Back to Journals » International Journal of General Medicine » Volume 15
Presenting Clinicoradiological Features, Microbiological Spectrum and Outcomes Among Patients with Septic Pulmonary Embolism: A Three-Year Retrospective Observational Study
Authors Yusuf Mohamud MF ![]() , Mukhtar MS
, Mukhtar MS ![]()
Received 1 March 2022
Accepted for publication 16 May 2022
Published 25 May 2022 Volume 2022:15 Pages 5223—5235
DOI https://doi.org/10.2147/IJGM.S364522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Farah Yusuf Mohamud, Mahad Sadik Mukhtar
Mogadishu Somali-Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Farah Yusuf Mohamud, Mogadishu Somali-Turkish Training and Research Hospital, 30 Street, Alikamin, Wartanabada District, Mogadishu, Somalia, Tel +252615591689, Email [email protected]
Background: Septic pulmonary embolism (SPE) is an unusual condition characterized by the implantation of infected thrombi into the pulmonary vasculature from a variety of infectious sources. This study aimed to illustrate the clinicoradiological features, microbiological spectrum, and clinical course of patients with SPE, as well as to promote the early identification, diagnosis, and prognosis of this unusual disease.
Methods: Nineteen patients with SPE collected from the electronic medical records of our hospital were retrospectively reviewed during three years.
Results: The study included twelve men and seven women with a mean age of 49 (15– 78). The most common presenting features were fever (79%) and shortness of breath (73.7%). Chronic kidney disease (68.4%) and diabetes (36.8%) were the most common comorbidities. The most common source of infection was venous catheters (58%). Staphylococcus aureus was the most predominant pathogen in about 52.6% of the cases. According to the CT findings, bilateral opacities were detected in all cases, flowing by nodular in 73.9% and cavitations in 57.9%. Central distributions were the most patterns regarding the location of the lesion seen in 47.4% of the patients. All patients received antimicrobial treatment, while 13 cases administered systemic anticoagulant. Most of the patients (73.7%) recovered from their illness, while 26.3% died. The median duration of hospitalization was 11.5 days. Oxygen saturation level and altered mental status were significantly associated with the mortality rate of SPE patients.
Conclusion: The study’s findings presented that altered mental status and low oxygen saturation are associated with a high mortality rate in SPE patients, especially those requiring critical care. Early diagnosis of an embolic phenomenon to other organ systems like the central nervous system can greatly influence the patient’s outcome.
Keywords: septic pulmonary embolism, hemodialysis, chest CT scan, intensive care unit, emergency
Background
Septic pulmonary embolism (SPE) is an unusual condition described as the implantation of infected thrombi into the pulmonary vasculature from primarily different infectious sites resulting in a parenchymal infection that generally presents with an insidious onset of fever, respiratory symptoms such as cough, shortness of breath, pleuritic chest pain, and lung infiltrates.1,2
Commonly microorganisms originate from the primarily extra-pulmonary infectious loci such as bone, skin, and other soft tissue infections, intravascular devices and catheters, peritonsillar abscesses, periodontal disease, infective endocarditis, and liver abscesses.1,3–6
The radiographic features of pulmonary SE have been described; in general, computer tomography (CT) seems to be more sensitive than chest radiography early in the course of infection and may reveal different features included multiple peripheral nodules, feeding vessel signs, pleural-butting, wedge-shaped peripheral lesions, cavity formation, and pleural effusion.7 The treatment outcomes in patients with SPE depend on the insight of the illness on initial presentation, early diagnosis of an embolic phenomenon to other organ systems like CNS, type of microorganism, level of antibiotic resistance, and source of infection obtained.1
Regardless of its life-threatening nature, data on patients with SPE have not been reported in Somalia. Therefore, this study aimed to illustrate the clinicoradiological features, microbiological spectrum, and outcome among patients with SPE as well as treatment outcomes in 19 Somalian patients with SPE to promote the identification, diagnosis, and prognosis of this unusual disease.
