Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence and Antimicrobial Sensitivity Patterns of Uropathogens, in Tikur Anbessa Specialized Hospital Emergency Medicine Department Addis Ababa, Ethiopia
Authors Firissa YB ![]() , Shelton D, Azazh A, Engida H
, Shelton D, Azazh A, Engida H ![]() , Kifle F, Debebe F
, Kifle F, Debebe F
Received 25 January 2023
Accepted for publication 16 March 2023
Published 23 March 2023 Volume 2023:16 Pages 1649—1656
DOI https://doi.org/10.2147/IDR.S402472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Yared Boru Firissa,1 Dominick Shelton,2 Aklilu Azazh,3 Hywet Engida,3 Fitsum Kifle,4 Finot Debebe3
1Emergency Medicine and Critical Care Department, ALERT Hospital, Addis Ababa, Ethiopia; 2Emergency Medicine Department, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada; 3Emergency Medicine and Critical Care Department, Tikur Anbessa Hospital, Addis Ababa, Ethiopia; 4Network for Perioperative and Critical Care, Addis Ababa, Ethiopia
Correspondence: Yared Boru Firissa, Department of Emergency Medicine and Critical Care, ALERT Hospital, Addis Ababa, 165, Ethiopia, Email [email protected]
Background: Empirical treatment of infections remains a major contributing factor to the emergence of pathogens that are resistant to antibiotics. The study aimed to assess the prevalence and anti-microbial sensitivity patterns of uropathogens in the Emergency Medicine Department of Tikur Anbessa Hospital, Ethiopia.
Methods: Urine sample data collected over two years from January 2015 to January 2016 at Tikur Anbessa Hospital’s laboratory were retrospectively analyzed for bacterial pathogens, and their antimicrobial susceptibility. Antimicrobial sensitivity tests were done using the disc diffusion technique as per the standard of the Kirby-Bauer method.
Results: Of the total 220 samples that were collected, 50 (22.7%) were culture-positive. Male to female data ratio was 1:1.1. Escherichia coli was the dominant isolate (50%) followed by Enterococcus species (12%), Enterobacter species (12%), and Klebsiella species (8%). Overall resistance rates to Cotrimoxazole, Ampicillin, Augmentin, and Ceftriaxone were 90.4%, 88.8%, 82.5%, and 79.3%, respectively. The sensitivity rates for Chloramphenicol, Amikacin, Vancomycin, Meropenem, Cefoxitin, and Nitrofurantoin ranged from 72% to 100%. The antibiogram of isolates showed that 43 (86%) isolates were resistant to two or more antimicrobials, and 49 (98%) were resistant to at least one antibiotic.
Conclusion and Recommendation: Urinary tract infections are mostly caused by Gram-negative bacteria predominantly in females and Escherichia coli are the most common isolates. Resistance rates to Cotrimoxazole, Ampicillin, Augmentin, and Ceftriaxone were high. Chloramphenicol, Amikacin, Vancomycin, Meropenem, Cefoxitin, and Nitrofurantoin are considered appropriate antimicrobials for the empirical treatment of complicated urinary tract infections in the emergency department. Yet, using antibiotics indiscriminately for patients with complicated UTIs may increase the resistance rate and also lead to treatment failure, hence the prescriptions should be revised following the culture and sensitivity results.
Keywords: uropathogens, culture, emergency, Ethiopia
Background
Urinary tract infections (UTIs) are one of the most common types of bacterial infections in humans, occurring both in the community and in healthcare settings. UTI refers to a wide range of clinical conditions, from the asymptomatic presence of bacteria in the urine to severe kidney infection with subsequent sepsis.1
Females are more prone to UTIs than males, a phenomenon explained by their short urethra and its anatomical proximity to the anal orifice.2,3 Uropathogens are simple to identify as they mainly come from colonic flora,4 and this serves as a rationale for the empirical treatment of community acquired UTI (CA-UTI).2,5 Empirical treatment, on the other hand, limits the ability to monitor antibiotic response and predisposes uropathogens that cause UTI to resistance.5,6 Despite their use as practical methods for efficient resource use, empirical management plans must be regularly updated to account for shifting pathogen susceptibility patterns.6 This is particularly true for developing nations, where the lack of resources for routine antibiotic sensitivity test compounds an additional challenge.6
In recent years, the resistance of uropathogens to previously effective antibiotics has become a global phenomenon.7–9 Antimicrobial resistance (AMR) is currently estimated to account for more than 700,000 deaths per year worldwide.10 If no appropriate measures are taken to halt its progress, it is projected to cost approximately 10 million lives and about US$100 trillion per year by 2050.10 In contrast to other health issues, Anti-microbial Resistance (AMR) is a problem that concerns every country, irrespective of its level of income and development. According to the WHO report from 2014, Africa and South-East Asia are the regions with no established AMR surveillance systems.11
The lack of quality data is challenging, resulting in inadequate treatment guidelines for the local situation. The gap in public health capacity is also an issue given the rapidly evolving resistance mechanisms of the pathogens and the emergence of multidrug-resistant bacteria that can only be detected through systematic screening in quality-assured microbiology laboratories.12,13 Given the widespread irrational use of antibiotics in Africa, the situation is dire9,11 as compared to developed nations.
