Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Prescriber Attitudes, Experiences, and Proclivities Toward Digital Medicine and How They Influence Adoption of Digital Medicine Platforms
Authors Ruetsch C ![]() , Davis T, Liberman JN
, Davis T, Liberman JN ![]() , Velligan DI
, Velligan DI ![]() , Robinson D, Jaeger C, Carpenter W, Forma F
, Robinson D, Jaeger C, Carpenter W, Forma F
Received 7 May 2021
Accepted for publication 4 November 2021
Published 16 December 2021 Volume 2021:17 Pages 3715—3726
DOI https://doi.org/10.2147/NDT.S318344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Charles Ruetsch,1 Tigwa Davis,1 Joshua N Liberman,1 Dawn I Velligan,2 Delbert Robinson,3 Chris Jaeger,4 William Carpenter,5 Felica Forma6
1Health Analytics, LLC, Columbia, MD, USA; 2Department of Psychiatry, University of Texas Health Science Center at San Antonio, San Antonio, TX, USA; 3Departments of Molecular Medicine and Psychiatry, The Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, USA; 4JHC Solutions, LLC, San Francisco, CA, USA; 5Maryland Psychiatric Research Center, University of Maryland School of Medicine, Baltimore, MD, USA; 6Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, NJ, USA
Correspondence: Charles Ruetsch
Health Analytics, LLC, 9200 Rumsey Road Suite 215, Columbia, MD, 21045, USA
Tel +1 410-997-3314
Email [email protected]
Background: Psychiatric prescribers (prescribers) typically assess medication adherence by patient or caregiver self-report. Despite likely clinical benefit of a new digital medicine technology, the role of specific prescriber attitudes, behaviors, and experiences in the likelihood of adoption is unclear.
Objective: To identify prescriber characteristics that may affect adoption of the ingestible event marker (IEM) platform.
Design: A survey of prescribers treating seriously mentally ill patients was conducted. Factor analysis was performed on 11 items representing prescriber characteristics believed to be related to endorsement of the IEM platform. Four factors were extracted. Regression analysis was used to test the strength of the relationships between the factors and likelihood of adoption of the IEM platform.
Results: A total of 131 prescribers completed the survey. Most (84%) agreed that visits allow enough time to monitor adherence. Factor analysis revealed four underlying dimensions: 1) perspectives on the value of adherence; 2) concerns about measuring adherence; 3) views toward digital health technologies; and 4) views on payer role/reimbursement. Factors 1 and 3 were related to gender, the belief that computerization benefits prescribers, the presence of office support staff, and the belief that new digital medicine (DM) technology will be cost prohibitive. Willingness to adopt the IEM platform was related to gender (p < 0.05) and perspectives on the value of adherence (p < 0.05), with those scoring higher on that measure also being more likely to adopt.
Conclusion: Psychiatric prescribers are concerned about medication adherence, perceive current monitoring tools to be problematic, and are open to using digital technologies to improve accuracy of adherence assessment. Relationships among prescriber characteristics, beliefs, and experiences should be considered when developing educational materials, particularly when the goal is to encourage adoption and use of the IEM platform.
Keywords: medication adherence, digital health technologies, antipsychotic, mental illness, personalized medicine, gender differences
Introduction
Mental illnesses are common, affecting nearly one in five, or approximately 47 million, US adults.1 Mental illness can profoundly disrupt personal and family relationships, often leads to lost worktime and reduced productivity, and, if severe, can interfere with basic activities of daily living.1–3
Serious mental illness (SMI), including major depressive disorder (MDD), bipolar disorder (BD), and schizophrenia (SZ), are often difficult to treat as they may need additional support compared to patients with other disorders4,5 potentially escalating healthcare costs.6–9
One of the major drivers of increased healthcare costs is relapse, which is partially due to medication non-adherence.10–12 As psychiatric pharmacotherapeutic effectiveness often depends upon consistent long-term medication use, an accurate and timely assessment of medication non-adherence is beneficial.13 Medication adherence is difficult to assess in general, but may be even more challenging in psychiatry,14 where prescribers tend to overestimate their patients’ medication adherence15–17 and use assessment methods that are unreliable, which can result in treatment decisions that are ill-informed. By contrast, when presented with credible medication adherence information, prescribers may alter their prescribing patterns and treatment decisions to consider their patients’ level of medication compliance.18
The current rise of digital health technologies offers important prospects to transform therapeutics to digital personalized medicine (DPM), and by extension, increase our capacity to measure patient outcomes in the real world, in real time.19 Ingestible event marker (IEMs) are perhaps the most advanced technology available to help prescribers discern between medication non-adherence and medication ineffectiveness when considering treatment modification for patients whose symptoms are not well controlled.20 Antipsychotic IEM systems consist of an ingestible sensor embedded within an oral medication, a wearable sensor patch, an application on a mobile device, and portal for healthcare professionals and caregivers.21 The ingestible sensor is activated upon contact with the patient’s gastric fluid21 and transmits a signal to the wearable sensor patch as it passes through the alimentary canal. From the patch, a secure digital record is sent to a cloud-based application on the patient’s mobile device via Bluetooth®.21 The application records the date and time of medication ingestion, activity and rest, as well as self-reported data such as mood and sleep quality. All data are then transmitted to the physician as well as authorized family members or other caregivers.22,23
While use of an IEM system could potentially facilitate improved patient care, the medical profession, and psychiatry in particular, has historically delayed uptake of digital tools.24,25 Further, little data are available to support how to discern who will adopt adherence monitoring and reporting systems such as the IEM and what the drivers of and barriers to adoption might be. Hatch et al reported that enthusiasm for digital platforms, training, and financial drivers would be influential in prescriber decisions to adopt the technology.26 In contrast, barriers to adoption range from concern over reimbursement, the ability to integrate the technology into usual care, the potential for increased liability, and other logistical challenges.26
The objectives of this research were to identify potential barriers and drivers of adoption of digital medicine technologies and to assess if barriers and drivers aggregate into dimensions that could provide insight into the broader set of clinical priorities that influence digital medicine technology adoption.
Methods
Study Design
The study was a cross-sectional online survey, conducted between April and October 2019, of clinicians with prescribing authority (psychiatrists and advanced practice registered nurses), residing in the US who treat patients with MDD, BD, or SZ.
Identification and Selection of Study Participants
Potentially eligible participants were identified from national lists of psychiatric prescribers and invited to participate by email. Eligible participants met each of the following criteria:
US licensed medical doctor (MD) and Board-certified Psychiatrist by the American Board of Psychiatry and Neurology, or US licensed Doctor of Osteopathic Medicine (DO) and Board Certified by the American Osteopathic Board of Neurology and Psychiatry, or Advanced Practice Registered Nurse or nurse practitioner or clinical nurse specialist (collectively referred to as NP). Each participant was required to have treated at least 10 patients per month within the US with one of the following mental illnesses: MDD, BD, and SZ.
