Back to Journals » Clinical Ophthalmology » Volume 17
Preservative-Free versus Benzalkonium Chloride–Preserved Latanoprost Ophthalmic Solution in Patients with Primary Open-Angle Glaucoma or Ocular Hypertension: A Phase 3 US Clinical Trial
Authors Bacharach J, Ahmed IIK ![]() , Sharpe ED, Korenfeld MS
, Sharpe ED, Korenfeld MS ![]() , Zhang S, Baudouin C
, Zhang S, Baudouin C ![]()
Received 29 March 2023
Accepted for publication 18 August 2023
Published 1 September 2023 Volume 2023:17 Pages 2575—2588
DOI https://doi.org/10.2147/OPTH.S414015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jason Bacharach,1 Iqbal Ike K Ahmed,2 Elizabeth D Sharpe,3 Michael S Korenfeld,4 Steven Zhang,5 Christophe Baudouin6
1North Bay Eye Associates, Sonoma County, CA, USA; 2John Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 3Glaucoma Consultants and Center for Eye Research, Mt. Pleasant, SC, USA; 4Comprehensive Eye Care, Washington, MO, USA; 5Thea Pharma, Inc, Lexington, MA, USA; 6Quinze-Vingts National Ophthalmology Hospital & Vision Institute, Paris Saclay-Versailles-Saint Quentin University, IHU Foresight, Paris, France
Correspondence: Jason Bacharach, Email [email protected]
Purpose: To evaluate the safety and efficacy of a preservative-free latanoprost 0.005% formulation (T2345) in patients with primary open-angle glaucoma (POAG) or ocular hypertension (OHT) compared to benzalkonium chloride–preserved latanoprost 0.005% (BPL) formulation in the United States (US).
Patients and Methods: A prospective, randomized, multicenter, observer-masked, parallel-group study enrolled 335 patients diagnosed with POAG or OHT from 31 US sites who had adequately controlled intraocular pressure (IOP; ≤ 18 mm Hg) with latanoprost monotherapy. After a ≥ 72-hour washout period, patients were randomized to T2345 (n=165) or BPL (n=170) groups. Study drugs were dosed once-daily from Day 0 to Day 84 in one or both eyes. The study eye was the eye with lower IOP at baseline. The primary efficacy measure was the between-group comparison of the mean IOP values in the study eye at each time point (8 AM, 10 AM, and 4 PM on Days 15, 42, and 84). Safety measurements included ocular and systemic treatment-emergent adverse events (TEAEs).
Results: Both T2345 and BPL adequately controlled IOP with 95% CIs within 1.5 mm Hg in the study eye at all assessed time points. The percentages of patients with diurnal IOP < 18 mm Hg at Day 84 were 73.1% vs 78.7% for the T2345 and BPL groups, respectively. Adverse events were generally mild-to-moderate and primarily ocular. Fewer patients in the T2345 group experienced ocular TEAEs (13.9% vs 22.5%, respectively) and TEAEs with a suspected relationship to the study medication compared with the BPL group (5.5% vs 11.8%, respectively). The most common ocular TEAEs were instillation site pain and conjunctival hyperemia.
Conclusion: In patients with POAG or OHT, both T2345 and BPL maintained IOP at or below clinically meaningful values for the duration of the study. T2345 showed a favorable safety profile, with numerically lower incidences of ocular TEAEs than BPL.
Keywords: glaucoma, ocular hypertension, intraocular pressure, benzalkonium chloride, latanoprost, preservative
Corrigendum for this paper has been published.
Introduction
Glaucoma, the leading cause of irreversible blindness worldwide, has a rising prevalence with age.1,2 Globally, approximately 80 million people have been diagnosed with glaucoma, and this number is expected to exceed 111 million by 2040 because of the rapidly aging population.1,2 Glaucoma is a chronic disease characterized by progressive optic neuropathy caused by retinal ganglion cell damage, and the only known modifiable risk factor is intraocular pressure (IOP).3 Early and effective IOP reduction is crucial for preserving optic nerve function and visual field (VF) stability and is therefore the mainstay of glaucoma treatment.3–6 As a chronic condition, glaucoma requires long-term, even lifelong, treatment.
In newly diagnosed patients with primary open-angle glaucoma (POAG) or ocular hypertension (OHT), single topical hypotensive medication is often the initial treatment. However, factors such as disease severity, optic nerve damage, and patient age may necessitate a more complex polypharmacy approach from the onset.7 There are several classes of topical ocular hypotensive medication, each with distinct mechanisms of action. These include α-adrenoceptor agonists, β-adrenoceptor blockers, carbonic anhydrase inhibitors, rho kinase inhibitors, and prostaglandin agonist analogs (PGAs).3 PGAs such as latanoprost are the most frequently prescribed drug class because not only are they effective and generally better tolerated than the alternatives but they also only require once-daily instillation.7
The first PGA approved as first-line therapy for glaucoma was latanoprost, the ester prodrug of prostaglandin F2α, first marketed in the United States (US) in 1996 by Pharmacia & Upjohn (later, by Pfizer) in a 0.005% ophthalmic solution as Xalatan®. Like many topically administered ophthalmic medications, this formulation of latanoprost is formulated with the preservative benzalkonium chloride (BAK). BAK acts as a broad antimicrobial agent, enabling the drug to be packaged in multidose bottles. Furthermore, it is postulated that BAK may enhance the penetration of ophthalmic formulations by loosening tight junctions between corneal epithelial cells.8–12
Over the past few decades, however, a multitude of in vitro, in vivo, preclinical, clinical, and epidemiological studies have shown that chronic BAK exposure, principally from the use of BAK-preserved glaucoma medications, can adversely impact ocular surface health and patients’ quality of life (QOL).8,13–18 The most significant changes to the ocular surface include tear film instability, conjunctival inflammation, subconjunctival fibrosis, epithelial apoptosis, and corneal surface impairment. Clinically, the effects of chronic BAK exposure typically manifest as dry eye or ocular surface disease (OSD), and OSD has been reported in up to 59% of patients with glaucoma.13,18 Side effects include ocular hyperemia, burning, stinging, foreign body sensation, and itching, and although some of these adverse events (particularly conjunctival hyperemia) can also be attributed to the proinflammatory effects of PGAs, BAK can further exacerbate these effects.14–17 In addition to impacting patients’ QOL, the occurrence of these symptoms can severely compromise tolerability and therefore proper regimen adherence.19,20
To avoid the potentially harmful effects of BAK, preservative-free latanoprost 0.005%, packaged in single-unit dose containers (T2345; Monoprost®, Laboratoires Théa),21 was developed. In a phase 3 trial performed in Europe, Rouland et al demonstrated the noninferiority of T2345 to BAK-preserved latanoprost 0.005% (BPL) in terms of lowering IOP in patients with POAG or OHT, while also noting improved local tolerance.22 These observations were reinforced by subsequent clinical trial comparisons of T2345 and BPL.14,22–27 T2345 has been commercially available in the European Union since 2012 and in Canada since 2016 and is now available in 46 countries for the treatment of POAG or OHT. T2345 (IYUZEH™, Thea Pharma, Inc.) was approved by the US Food and Drug Administration (FDA) in December 2022 based on data from the phase 3 trial reported here and from the European phase 3 trial.22 T2345 is currently the first and only preservative-free latanoprost option available in the United States. This study aimed to assess the efficacy and safety of the first FDA-approved preservative-free latanoprost formulation, T2345, in a United States-based patient population.