Method
The study population consisted of 19 patients admitted to the hospital from January 1, 2018, to December 22, 2020, whose medical records were retrospectively evaluated to identify patients with SPE in hospital information system (HIS) of Mogadishu Somali Turkey Education and Research Hospital, Mogadishu, Somalia.
The hospital employs about 1000 people, with over 600 of them working in the medical field. Internal medicine, emergency medicine, dermatology, ophthalmology, maternity and child health, critical care, general surgery, urology, thoracic surgery, cardiovascular surgery, orthopedics, neurosurgery, Otorhinolaryngology mental health, and dental medical services are all operational. The program will begin in conjunction with the Somalia Ministry of Health and the Turkish Ministry of Health. Every day, the hospital serves more than 50 acute ill patients.
The inclusion criteria included a chest computed tomography (CT) scan showing peripheral, central, or diffuse lung infiltrates indicative of SPE and the presence of active extra-pulmonary infection as a septic embolic source. Patients with other possible explanations for lung infiltrates, including corona virus-infected patients, patients who died in the emergency department, and those whose ages were less than 18 years, were excluded from the study.
Patients with SPE were identified using a hospital information system (HIS). We included the clinical parameters reviewed: age, sex, clinical course, clinical presentations, vital signs, laboratory results, microbiologic culture results, source or origin of infection, radiological findings included chest CT and echocardiography, treatment (including antibiotic regimens, anticoagulation, and other supportive treatment), co-morbid medical conditions, and outcomes. SPE patients were confirmed according to the diagnostic criteria described by Cook et al.3
Based on the Clinical and Laboratory Standards Institute (CLSI) system, we determined antimicrobial sensitivity and resistance through the standard Kirby-Bauer disk diffusion and commercial disks. The identification of the microorganisms was made using eosin methylene blue agar (EMB) and blood agar. Regarding the ESBL identification, positive cultures were assessed using cefuroxime + ceftriaxone and amoxicillin-clavulanic acid as the identifying disc to differentiate the growth patterns between antibiotics with and without lactamase inhibitor. Antimicrobial sensitivity and resistance were assessed using Mueller-Hinton agar. The antibiotic susceptibility of the pathogens was studied by using piperacillin/tazobactam 100/10 mcg, meropenem 10mcg, imipenem 10mcg, amikacin 30 mcg, ceftriaxone 30ug, clindamycin 2mcg, penicillin G 1 U, trimethoprim/sulfamethoxazole 1.25/23.75 mcg, vancomycin 30 mcg, tetracycline 30 mcg, and levofloxacin 5mcg.8
The chest CT was evaluated by two expert chest radiologists, who were unaware of the clinical information and the bacteriology to increase the reliability of the diagnosis, and the decisions concerning the CT findings reached by consensus.
The results were recorded and analyzed by SPSS software version 23.0, and outcomes were displayed as mean SD for continuous variables and percentage for categorical variables.
This study was approved by the research ethics committee of Mogadishu Somali Turkish Education and Research Hospital (Reference Number: MSTH/6385) and performed in accordance with the principles of the Declaration of Helsinki. The requirement to obtain written informed consent from each patient was waived because this was an observational retrospective study. The patients’ information were anonymous and non identifiable.
Results
Clinical and Socio-Demographic Characteristics
We extracted data from nineteen patients with clinicoradiological confirmed septic pulmonary embolism (SPE) admitted to the hospital between 02.01.2016 and 08.02.2021. Due to a lack of demographic and baseline data from the hospital information system (HIS), we excluded five of the 24 patients from the report.
There were 63.2% men and 36.8 women with a mean age of 49 (15–78). The potential source of infection was identified as venous catheter-associated with bloodstream infection predominantly (57.9%), followed by Soft tissue and bone sites (21%), Peritonsillar abscess (10.5%), and urine (5.3%). Table 1 lists the microorganisms detected.
