")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Prevalence and Associated Factors of Clinical Vitamin A Deficiency Among Pre-School Children 1–5 Years of Age in Rural Kebeles in Farta District, South Gondar Zone, Ethiopia: A Mixed Methods Study
Authors Yisak H , Elmneh R, Taklual W , Ewunetei A , Kefale B
Received 30 August 2020
Accepted for publication 6 October 2020
Published 20 October 2020 Volume 2020:13 Pages 1191—1201
DOI https://doi.org/10.2147/JMDH.S279571
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hiwot Yisak,1 Rishah Elmneh,2 Wubet Taklual,1 Amien Ewunetei,3 Belayneh Kefale4
1Department of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Amhara, Ethiopia; 2Department of Supply Chain, Distribution and Sales, Julphar Pharmaceuticals Plc, Addis Ababa, Ethiopia; 3Department of Pharmacology, College of Health Sciences, Debre Tabor University, Debre Tabor, Amhara, Ethiopia; 4Department of Clinical Pharmacy, College of Health Sciences, Debre Tabor University, Debre Tabor, Amhara, Ethiopia
Correspondence: Hiwot Yisak
Department of Public Health, College of Health Sciences, Debre Tabor University, PO Box 272, Debre Tabor, Amhara, Ethiopia
Tel +251 913728949
Email [email protected]
Background: Globally, pre-school children are the most at-risk population groups for vitamin A deficiency (VAD). The 2009 World Health Organization (WHO) report stated that one-third (190 million) of pre-school children worldwide are deficient in vitamin A. Both clinical and subclinical VAD have been a long-standing problem in developing countries. In Ethiopia, VAD was recognized as a public health problem 4– 5 decades before. Since then, researches conducted in other parts of the country still showed varied and high prevalence, which is 2– 8 times higher than WHO cut-off points. This community-based study was therefore conducted on pre-school children of rural kebeles in Farta district to determine the prevalence of clinical VAD (Bitot’s spot and night blindness) and associated factors.
Methods: A community-based cross-sectional mixed quantitative and qualitative study was conducted. Randomly selected 588 pre-school children participated in the study. The clinical aspect of the study investigated the presence of Bitot’s spots on the children’s eye with the aid of a magnifying loop and torch. Data on the history of night blindness were obtained from mothers/caregivers by using WHO standard questions. The qualitative study data were obtained via a key informant interview with the mothers/caregivers whose child has clinical VAD. Quantitative data were entered using Epi Data statistical software and analysed by using SPSS version 20 statistical software package. A bivariable logistic regression was employed, and variables that showed significant association with clinical VAD (P < 0.2) were entered a multivariable logistic regression model to identify independent predictors of clinical VAD.
Results: The prevalence of Bitot’s spot and night blindness was 0.8% and 1.2%, respectively. Pre-school children who were from highland (AOR: 3.71; 95% CI: 1.01– 13.68), a mother having antenatal care (ANC) visit during pregnancy of a child (AOR: 8.63; 95% CI: 2.58– 28.79), family monthly income (AOR: 8.63; 95% CI: 2.58– 28.79) and handwashing frequency were found to be determinants of VAD (p < 0.05).
Conclusion: Clinical vitamin A deficiency in the study area is of public health concern because the prevalence of Bitot’s and night blindness was above the WHO threshold level. Accordingly, effective preventive measures should be designed to reduce VAD prevalence.
Keywords: clinical vitamin A deficiency, Bitot’s spots, night blindness, Farta district
Plain language summary
Internationally children are at higher risk of vitamin A deficiency. World Health Organization report expressed that 33% (190 million) of children overall are insufficient in vitamin A. In Ethiopia, vitamin A deficiency was perceived as a general medical issue 4–5 decades prior. From that point forward, researches done long ago in different parts of the nation showed the varied and high result. So we examined clinical vitamin A deficiency, which has a manifestation of Bitot’s spots (foamy substance on the eye), night-visual impairment and related factors.
- We choose 588 children.
- We checked Bitot’s spots on the kids’ eye with amplifying light.
- We asked guardians’ information on the history of night-visual impairment and other factors related to vitamin A deficiency.
We found that out of the total children:
- 0.8% have Bitot’s spot 1.2% of them have of night-visual impairment
- Cumulatively 2% of children have clinical vitamin A deficiency
The investigators concluded that clinical vitamin A deficiency in the studied area is of great concern because; the commonness of Bitot’s and night-visual impairment was over the WHO edge level.