Prescribers reported the number of patients with MDD, BD, or SZ within their patient panel as well as their National Provider Identifier (NPI) number. Patient panel information was used to assign prescribers to one of three response groups based on the primary diagnosis in their practice. All remaining questions were specific to the diagnosis group to which they were assigned.
Questionnaire Design and Development
The questionnaire was developed by a steering committee comprised of experts in psychometrics, psychiatric treatment, psychiatric research and evaluation, and digital medicine. The first step in questionnaire development was identification of measurement domains. Review of literature, existing questionnaires, and expert guidance were all used. The domains were developed to assess specific relevant barriers to and drivers of adoption of a new digital technology designed to assess and monitor patient adherence with ingestion of oral psychiatric medication. The final list of domains included:
- Beliefs about medication adherence,
- Experience and confidence with digital technology in clinical practice,
- Perceived impact of adherence management and technology adoption on practice efficiency,
- Concerns about liability and responsibility,
- Belief about the effect of being monitored, and
- Incentives to digital medicine technology adoption.
Items for the demographics domain (age, gender, etc.) were taken from existing questionnaires, while manifest items for each of the measurement domains were generated by the steering committee with input from relevant content experts and the psychometrician. The final item set included 117 questions, of which 104 were generated by the steering committee. Of the 117 questions, 37 were Likert (4-point scale), 26 rank, 21 objective response, 19 dichotomous, and 14 were open-text. Items were assembled into a pilot instrument with instruction sets and relevant response fields. Also included in the questionnaire, prior to questions concerning barriers and drivers of IEM platform adoption, was a description of the IEM platform (Appendix A). Endorsement for each barrier to and driver of IEM adoption were captured on a four-point Likert scale consisting of the options “strongly agree,” “somewhat agree,” “somewhat disagree,” and “strongly disagree.” Additionally, other barriers and drivers were part of a rank order item format. Participants were requested to rank order items based on the importance to their decision-making or their possible adoption of the IEM technology. The combination of rank order of specific related barriers and drivers as well as the Likert scale of agree to disagree was used as the primary data for estimating the presence and strength of barriers to and drivers of adoption of the IEM technology for each participant.
A pilot test and cognitive debriefing interview were conducted on a sample of five psychiatric prescribers to better understand the survey instruction sets, items, and responses. Data captured on the debrief form were compiled and presented to the steering committee where final revisions were made to the instructions, items, and response arrays.
Recruitment
Psychiatric prescribers, including those identified from professional associations and previous study participants, were recruited via email invitation which included a hyperlink to the online survey. The online survey employed a user-friendly point-and-click interface for the informed consent as well as all questionnaire items and response arrays. Eligible participants were remunerated $175 for completing the survey. Additionally, prescribers who participated in the pilot survey and cognitive debriefing interview received $275 ($175 for the survey, $100 for the debriefing interview). Prior to initiating the questionnaire, all participants were presented with an online informed consent document that was reviewed and approved by Advarra IRB. The guidelines outlined in the Declaration of Helsinki were followed and the research protocol, questionnaire, and informed consent statement and process were reviewed and approved by the Advarra Institutional Review Board.
Statistical Analysis
Independent variables, including prescriber age, gender, level of clinical experience (years), practice type, and degree type, were summarized descriptively; frequencies and percentages were reported for categorical variables, while means and standard deviations were reported for continuous variables. For ease of interpretation, the frequency distribution of the four-point Likert scale were dichotomized into two-point scales consisting of “agree” and “disagree.” The original four-level responses were retained for other analyses. An exploratory factor analysis was performed on 11 items representing prescriber opinions, attitudes, and experiences believed to be related to likelihood of endorsement of the IEM platform (Appendix B). Principal components were examined and rotated using direct oblimin methodology with Kaiser normalization, allowing the items and factors to correlate. The final factors were characterized as underlying dimensions influencing willingness to adopt DM in general and the IEM platform specifically. Factors were correlated with questionnaire items indicating attitudes, experiences, beliefs, prescriber demographics, and work setting. For significance testing, differences in average factor scores were calculated between groups for the following independent variables: gender, prescriber type (physicians vs advance practice nurses), primary disease treated, as well as the attitudinal questions concerning barriers to widespread adoption of DM, which constituents benefit most from DM (ie, prescribers, payors, or patients), and barriers within their own practices (eg, availability of support staff, single or multispecialty office). Also, group differences were computed among those who indicated desire to be a beta site for the IEM platform and those who did not. Finally, the variable indicating a desire to be a beta site for the IEM platform was modeled as a proxy for endorsement enthusiasm. Desire to be a beta site was regressed onto a model that included provider characteristics as covariates (age and gender), degree (MD & DO vs NP), primary disorder (SC, BD, or MDD), and the predictors of interest. Tests of significance for observed differences among groups were conducted using chi-square tests for categorical variables and t-tests or ANOVA for continuous variables. The regression model was Ordinary Least Square (OLS). The R2 was tested using an F-test, and beta weights were tested using t-test of significance. The threshold for significance was set at 0.05. All analyses were conducted with SPSS V24 (IBM, Armonk, NY).
Results
Prescriber Characteristics
A total of 131 prescribing providers participated in the survey (Table 1). The prescribers were 79.4% physicians, 20.6% advanced practice registered nurses, 56.5% female, with an average age of 47.5 years. Forty-one percent practiced in the southern United States. The average time practicing was 17 (SD=12.2) years. The largest group of prescribers worked in an individual practice setting and a minority (19.1%) worked in multispecialty settings.