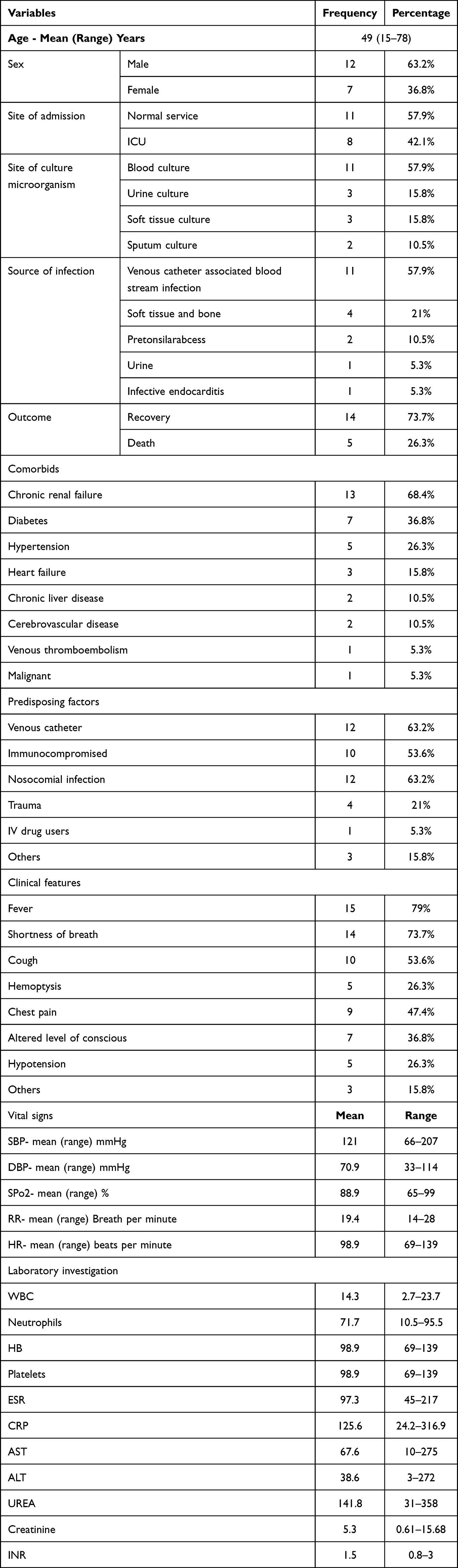 |
Table 1 Baseline Characteristics, Laboratory Findings and Outcomes of 19 Patients Diagnosed and Treated with Septic Pulmonary Emboli Between Years 2017 and 2020 |
The most common presenting features were fever (79%), Shortness of breath (73.7%), Cough (53.6%), Hemoptysis (26.3%), Chest pain (47.4%), and altered level of conscious (36.8%) (Table 1). Most patients had 84.2%, had at least one comorbidity, but chronic kidney injury (68.4%) was the most common comorbidity. Among all patients, 57.9% required non-intensive care unit admission, while the remaining was admitted to the intensive care unit (ICU). More than two-thirds of all patients were recovered, while 26.3% had died.
Laboratory Characteristics
A Complete blood count (CBC), liver function and Renal function tests was performed in all patients including those in the ICU and the mean differential CBC showed WBC (14.3505) (p 0.589, 95% [CI] 0.701–1.475) with Neutrophils being the most common, followed by ESR with a mean range of (97.2632) (p 0.885, 95% [CI] 0.957–1.157), ALT (38.5789) (p 0.866, 95% [CI] 0.957–1.025), AST (67.2632) (p 0.196, 95% [CI] 0.978–1.050), Creatinine (5.3474) (p 0.144, 95% [CI] 0.446–1.737), and UREA (141.7895) (p 0.081, 95% [CI] 0.970–1.047).
Microbiological Characteristics
Blood culture of both anaerobic and aerobic forms was performed for most patients in the study (57.9%), a culture of soft tissue (15.8%), sputum (15.8%), and urine (10.5%) were also performed in some patients.