Identified risk factors for vitamin A deficiency
- Living in high-land agro-ecology
- Mothers not having pregnancy follow-up
- Family monthly income of less than 16.7 USD
- Washing frequency less than 3 times a day and
- Hand washing with water only
Introduction
Vitamin A is a fat-soluble vitamin that a body gets in limited quantities from diets, and the surplus can be stored principally in the liver. It plays a significant role in various body functions, such as vision, growth, immunity, integrity of epithelial cells and survival. The recommended daily allowance (RDA) for vitamin A varies according to age and gender. If the intake of vitamin A is below the required level, a variety of manifestations may occur, which can collectively be called Vitamin A Deficiency Disorders (VAD).1,2
In pre-school children, the prevalence of Bitot’s Spot >0.5% and child night blindness >1% are used as WHO cut-off points to declare that VAD is of public health importance in the community. Bitot’s spots are typically dry-appearing triangular patches of xerosed conjunctiva with a layer of foam on the surface, usually located temporal to the cornea. And night blindness is an early symptom which is an inability to see in dim light, whereas xerophthalmia is a dry eye which is a medical condition in which the eye fails to produce tears. It may be caused by vitamin A deficiency, which is sometimes used to describe that condition, although there may be other causes.3 At the community level, WHO recommends that when 2% to 10%, 10% to 20%, and more than 20% of children in a population have serum retinol levels less than 0.7 µmol/L, the communities should be considered as mildly deficient, moderately deficient, and severely deficient, respectively.4,5
In 2005 the Ethiopian Health and Nutrition Research Institute (EHNRI) conducted a national clinical vitamin A deficiency survey on pre-school children. The survey results revealed that, at the national level, the prevalence of night blindness was 0.7%. On the other hand, Bitot’s spots prevalence rate was 1.7%, which is more than three times of the WHO threshold (0.5%) suggesting that vitamin A deficiency is a public health problem even though there is periodic high-dose vitamin A supplementation programs which have been established over the last three decades in Ethiopia to increase child survival and decrease the incidence of pediatric blindness.2
Globally, pre-school children and reproductive-age women are the two most common groups of the population at risk of vitamin A deficiency.6 According to a recent WHO report (2009), one-thirds (190 million) of the world’s pre-school children were vulnerable to xerophthalmia in 2009.7 Aserat et al, 2002 suggested that pre-school children are likely to be at risk of xerophthalmia due to relatively high growth requirements and relatively low vitamin A body store.8
Both clinical and subclinical VAD have been a long-standing problem in developing countries. In Ethiopia, VAD was recognized as a public health problem 4–5 decades before. Since then, research conducted in different parts of the country still showed higher prevalence, which is 2–8 times higher than WHO cut-off points.2,9,10
Vitamin A deficiency is a disabling and potentially fatal public health problem in children under the age of 6. It is also a major cause of preventable childhood blindness and a significant contributor to morbidity and mortality from infections.11 Approximately 30% of the world’s childhood blindness is due to VAD, and 250,000–500,000 children are blind every year. According to the research done byet al, 2007, the severity of VAD can be explained by looking at the estimated relative risks in pre-school age children of 1.86 for measles mortality, 2.15 for diarrhoea mortality, 1.78 for malaria mortality and 1.13 for other infectious disease mortality.12
Evidence shows that the chances of survival of pre-school children are increased when vitamin A status improves because improving the vitamin A status of children with a deficiency can reduce the measles and diarrhea mortality rates by 50% and 33%, respectively, and can reduce the risk of all causes of mortality by 23–34%.13,14 Obviously for intervention up-to-date, comprehensive and aggregated information on the magnitude of clinical VAD is required.
However, existing literatures on VAD in Ethiopia showed that there is a lack of data on the area-specific extent of clinical VAD and associated factors among pre-school children. Therefore, this community-based research was conducted on pre-school children of rural kebeles in Farta district to determine the prevalence of Bitot’s spot, night blindness and associated factors.
Methods
Study Area
This study was conducted in rural kebeles (local name for sub-division of a district) of Farta district, which is one of the districts in the region of Amhara in Ethiopia. Therea total of 41 kebeles, 38 of which are rural. Part of the South Gondar Zone, Farta is bordered to the South by Este, to the West by Fogera, to the North by Ebenat and to the East by Lay-Gayint. Farta surrounds the town of Debre Tabor. Based on the 2007 national census conducted by the Central Statistical Agency (CSA), of Ethiopia, this district has a total population of 232,181, of whom 118,513 are males, and 113,668 are females; 6783 or 2.92% are urban inhabitants. With an area of 1099.25 square kilometers, Farta has a population density of 211.22, which is greater than the Zonal population density (145.56 persons per square kilometer). A total of 49,986 households were registered in this district, resulting in an average of 4.64 persons to a household. The majority of the inhabitants practiced Ethiopian Orthodox Christianity, with 99.61% reported it as their religion.
Study Design and Population
A community-based cross-sectional mixed quantitative and qualitative study was conducted from 1 January to15 February 2019. The population for the quantitative study included pre-school children (1–5 years) and mothers/caregivers living in randomly selected Farta rural kebeles included in the sample and presented at the data collection time. The populations for the qualitative study were mothers/caregivers living in the randomly selected rural kebeles, whose children had a clinical symptom of vitamin A deficiency.
Inclusion and Exclusion Criteria
Being a pre-school (1–5 years) children of Farta district and had a mother/caregiver at home at the time of first/second visit during the survey was considered as inclusion criteria. Children who had a problem of seeing during day time and who were already blind at the time of data collection will be excluded.
Sample Size and Sampling Techniques
The prevalence of Bitot’s spots in a study conducted on children in Ethiopia was reported to be 6.7%.15 Taking the margin of error as 3% and using a single population proportion formula, the final sample size was calculated. Then, 10% non-response was considered and multiplied by the design effect of 2, and a final sample size of 588 was determined. For the qualitative study or in-depth interview 10 key informants (mothers) were included. Since the total numbers of mothers having a child with VAD were 12, 84% of them were selected by considering information saturation. Multi-stage cluster sampling is a practical means of sampling the population at risk of VAD.3 In this study, a multi-stage cluster sampling technique was used to select the population of the study. The 38 rural kebeles in Farta district were stratified into high-land and middle-land. Three kebeles from the high-land and five kebeles from the middle-land were randomly included in the study. The calculated sample size was allocated to each kebele in proportion to, the total number of children obtained from the census in each selected kebele/cluster. The first household for the study was selected using a simple randomized technique, and every 12th household was visited. If there is now at least one child (with the age of 1–5 years), the adjacent household was visited. One randomly selected child from each household was examined in the case of more than one eligible pre-school child in the household (Figure 1).