Methods
This was a prospective, randomized, multicenter, observer-masked, parallel-group noninferiority pivotal phase 3 trial conducted between August 2013 and November 2014 at 31 sites across the US. The trial was designed to investigate the noninferiority of preservative-free latanoprost 0.005% (50 µg/mL) ophthalmic solution, T2345 (IYUZEH™, Thea Pharma, Inc.), to BPL 0.005% ophthalmic solution (Xalatan®, Pfizer) in lowering IOP in patients with POAG or OHT.
The study was conducted in accordance with applicable Good Clinical Practice regulations and guidelines. The study was registered on the ClinicalTrials.gov website with the identifier NCT02059278.
Patients
The study enrolled male and female patients (aged ≥18 years) with a history of POAG or OHT and elevated IOP that was adequately controlled (IOP ≤18 mm Hg, as determined by calibrated Goldmann applanation tonometry) while receiving latanoprost 0.005% ophthalmic solution monotherapy for at least 4 weeks before screening (Day −7 to Day −10). Eligible patients were required to have stable VFs and stable corrected Snellen visual acuity better than 20/200 in the study eye as well as a Shaffer gonioscopic grade of ≥3 in ≥3 quadrants in both eyes. All patients completed at least 3 days of washout before commencing study medication, with a median washout duration in both groups of 7.0 days. The T2345 group had a washout duration range of 3 to 372 days (mean duration: 8.5 days), which was 3 to 38 days in the BPL group (mean duration: 6.3 days). The median washout duration in both groups was 7 days.
Key exclusion criteria included a mean VF deviation of <-20 decibels (dB), a mean IOP >28 mm Hg at baseline, aphakia, any scotoma within 5° of fixation on VF examination, and the use of any other glaucoma medication (other than latanoprost) 2 weeks before screening. The eye with the lower diurnal IOP at screening was designated as the study eye. If both eyes had the same IOP, the study eye was considered the right eye. If both eyes qualified for study inclusion, both eyes were treated with the study drug to ensure adequate IOP control. Patients with one eye qualifying but both eyes having glaucoma and the fellow eye requiring glaucoma medications were excluded. All ophthalmic assessments were performed bilaterally. A full list of study inclusion and exclusion criteria is provided in Supplementary Material 1.
At baseline, patients who met all eligibility criteria were randomized to receive either T2345 or BPL in a 1:1 ratio, according to a randomized block design. A double-masked study design was not feasible because T2345 is supplied in single-dose unit containers and BPL is supplied in a multidose dropper bottle. However, the identities of the study medications were masked to the investigator, to study personnel responsible for ophthalmic evaluations, and to the sponsor personnel responsible for monitoring and medical evaluation of the data. Additionally, IOP measurement readouts were masked to the investigator and were instead read and recorded by another staff member. For any given patient, IOP was measured using the same tonometer and by the same observer (who was to be the investigator/designee) throughout the study, where possible.
Patients were asked to administer one drop into one or both eyes (if both eyes qualified for the study) at 8 PM (±30 minutes), beginning on the night of the baseline visit and continuing for 84 days. If the first drop did not contact the ocular surface during instillation, the patient was to wait approximately 10 to 15 seconds and administer a second drop.
Measures for treatment adherence included systematic drug inventory via the Datatrak Electronic Data Capture system (Datatrak International, Beachwood, Ohio) and staggered dispatch of a three-box drug kit, with only the first box sent initially and the rest sent at set intervals. At every visit, adherence and instillation timings were assessed, and patients returned all medication materials for tracking. Any deviations were documented in the electronic case report form, providing a robust system to ensure compliance and monitor treatment usage.
Assessment Parameters
The primary efficacy endpoint was the between-group comparison of the mean change in IOP values from baseline in the study eye at each time point (8
Safety outcomes were measured through a combination of TEAE reporting, ocular signs on slit lamp examination, and ocular symptoms upon instillation. Conjunctival hyperemia was scored using the McMonnies photographic scale (graded by the investigator from 1 to 6). Other biomicroscopic findings were scored on a four-grade scale of none (0), mild (1), moderate (2), and severe (3). All TEAEs observed by the investigator or reported by patients were recorded, along with their severity and potential relationship to the study treatment. Investigators also assessed the comfort of the study medication in the safety population on Day 15, Day 42, and Day 84 visits via an investigator global local tolerance questionnaire, where patients could choose from the options of very satisfactory, satisfactory, not satisfactory, and unsatisfactory.
Statistical Analyses
Statistical analyses were performed using SAS software version 9.2 (SAS Institute, Cary, North Carolina, USA). Descriptive statistics were provided for the continuous variables, and categorical variables were summarized with counts and percentages.
For the change of IOP from baseline and the change of IOP from screening, at each study visit and time point and for the diurnal IOP, the treatment groups were compared using an analysis of covariance (ANCOVA) model that controlled for pooled study site and baseline/screening IOP. A separate analysis was carried out on the data for the study eye, the treated contralateral eye, and the average of the treated eyes. The difference and 95% CI between treatment groups in adjusted least-square means were presented. All statistical tests were two-sided at the 5% level of significance.
All randomized patients who received at least one dose of the study drug were included in the intent-to-treat (ITT) population; this criterion also includes the safety population. The per-protocol (PP) population consisted of ITT patients with no major protocol violations and no missing data points.
Efficacy analyses were performed on the PP population for the primary efficacy endpoint. Analyses of the primary efficacy variable were also conducted with the ITT population using both observed data and the last observation carried forward approach.
A mixed model of repeated measures (MMRM) analysis was carried out to further evaluate the impact of treatment on IOP. Between-group comparisons were tested using an MMRM model that included the following as fixed factors: treatment, visit, time point, treatment by visit interaction, treatment by visit by time point interaction, patient by time point, and site as a random factor. The objective of this model was to optimally control for IOP variations that could not be linked to treatment. For this purpose, factors influencing the evolution of IOP (patient-specific variations, IOP variations during the day, and measurement biases arising from differences in assessments between assessors and centers) were modeled in order to have an unbiased estimation of the impact of the treatment on IOP.
Results
Patient Disposition and Baseline Characteristics
A total of 335 patients were randomized to receive study treatments: 165 in the T2345 group and 169 in the BPL group (safety population; Figure 1). The ITT population consisted of 334 patients (164 in the T2345 group and 170 in the BPL group), and 325 patients were included in the PP population (161 patients in the T2345 group and 164 patients in the BPL group). The study was completed by 98.2% of patients in the T2345 group and 98.2% of patients in the BPL group, with the most common reasons for early discontinuation from the study being TEAEs and consent withdrawal (Figure 1). No relevant differences in baseline patient characteristics were noted between treatment groups (Table 1), with the mean ± standard deviation (SD) age and proportion of patients with POAG in the T2345 and BPL groups being 67.1±10.2 years and 66.1±11.0 years, respectively, and 72.0% and 78.8%, respectively. The mean ± SD diurnal IOP at baseline (after the minimum 3-day washout) was 18.8 mm Hg ± 2.9 in the T2345 group and 19.2±3.1 mm Hg in the BPL group.