To design suitable interventions, it is important to understand the status of AMR and identify rollout gaps. The most recent version of the national Ethiopian treatment guideline recommends using Trimethoprim/Sulfamethoxazole (TMP-SMX) and Norfloxacin for the empirical treatment of CA-UTI in Ethiopia, one of the second-most populous regions of Africa.14 However, we believe that there might be significant antibiotic resistance to the recommended treatments, and as a result, the likelihood of treatment failure is rising with the continued empirical use of these medications. As such, the study aimed to assess antibiotic resistance to both the suggested treatments and other drugs, as well as to identify patterns of resistance to a wide range of potentially helpful alternatives for the treatment of UTIs in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia.
Methods
This study was conducted at Tikur Anbessa Specialized Hospital. It is the largest referral and tertiary-level teaching hospital in Ethiopia, located in the heart of Addis Ababa, the capital city.15 The hospital is administered by Addis Ababa University and is the largest tertiary unit and the oldest teaching hospital in Ethiopia, with over 800 beds. It provides teaching for about 300 medical students and 350 residents every year and has more than 800 beds.15 It offers diagnosis and treatment for approximately 370,000–400,000 patients a year.15 The hospital’s laboratory is one of the biggest and most advanced award-winning laboratories, providing services like culture and sensitivity, gram stain, blood chemistry, complete blood count (CBC), GeneXpert, and acid-fast bacillus (AFB) for the diagnosis of tuberculosis (TB). The hospital is also known for its multidisciplinary collaborative research with both local and international universities.
After receiving ethical approval from Addis Ababa University and a letter of support from the department of emergency medicine and critical care, a retrospective two-year record review was carried out on all UTI patients older than 14 years for whom culture and sensitivity tests were performed in the study. This review covered the period from January 2015 to December 2016. The data was retrieved and recorded in a data extraction sheet from the laboratory logbook, which contains patient age, sex, date of collection, department, isolated bacteria, and an antimicrobial susceptibility profile. The data were collected by nurses trained for this purpose. Data were cleaned, coded, and analyzed using the SPSS software program, version 21.0.
A sample taken from centrifuged urine and the sediment is evaluated for the proportion of polymorph nuclear cells (leukocytes), as >10/HPF is indicative of the presence of pathogenic bacteria. A urine sample containing less than 5 PMN cells/HPF was not cultured. The specimen is inoculated onto CLED, blood agar base, and MacConkey agar. MacConkey is to selectively grow gram-negative bacteria by discriminating between gram positives and differentiating between lactose fermenting and non-lactose fermenting gram-negative bacteria. Blood agar is a basic medium that can support both Gram-negative and Gram-positive bacteria, allowing us to cultivate a pure colony for further identification and DST testing. Colonies with a significant number (105 CFU/mL) from CLED Agar were subjected to Gram staining. Antimicrobial sensitivity tests were done using the disc diffusion technique as per the standard of the Kirby-Bauer method, and CLSI criteria were used for break point.
Results
Sociodemographic Information
From January 2015 to December 2016, a total of 220 urine samples were collected and analyzed. The age of the patients ranged from 14 to 100 years, with a mean age of 32.26 (SD = 14.45) years. The mean ages of male and female patients were 35.1 (SD = 15.8) and 30.78 (SD = 12.4) years, respectively. One hundred nineteen (54%) urine samples were from females, and 101 (46%) were from male patients, with a male-to-female ratio of 1:1.17 as shown in Table 1.