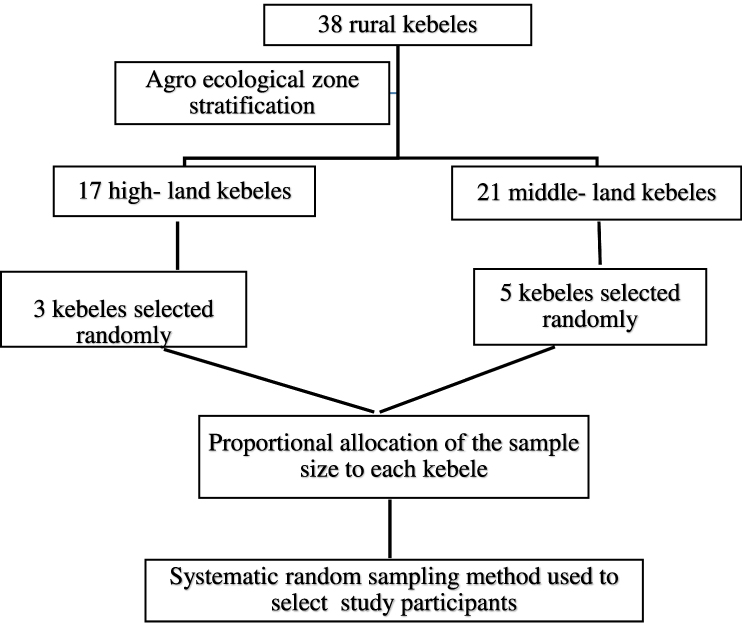 |
Figure 1 Schematic presentation of sampling technique for assessment of prevalence of clinical vitamin A deficiency and associated factors among pre-school children in rural kebeles of Farta district, South Gondar zone, Ethiopia. |
Data Collection
Data for the clinical examination were collected by the data collectors (ophthalmic nurses), preferably by daylight screening of the Bitot’s spots, with the use of a magnifying loop and torches. The data about the history of child night blindness have been taken from the interview of mothers or immediate caregivers. The first four questions of the WHO algorithm3 for the assessment of night blindness were enquired from mothers of pre-school children. All participants who complained that they had of having a problem seeing at low light level but had no problem seeing during the day and who were different from most other children in their community were considered to have night blindness. Information on age, sex, ethnicity, history of breastfeeding and information on maternal education, marital status and occupation was collected by interviewer-administered standard pre-tested questionnaire adapted from the National Nutritional Survey in Ethiopia. Data for the qualitative study were collected from a key informant interview with mothers/caregivers whose child has a clinical VAD. The key informant interview was recorded in a tape recorder and transcribed and written to notebooks every day after the interview.
Data Processing and Analysis
After the data collection process, the data were checked for completeness, consistency and clearance accordingly. Data were entered using Epi Data statistical software and analysed by using excel 2007 format and SPSS version 20 statistical software packages. Descriptive statistics have been computed to determine the prevalence of Bitot’s spot and night blindness and the percentage of Bitot’s spots and night blindness have been analyzed as per age group, gender and other variables. Bivariable logistic regression analysis was performed to investigate the associations of each independent variable with the occurrence of clinical VAD. Multivariable logistic regression analysis was done for a P value of <0.20 to determine the independent predictors of the occurrence of clinical VAD. Adjusted Odds Ratio (AOR) with its confidence interval (CI), 95% was reported in each logistic regression analysis. P-value < 0.05 was considered as statistically significant. The data collected from qualitative methods using key informant interviews with open-ended questions were organized by the question, coded and transcribed after analyzing how all key informants replied to each question. Four thematic areas were chosen to categorize the responses of key informants. These are steps taken to avoid and treat VAD, information and awareness about vitamin A, food and sanitation practices and agricultural practices. Selected quotations were used in the study to demonstrate the significance of the term.