Seven microorganisms have shown growth in the culture, with staphylococcus aureus being the most pathogen identified in the cultures (about 52.6% of the total cases), followed by Escherichia coli (15.8%). Only one patient was isolated from extended-spectrum β-lactamases (ESBL)-producing Escherichia coli, and none of our patients were founded multiple drug resistance (MDR).
We performed an antimicrobial susceptibility profile of 12 varying antibiotic categories. Trimethoprim/sulfamethoxazole (TMP/SMX), Ampicillin, and Ceftriaxone expressed the highest resistance level, about a 100% resistance pattern against SPE pathogens disregarding a specific pathogen. On the other hand, Clindamycin, Tigecycline, Vancomycin, and amikacin revealed the overhead sensitivity rate among all microbes in about 100% of the cases. Comprehensive details about antimicrobial resistance against bacterial pathogens are shown in Table 2.
 |
Table 2 Microbiologic Features, Chest Computed Tomographic Findings, and Management of 19 Patients Diagnosed with Septic Pulmonary Emboli Between Years 2017 and 2020 |
Radiological Characteristics
Chest computed tomography (CT) scans were performed for all 19 patients, and typical characteristics for images of the pathological findings in SPE cases are presented in Figure 1. According to the location of the lesion, central distributions were the most patterns in all the patients (47.4%), followed by peripheral distribution (26.3%), while diffuse distributions were represent 26.3%.
 |
Figure 1 (A and B). Panel (A): An axial enhanced chest CT scan demonstrating Multiple predominantly solid pulmonary nodules randomly distributed throughout both lungs, some of which with central cavitations in the right side. Panel (B): An axial enhanced chest CT scan showing with multiple small peripheral cavitating pulmonary nodules with bilateral pleural effusion. |
On the other hand, as stated by the type of lesions on the chest CT, bilateral opacities were the most common radiographic type of lesions finding and were presented in all the patients (100%), followed by nodular (73.9%), cavitation (57.9%), consolidation (47.4%), non-nodular (26.3%), pleural effusion (26.3%) and Feeding vessel sign (15.8%).
Echocardiography
Transthoracic echocardiography was performed in 15 patients, and we detected significant abnormalities only in one patient, which demonstrated a large, echogenic mobile focus attached to the tricuspid valve and severe tricuspid regurgitation. Figure 2 (A&B) depicts the patient’s echocardiogram picture. None of our patients underwent transesophageal echocardiography.
 |
Figure 2 (A and B). Panel (A): A transthoracic echocardiography study of a 33 years old male revealed with a large, echogenic mobile focus attached to the tricuspid valve.Panel (B) : A transthoracic echocardiography finding demonstrated with severe tricuspid regurgitation. |
Management and Prognostic Factors for the Outcome Among Patients of SPE
After an empirical antibiotic regimen, all patients received parenteral antimicrobial therapy correlated to the culture results with duration of 5 to 10 weeks. Aside from antimicrobial treatment, the management of these patients included systemic anticoagulant (13 cases), extra-pulmonary fasciotomy and abscess drainage (three cases), and debridement (two cases).
Most of the patients (73.7%) recovered from their illness. The median duration of hospitalization was 11. 5 days (range, 3 to 69 days). A Follow-up CT scan manifested improvement following antimicrobial therapy, except for two patients who were unavailable for follow-up after discharge from the hospital. No identifiable long-term complications were resulting from SPE.
The total mortality rate for SPE patients in this study was 26% (5 patients). Logistic regression and a univariate study of clinical, predisposing, vital, and laboratory parameters were used to evaluate prognostic factors for the outcome of SPE patients. The patient’s oxygen saturation level and altered mental state were associated with a high SPE mortality rate (Table 3).
 |
Table 3 Baseline Characteristics, Univariate Analysis and Logistic Regression Analysis of Outcome Factors for 19 Patients with SPE Between Years 2017 and 2020 |
Discussion
Septic pulmonary embolism (SPE) is an unusual condition characterized by the implantation of infected thrombi into the pulmonary vasculature from a variety of infectious sources, resulting in a parenchymal infection with high morbidity and death.1,2 In this study, we point up the clinicoradiological features, microbiological spectrum, and clinical course of patients with SPE, as well as to promote the identification, diagnosis, and prognosis of this unusual disease.