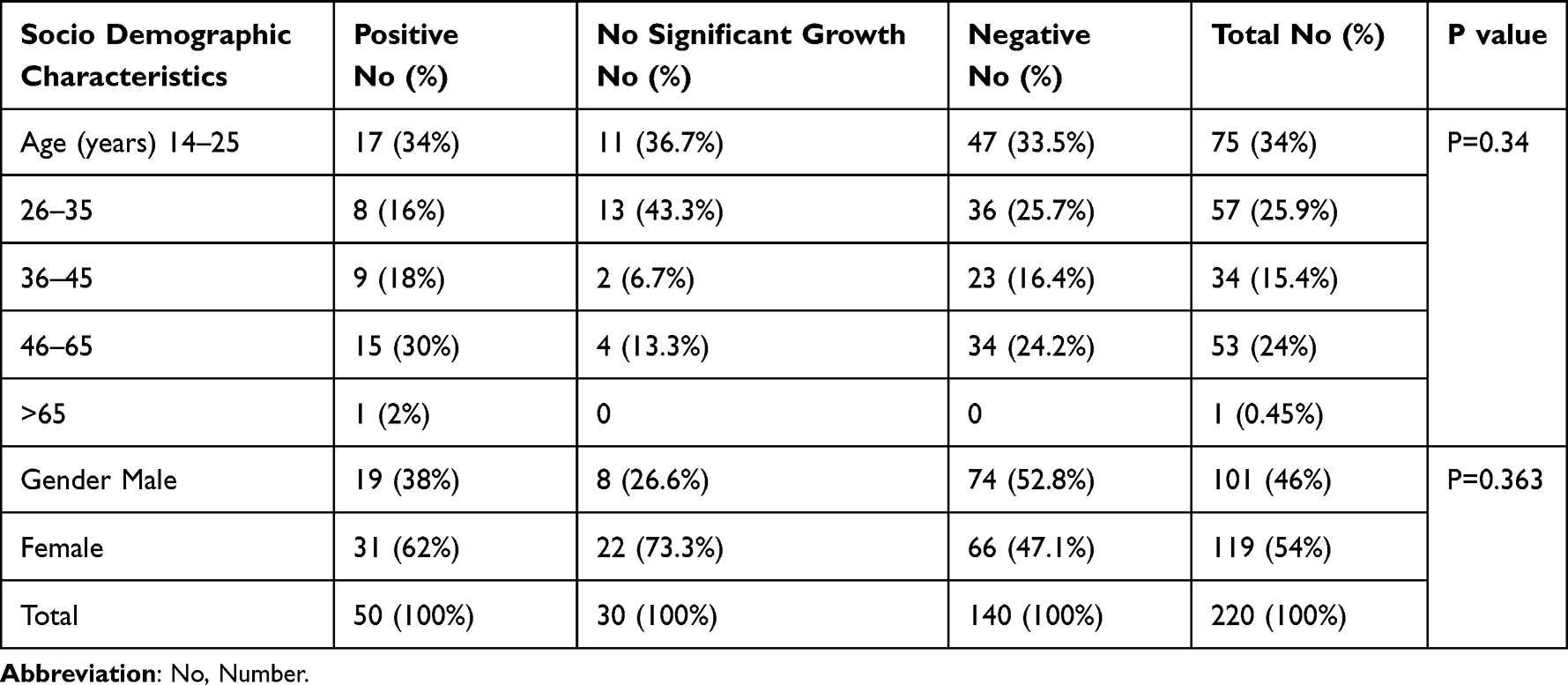 |
Table 1 Age and Sex Distribution of Patients with Urine Culture and Sensitivity, Tikur Anbessa Specialized Hospital Emergency Department from Jan 1 2015 to Dec 30 2016, Addis Ababa Ethiopia |
Prevalence of Uropathogens
The overall prevalence of uropathogens was 22.7%. The majority of the pathogens (14%) were isolated from females. Most of the uropathogens were isolated from patients in the age range of 14 to 25 years (Table 1). E. coli was the most predominant pathogen (50%) isolated from urine samples (Figure 1). The gram-negative and gram-positive bacteria were responsible for 84% and 16% of the isolates, respectively.