Results
A total of 581 children (1–5 years of age) with corresponding mothers/caregivers participated in the study, making a response rate of 98.8%. Of the participants, 396 (68.2%) and 185 (31.8%) live in high-land and middle-land agro-ecological zone, respectively. The majority of study subjects were Orthodox Christians 572 (98.5%) and Amhara in ethnicity 578 (99.48%). In addition, 512 (88.1%) of the mothers/caregivers were married, and 488 (84%) were housewives. Regarding the income status, 367 (63.2%) families earn less than 16.7 USD per month. Concerning mothers/caregivers characteristics, 435 (74.9%) had no formal education, and 365 (62.8%) had 1–4 children, 468 (80.6%) had an experience of taking additional food (extra food they consumed in addition to what they usually consume during in state of non-pregnancy and non-lactation) during pregnancy and lactation (Table 1).
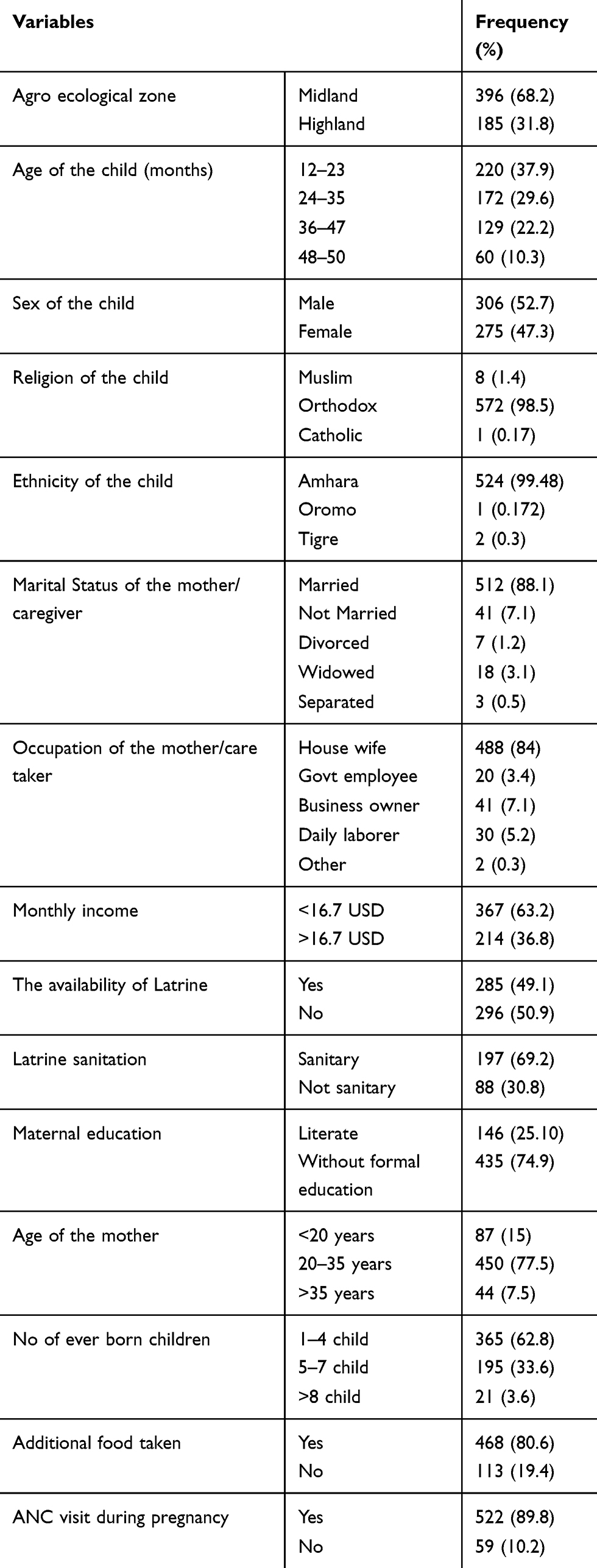 |
Table 1 Socio-Economic and Demographic Characteristics of the Study Participants in Rural Kebeles of Farta District, South Gondar Zone, Ethiopia, 2019 (n=581) |
Feeding and Dietary Characteristics of the Participants
Breastfeeding data and complementary feeding practices were collected for children below the age of 3 years. All the mothers (392) of these children reported that they had breastfeeding practice, but only 198 (50.5%) of the mothers had started breastfeeding immediately (within an hour) after delivery. Regarding the frequency of breastfeeding, 90 (23%) feed <8 times per day, while 302 (77%) breastfeed more than eight and above times a day. Furthermore, 210 (53.6%) of mothers have been breastfeeding for more than 6 months without introducing complementary food, while 162 (41.3%) have practiced exclusive breastfeeding for 6 months and started complementary food exactly at the age of 6 months. During illness 323 (82.4%) of respondents change the feeding practice of their child and among the changes, 249 (77.1%) changed by providing additional food (Table 2). It was found that all study participant children received vitamin A supplementation. With respect to dietary patterns, intake of vitamin A rich foods were assessed, and 293 (50.4%) of children usually eat dark green vegetables less than three times per week. About 397 (68.4%) of the mothers/caregivers know less than five food items rich in vitamin A.
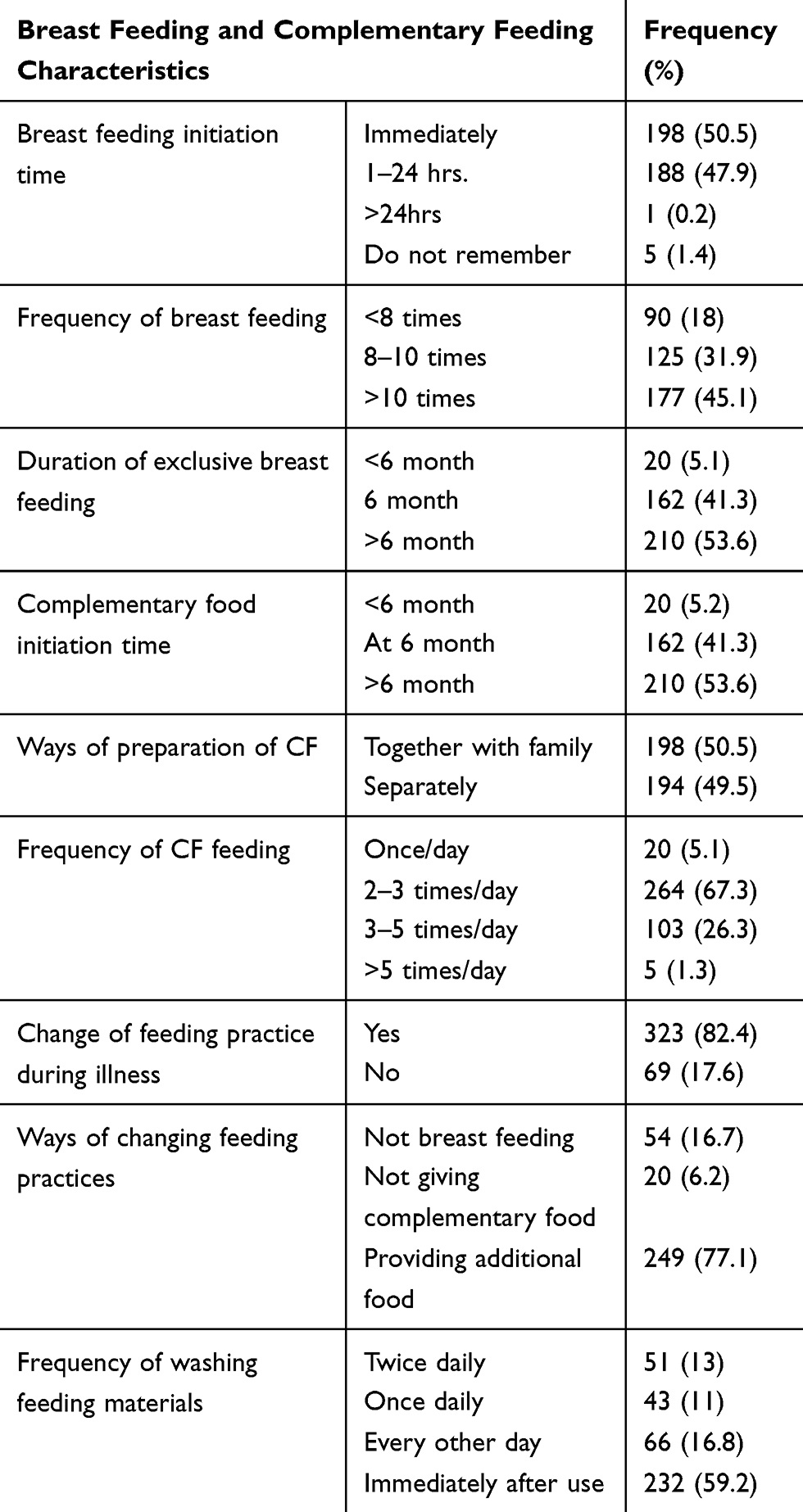 |
Table 2 Breast Feeding and Complementary Feeding Characteristics of Participants Below Three Years (n=392), in Rural Kebeles of Farta District, South Gondar Zone, Ethiopia, 2019 |
The Prevalence of Clinical Vitamin A Deficiency
The overall prevalence of clinical vitamin A deficiency was 2.0%, while the prevalence of night blindness, the earliest symptom of VAD, was 1.2% and the prevalence of Bitot’s spot, the objective indicator of VAD, was 0.8% (Table 3).