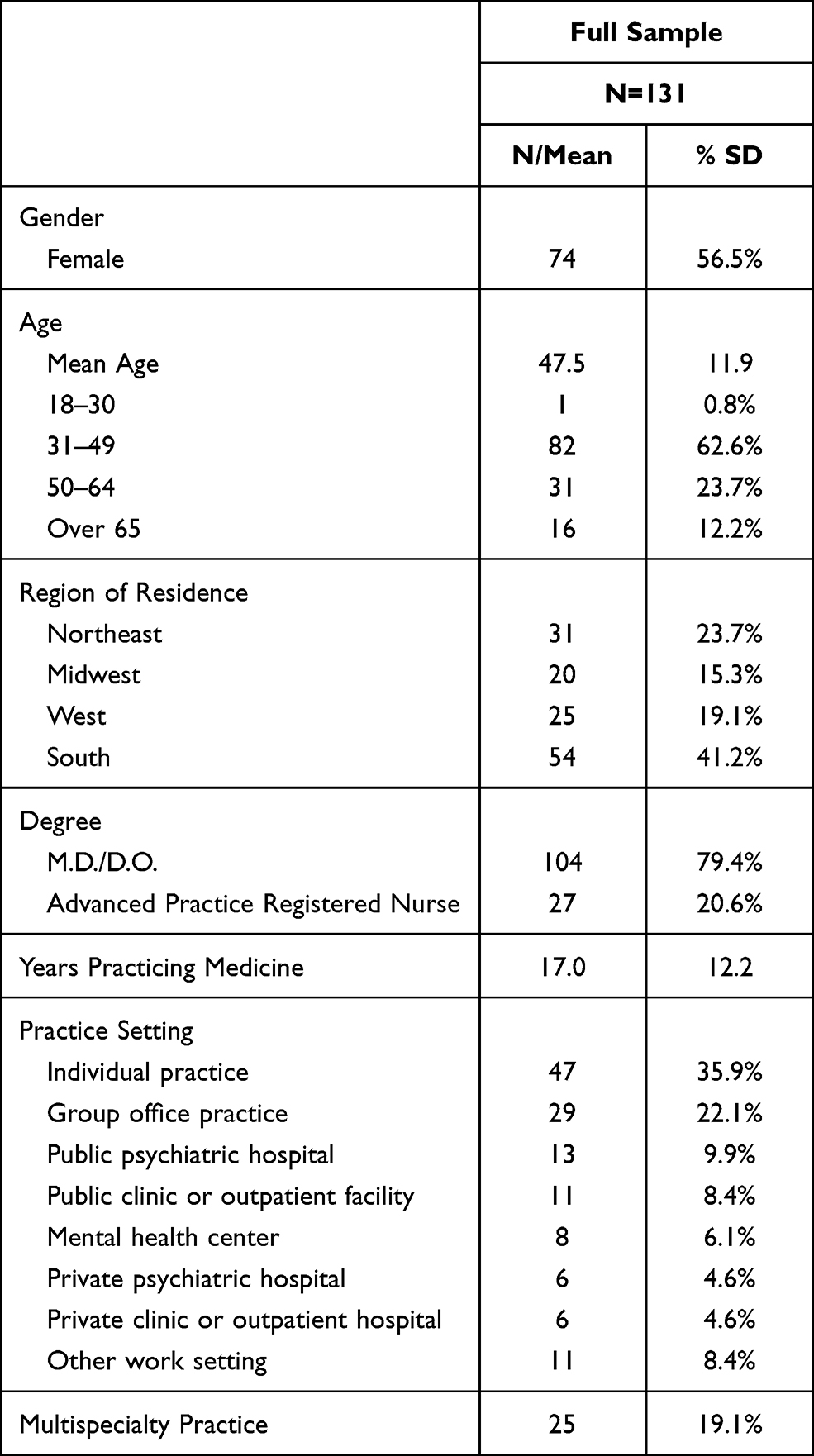 |
Table 1 Prescriber Characteristics |
Perspectives on Adherence
The majority of prescribers (84.0%) reported adequate time to assess medication adherence, while only 66.4% reported confidence in accurately estimating patient-specific adherence (Table 2). Most prescribers (91.6%) were concerned about the validity of self-reported adherence, and prescribers providing care for BD and SZ patients were significantly more concerned than those providing care for MDD patients (95.7% and 97.4% vs 82.6%; p < 0.05). Most (67.2%) reported concern about their ability to adequately monitor adherence, but this concern varied significantly by patient population, with the highest level of concern reported about patients with SZ (84.6%), followed by BD (73.9%) and MDD (45.7%) (p < 0.05).
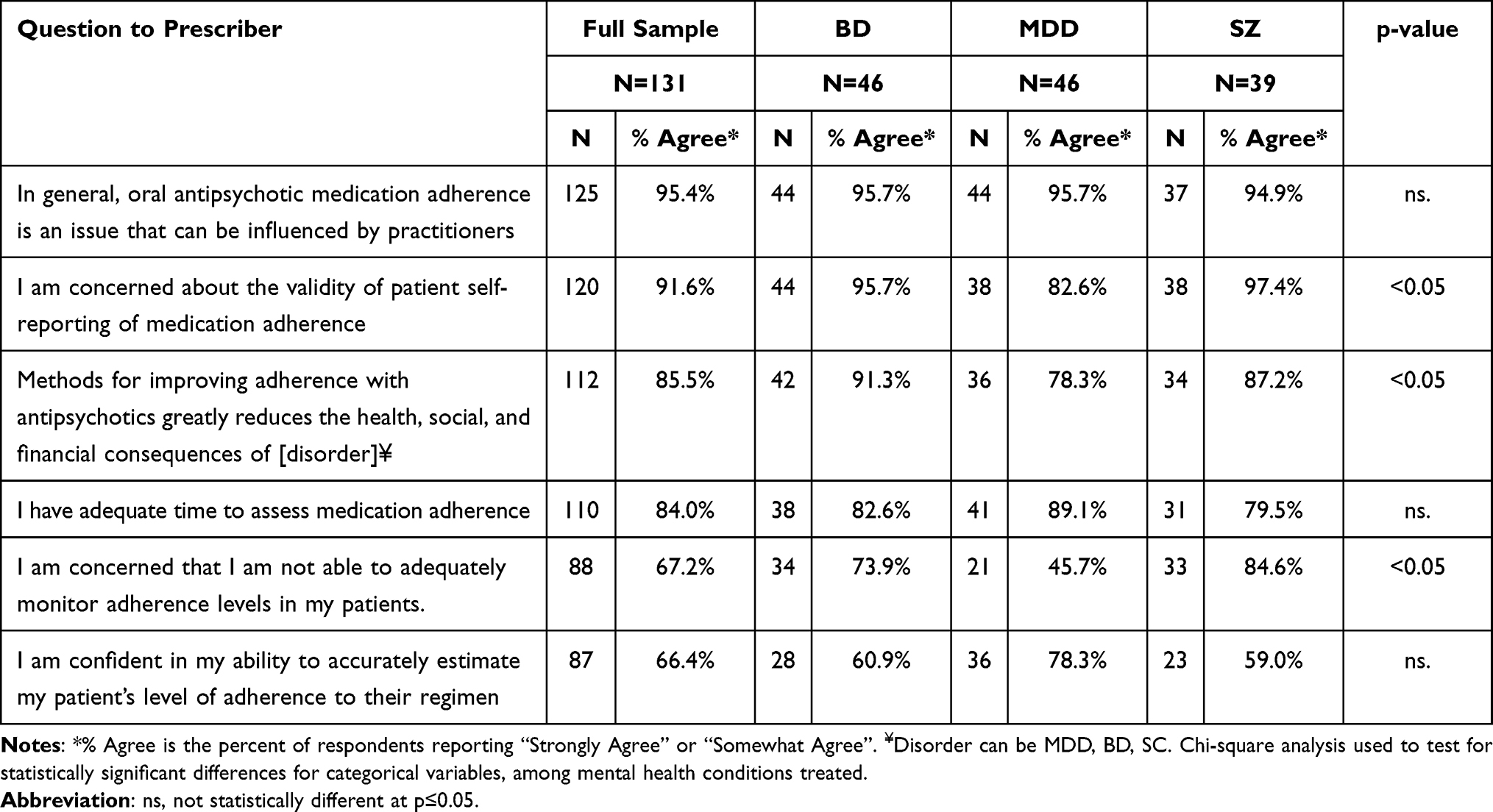 |
Table 2 Prescriber Perspectives on Managing Medication Adherence, Overall and by Mental Health Condition Managed |
Nearly all (95.4%) prescribers believed that oral antipsychotic medication adherence can be influenced by them or another practitioner and most (85.5%) reported that methods for increasing medication adherence would greatly decrease health, social, and financial consequences with the greatest percentage of them treating BD (91.3%) compared to SZ (87.2%) and MDD (78.3%).