 |
Figure 1 Bacterial isolates of patients who have urine culture and sensitivity done, Tikur Anbessa Specialized Hospital emergency department from Jan 1, 2015 to Dec 30, 2016. |
Antibiotic Susceptibility Pattern of Uropathogens
The overall antibiotic susceptibility profiles of bacterial isolates are shown in Table 2. When the number of bacteria tested for specific antibiotics is observed, the resistance rate shows that resistance to Cotrimoxazole was the highest, with an overall resistance rate of (90.4%), followed by Ampicillin (88.8%), Augmentin (82.5%), and Ceftriaxone (79.3%). The antibiotics meropenem, amikacin, vancomycin, and cefoxitin were all found to be susceptible (Table 3). Because of the non-sustained availability of those antibiotics for which all tested etiologies are sensitive, only a few organisms were tested. Klebsiella species are dominant in male patients and almost resistant to all antibiotics, which shows the risk of having a resistant strain is higher in male patients. Species specific antimicrobial resistance rates are displayed in Table 3. E. coli showed high resistance rates to Cotrimoxazole (85.7%), Ampicillin (76.9%), and Augmentin (71.4%). The other three most common isolates exhibited resistance patterns of (80–100%) to Ampicillin, Cotrimoxazole, and Augmentin.
 |
Table 2 Overall Antimicrobial Susceptibility Profiles of Urine Samples from Patients Who Have Urine Culture and Sensitivity Done, Tikur Anbessa Specialized Hospital Emergency Department from, Jan 1 2015 to Dec 30 2016, Addis Ababa Ethiopia |
 |
Table 3 Overall Proportion of the Isolates’ Resistant to All Tested Antimicrobials, Tikur Anbessa Emergency Department from, Jan 1 2015 to Dec 30 2016, Addis Ababa, Ethiopia |
With no resistance rate, all (100%) E. coli isolates were susceptible to Vancomycin, Meropenem, Amikacin, and Cefoxitin. The other three common isolates were sensitive to Nitrofurantoin, Cefoxitin, Amikacin, and Vancomycin with resistance rates of 0%–17%.
Multidrug Resistance Pattern of Uropathogens
In this study, the overall resistance pattern of isolated uropathogens to more than one antimicrobial was 86%, and only 1 (2%) isolate was sensitive to all antimicrobials for which sensitivity was checked. The antimicrobial resistance rates of common isolates to more than one antibiotic were 80% (E. coli), 83.3% (Enterococcus), 100% (Enterobacter), and 100% (Klebsiella) (Table 4).
 |
Table 4 Multi Drug Resistance Pattern of Isolates of Urine Culture, Tikur Anbessa Specialized Hospital Emergency Department from Jan 1 2015 to Dec 30 2016, Addis Ababa Ethiopia |
Discussion
While urinary tract infections remain one of the most common disease patterns diagnosed worldwide, the management of these infections has become challenging due to the ever-rising emergence of antimicrobial drug resistance. The overall isolation rate of uropathogens in this study was found to be 22.7%, which is slightly lower than the rates reported from previous research conducted at this hospital.17 However, the rate was similar to that of Adugna et al.18 In this study, E. coli was the most predominant bacterium isolated from urine, followed by Enterobacter spp., Enterococcus spp., and Klebsiella spp. The isolation rates of E. coli, which is the most common isolate, and other pathogens in this study were comparable to the rates documented previously and also strongly agreed with similar research.8,13,16,19
Statistically, a significant difference was not observed between the two genders, though most pathogens were isolated from females (P = 0.34). Physiological and anatomical differences are accounted for by the differences between males and females. Females are more susceptible to infection than males, a phenomenon explained by their short urethra and its anatomical proximity to the anal orifice.3,4
This study showed that gram-negative bacteria were more frequent (84%) than gram-positive bacteria (16%). Similar findings have been reported by Tiruneh et al from Gondar, Ethiopia, and other studies done elsewhere.16,19–22 Bacterial uropathogenic isolates from patients with UTIs revealed the presence of extremely high levels of single and multiple antimicrobial resistance to commonly prescribed drugs.
The most frequently isolated bacterial isolates were found to be highly resistant to ciprofloxacin but sensitive to Nitrofurantoin. This result is different from the one documented previously in this hospital,17 in which the isolated organisms were highly sensitive to the aforementioned antimicrobials. Similar findings are reported by Gondar, including that bacterial isolates are highly resistant to CAPH.12,16
Enterococcus spp., Enterobacter spp., and Klebsiella spp. were found to be resistant to Ceftriaxone, Ceftazidime, Ciprofloxacin, Cotrimoxazole, Gentamicin, and Nalidixic Acid but sensitive to Nitrofurantoin, Vancomycin, and Cefoxitin. This finding is in contrast with a study done by Kibret et al,1 in which both gram-negative and gram-positive isolates are very sensitive to Gentamicin and Ciprofloxacin. Additionally, reports from a previous study done in the same hospital17 show that gram-negative isolates were mainly sensitive to Ciprofloxacin, Norfloxacin, and Nitrofurantoin, a finding that is also in contrast with ours. In this study, both gram-negative and gram-positive isolates were sensitive to Vancomycin at an equal rate, which may indicate Vancomycin is covering both gram-negative and gram-positive bacteria equally in this particular study, even though it is a drug of choice to cover gram-positive bacteria.