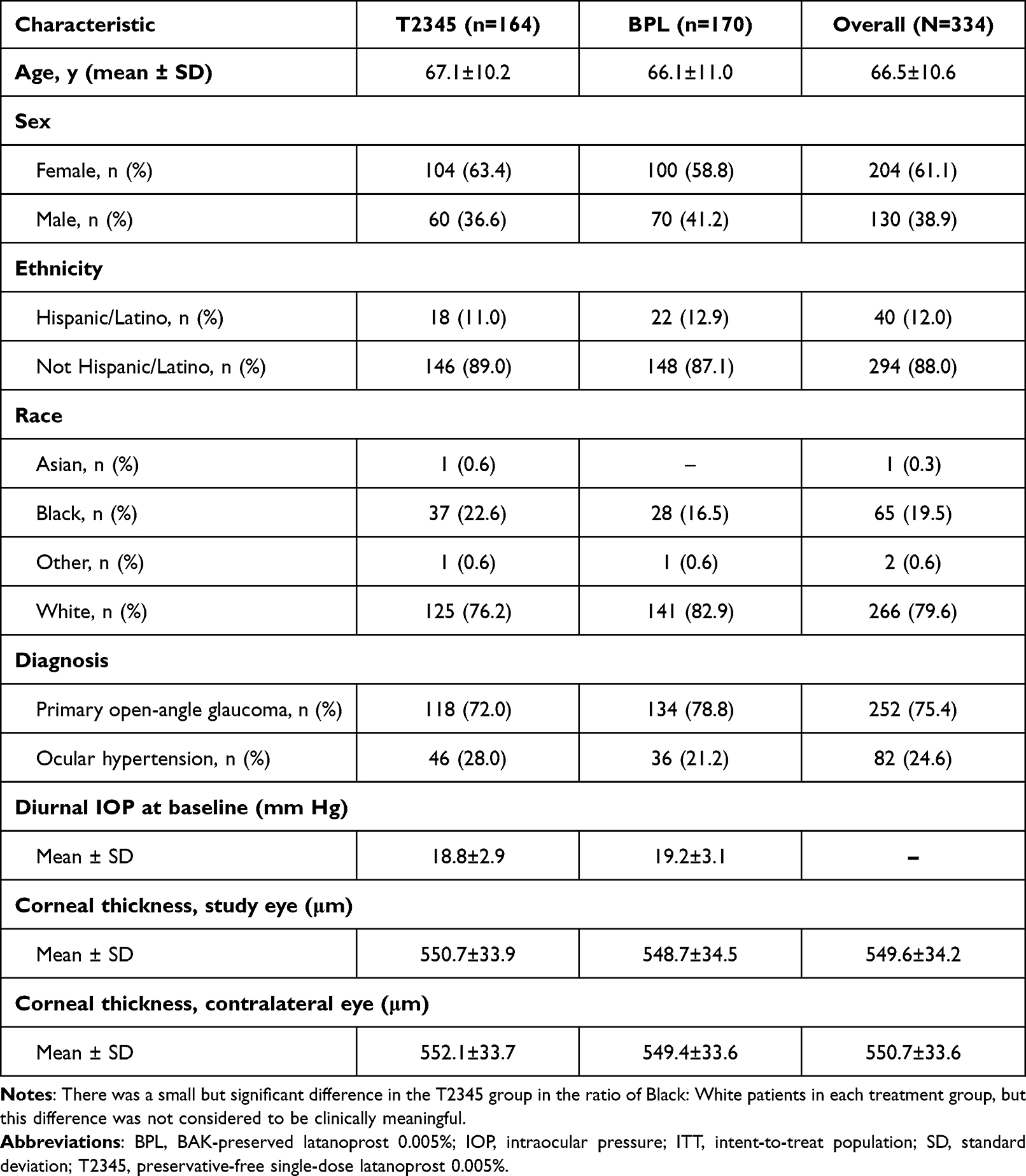 |
Table 1 Summary of Baseline Patient Characteristics for the T2345 and BPL Treatment Groups (ITT Population) |
 |
Figure 1 Patient disposition (a), and study design (b), specifying the timings of screening, washout periods, and assessment schedule timings. *One patient was initially assigned a specific randomization number, but the study medication for this number (BPL) was unusable because it had frozen on the delivery dock. In accordance with the protocol, the patient was assigned the next randomization number, which specified T2345 administration. This patient was analyzed with the T2345 group for the safety population (actual treatment) and with the BPL group for the ITT population. The patient was excluded from the PP population. **Patient had ≥1 discontinuing reason. AE, adverse event; BAK, benzalkonium chloride; BPL, BAK-preserved latanoprost 0.005%; ITT, intent-to-treat; LTFU, lost to follow-up; PP, per protocol; T2345, preservative-free single-dose latanoprost 0.005%. |
IOP-Lowering Efficacy
Both treatments provided clinically meaningful reductions in IOP from baseline to all follow-up visits and time points (Figure 2a). At Day 84, the mean ± SD diurnal IOP was 16.3±2.5 mm Hg in the T2345 group and 15.7±2.6 mm Hg in the BPL group, representing percentage IOP decreases of 13.8% and 17.7%, respectively.
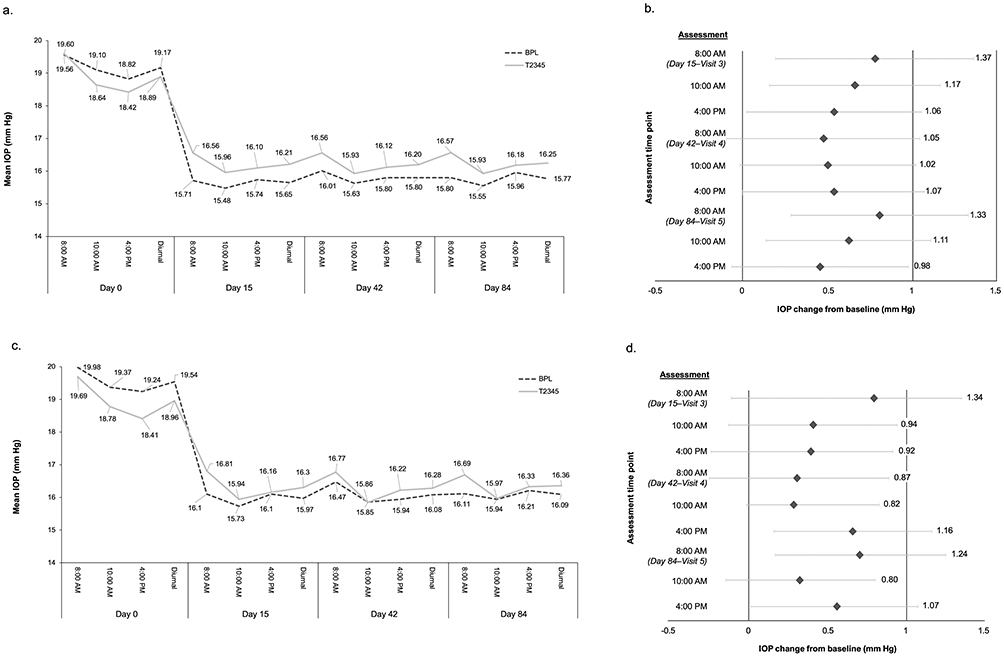 |
Figure 2 Mean IOP values in the study eye in the T2345 and BPL-treated groups (a) and difference in IOP (mm Hg) change from baseline levels between each group at each time point (intent-to-treat population; (b), and in the contralateral eye (c and d). Abbreviations: BAK, benzalkonium chloride; BPL, BAK-preserved latanoprost 0.005%; IOP, intraocular pressure; T2345, preservative-free single-dose latanoprost 0.005%. |
For the primary efficacy endpoint, the two-sided 95% CI of both T2345 and BPL were within 1.5 mm Hg for all time points (9/9) assessed in the study eye of the PP population (Figure 2a). However, only 1/9 time points (Day 84, 4 pm) was within the noninferiority margin of 1.0 mm Hg, with 4/9 time points exceeding this noninferiority margin by 0.07 mm Hg or less (Figure 2b).