Perspectives on Digital Health and the IEM Solution
In general, prescribers believed that an IEM solution would be beneficial to their patients. Specifically, 77.9% of prescribers agreed that an IEM would improve clinical outcomes (Table 3) and 75.5% agreed that the device was in their patients’ best interest. Nearly two-thirds of prescribers (64.9%) reported that an IEM solution would “enhance” the clinical alliance with their patients, while 35.1% reported that it would “erode” their clinical alliance. Overall, 71.8% reported the solution would increase patient engagement with their treatment.
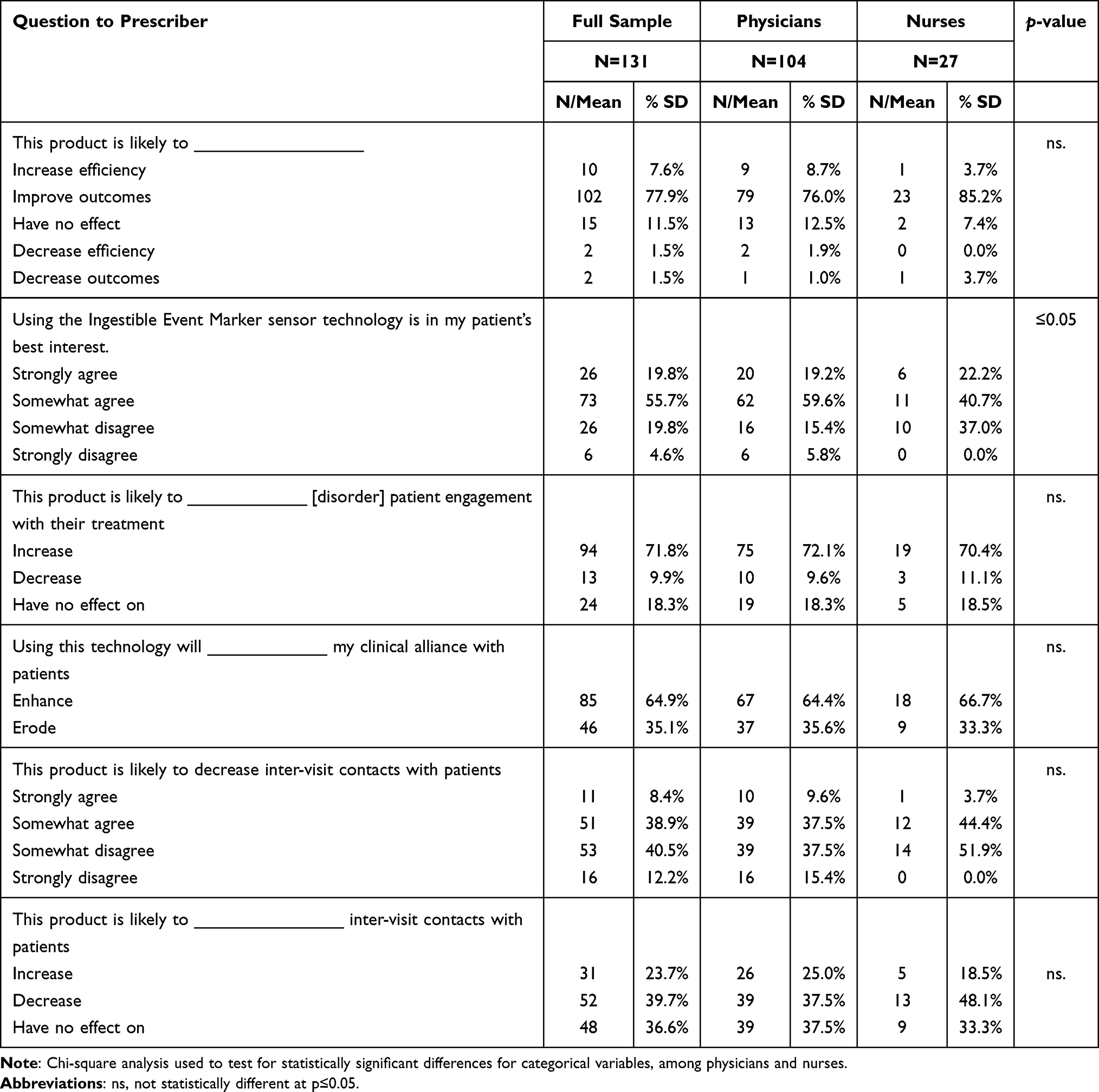 |
Table 3 Prescriber Perspectives on the IEM Technology |
Eleven items (Table 4, Appendix B) representing prescriber opinions, attitudes, and experiences believed to be related to likelihood of endorsement of the IEM platform were analyzed using exploratory factor analysis. Examination of the principal components revealed 5 components with eigenvalues over 1.0. However, the fifth component’s eigenvalue was 1.087 and accounted for less than 10% of the total variance. Also, examination of the scree plot (Figure 1) indicated a clear notch in the eigenvalue curve at the fourth component. Retaining 4 principal components accounted for 61.89% of the total variance. Therefore, a four-factor model was computed, and oblique rotation produced an adequate solution within 19 iterations. The structure matrix (Table 4) reveals four clear factors with manifest indicators all having loadings over 0.6: Factor 1: perspectives on the value of adherence; Factor 2: concerns about measuring adherence; Factor 3: views toward digital health technologies; and Factor 4: views on payer role/reimbursement.