Similar to previous SPE studies, the manifestations of fever, shortness of breath, cough, hemoptysis, and chest pain were the most common clinical presentations of patients with SPE in our study.3,5,9,10
One of the most extensive and early studies from china regarding SPE reported by Jiang J et al presented that 21.4% of cases of SPE were seen in the setting of Skin and other soft tissue infections secondary to nosocomial infection, in contrast to the western countries where IV drug abuse had been a common predisposing factor for SPE.11,12 GOODWIN NJ and associates reported that Infection-related to catheters inserted for diagnostic or therapeutic interventions, including hemodialysis catheter, has appeared as a common cause of SPE, along with increasing numbers of immunocompromised patients.1,13 The present study describes the importance of venous catheter-associated bloodstream infections as a fundamental source. At the same time, only one of our patients was IV drug abuse, and none of the patients were isolated septic abortion.
Various gram-negative, gram-positive bacteria and fungi are related to SPE, and the distribution of the pathogens is separate according to the studies reported. In the present study, staphylococcus aureus was the most common causative microorganism isolated from different sources of culture that are similar to the previously reported studies.3,14–16 A study from South Korea by Lee SJ et al revealed that Klebsiella pneumoniae was the most common isolated pathogen detected in culture.5
Decisions regarding selection specific antimicrobial use and duration of treatment were responsible for the pathogen detected from the culture and its antibiotic susceptibility. In the present study, Trimethoprim/sulfamethoxazole (TMP/SMX), Ampicillin, and Ceftriaxone expressed the highest resistance level, about a 100% resistance pattern against SPE pathogens, while Clindamycin, Tigecycline, Vancomycin, and amikacin revealed the overhead sensitivity rate among all microbes in about 100% of the cases.
In this study, almost one-third of the patients had Chronic renal failure (68.4%), followed by diabetic 36.8%) and hypertension (26.3%).
As suggested by Kuhlman and cook, the diagnosis of SPE can be made based on the chest CT findings, although the findings are not pathognomonic.3,9 All patients who enrolled in this study underwent chest CT during their hospitalization. Bilateral parenchymal opacities (100%), nodules (73.9%), and cavitations (57.9%) were the most common radiological manifestations in our study. In contrast to our research, pulmonary nodules were the most common chest CT feature reported by the previous studies.3,5 According to the research by Goswami and Liu et al, All patients had peripheral nodular lesions on chest CT scan, and therefore probably caused by septic occlusion of the small peripheral pulmonary arterial branches.1,2 In the studies of KWON, the detailed CT characteristics of peripheral nodules in pulmonary septic emboli may be able to differentiate the causative microorganisms and to provide additional information regarding treatment plans in patients with SPE.17,18
In the absence of adequacy of echocardiographic findings or other signs of infective endocarditis were needed for further evaluation to identify the infectious source as reported by VOS et al.19 In this study, echocardiography was performed for 15 patients. We detected significant abnormalities for only one patient found to have tricuspid valve vegetations with mitral and tricuspid regurgitation. Transesophageal echocardiography is known to provide greater spatial resolution compared to the transthoracic approach, and it is a superior method for detecting small vegetation.20
The mortality rate for SPE in the current study was 26.3% (5 patients), while the recovery rate was 73.7%.14 The probable reasons for mortality include refractory shock with resultant renal failure or grave pulmonary complications, including hemorrhage and hemoptysis. In 2013, Goswami et al described 40 patients with SPE; eight (20%) patients did not survive during hospitalization.1 Another data from MacMillan et al reported that eight patients have died from SPE with a mortality rate of 13.3%.12
Early diagnosis of an embolic phenomenon to other organ systems like the central nervous system can significantly influence a patient’s outcome, as NISHIMURA and his associates reported.21
Öz A et al demonstrated that elevated levels of plasma osmolality may have a predictive value for in-hospital mortality in acute pulmonary embolism patients.22
In the current study, the prognostic factors associated with the outcome of SPE patients included low-level oxygen saturation and altered mental status and significantly associated with a high mortality rate of SPE patients. This study suggests that microbiological and radiological findings, comorbidities, and laboratory characteristics do not affect prevalence and impact on mortality in patients with SPE. Hypotension, fungal infection, infections caused by MDRPs, severe coagulation abnormalities, and septic shock accompanied by multiple organ failure were all identified as risk factors for SPE mortality by Jiang and Ye et al, which are incompatible with the current study findings.11,23
Limitations
The retrospective aspect of this research and the selection bias involved in a single-centre study are the main limitations of our research.