In an analysis of the contralateral (worse) eye (Figure 2c), the 95% CI was within 1.5 mm Hg for all time points (9/9) and within 1.0 mm Hg for the majority of time points (5/9) (Figure 2d). Several other analyses also supported the noninferiority of T2345 and BPL (summarized in Table 2). Specifically, when mean screening visit IOPs in the study eye were analyzed as baseline, and also when the mean IOPs of all treated eyes were assessed, the 95% CIs in both treatment groups were within 1.5 mm Hg at all time points evaluated and within 1.0 mm Hg for the majority of time points. Furthermore, both criteria for noninferiority were also met in the MMRM analysis, when IOP was assessed using mean IOP values from either the study eye or the contralateral eye in the PP population and also when using mean IOP values from the contralateral eye in the ITT population.
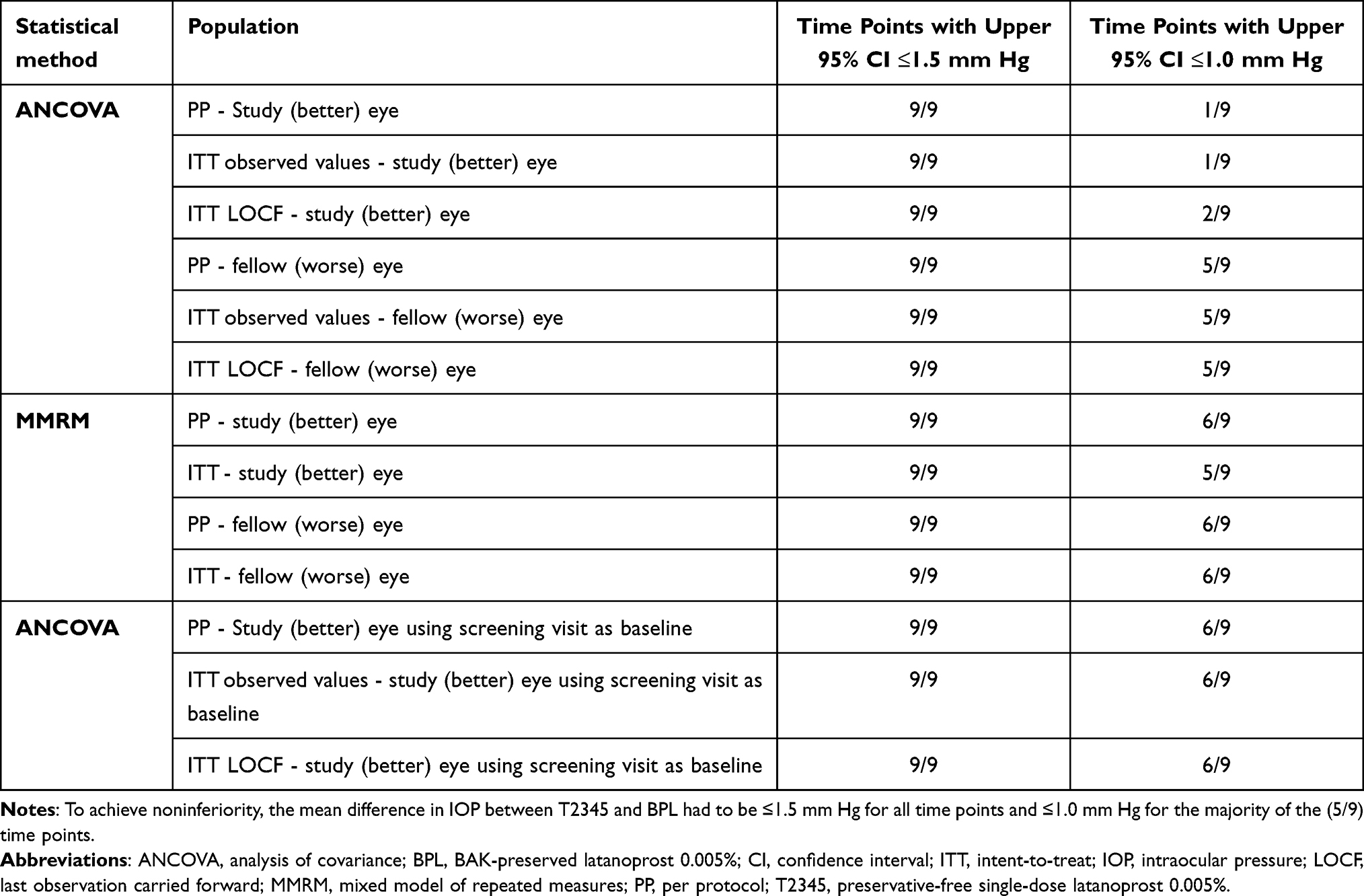 |
Table 2 Statistical Analyses of Noninferiority Criteria |
The percentage of patients with IOP <18 mm Hg at all time points assessed was similar between groups (Figure 3). At one time point (8:00 AM) of Visit 3, the difference between the T2345 and BPL groups was >10%, with a greater percentage of patients in the BPL group compared with the T2345 group having IOP <18 mm Hg. However, at the 10 AM and 4 PM time points of Visit 3, the percentage of patients with IOP <18 mm Hg was similar between the treatment groups. At day 84, 73.1% of patients in the T2345 group and 78.8% in the BPL group had IOPs <18 mm Hg, respectively.
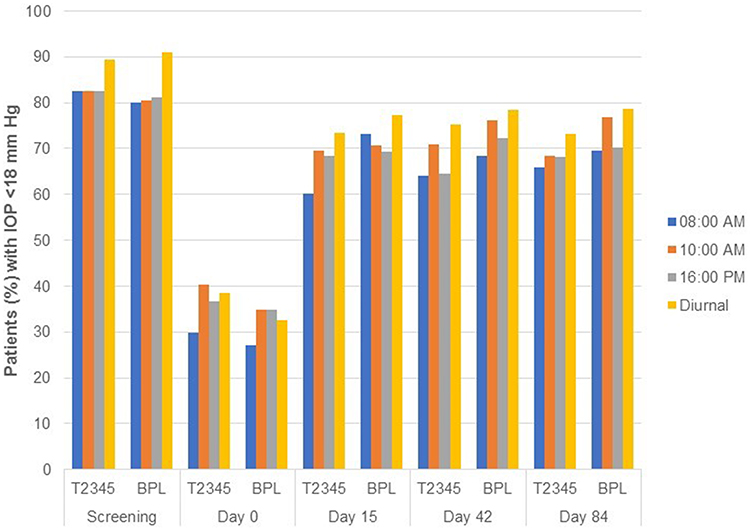 |
Figure 3 Proportion of patients with IOP <18 mm Hg in the study eye (per-protocol population). Abbreviations: BAK, benzalkonium chloride; BPL, BAK-preserved latanoprost 0.005%; IOP, intraocular pressure; T2345, preservative-free single-dose latanoprost 0.005%. |
Visual Field
From screening to Day 84, the mean VF changes from baseline in the study eye for the T2345 and BPL groups were −0.169 ± 1.607 and −0.166 ± 1.680, respectively, with median changes of −0.190 and −0.070. In the fellow eye, mean changes from baseline were 0.067 ± 2.124 and −0.094 ± 1.466 for the T2345 and BPL groups, respectively, with median changes of −0.035 and −0.040.