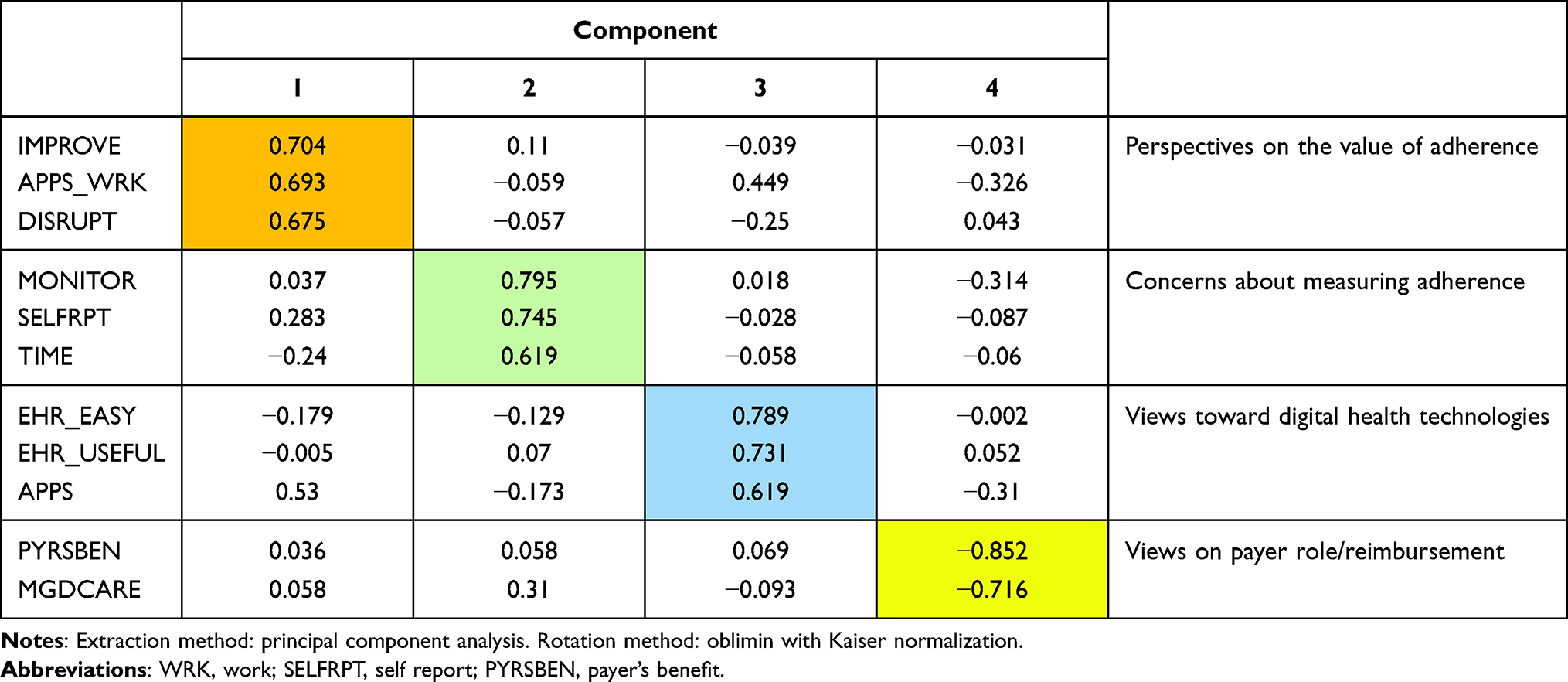 |
Table 4 Factor Structure Matrix |
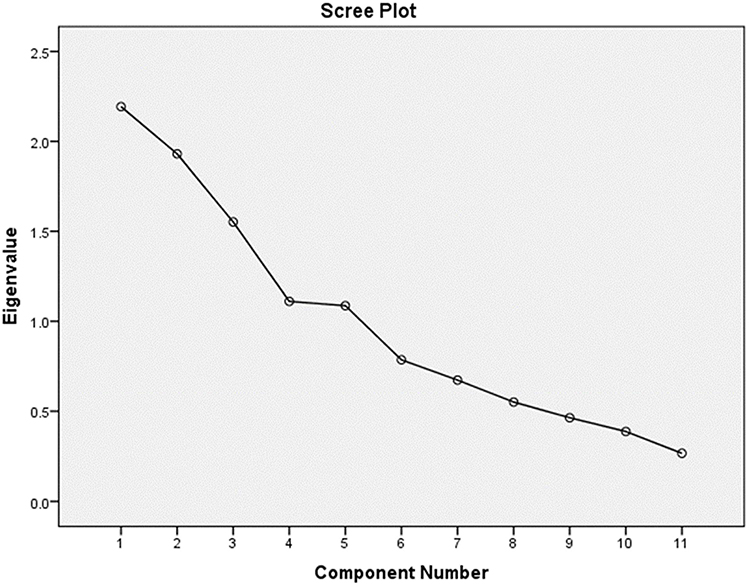 |
Figure 1 Scree plot illustrating eigenvalues (y-axis) and the number of factors (x-axis) that should be generated. The slope of the scree plot begins to level following the fourth factor, indicating a four-factor solution is optimal for the analysis. |
To characterize the underlying dimensions measured by the four factors, relationships among the factors and questionnaire items indicating attitudes, experiences, beliefs, prescriber demographics, and work setting were calculated (Table 5). Groups that scored higher on Factor 1: perspectives on the value of adherence included women, those who believe that computerization benefits prescribers, and those who have office staff to aid in prior authorization. Conversely, those who believe that new DM technology will be cost prohibitive scored lower on Factor 1 (p < 0.05). Those with higher scores on Factor 3: views toward digital health technologies were more likely to be female, those who believe that computerization benefits prescribers, those who were disrupted 5 or fewer hours per week when the current EMR was first installed, and those who work in a multispecialty practice. By contrast, lower scores on Factor 3 were related to belief that new DM technology will be cost prohibitive, and that computerization does not necessarily benefit payers (p < 0.05). Finally, willingness to be a beta test site for the IEM platform was positively correlated (Table 6) with Factor 1: perspectives on the value of adherence and Factor 2: concerns about measuring adherence (p < 0.05). Similarly, belief that using the IEM platform is in the patient’s best interest is correlated with Factor 1: perspectives on the value of adherence (p < 0.05).