Another limitation of the study is that several cases of infective endocarditis may have been missed since transthoracic echocardiography was not performed on all patients. None of them underwent transesophageal echocardiography.
Finally, due to the limited patient sample, we were unable to classify significant predictors of mortality.
Despite these limitations, our research offers the clinicoradiological features, microbiological spectrum, and clinical course on patients with SPE who do not or require critical care, as well as treatment outcomes in patients with SPE to promote the identification, diagnosis, and prognosis of this unusual disease.
Conclusion
Combining clinical suspicion with a strong knowledge of fundamental chest CT scan may allow emergency physicians to rule in and promote the identification, diagnosis, and treatment of this unusual disease.
Early diagnosis of an embolic phenomenon to other organ systems like CNS can significantly impact a patient’s outcome.
The findings of this study presented that altered mental status and low oxygen saturation are associated with a high mortality rate in patients with SPE, especially those requiring critical care.
There are a number of gaps in our knowledge around public involvement in SPE that follow from our findings, and would benefit from further research,including some of the risk factors of SPE were not mentioned in this research like HIV, aspergillosis, fungal ball and to measure the association between risk factors and SPE. Also, it is needed population based studies to evaluate the incidence and long-term outcome of SPE.
Data Sharing Statement
The data that support the findings of this study are available from Mogadishu Somali Turkish Training and Research Hospital. Data are however available from the authors upon reasonable request and with permission of Mogadishu Somali Turkish Education and Research Hospital.
Ethics Approval and Consent to Participate
We received approval from the Mogadishu Somali Turkish Training and Research Hospital review board, and written informed consent was waived (MSTH/6385) because the data was acquired retrospectively from medical records. We declare that we have followed our work center’s protocols. The privacy of the patient’s information was protected.
Acknowledgments
To a specialist at the radiology and microbiology departments who helped in reviewing of patient’s CT scan findings and culture and sensitivity pattern.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare no funding source was received for this study.
Disclosure
The authors report no competing interests in this work.
References
1. Goswami U, Brenes JA, Punjabi GV, LeClaire MM, Williams DN. Associations and outcomes of septic pulmonary embolism. Open Respir Med J. 2014;8(1):28. doi:10.2174/1874306401408010028
2. Liu S, Xie J, Chen Y, et al. Presenting features and clinical course of 34 patients with septic pulmonary embolism caused by right-sided infective endocarditis. Chin Med J. 2014;127(15):2735–2739.