If the VF test was abnormal, the investigator assessed whether the result was due to a glaucomatous defect. Abnormal VF results due to glaucomatous defects in the study eye were observed in 12.1% (20 patients) and 13.0% (21 patients) of the T2345 group at Visits 1 and 5, compared with 18.9% (32 patients) and 18.2% (30 patients) in the BPL group. In the fellow eye, these defects were noted in 15.2% (25 patients) and 14.8% (24 patients) of the T2345 group at Visits 1 and 5 compared with 19.5% (33 patients) and 18.2% (30 patients) in the BPL group, respectively.
Safety and Tolerability
T2345 was well tolerated throughout the trial. A smaller proportion of patients in the T2345 group than in the BPL group experienced any TEAE (25.5% vs 30.8%; Supplementary Table 1) or any ocular TEAEs (13.9% vs 22.5%, respectively; Supplementary Table 2). Ocular TEAEs with a suspected relationship to the study medication were reported in fewer patients in the T2345 group (9 [5.5%] patients) than in the BPL group (20 [11.8%] patients). All treatment-related TEAEs were ocular; no nonocular TEAEs were suspected to be related to study medication for either the T2345 or BPL group. The most common treatment-related TEAEs by preferred term (Medical Dictionary for Regulatory Activities; MedDRA) for T2345 were instillation site pain (3 patients, 1.8%) and conjunctival hyperemia and instillation site pruritus (2 patients, 1.2%; Table 3). The most common TEAEs suspected to be related to BPL were instillation site pain (8 patients, 4.7%), conjunctival hyperemia (4 patients, 2.4%), punctate keratitis (3 patients, 1.8%), and instillation site abnormal sensation and instillation site complication (2 patients, 1.2%). Serious TEAEs were observed in 1 (0.6%) T2345-treated patient and 4 (2.4%) BPL-treated patients, but none were ocular or considered to be treatment-related.
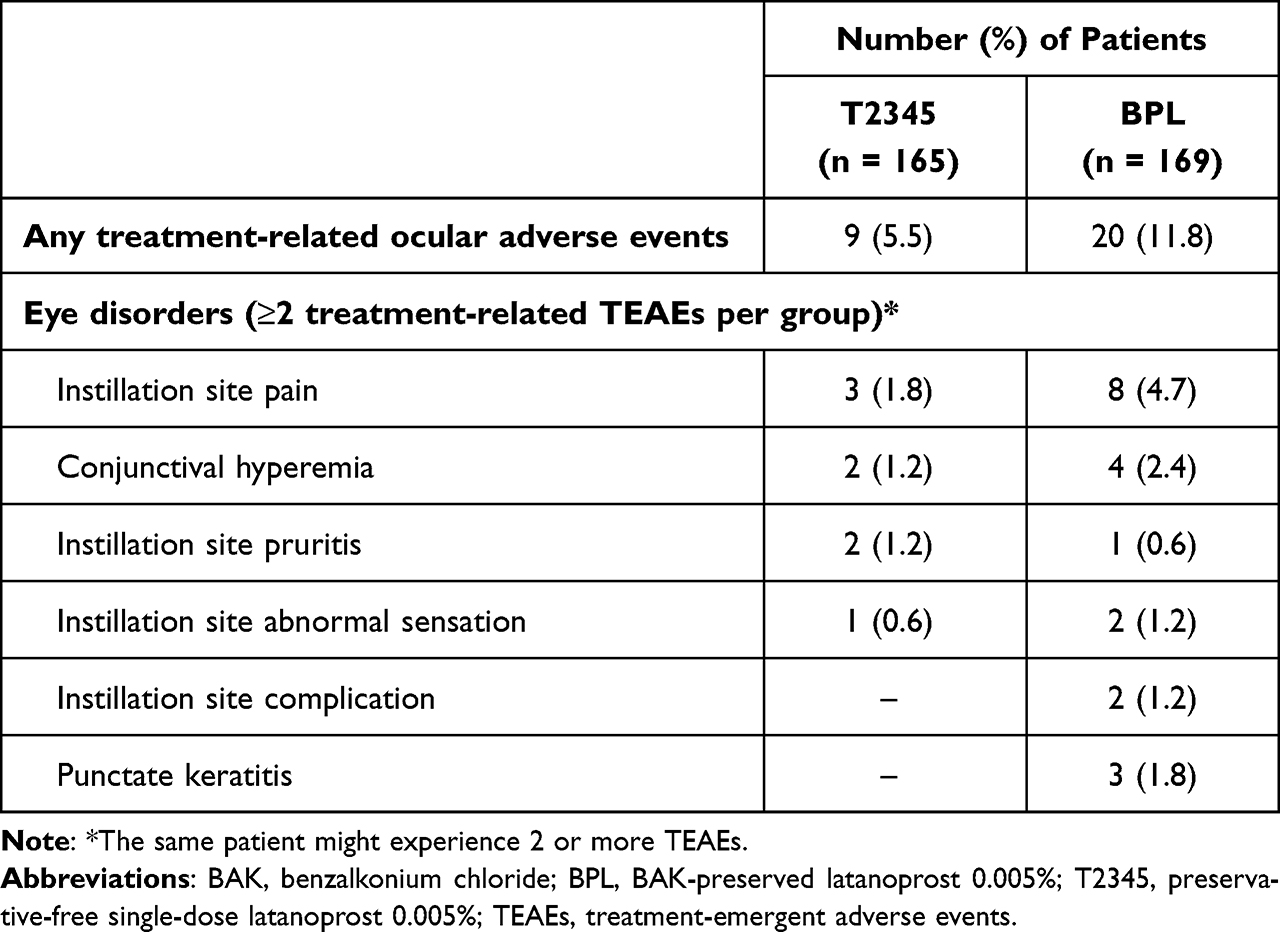 |
Table 3 Number (%) of Patients with Most Common Ocular Treatment-Emergent Adverse Events with Relationship to Study Medicine by Preferred Term (Safety Population) |
For one patient in the BPL group, administration of the study drug was temporarily ceased due to corneal abrasion (of moderate intensity) that later resolved. Two patients had TEAEs that were suspected of being related to the study drug, resulting in study drug discontinuation. One was a patient who received T2345 and experienced conjunctivitis (of moderate intensity) that later resolved, and the other was a patient who received BPL and who experienced both blepharitis and conjunctival hyperemia (of moderate intensity), neither of which had resolved by the end of the trial.
No significant between-group differences were observed in terms of clinically significant abnormalities on slit lamp examination, on ophthalmoscopy/dilated fundus examination, or in McMonnies scale scores of conjunctival hyperemia in either the study or treated contralateral eyes, with the prevalence of each item being low in both treatment groups. The incidence of conjunctival hyperemia as a TEAE was numerically higher in patients who received BPL than in those receiving T2345 (n=4 versus n=2), although this difference was not statistically significant. In terms of the Investigator Assessment of Comfort of the Study Medication questionnaire results, ratings in both groups were “very satisfactory” for most patients at all visits and were either “very satisfactory” or “satisfactory” for at least 98.2% of all patients at any time point in both groups (Figure 4).