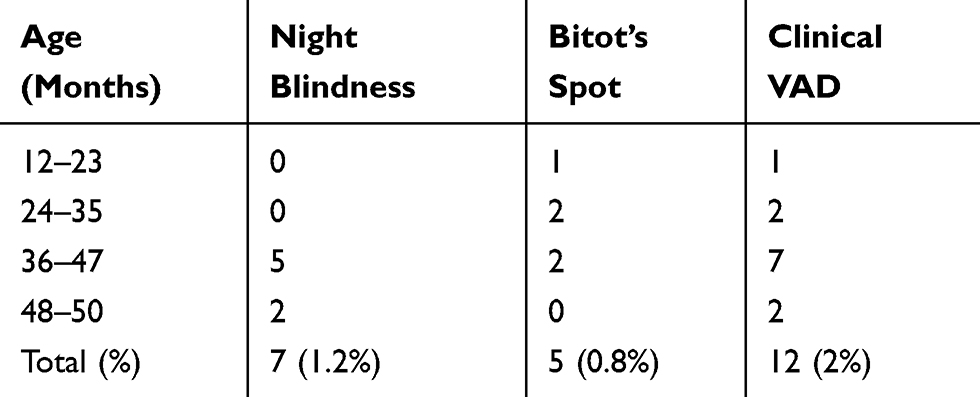 |
Table 3 The Prevalence of Clinical Vitamin a Deficiency Across Different Age Groups of Pre-School Children in Rural Kebeles of Farta District, South Gondar Zone, Ethiopia, 2019 (n=581) |
Factors Related to Clinical Vitamin A Deficiency
During the bivariable analysis, living in the high-land agro-ecological zone, age of the child in months, and availability of latrine were associated with clinical vitamin A deficiency. From maternal factors not having ANC visit during pregnancy was related to a higher risk of VAD. The risk of child clinical VAD was also higher on those whose mothers/caregivers practice hand washing with water only (Table 4). The multivariable analysis was conducted to identify the predictors of vitamin A deficiency.
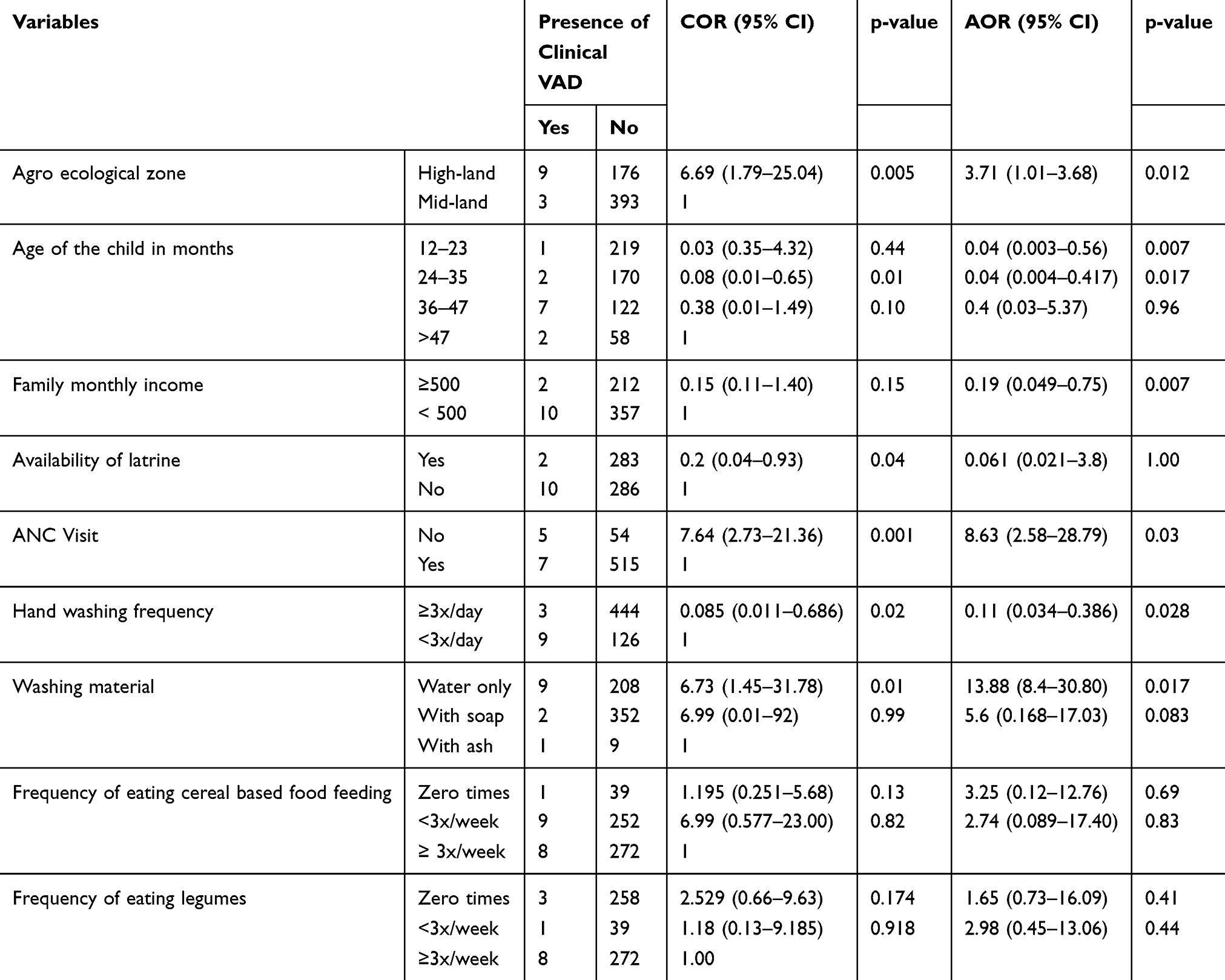 |
Table 4 Factors Associated with Clinical Vitamin a Deficiency Among Pre-School Children in Rural Kebeles of Farta District, South Gondar Zone, Ethiopia, 2019 |
In the multivariable analysis, it was found that children living in high-land were 3.71 times more likely to have clinical vitamin A deficiency as compared to children living in middle-land (AOR: 3.71; 95% CI: 1.01–13.68). Those children with a family monthly income of ≥16.7USD were 81% less likely to have clinical VAD as compared to those with a family monthly income of <500 birr (AOR: 0.19; 95% CI: 0.049–0.75). Besides, the odds of having clinical vitamin A deficient child is higher for those mothers who had no ANC visit (AOR: 8.63; 95% CI: 2.58–28.79).
A key informant interview was conducted with 10 key informants who were the mothers or caregivers of children with clinical vitamin A deficiency. Guiding questions have been grouped into four thematic areas, which include actions taken to prevent and treat vitamin A deficiency, information and awareness about vitamin A, feeding and sanitary practice and agricultural practice.
Concerning the action taken to prevent and treat vitamin A deficiency, half of the respondents said they were going to a health facility for treatment of vitamin A deficiency, and the rest used to go to traditional healers (“Awaki” in local language) and used traditional home treatments. For instance, a 31-year-old housewife said:
Night-blindness is a hereditary disease, and it is an evil spirit, and there is no solution to this issue. “So there is no solution by going to the health facility, and it is better to go to Awaki.
Some of the respondents also explained that there are traditional practices and herbal remedies that they give during sickness to children; for example, a 45-years-old woman who said: “I am going to make a rub on their body with wheat, which I am going to chew on their body to recover from measles”. Almost all mothers said that the availability of tracer drugs in the health post is not constant throughout the year. Regarding information and awareness about night blindness, most of the respondents had heard about vitamin A, and those who were aware of it had received information from health extension workers. Most of the key informants replied that their children were on monotonous dietary characteristics, and few use a variety of foods. Few of the key informants use water treatment methods at home concerning sanitary issues. Since most areas have water scarcity, hand washing practices, personal hygiene and other sanitary activities are kept irregularly. For example, a 40-years-old woman said