In our study, antibiotic susceptibility data revealed that virtually all isolates (98%) were resistant to at least one antibiotic, and most of the isolates (86%) were resistant to two or more antibiotics. These findings were extremely higher than the resistance rates that were observed in other studies,16,17 the reason for which might be the use of antibiotics and antimicrobial treatment prior to presentation to the hospital.
Conclusion and Recommendation
This study outlined that urinary tract infections are most commonly caused by Gram-negative bacteria, predominantly in females, E. coli is the most prevalent isolate, and the multidrug resistance of urinary tract infections was significantly high in the largest referral hospital in Ethiopia, Tikur Anbessa, with almost all bacteria tested for more than one drug resistance except for E. coli. Almost all bacterial isolates tested were resistant to Co-trimoxazole, Ampicillin, Augmentin, and Ceftriaxone. Most bacterial isolates were found to be sensitive to Vancomycin, Chloramphenicol, Amikacin, Meropenem, Cefoxitin, and Nitrofurantoin, indicating that these medications could be used as the first line of empirical treatment for complicated UTIs in emergency rooms. However, using antibiotics indiscriminately for patients with complicated UTIs may increase the resistance rate and lead to treatment failure, hence the prescriptions should be revised following the culture and sensitivity results.
Limitation
A limitation of this study can be understood in light of the following: Tikur Anbessa Hospital, as one of the largest tertiary units in the country, has a plethora of referral cases, the majority of which consist of debilitating comorbidities, like DM, malignancies, spinal cord injury, and septic shock, and not isolated UTO. This retrospective study is based on the results of routine microbiological tests carried out from 2015 through 2016, and so due to the nature of the retrospective analysis, tracing patients’ clinical settings was challenging and beyond the scope of the study. Additionally, the practice trends in the hospital are that culture and sensitivity tests are done for inpatients and not for those seeking outpatient care, which skews the caseload towards that of a complicated UTI. Moreover, the study was done in a single center, and the sample size is also limited, so it is difficult to generalize the finding to other hospitals; however, the finding helps as a foundation for future large-scale studies.
Declarations
All authors declare that this research is entirely our own, except where clearly stated otherwise, and that it has not been submitted in whole or in part to any previous research.
Data Sharing Statement
The article and its supporting files contain the datasets that support its conclusions. Any additional material can be obtained upon reasonable request.
Ethics Consideration
Ethical approval for the study has been sought and obtained from Addis Ababa University’s Ethical Review Board, and the need for individual level consent was waived as the study collects only lab results and de-identified patient information. All authors confirm that this study complies with the Declaration of Helsinki.
Consent to Publish
Informed consent was obtained from Tikur Anbessa Specialized Hospital Emergency Medicine Department and Laboratory Unit to Use secondary data recorded on the log book. Consent was not taken from the patients because we used secondary data and patients were not identified in information provided on a logbook.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Kibret M, Abera B. Prevalence and antibiogram of bacterial isolates from urinary tract infections at Dessie Health Research Laboratory, Ethiopia. Asian Pac J Trop Biomed. 2014;4(2):164–168. doi:10.1016/S2221-1691(14)60226-4
2. Hummers-Pradier E, Kochen MM. Urinary tract infections in adult general practice patients. Brit J Gen Pract. 2002;52:752–761.
3. McLaughlin SP, Carson CC. Urinary tract infections in women. Med Clin North Am. 2004;88:417–429. doi:10.1016/S0025-7125(03)00148-2
4. Yamamoto S, Tsukamoto T, Terai A, Kurazono H, Takeda Y, Yoshida O. Genetic evidence supporting the fecal-perineal-urethral hypothesis in cystitis caused by Escherichia coli. J Urol. 1997;157:1127–1129. doi:10.1016/S0022-5347(01)65154-1
5. Miller LG, Tang AW. Treatment of uncomplicated urinary tract infections in an era of increasing antibiotic resistance; a concise review for clinicians. Mayo Clin Proc. 2004;79:1048–1054. doi:10.4065/79.8.1048
6. WHO. Community-Based Surveillance of Antimicrobial Use and Resistance in ResourceConstrained Settings; Report on Five Pilot Projects. 20 Apia Avenue, 1211 Geneva, Switzerland: WHO Press; 2009.