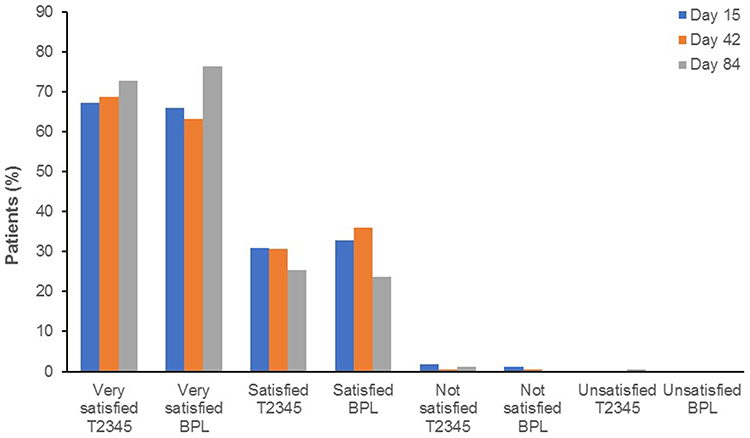 |
Figure 4 Investigator assessment of comfort of the study medication scores (safety population) split by treatment group and assessment date. Abbreviations: BPL, BAK-preserved latanoprost 0.005%; T2345, preservative-free single-dose latanoprost 0.005%. |
Discussion
This study evaluated the safety and efficacy of T2345 compared to BPL in a US patient population with POAG or OHT. To demonstrate the noninferiority between T2345 and BPL, the 95% CI of the difference between the two treatments had to be within 1.5 mm Hg for all time points measured and within 1.0 mm Hg for the majority of the time points measured. In the prespecified primary efficacy analysis using the PP population, the 95% CI of the difference between T2345 and BPL in the study eye was within 1.5 mm Hg for all time points measured but not within 1.0 mm Hg for the majority of the time points. Therefore, both predefined criteria for noninferiority were not met. Nonetheless, T2345 demonstrated the ability to maintain IOP below the clinically meaningful level of 18 mm Hg for the duration of the study, starting at Day 15, with a mean ±SD diurnal IOP reduction in the study eye at Day 84 of 2.6 mm Hg ±2.4 (~13.8%) from baseline. There was a numeric difference in the percentages of patients with IOP <18 mm Hg in the study eye between the T2345 and BPL groups. However, the difference was not statistically significant.
T2345 was well tolerated throughout the study. Ocular TEAEs were reported at a lower incidence in the T2345 group (13.9%) than in the BPL group (22.5%), and fewer patients in the T2345 group (5.5%) than in the BPL (11.8%) group experienced treatment-related ocular TEAEs. In terms of ocular TEAEs judged to be related to the study medication, only conjunctival hyperemia, instillation site pain, and instillation site pruritis exceeded an incidence of 1% in T2345 patients, compared with conjunctival hyperemia and punctate keratitis as well as pain, abnormal sensation, and complications at the instillation site exceeding a 1% incidence in BPL-treated patients.
In the European phase 3 noninferiority trial that compared T2345 with BPL in a population of 463 patients with POAG or OHT, the criteria for noninferiority was met.22 The mean estimated difference on Day 84 between the T2345 and BPL groups in terms of the change from baseline IOP was 0.417 mm Hg with a 95% CI of −0.006 to 0.840 mm Hg. This study also demonstrated a mean ± SD IOP reduction in the study eye of 8.6 ± 2.6 mm Hg (~36%) at Day 84 (versus baseline) in the T2345 group and 9.0 ± 2.4 mm Hg (~38%) in the BPL group in the modified ITT (mITT) population. These findings are consistent with what has been reported in phase 3 clinical trials for BPL and potassium sorbate–preserved latanoprost 0.005%,28 with reductions of 6–8 mm Hg from baseline for both, along with IOP reductions reported for other PGAs (~25%-33%).29,30
An important difference between these clinical trials and the current trial is the baseline IOP levels. Patients in the European T2345 clinical trial had a mean baseline IOP of 24.1 mm Hg.22 In the current trial, the mean diurnal baseline IOP was 18.8 mm Hg in the T2345 group and 19.2 mm Hg in the BPL group. The lower the baseline IOP, the less of an effect one would expect to see, and this is also likely why the mean reduction in IOP with BPL was only 3.4 mm Hg (17.7%), which is significantly lower than what has been previously reported.31 The difference in baseline IOPs may be attributed to the short and variable washout period in the US trial (with median duration of 7 days in both groups), which may have been insufficient to achieve normal nontreated values. Indeed, after the washout period, patients only had a 4.1 mm Hg increase in IOP from screening compared with an 8.6 mm Hg increase in the European phase 3 trial. Remarkably, however, even with a mean baseline IOP close to the clinical threshold of 18 mm Hg, T2345 was able to reduce IOP by approximately 3 mm Hg.
Other factors may also have contributed to the noninferiority criteria not being achieved in this study. These include the selection of the better eye instead of the worse eye (ie the eye with the higher IOP at baseline) as the study eye, a smaller sample size, and the use of different statistical methods compared with the European phase 3 trial. Indeed, when additional analyses were performed, either on the contralateral eye or average of both eyes, using Visit one as baseline for the study eye (to mitigate some of the washout variability), or by applying a MMRM analysis (similar to that used in the European phase 3 trial), both criteria for noninferiority were met. Alternatively, one theoretical benefit of formulating topically applied ophthalmic medications with BAK is that it can act as a penetration enhancer, potentially enabling higher drug doses to be delivered to intraocular structures and resulting in greater drug efficacy.9,10 Therefore, it could be hypothesized that some of the drug efficacy may have been lost with T2345. However, considering the evidence base of ex-US studies in the literature that have demonstrated the noninferiority of T2345 to BPL and other preserved PGAs, including head-to-head clinical comparisons,27 and several other studies with significantly different study designs, such as crossover studies,32 observational studies,19,33 and meta-analyses14,26 along with the results from the additional analyses in the current study, this does not seem likely. Although this study did not meet certain noninferiority criteria, the FDA approved T2345 based on totality of evidence submitted including the European pivotal trial described here.22
T2345 was developed in an effort to eliminate the detrimental effects of BAK on the ocular surface. BAK-free PGAs have been shown to reduce the incidence of ocular signs and symptoms, such as irritation, pain, discomfort, and dry eyes, compared with BAK-containing formulations.27,34 In the current study, both T2345 and BPL were well tolerated, although T2345 may have had a more favorable safety profile. A smaller proportion of patients in the T2345 group (13.9%) experienced ocular TEAEs compared with those in the BPL group (22.5%). Furthermore, the incidence of treatment-related ocular TEAEs in the T2345 group was approximately half of that of the BPL group (5.5% vs 11.8%). Similar findings were reported in a recent post hoc pooled analysis that compared patient tolerance and IOP-lowering efficacy of T2345 to BPL from 3 randomized clinical trials (two Phase 3 studies and a Phase 4 study) and 2 international real-world evidence observational studies.14 This analysis of 3610 patients found that T2345 was 2 times more effective in reducing ocular hyperemia and an OSD composite score compared with BPL (ie, there was a 32.2% decrease in ocular signs and symptoms with T2345 compared with 14.1% with BPL). The mean IOP was similar between the groups at 3 months. Although the results of the current study are consistent with studies demonstrating improved local tolerance with BAK-free formulations, the full benefit of preservative-free T2345 on the ocular surface may not have been elucidated in this relatively short-term study.