I usually fetch water from a distance of 45minutes, and I have six kids at home, so I only use this water for cooking. If I have to wash their clothes, I have to do it on holidays.
Hence, the observation from the respondents reveals that there is a gap in awareness of VAD and sanitation practices.
Discussions
In the present study, a quantitative and qualitative cross-sectional study was conducted to determine the prevalence of clinical VAD and associated factors of pre-school children in Farta district. The prevalence of clinical vitamin A deficiency measured by both Bitot’s spots and night blindness in the present study was determined to be (2%). The magnitude of Bitot’s spots (0.8%) reported by this study was above the WHO threshold (>0.5%) for classifying VAD as a serious public health problem. Similarly, the magnitude of night blindness was found to be 1.2%, which was above the WHO threshold (>1%).3
This finding suggested that clinical vitamin A deficiency is an issue of public health importance with the problem ranged from mild to moderate. According to the 2010 EHNRI report, the overall prevalence of Bitot’s spots and night blindness in Ethiopia was 1.7% and 0.8%, respectively.2 Specifically for the Amhara regional state, the prevalence was 3.2% for Bitot’s spots and 1% for night blindness, respectively. Thus, the prevalence of Bitot’s spots in this study was found to be half of the national prevalence and one-quarter of the regional prevalence. The prevalence of night blindness in this study was documented to be higher than both the national and regional figures. But it was still lower than that of the studies conducted in Arsi by Aserat et al, in 2002 (Bitot’s spots = 2.2%, night blindness = 7.2%) and Northern Showa by Aweke et al, in 2012 (Bitot’s spots = 3.5%, night blindness= 3.1%).8,16 The variation might be because of the time gap that the studies were conducted during which the government were doing health promotion activities.
From this study living in the high-land climatic zone is one risk factor for clinical VAD; highlanders were 3.71 times more likely to have the deficiency (AOR: 3.71, 95% CI: 1.01–13.68). Inadequacy in intake of protective foods such as green leafy vegetables might be the cause for it since the type of produced foods varies among climatic zones. The effect of climate on VAD was evidenced by a community-based cross-sectional study that was carried out in six drought-affected areas of India in 2003 which showed that the prevalence of Bitot’s spots was significantly higher in dry areas (AOR: 2.0; 95% CI: 1.6–2.7).4 The variation may be attributed to the type of plants and crops cultivated in the area. This can be compounded by the statement from the key informant interview, where almost all highlanders cultivate potatoes and wheat, and their need for vegetables and staple food is by purchasing from town. For Instance “A 37-year-old housewife living in highland said that she had to go to town to buy vegetables for household consumption, which is 20 birr for a single trip”.
