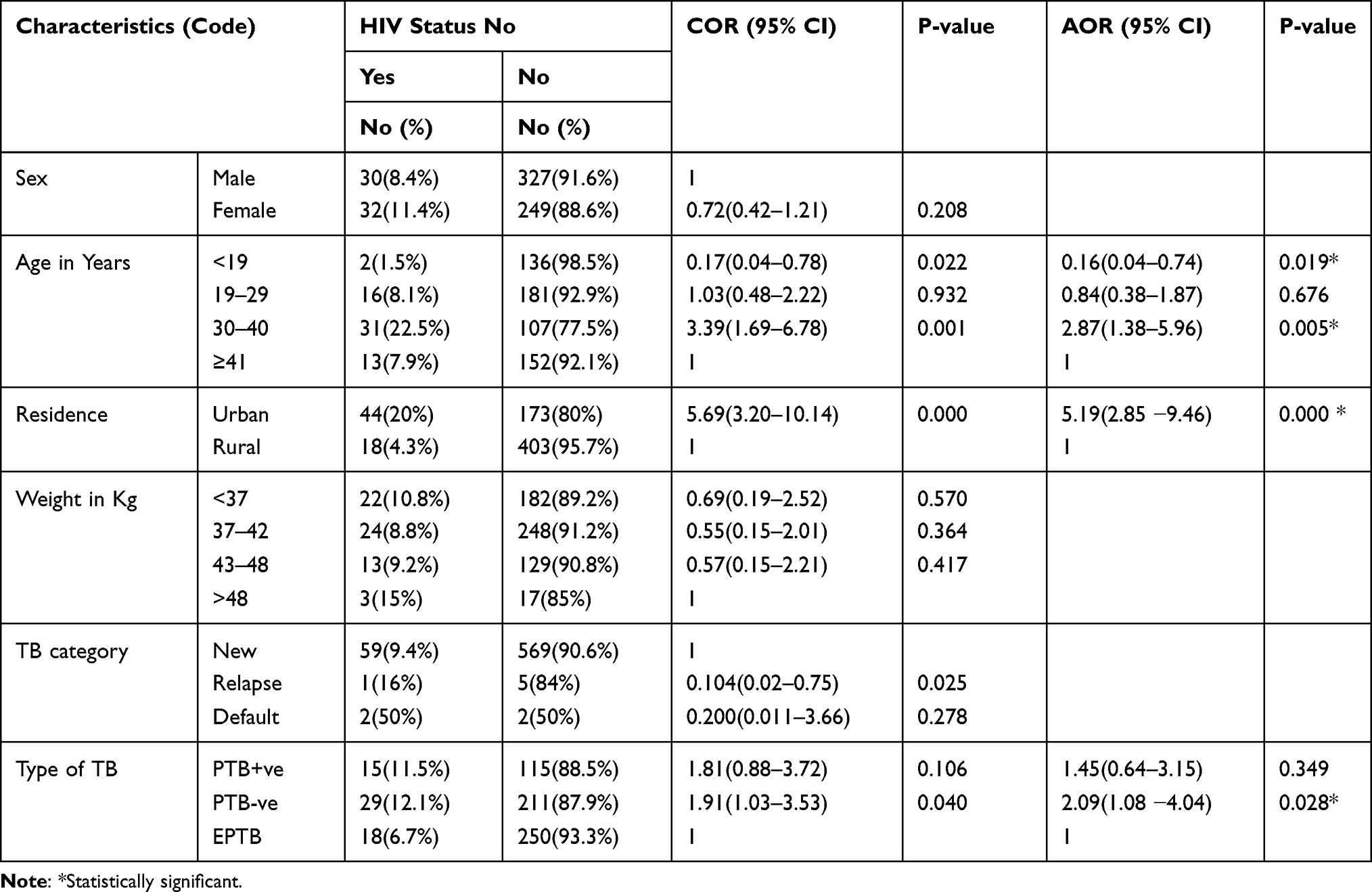 |
Table 3 Risk Factors That Associated with HIV Co-Infection Attended Among TB Patients at Kolla Diba Health Center, Gondar, Ethiopia 2018–2019 |
Discussion
In the present study, the prevalence of HIV co-infection was found to be 9.7%. The finding was similar to other studies conducted at Northwest Ethiopia, Dabat (11.4%), and 2012 WHO report (13.0%).8 But the finding was lower than the studies conducted in Addis Ababa (45.3%), Debre Markos Hospital 20 (44.8%), Felege Hiwot Hospital, revealed 21 (33.5%), FMOH annual report (31%),6 Cameron 14 (23.8%), Asia 10 (22%) And it was higher other studies.11,13 The difference might be due to the increasing public awareness, study area, study design, health system infrastructure.
About 51.6% of HIV co-infected TB patients were females. This was in line with another study.12 This might be due to the higher exposure of females for sexual activities earlier than men in case of economic reasons.