3. Cook RJ, Ashton RW, Aughenbaugh GL, Ryu JH. Septic pulmonary embolism: presenting features and clinical course of 14 patients. Chest. 2005;128(1):162–166. doi:10.1378/chest.128.1.162
4. Hatani T, Takemura M, Inoue D, et al. Septic pulmonary embolism due to periodontal disease. Respirology. 2013;18(2):308–312. doi:10.1111/j.1440-1843.2012.02278.x
5. Lee SJ, Cha SI, Kim CH, et al. Septic pulmonary embolism in Korea: microbiology, clinicoradiologic features, and treatment outcome. J Infect. 2007;54(3):230–234. doi:10.1016/j.jinf.2006.04.008
6. Yang W, Lin HD, Wang LM. Pyogenic liver abscess associated with septic pulmonary embolism. J Chin Med Assoc. 2008;71(9):442–447. doi:10.1016/S1726-4901(08)70146-1
7. Stawicki SP, Firstenberg MS, Lyaker MR, et al. Septic embolism in the intensive care unit. Int J Crit Illn Inj Sci. 2013;3(1):58. doi:10.4103/2229-5151.109423
8. Mohamed AH, Mohamud MF, Mohamud HA. Epidemiology and antimicrobial susceptibility pattern of uropathogens in patients with the community-and hospital-acquired urinary tract infections at a tertiary hospital in Somalia. Jundishapur J Microbiol. 2020;13(9). doi:10.5812/jjm.107453
9. Kuhlman JE, Fishman EK, Teigen C. Pulmonary septic emboli: diagnosis with CT. Radiology. 1990;174(1):211–213. doi:10.1148/radiology.174.1.2294550
10. Yu Song X, Li S, Cao J, Xu K, Huang H, Jun Xu Z. Cardiac septic pulmonary embolism: a retrospective analysis of 20 cases in a Chinese population. Medicine. 2016;95(25):e3846.
11. Jiang J, Liang QL, Liu LH, et al. Septic pulmonary embolism in China: clinical features and analysis of prognostic factors for mortality in 98 cases. BMC Infect Dis. 2019;19(1):1–2. doi:10.1186/s12879-019-4672-1
12. MacMillan JC, Milstein SH, Samson PC. Clinical spectrum of septic pulmonary embolism and infarction. J Thorac Cardiovasc Surg. 1978;75(5):670–678. doi:10.1016/S0022-5223(19)41311-1
13. Goodwin NJ, Castronuovo JJ, Friedman EA. Recurrent septic pulmonary embolization complicating maintenance hemodialysis. Ann Intern Med. 1969;71(1):29–38. doi:10.7326/0003-4819-71-1-29
14. Lark RL, Chenoweth C, Saint S, et al. Four year prospective evaluation of nosocomial bacteremia; epidemiology, microbiology, and patient outcome. Diagn Microbiol Infect Dis. 2000;38(3):131Y–140Y.
15. Connolly J, Tarver RD, Meyer C, Winer-Muram H. Fever and patchy infiltrates: pulmonary septic emboli. Semin Respir Infect. 2002;17(1):85–88.
16. Osei C. Septic pulmonary infarction: clinical and radiographic manifestations in 11 patients. Mt Sinai J Med. 1979;46:145–148.
17. Wong KS, Lin TY, Huang YC, Hsia SH, Yang PH, Chu SM. Clinical and radiographic spectrum of septic pulmonary embolism. Arch Dis Child. 2002;87(4):312–315. doi:10.1136/adc.87.4.312
18. Kwon WJ, Jeong YJ, Kim KI, et al. Computed tomographic features of pulmonary septic emboli: comparison of causative microorganisms. J Comput Assist Tomogr. 2007;3(3):390–394. doi:10.1097/01.rct.0000243455.23308.a9
19. Vos FJ, Kullberg BJ, Sturm PD, et al. Metastatic infectious disease and clinical outcome in Staphylococcus aureus and Streptococcus species bacteremia. Medicine. 2012;91(2):86–94. doi:10.1097/MD.0b013e31824d7ed2
20. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;22:e57–e185.
21. Sexton DJ, Spelman D. Current best practices and guidelines: assessment and management of complications in infective endocarditis. Cardiol Clin. 2003;2:273–282. doi:10.1016/S0733-8651(03)00031-6
22. Öz A, Çınar T, Hayıroğlu Mİ, Avşar Ş, Keskin M, Orhan AL. The predictive value of plasma osmolality for in‐hospital mortality in patients with acute pulmonary embolism. Clin Respir J. 2019;13(3):174–183. doi:10.1111/crj.13001
23. Ye R, Zhao L, Wang C, Wu X, Yan H. Clinical characteristics of septic pulmonary embolism in adults: a systematic review. Respir Med. 2014;108(1):1–8. doi:10.1016/j.rmed.2013.10.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.