7. Gupta K, Hooten TM, Stamm WE. Increasing antimicrobial resistance and the management of uncomplicated community-acquired urinary tract infections. Ann Int Med. 2001;135:41–50. doi:10.7326/0003-4819-135-1-200107030-00012
8. Schito GC, Naber KG, Botto H, Palou J, Mazzei T, Gualco L. The ARSEC study: an international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int J Antimicrob Agents. 2009;34(5):407–413. doi:10.1016/j.ijantimicag.2009.04.012
9. Okeke IN, Laxminarayan R, Bhutta ZA, et al. Antimicrobial resistance in developing countries. Part I: recent trends and current status. Lancet Infect Dis. 2005;5(8):481–493. doi:10.1016/S1473-3099(05)70189-4
10. UNEP - UN Environment Programme. Antimicrobial resistance: a global threat; 2023. Available from: https://www.unep.org/explore-topics/chemicals-waste/what-we-do/emerging-issues/antimicrobial-resistance-global-threat.
11. World Health Organization. Antimicrobial resistance global report on surveillance: 2014 summary. World Health Organization; 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/112647/WHO_HSE_PED_AIP_2014.2_eng.pdf.
12. Liu YY, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168. doi:10.1016/S1473-3099(15)00424-7
13. Xavier BB, Lammens C, Ruhal R, et al. Identification of a novel plasmid-mediated colistin-resistance gene, mcr-2, in Escherichia coli, Belgium, June 2016. Euro Surveill. 2016;21(27). doi:10.2807/1560-7917.ES.2016.21.27.30280
14. DACA. Standard treatment guideline for district hospital- Ethiopia. 2004:277.
15. Addis Ababa University College of health science, Background of Tikur Anbessa Hospital ; 2023. Available from: aau.edu.et/chs/tikur-anbessa-specialized-hospital/background-of-tikur-anbessa-hospital/.
16. Tiruneh M, Yifru S, Gizachew M, et al. Changing trends in prevalence and antibiotics resistance of uropathogens in patients attending the Gondar University Hospital, Northwest Ethiopia. Int J Bacteriol. 2014;2014:629424. doi:10.1155/2014/629424
17. Kabew G. A retrospective study on prevalence and antimicrobial susceptibility patterns of bacterial isolates from urinary tract infections in TikurAnbessa Specialized Teaching Hospital Addis Ababa, Ethiopia, 2011, Ethiopia. J Health Dev. 2013;27(2):111–117.
18. Adugna B, Sharew B, Jemal M. Bacterial profile, antimicrobial susceptibility pattern, and associated factors of community- and hospital-acquired urinary tract infection at Dessie Referral Hospital, Dessie, Northeast Ethiopia. Int J Microbiol. 2021;2021:5553356. doi:10.1155/2021/5553356
19. Beyene G, Tsegaye W. Wondewosentsegaye: bacterial uropathogens in urinary tract infection and antibiotic susceptibility pattern. Ethiop J Health Sci. 2011;21(2):141–146. doi:10.4314/ejhs.v21i2.69055
20. Ronald A. The etiology of urinary tract infection: traditional and emerging pathogens. Am J Med. 2002;113(Supl 1A):14S–19S. doi:10.1016/S0002-9343(02)01055-0
21. Alhumaid S, Al Mutair A, Al Alawi Z, et al. Antimicrobial susceptibility of gram-positive and gram-negative bacteria: a 5-year retrospective analysis at a multi-hospital healthcare system in Saudi Arabia. Ann Clin Microbiol Antimicrob. 2021;20(1):43. doi:10.1186/s12941-021-00450-x
22. Kasew D, Desalegn B, Aynalem M, et al. Antimicrobial resistance trend of bacterial uropathogens at the university of Gondar comprehensive specialized hospital, northwest Ethiopia: a 10 years’ retrospective study. PLoS One. 2022;17(4):e0266878. doi:10.1371/journal.pone.0266878
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.