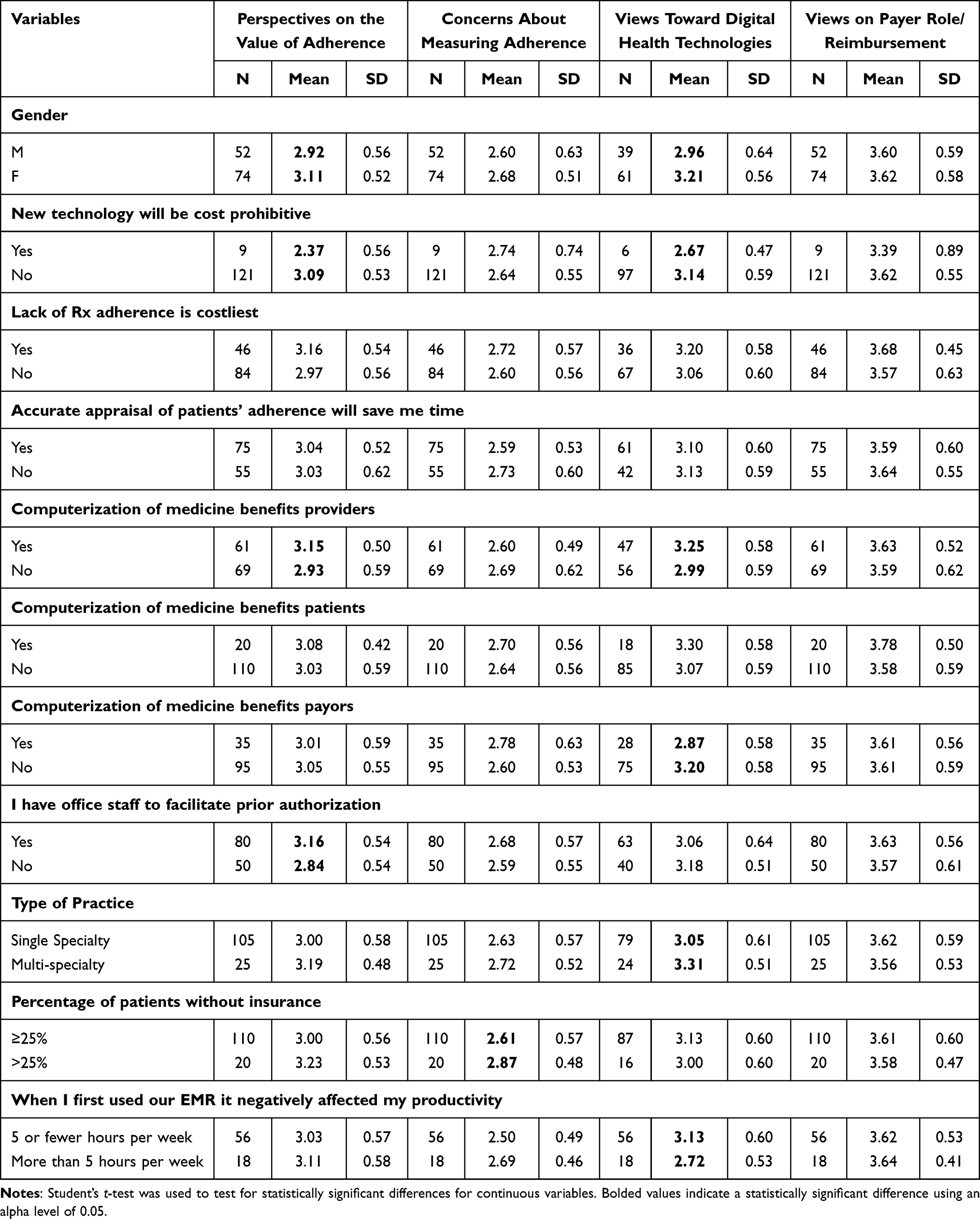 |
Table 5 Descriptive Statistics |
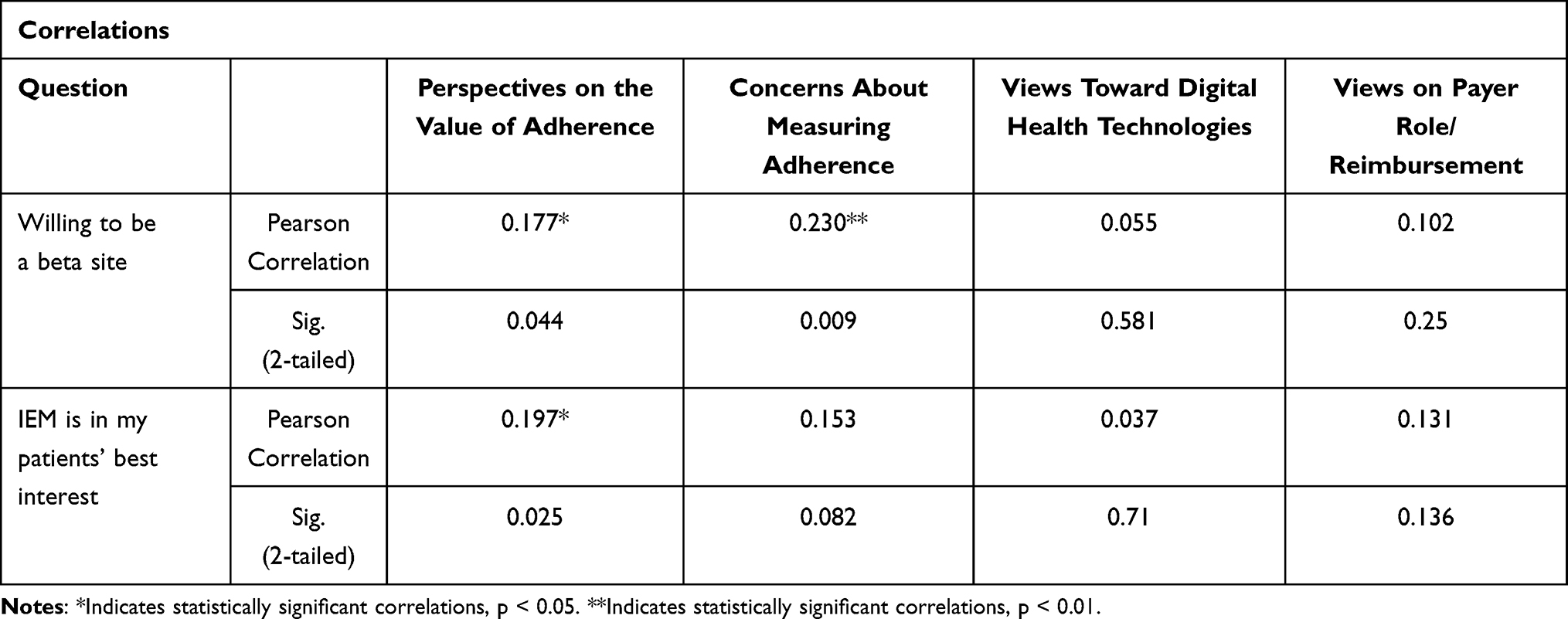 |
Table 6 Correlation Matrix |
Regression analysis was used to further examine prescriber dimensions related to adoption of an IEM platform. Willingness to be a beta site for the IEM platform was used as a proxy measure for willingness to adopt the platform. Independent variables were selected from the bivariate results and included prescriber characteristics (age and gender, degree), belief that the current EHR system reduced productivity when first installed, and the four underlying factors. The model significantly predicted the proxy for platform adoption (R2 = 0.239, p < 0.05). Significant predictors were gender (females more likely to endorse IEM, p < 0.05) and Factor 1: perspectives on the value of adherence (p < 0.05) with those scoring higher on Factor 1 also more likely to report wanting to be a beta site for the platform (Table 7).