The prevalence of HIV co-infection among TB patients was found to be higher (53%) in younger age groups (<19 years) and in the age group of 30–40 years which is 2.87 times more risk than the other age group. The age group is significantly associated with HIV co-infection (P<0.05). This is consistent with other studies conducted at Dabat and Debre Markos hospital.9,13
This study showed that urban residents of TB patients have a fivefold chance of being HIV co-infected. The finding was found to be strongly and significantly associated with HIV co-infection. This was similar to the study which was done in the Southern Nations, Nationalities, and Peoples’ Region (SNNPR).14 These associations might be due to the problem of urban health extension programmed implementation and displacement of peoples from rural to urban because of their labor work.
In this study, higher HIV co-infection 29 (46.7%) was found in pulmonary negative individuals which were 2.09 folds risk of being HIV co-infected and the extrapulmonary type was found to be 18 (29%). HIV co-infection is significantly associated with smear-negative pulmonary tuberculosis cases. This was similar to the study done in Northern Ethiopia.9,10
Conclusions and Recommendations
In the study, HIV co-infection was statistically and significantly associated with age, residence, and type of TB. In urban dwellers, HIV co-infected was higher than in rural dwellers. To alleviate those problems further studies strengthening, and scale-up for TB and HIV collaborative activities (prevention and control aspects) is recommended. In the study area (Ethiopia) there is a disease prevention program called the Health Extension Program. To strengthen the health extension program, creating awareness about HIV-TB co-infection in the community should be recommended.
Abbreviations
AIDS, Acquired Immunodeficiency syndrome; ART, Anti-Retroviral Therapy; CPT, Cotrimoxazole Preventive Therapy; EPTB, Extra-pulmonary Tuberculosis; FMOH, Federal Ministry of Health; HIV, Human Immunodeficiency Virus; OIs, Opportunistic Infections; OR, Odds Ratios; PLWHA, People Living with HIV/AIDS; PTB, Pulmonary Tuberculosis; SPSS, Statistical Package for Social Sciences; STD, Sexually Transmitted Diseases; TB, Tuberculosis; TDR, Tropical Disease Research; WHO, World Health Organization.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to this work, in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported both financially and materially by Ethiopian Public Health Institution (EPHI) in collaboration with Addis Ababa University.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Tesfaye B, Alebel A, Gebrie A, Zegeye A, Tesema C, Kassie B. The twin epidemics: prevalence of TB/HIV co-infection and its associated factors in Ethiopia; a systematic review and meta-analysis. PLoS One. 2018;13(10):e0203986. doi:10.1371/journal.pone.0203986
2. Addo KK, Ampofo WK, Owusu R, et al. First nationwide survey of the prevalence of TB/HIV co-infection in Ghana. J Tuberc Res. 2018;6:135–147. doi:10.4236/jtr.2018.62013
3. Federal Democratic Republic of Ethiopia Ministry of Health. Guideline for clinical and programmatic management of TB, leprosy and TB/HIV in Ethiopia,5 edition
4. Kedir W. Assessment of HIV seroprevalence among registeredTuberculosisPatientsinArsiZone, South East Ethiopia. 2011.
5. Gao J, Zheng P, Fu H, Zheng JC. Prevalence of TB/HIV co-infection in countries except China: a systematic review and meta-analysis. PLoS One. 2013;8(5):e64915. doi:10.1371/journal.pone.0064915
6. CDC. National center for HIV/AIDS, viral hepatitis, STD, and TB prevention division of tuberculosis elimination.
7. TDR operational research to reduce TB. TB and HIV research;[email protected].
8. WHO. Global tuberculosis report launched. October 24, 2012/2013
9. Ahmed E, Girma T, Moges W, Mengistu E. Tuberculosis and human immune deficiency virus co-infection in Debre Markos Referral Hospital in Northwest Ethiopia. a Five Years Retrospective Study. JAIDS Clin Res. 2013;4:263. doi:10.4172/2155-6113.1000263
10. Bezabih B, Demilew B, Andargie N. Assessment of tuberculosis and HIV co-infection among patients attending TB clinic in FelegeHiwot Hospital, Bahirdar, North West Ethiopia. 2009/2010.
11. Afework K, Getahun M, Belete ED, et al. Coinfection and clinical manifestations of tuberculosis in human immunodeficiency virus-infected and uninfected adults in Gondar teaching hospital, Northwest Ethiopia. J Microbiol Immunol Infect. 2007;40:116–122.
12. Sebsibe T, Takele T. HIV co-infection among tuberculosis patients in Dabat, northwest Ethiopia. J Infect Dis Immun. 2013;5(3):29–32. doi:10.5897/JIDI2013.0117
13. Wondimeneh Y, Muluye D, Belyhun S. Prevalence of pulmonary tuberculosis and immunological profile of HIV co-infected patients in Northwest Ethiopia. BMC Res. 2012;5:331.
14. Datiko DG, Yassin MA, Chekol LT, Kabeto LE, Lindtjørn B. The rate of TB-HIV co-infection depends on the prevalence of HIV infection in a community, in the Southern Nations, Nationalities, and Peoples’ Region (SNNPR) of Ethiopia. BMC Public Health. 2008;2458-8:266. doi:10.1186/1471-2458-8-266
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.