Additional limitations in this trial include the sample size (334 patients in the ITT population), which is almost 40% lower than the sample size for the T2345 European trial.22 Furthermore, the exclusion of patients known to be intolerant of BAK or the study drugs made the study population not wholly representative of the real-world patient population.
The option of having a preservative-free iglaucoma medication that has similar IOP-lowering efficacy as preserved medications, but with improved tolerability, may have important clinical implications. Poor tolerability can negatively impact patients’ QOL and contribute to poor regimen adherence and patients not refilling their prescription.35,36 Therefore, improving tolerability may lead to better patient adherence to glaucoma therapy regimens, potentially improving the long-term efficacy of the medication. Moreover, reducing the risk of OSD may improve patients’ QOL.37,38 Finally, better regimen adherence and persistence, as well as fewer consultations for BAK-induced OSD, may result in cost savings for patients and healthcare providers.15,37
Conclusion
Several clinical studies conducted outside of the US have demonstrated that T2345 is comparable to BPL in lowering IOP and has an improved tolerability profile. The current study supports these findings, with comparable IOP-lowering efficacy shown with T2345 and BPL in patients with POAG or OHT. T2345 was also well tolerated with a lower incidence of overall ocular TEAEs compared with BPL. The combination of T2345’s efficacy, favorable tolerability profile, and the fact that chronic exposure to BAK has significant potential long-term risksall make T2345 a suitable and potentially preferable alternative to BAK-preserved latanoprost for the management of patients with glaucoma or OHT.
Abbreviations
AE, adverse event; BAK, benzalkonium chloride; CI, confidence interval; IOP, intraocular pressure; IRB, Institutional Review Board; ITT, intent-to-treat; POAG, primary open-angle glaucoma; PP, per-protocol; OHT, ocular hypertension; SAE, serious AE; TEAE, treatment-emergent AE; US, United States; VF, visual field.
Data Sharing Statement
Thea Pharma Inc is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, analysis plans), provided that the trials are not part of an ongoing or planned regulatory submission. This commitment covers requests for clinical trial data for unlicensed products and indications.
These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent scientific research and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA).
Data requests can be submitted at any time after the product is approved in the US and Europe and after the acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered upon review.
For more information on the process or to submit a request, visit the following link: https://theapharmainc.com/contact-us.
All data sharing will abide by the prevailing privacy regulations and guidelines to protect the confidentiality and privacy of the patients.
Ethical Considerations
The study was authorized by the Institutional Review Board (IRB), Alpha IRB, and informed consent was obtained from all patients. All components of this research followed the tenets of the Declaration of Helsinki, complied with International Council for Harmonisation guidelines, and complied with all applicable US federal regulations as well as local legal and regulatory requirements.
Acknowledgments
Mark Hillen, BSc, PhD, and Esther Tazartes, MS, of the Global Outcomes Group, Inc., provided editorial assistance, which was funded by Laboratoires Théa.
Funding
This study was funded by Laboratoires Théa.
Disclosure
Dr. Michael S. Korenfeld is a consultant for Novartis, Orasis, EyePoint Pharmaceuticals, Allysta Pharmaceuticals, Jotteq, Santen, and ZEISS. Prof. Christophe Baudouin is a consultant for AbbVie, Alcon, Horus Pharma, Oculis, Santen, and Théa. Dr. Steven Zhang is employed by Thea Pharma. Inc. Dr. Bacharach is a consultant for Thea Pharma Inc. and receives funding for research from Thea Pharma Inc. Dr. Ike K. Ahmed reports C-Consultant/Consulting Fees S-Speakers Honoraria/ R- Research Grant/Support from: 1. Aequus: C 2. Ace Vision: C 3. Aerie Pharmaceuticals: C, R 4. Akorn: C 5. Alcon: C,S,R 6. Allergan: C,S,R 7. Aquea Health, Inc: C 8. ArcScan: C 9. Avellino Lab USA, Inc: C 10. Avisi: C 11. Bausch Health: C 12. Beaver Visitec: C 13. Beyeonics: C 14. Bionode: C, R 15. Carl Zeiss Meditec: C,S 16. Centricity Vision, Inc: C 17. CorNeat Vision: C 18. Custom Surgical: C 19. Elios Vision: C 20. ElutiMed: C 21. Equinox: C 22. eyeFlow, Inc: C 23. EyeMed: C 24. EyeQ Technologies: C 25. Exhaura Limited: C 26. Genentech: C 27. Glaukos: C, R 28. Gore: C 29. Heine: C, S 30. Heru: C 31. Iantrek: C 32. InjectSense: C 33. Iridex: C 34. iCare: R 35. iStar: C 36. Ivantis: C, R 37. Johnson & Johnson Vision: C, S, R 38. Labtician Thea: C 39. LayerBio: C 40. Leica Microsystems: C 41. Life Long Vision: C 42. Long Bridge Medical, Inc: C 43. MicroOptx: C 44. MST Surgical: C, S 45. Myra Vision: C 46. New World Medical: C, R 47. NovaEye: C 48. Ocular Instruments: C 49. Ocular Therapeutix: C 50. Oculo: C 51. Oculus Surgical: C 52. Omega Ophthalmics: C 53. PolyActiva: C 54. PulseMedica: C 55. Radiance Therapeutics, Inc: C 56. Radius XR: C 57. Rheon Medical SA: C 58. Ripple Therapeutics: C 59. Sanoculis: C 60. Santen: C, R 61. Singapore Biodesign Programme Office 62. Shifamed, LLC: C 63. Sight Sciences: C 64. Smartlens, Inc: C 65. Stroma: C 66. Thea Pharma: C 67. TFS Health Science: C 68. ViaLase: C 69. Visus Therapeutics: C 70. Vizzario: C 71. VSY Biotechnology: C 72. Zilia, Inc: C. Dr. Elizabeth Sharpe works solely for the Veterans Administration. She is not a paid consultant for or an employee of any other company. The authors report no other conflicts of interest in this work.
References
1. Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Allison K, Patel D, Alabi O. Epidemiology of glaucoma: the past, present, and predictions for the future. Cureus. 2020;12(11):e11686. doi:10.7759/cureus.11686
3. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi:10.1001/jama.2014.3192
4. Musch DC, Gillespie BW, Lichter PR, Niziol LM, Janz NK, CIGTS Study Investigators. Visual field progression in the Collaborative Initial Glaucoma Treatment Study: The impact of treatment and other baseline factors. Ophthalmology. 2009;116(2):200–207. doi:10.1016/j.ophtha.2008.08.051
5. Nouri-Mahdavi K, Hoffman D, Coleman AL, et al. Predictive factors for glaucomatous visual field progression in the Advanced Glaucoma Intervention Study. Ophthalmology. 2004;111(9):1627–1635. doi:10.1016/j.ophtha.2004.02.017
6. Leske MC, Heijl A, Hussein M, et al. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48–56. doi:10.1001/archopht.121.1.48
7. Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021;128(1):71–P150. doi:10.1016/j.ophtha.2020.10.022
8. Baudouin C, Labbe A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
9. Brunner J, Ragupathy S, Borchard G. Target specific tight junction modulators. Adv Drug Deliv Rev. 2021;171:266–288. doi:10.1016/j.addr.2021.02.008
10. Burstein NL. Preservative alteration of corneal permeability in humans and rabbits. Invest Ophthalmol Vis Sci. 1984;25(12):1453–1457.