This study shows that there is no significant difference in the prevalence estimation of clinical VAD by gender. This might be due to the absence of gender discrimination with regard to feeding and caring for pre-school children. This is similar to the study conducted by Kurugöl et al, (2000), Nana et al, (2005), and Paracha et al, (2000)17–19 However, it was found against the study conducted in India, which found a higher risk of vitamin A deficiency among male children.
As it can be seen from multi-variable regression analysis, children aged 12–23 months were 96% less likely to have clinical VAD compared to children of age higher than 47 months. A similar finding was observed in a study conducted in India where children aged 3–5 years had a higher risk of VAD (OR: 7.23; 95% CI: 3.78–13.82) as compared to younger correspondents.4 In another study by Arlappa et al, (2011) children of 3–5 years were at higher risk again (OR: 1.4; 95% CI: 1.0–2.0).1,20 The higher prevalence of VAD observed in this age group reflects the cumulative effect of inadequate dietary intake and non-coverage of above 3-year-old children for vitamin A supplementation.
Factors like maternal education (literacy), occupation and family size did not show significant association at 20% of significance level during bivariable analysis. Similarly, these factors did not have any bearing on the prevalence of VAD in the study which assessed the prevalence of clinical and sub-clinical vitamin A deficiency among rural pre-school children of West Bengal, India.1 But a study conducted by Laxmaiah et al, (2012) indicated that the risk was significantly higher among children of laborers (OR:52.9; 95% CI: 2.1–3.9) compared to other occupations and the odds of having Bitot’s spots was also significantly higher among the children of illiterate mothers (OR: 2.7; 95% CI: 2.2 −3.3).21 Lack of significant association in the current study might be because, most of the study participant mothers were housewives and illiterates 488 (84%),435 (74.9%), respectively.
Regarding the consumption of vitamin A rich foods, the majority of the study subjects have a habit of consuming dark green vegetables less than three times a week, which can be taken as a cause for VAD. The most important staple food consumed was white potato, which is virtually devoid of yellow carotenoid pigment, which serves as a source of pro-vitamin A.22 For instance, a 45 years old house-wife said that in the locality “injera” is the most delicious staple foods made of wheat, barley or teff that we eat on a daily basis for our children and us”. Thus, a staple food that is being consumed by most children daily may lead to monotonous dietary character. This was explained in studies conducted in Burkina Faso in 2004 which assessed the consumption of vitamin A rich foods by pre-school children in VAD community; it found that the general picture of the food consumption patterns is a monotonous cereal-based diet.18 Similarly, a study conducted by Tsegaye et al, (2010) assessed the magnitude of vitamin A in Ethiopia. It stated that the observed high prevalence of morbidity, inadequate consumption of fruits and vegetables, and the monotonous cereal-legume diet are the likely factors that may have exacerbated vitamin A deficiency in various regions.2
Different studies revealed that ANC visit of mothers was associated with low risk of VAD. Similar to the study conducted by Aweke et al (2012),16 the current study found that the odds of having VAD was higher for those mothers who had no ANC visit compared to those mothers who had to follow up (AOR: 8.63; 95% CI: 2.58–28.79). This might be due to the information they receive during the visiting time. For instance, in the key informant interview, a 33 years old housewife said: “I heard about vitamin A deficiency problems and food sources of vitamin A while I was attending ANC follow up in the health post”.
Income was also found to be one determinant factor of clinical vitamin A deficiency. Thus, the odds of having the deficiency was lower in the higher income level (≥16.7USD) with (AOR: 0.19; 95% CI: 0.049–0.75). This may be due to the ability to purchase vitamin A rich foods. Similarly, the study conducted in China indicated that living in a poor western area or a mother with low income has a high risk of VAD.23
Conclusions
The results presented here demonstrate the prevalence of Bitot’s spots and night blindness were above the WHO threshold. The study also revealed that income (<16.7USD), agro-ecological zone (living in high-land), hand washing material (washing with water only) and not having ANC visit are associated with clinical vitamin A deficiency. In conclusion, clinical vitamin A deficiency rates of the study area showed that VAD is of public health concern because the prevalence of night blindness and Bitot’s spots were above the WHO level. Accordingly, effective preventive measures should be designed to reduce VAD prevalence.
Future Direction of This Study
Health extension workers should continuously educate the community about night blindness, Bitot’s, the causes, the prevention and other issues. There should be community-based education to increase the awareness and knowledge about vitamin A and the deficiencies, consumption of diversified diets. Further studies are recommended to assess the subclinical vitamin A status of the children in the area.
Limitation of the Study
Children who had a problem of seeing during day time and those who were blind at the time of data collection were excluded. Therefore, this study could not detect the VAD of this segment of the population.
Abbreviations
EBF, Exclusive Breast Feeding; EHNRI, Ethiopian Health and Nutrition Research Institute; EPI Info, Epidemiological Information; FMOH, Federal Ministry of Health; HH, House Hold; IVACG, International Vitamin A Consultative Group; NNHBI, National Nutrition and Health Bureau of India; SPSS, Statistical Package for Social Sciences; UNICEF, United Nations International Children Emergency Fund; VA, Vitamin A; VAD, Vitamin A deficiency; WHO, World Health Organization.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on a reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The ethical approval and clearance for this study have been obtained from Debre Tabor University College of Health Sciences Institutional Research Ethics Review Committee (IRERC) with the reference number of DTU/re/85/91/2019. At all levels, officials were contacted with a formal letter obtained from the IRERC to secure permission. A permission letter has been submitted to South Gondar Zonal Health Bureau, Farta district administrative health office, and district Health Offices and Kebeles involved in the study. Informed written signed consent has been obtained from mothers of the children or their caregivers, including publication of anonymized response following the explanation about the purpose of the clinical examination. Then, at the end of clinical examination and administering the questioner health education about VAD, consumption of vitamin A rich foods has been given in general and in particular for those who has been presented with VAD symptoms has been linked with the kebele health extension workers for supplementation of a standard dose of vitamin A capsule. The key informant interview with the mothers/caregivers of children with Bitot’s spots or night blindness has been held in a separate area in one-to-one interviews.