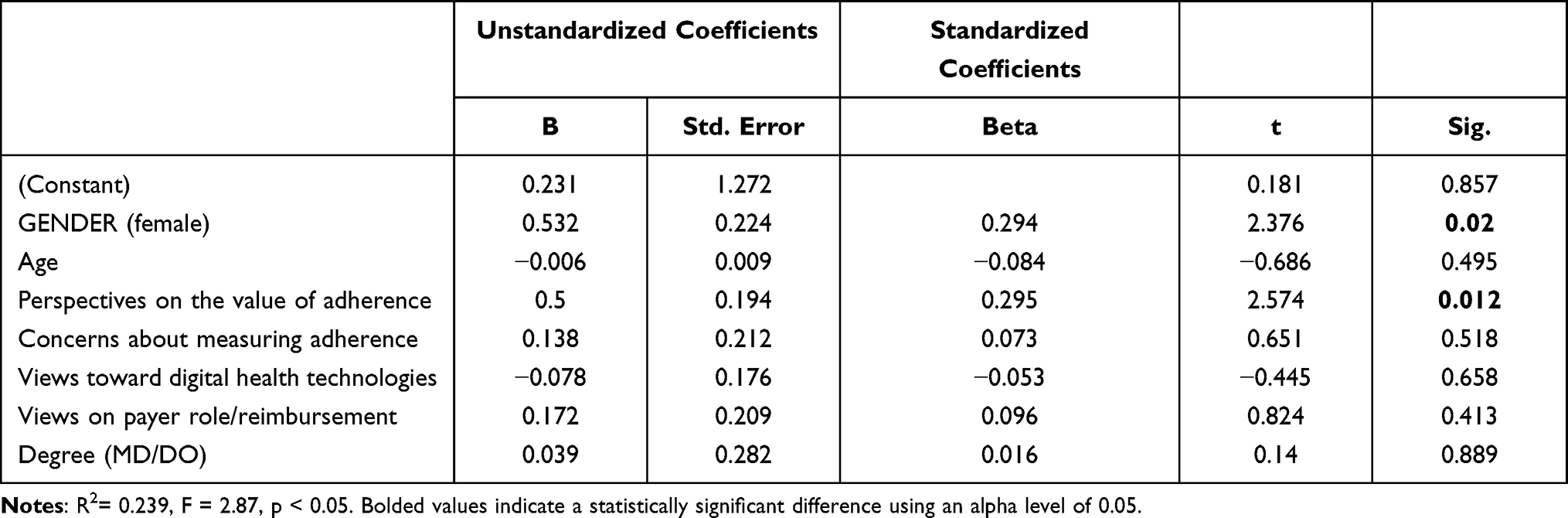 |
Table 7 Ordinary Least Squares Regression Coefficients: Predicting Willingness to Be a Beta Site |
Discussion
The digitalization of medicine (including healthcare IT, apps, software as a medical device (SaMD), wearables, sensors, therapeutics with an ingestible sensor and more) is the future of healthcare, and digital health technology research, development and adoption is rapidly increasing.27–29 Digitalization provides real-time, or near real-time, health information, reduces inefficiencies, improves patient access, reduces cost of care, increases quality of care, can improve outcomes, and makes medicine more personalized for patients.30–32 While digital technologies and medicine hold great promise, healthcare providers may be reluctant to adopt these technologies due to concerns over patient data security, their responsibility when using digital technologies, or their competence with the technology.32
The high rate of medication nonadherence among psychiatric patients combined with psychiatric prescribers’ tendency to overestimate their patients’ level of adherence to medication17 is a contributor to elevated health service utilization and potentially avoidable costs.33 Digital health technologies that provide prescribers with accurate adherence information can help to address these issues. The purpose of this study was to use prescriber reaction to the IEM platform to develop a general model of the decision process used by psychiatric providers when considering adoption of digital technologies that assist in the assessment of patient adherence to medication.
Used as the stimulus in this assessment of barriers and drivers, the IEM platform records the date and time of medication ingestion and offers prescribers timely information on their patients’ medication adherence to potentially improve treatment and prescribing decisions.18 Though most prescribers reported having adequate time and resources to assess and to influence their patients’ adherence to medications, fewer expressed confidence in their ability to accurately assess their patients’ adherence (Table 2). They also expressed that the IEM platform would be beneficial, improve outcomes, and be in their patient’s best interest (Table 3). Taken together, these results indicate prescriber endorsement of an IEM device or similar platform.
Additionally, we measured prescriber opinions, attitudes, and experiences believed to be related to the likelihood of endorsement of the IEM platform. Eleven questionnaire items indicating the level of ease using their current EHR system and its utility, experience, and judgment of the utility of digital apps in medicine, experience with and attitudes toward assessing their patient’s level of adherence, and the responsibility that managed care ought to have in prescriber assessment of patient medication adherence were factor analyzed. A four-factor model emerged from an exploratory factor analysis of these 11 items.
Relationships among the four factors and other items on the questionnaire revealed insights about their meaning, particularly concerning a prescriber’s decision process when considering endorsement of the IEM platform. Bivariate relationships revealed that two of the factors (Factor 1 and Factor 3) had several significant relationships to other prescriber characteristics, attitudes, beliefs, and experiences. Women, those who believe that computerization benefits prescribers, and those with office support staff are more positive about the value of assessing adherence, while those who believe that digital medicine is cost prohibitive were weaker in this belief. Similarly, women and those who believe that computerization benefits prescribers had more positive views toward digital health technologies in medicine, while those believing digital technology to be cost prohibitive were less positive. The regression analysis confirmed some, but not all, of these relationships in multivariate space. Women and those more positive about the value of adherence monitoring were more likely to endorse the proxy measure of willingness to adopt the IEM platform.
Studies examining gender differences in the adoption of mHealth, and digital technologies are limited, and results are inconsistent. Studies by Zhang et al34 and Illiger et al35 found that men are more likely to adopt mHealth solutions, while recent data published by Doximity show that women are adopting telehealth solutions 25% more than their male colleagues.36 The underpinnings of the gender differences presented here will require further study, however, prescriber endorsement of a digital technology often involves a belief that the device is a good fit for the prescriber and their patient population, results in better collaboration and transparency, streamlines daily workflow, empowers the clinician and provides an improved quality of care for the patient.30–32
Finally, the current results suggest specific prescriber characteristics and knowledge gaps that may be useful in tailoring educational programs focused on using digital applications to monitor medication adherence, potentially making them more interesting. For example, educational materials could reinforce the rationale for monitoring medication adherence, as well as expose prescribers to the value of digital apps for men and for those who believe that digital medicine is cost prohibitive. By contrast, those with office support staff or who believe that computerization is helpful may be less interested in the rationale for monitoring adherence and already accept that digital apps can be helpful in medicine.
Study Limitations
This study had several limitations that should be considered when interpreting the results. First, sample size was limited, and respondents represented a convenience sample, which may limit generalizability based on respondent age, and degree distribution. Second, respondents did not have an ability to interact directly with, or test, the IEM sensor technology; rather, the device was described within the questionnaire. Third, the respondents self-reported which may have introduced bias.
Conclusions
Psychiatric providers are concerned about medication adherence, perceive current monitoring tools to be problematic, and are open to using digital medicine technologies to improve accuracy of adherence assessment. Gender, belief that computerization benefits prescribers, belief that digital medicine is cost prohibitive, presence of office support staff, and type of practice (single v. multispecialty) are all related to the two underlying dimensions: perspectives on the value of adherence and views toward digital health technologies. Regression analysis indicated that gender and perspectives on the value of adherence were related to willingness to be a beta site for the IEM platform, a proxy for willingness to adopt it. Relationships between prescriber characteristics, beliefs, experiences, and the underlying dimensions that influence the decision to adopt the IEM platform could be used to tailor educational materials to the specific knowledge needs and interests of prescribers who wish to know more about the use of digital tools to monitor medication adherence.