11. Majumdar S, Hippalgaonkar K, Repka MA. Effect of chitosan, benzalkonium chloride and ethylenediaminetetraacetic acid on permeation of acyclovir across isolated rabbit cornea. Int J Pharm. 2008;348(1–2):175–178. doi:10.1016/j.ijpharm.2007.08.017
12. Okabe K, Kimura H, Okabe J, et al. Effect of benzalkonium chloride on transscleral drug delivery. Invest Ophthalmol Vis Sci. 2005;46(2):703–708. doi:10.1167/iovs.03-0934
13. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350–355. doi:10.1097/IJG.0b013e31815c5f4f
14. Harasymowycz P, Hutnik C, Rouland JF, et al. Preserved versus preservative-free latanoprost for the treatment of glaucoma and ocular hypertension: a post hoc pooled analysis. Adv Ther. 2021;38(6):3019–3031. doi:10.1007/s12325-021-01731-9
15. Thygesen J. Glaucoma therapy: preservative-free for all? Clin Ophthalmol. 2018;12:707–717. doi:10.2147/OPTH.S150816
16. Stalmans I, Lemij H, Clarke J, Baudouin C. Signs and symptoms of ocular surface disease: the reasons for patient dissatisfaction with glaucoma treatments. Clin Ophthalmol. 2020;14:3675–3680. doi:10.2147/opth.S269586
17. Alm A. Latanoprost in the treatment of glaucoma. Clin Ophthalmol. 2014;8:1967–1985. doi:10.2147/OPTH.S59162
18. Baudouin C, Renard JP, Nordmann JP, et al. Prevalence and risk factors for ocular surface disease among patients treated over the long term for glaucoma or ocular hypertension. Eur J Ophthalmol. 2012:1:56. doi:10.5301/ejo.5000181
19. Wolfram C, Stahlberg E, Pfeiffer N. Patient-reported nonadherence with glaucoma therapy. J Ocul Pharmacol Ther. 2019;35(4):223–228. doi:10.1089/jop.2018.0134
20. Kastelan S, Tomic M, Metez Soldo K, Salopek-Rabatic J. How ocular surface disease impacts the glaucoma treatment outcome. Biomed Res Int. 2013;2013:696328. doi:10.1155/2013/696328
21. Thea Pharmaceuticals Ltd. Summary of Product Characteristics. MONOPOST latanoprost 50 mcg/mL eye drops, solution in single-dose container. Available from: https://www.medicines.org.uk/emc/product/2978/smpc.
22. Rouland JF, Traverso CE, Stalmans I, et al. Efficacy and safety of preservative-free latanoprost eyedrops, compared with BAK-preserved latanoprost in patients with ocular hypertension or glaucoma. Br J Ophthalmol. 2013;97(2):196–200. doi:10.1136/bjophthalmol-2012-302121
23. Muñoz Negrete FJ, Lemij HG, Erb C. Switching to preservative-free latanoprost: impact on tolerability and patient satisfaction. Clin Ophthalmol. 2017;11:557–566. doi:10.2147/opthOPTH.S126042
24. Economou MA, Laukeland HK, Grabska-Liberek I, Rouland JF. Better tolerance of preservative-free latanoprost compared to preserved glaucoma eye drops: the 12-month real-life FREE study. Clin Ophthalmol. 2018;12:2399–2407. doi:10.2147/opthOPTH.S176605
25. Denis P. Unpreserved latanoprost in the treatment of open-angle glaucoma and ocular hypertension. A multicenter, randomized, controlled study. J Fr Ophtalmol. 2016;39(7):622–630. doi:10.1016/j.jfo.2016.05.006
26. Cucherat M, Stalmans I, Rouland JF. Relative efficacy and safety of preservative-free latanoprost (T2345) for the treatment of open-angle glaucoma and ocular hypertension: an adjusted Indirect comparison meta-analysis of randomized clinical trials. J Glaucoma. 2014;23(1):e69–75. doi:10.1097/IJG.0b013e3182a075e6
27. Misiuk-Hojlo M, Pomorska M, Mulak M, et al. The RELIEF study: tolerability and efficacy of preservative-free latanoprost in the treatment of glaucoma or ocular hypertension. Eur J Ophthalmol. 2019;29(2):210–215. doi:10.1177/1120672118785280
28. Shen Lee B, Malhotra R, Sall K, Mitchell B, Peace J. Open-label extension study comparing latanoprost 0.005% without vs with benzalkonium chloride in open-angle glaucoma or ocular hypertension. Clin Ophthalmol. 2022;16:2285–2293. doi:10.2147/opth.S367756
29. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Open-Angle Glaucoma. San Francisco: American Academy of Ophthalmology; 2010.
30. Wirta D, Malhotra R, Peace J, et al. Noninferiority study comparing latanoprost 0.005% without versus with benzalkonium chloride in open-angle glaucoma or ocular hypertension. Eye Contact Lens. 2022;48(4):149–154. doi:10.1097/ICL.0000000000000860
31. Camras CB. Comparison of latanoprost and timolol in patients with ocular hypertension and glaucoma: a six-month masked, multicenter trial in the United States. The United States Latanoprost Study Group. Ophthalmology. 1996;103(1):138–147. doi:10.1016/s0161-6420(96)30749-5
32. Aptel F, Choudhry R, Stalmans I. Preservative-free versus preserved latanoprost eye drops in patients with open-angle glaucoma or ocular hypertension. Curr Med Res Opin. 2016;32(8):1457–1463. doi:10.1080/03007995.2016.1202818
33. Aspberg J, Heijl A, Jóhannesson G, Lindén C, Andersson-Geimer S, Bengtsson B. Intraocular pressure lowering effect of latanoprost as first-line treatment for glaucoma. J Glaucoma. 2018;27(11):976–980. doi:10.1097/ijg.0000000000001055
34. Uusitalo H, Chen E, Pfeiffer N, et al. Switching from a preserved to a preservative-free prostaglandin preparation in topical glaucoma medication. Acta Ophthalmol. 2010;88(3):329–336. doi:10.1111/j.1755-3768.2010.01907.x
35. Fenwick EK, Man RE, Aung T, Ramulu P, Lamoureux EL. Beyond intraocular pressure: optimizing patient-reported outcomes in glaucoma. Prog Retin Eye Res. 2020;76:100801. doi:10.1016/j.preteyeres.2019.100801
36. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
37. Skalicky SE, Goldberg I, McCluskey P. Ocular surface disease and quality of life in patients with glaucoma. Am J Ophthalmol. 2012;153(1):1–9 e2. doi:10.1016/j.ajo.2011.05.033
38. Quaranta L, Riva I, Gerardi C, Oddone F, Floriani I, Konstas AG. Quality of life in glaucoma: a review of the literature. Adv Ther. 2016;33(6):959–981. doi:10.1007/s12325-016-0333-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.