Consent to Publish
All the authors have agreed and gave consent for the publication.
Acknowledgment
Our thanks goes to all staff members of the South Gondar zonal Health Bureau and Farta district health office staff members for providing us with valuable information.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The author (s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Rishah Elmneh is an employee of Julphar Pharmaceuticals plc. The authors report no other potential conflicts of interest for this work.
References
1. Arlappa N, Balakrishna LA, Harikumar N, Brahmam R. Clinical and sub- clinical vitamin A deficiency among rural pre-school children of Maharashtra, India. Ann Hum Biol. 2010;37(2):282. doi:10.3109/03014460902991979
2. TsegayeD.T, AliA, MekonenY, HaiderJ, UmetaM. Magnitude and distribution of vitamin A deficiency in Ethiopia. Food Nutr Bull. 2010;31(2):234– 241. doi:10.1177/156482651003100206
3. WHO.Indicators for Assessing Vitamin A Deficiency and Their Application in Monitoring and Evaluating Intervention Programs. World Health Organization. 2009.
4. Arlappa N, Venkaiah K, Brahmam GN. Institute of nutrition severe drought and the vitamin A status of rural pre-school children in India. Indian J Med Res. 2008;35:577–586.
5. Global database on Vitamin A deficiency [Internet]. 2009.
6. John.B.Mason, Mahshid Lofti, Nita Dalmiya, Kavita Sethuraman, Scott Geibel, Kari Gillenwater, Karen Mason and Nancy Mock. World Micro Nutrient Report on Current Progress and Trends in the Control of Vitamin A, Lodine, and Iron Deficiencies, [Internet]. World Micronutrient Initiative; UNICEF.2001.
7. WHO.. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency. World Health Organization.2009.
8. Aserat Y, Omwenga A, Muita J. Prevalence of vitamin A deficiency among pre-school and school aged children in Arssi zone, Ethiopia. East Afr Med J. 2002;79(7):355–359. doi:10.4314/eamj.v79i7.8838
9. Sahile Z, Yilma D, Tezera R, et al. Prevalence of vitamin A deficiency among pre-school children in Ethiopia: a systematic review and meta-analysis. Biomed Res Int. 2020;2020:8032894. doi:10.1155/2020/8032894
10. Tadesse L, Shawel D, Kidanu Y, Meskel GG, Yifter H, Mulugeta A. Module of Vitamin A Deficiency for the Ethiopian Health Center Team. EPHTI and USAID.2005.
11. WH O. Vitamin and Mineral Requirements in Human Nutrition. World Health Organization; 2004.
12. Ezzati M, Lopez AD, Rodgers A, Murray CJ. Comparative quantification of health risks. In: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. Geneva: World Health Organization;Editors;Eileen Brown and James Akre.2004:1987–1997.
13. Ansstas G, Hakore J, Gopalswamy N. Vitamin A deficiency. 2014. Available from: http://emedicine medscape com/article/126004-overview.
14. Labonté R, Schrecker T, Packer C, Runnels V. Globalization and Health: Pathways, Evidence and Policy. Routledge; 2009.
15. Wolde-Gebriel Z, Gebru H, Fisseha T, West C. Severe vitamin A deficiency in a rural village in the Hararge region of Ethiopia. Eur J Clin Nutr. 1993;47(2):104–114.
16. Aweke K, Habtamu F, Akalu G. Nutritional status of children in food insecure households in two districts of North Showa Zone, Ethiopia. African J. Food, Agric. Nutr. Dev. 2012;12(2):5915–5927.
17. Kurugöl Z, Egemen A, Keskinoğlu P, Darcan S, Akşit S. Vitamin A deficiency in healthy children aged 6–59 months in Izmir Province of Turkey. Paediatr Perinat Epidemiol. 2000;14(1):64. doi:10.1046/j.1365-3016.2000.00229.x
18. Nana CP, Brouwer ID, Zagré N-M, Kok FJ, Traoré AS. Community assessment of availability, consumption, and cultural acceptability of food sources of (pro) vitamin A: toward the development of a dietary intervention among pre-school children in rural Burkina Faso. Food Nutr Bull. 2005;26(4):356–365. doi:10.1177/156482650502600405
19. Paracha PI, Jamil A, Northrop-Clewes CA, Thurnham DI. Interpretation of vitamin A status in apparently healthy Pakistani children by using markers of subclinical infection. Am J Clin Nutr. 2000;72(5):1164–1169. doi:10.1093/ajcn/72.5.1164
20. Arlappa N, Balakrishna N, Laxmaiah AP, et al. Prevalence of vitamin A deficiency and its determinants among the rural pre-school children of Madhya Pradesh, India. Ann Hum Biol. 2011;38(2):131–136. doi:10.3109/03014460.2010.498794
21. Laxmaiah A, Nair MK, Arlappa N, et al. Prevalence of ocular signs and subclinical vitamin A deficiency and its determinants among rural pre-school children in India. Public Health Nutr. 2012;15(4):568–577. doi:10.1017/S136898001100214X
22. Sachdeva S, Alam S, Beig FK, Khan Z, Khalique N. Determinants of vitamin A deficiency amongst children in Aligarh district, Uttar Pradesh. Indian Pediatr. 2011;48(11):861–866. doi:10.1007/s13312-011-0140-8
23. Jingxiong J, Toschke AM, von Kries R, Koletzko B, Liangming L. Vitamin A status among children in China. Public Health Nutr. 2006;9(8):955–960. doi:10.1017/PHN2006944
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.