Article Highlights
- Even if they have adequate time to assess their patients’ adherence to medications, fewer prescribers have confidence in their ability to accurately assess it.
- Educational materials designed to increase likelihood of adoption of the DMS could reinforce the rationale for monitoring medication adherence.
- By contrast, those with office support staff or who believe that computerization is helpful may not need the rationale for monitoring adherence to increase adoption.
Social Media Contents
Survey of 131 psychiatric care clinicians delivers key insights to help guide adoption of digital medicine in clinical practice.
Acknowledgments
The authors wish to thank Sara Heverly-Fitt for her project management and analytic support and Margaret L Stinstrom for her administrative support.
Funding
Financial support for this study was provided entirely by a contract with Otsuka Pharmaceutical Development & Commercialization, Inc. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Disclosure
Dr Charles Ruetsch reports grants, personal fees from Otsuka America, during the conduct of the study; personal fees from Pear Therapeutics for consulting on digital therapeutics, involved in HEOR Project in the area of major depressive disorder for Janssen Scientific Affairs and Acadia Pharmaceuticals, personal fees from Atentiv for consulting on digital therapeutic HEOR evidence generation plan, outside the submitted work. Dr Tigwa Davis reports personal fees from Otsuka America Pharmaceutical, Inc., during the conduct of the study. Dr Joshua N Liberman reports funding from Otsuka Pharmaceutical Development & Commercialization, Inc. for his affiliation, Health Analytics LLC research services. Dr Dawn I Velligan reports non-financial support for consultant speaker’s bureau and manuscript preparation from Otsuka, during the conduct of the study; advisory board for Lindra, Alkermes, Janssen, and Otsuka, outside the submitted work. Dr Delbert Robinson reports personal fees from Health Analytics, during the conduct of the study; personal fees and/or grants from Otsuka and Lundbeck, outside the submitted work. Dr William Carpenter reports personal fees from Boehringer Ingelheim for data management and safety board, personal fees from Tiva for presentation, personal fees from Lundbeck as an advisor, outside the submitted work. Felicia Forma is an employee of Otsuka Pharmaceutical Development & Commercialization, Inc. The authors report no other conflicts of interest in this work.
References
1. Mental illness; 2019. Available from: https://www.nimh.nih.gov/health/statistics/mental-illness.shtml.
2. Fadden G, Bebbington P, Kuipers L. The burden of care: the impact of functional psychiatric illness on the patient’s family. Br J Psychiatry. 1987;150:285–292. doi:10.1192/bjp.150.3.285
3. Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA. 2003;290(18):2443–2454. doi:10.1001/jama.290.18.2443
4. Fava M, Kendler KS. Major depressive disorder. Neuron. 2000;28(2):335–341. doi:10.1016/S0896-6273(00)00112-4
5. Griswold KS, Pessar LF. Management of bipolar disorder. Am Fam Physician. 2000;62(6):
6. Gibson TB, Jing Y, Smith Carls G, et al. Cost burden of treatment resistance in patients with depression. Am J Manag Care. 2010;16(5):370–377.
7. Greenberg P, Corey-Lisle PK, Birnbaum H, Marynchenko M, Claxton A. Economic implications of treatment-resistant depression among employees. Pharmacoeconomics. 2004;22(6):363–373. doi:10.2165/00019053-200422060-00003
8. Ivanova JI, Birnbaum HG, Kidolezi Y, Subramanian G, Khan SA, Stensland MD. Direct and indirect costs of employees with treatment-resistant and non-treatment-resistant major depressive disorder. Curr Med Res Opin. 2010;26(10):2475–2484. doi:10.1185/03007995.2010.517716
9. Begley CE, Annegers JF, Swann AC, et al. The lifetime cost of bipolar disorder in the US: an estimate for new cases in 1998. Pharmacoeconomics. 2001;19(5 Pt 1):483–495. doi:10.2165/00019053-200119050-00004
10. Keck PE
11. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. doi:10.1001/archinte.160.14.2101
12. Ta JT, Sullivan SD, Tung A, Oliveri D, Gillard P, Devine B. Health care resource utilization and costs associated with nonadherence and nonpersistence to antidepressants in major depressive disorder. J Managed Care Specialty Pharm. 2021;27(2):223–239. doi:10.18553/jmcp.2021.27.2.223
13. Yen CF, Chen CS, Ko CH, et al. Relationships between insight and medication adherence in outpatients with schizophrenia and bipolar disorder: prospective study. Psychiatry Clin Neurosci. 2005;59(4):403–409. doi:10.1111/j.1440-1819.2005.01392.x
14. Berk L, Hallam KT, Colom F, et al. Enhancing medication adherence in patients with bipolar disorder. Hum Psychopharmacol. 2010;25(1):1–16. doi:10.1002/hup.1081
15. Byerly M, Fisher R, Whatley K, et al. A comparison of electronic monitoring vs. clinician rating of antipsychotic adherence in outpatients with schizophrenia. Psychiatry Res. 2005;133(2–3):129–133. doi:10.1016/j.psychres.2004.11.002
16. Murri R, Ammassari A, Trotta MP, et al. Patient-reported and physician-estimated adherence to HAART: social and clinic center-related factors are associated with discordance. J Gen Intern Med. 2004;19(11):1104–1110. doi:10.1111/j.1525-1497.2004.30248.x
17. Stephenson JJ, Tunceli O, Gu T, et al. Adherence to oral second-generation antipsychotic medications in patients with schizophrenia and bipolar disorder: physicians’ perceptions of adherence vs. pharmacy claims. Int J Clin Pract. 2012;66(6):565–573. doi:10.1111/j.1742-1241.2012.02918.x
18. Shafrin J, May SG, Shrestha A, et al. Access to credible information on schizophrenia patients’ medication adherence by prescribers can change their treatment strategies: evidence from an online survey of providers. Patient preference adherence. 2017;11:1071–1081. doi:10.2147/PPA.S135957
19. Özdemir V. The changing face of personalized medicine and clinical pharmacology with digital drugs and real-time pharmacodynamics. Omics. 2020;24(4):173–174. doi:10.1089/omi.2020.0035
20. Lee DJ, Farchione TR, Mathis MV, Muniz J, Muoio BM. US Food and Drug Administration’s approval of aripiprazole tablets with sensor: our perspective. J Clin Psychiatry. 2018;79(3). doi:10.4088/JCP.18com12255
21. Otsuka Pharmaceutical Co. L. Prescribing Information - Abilify MYCITE (aripiprazole tablets with sensors); 2017.
22. Plowman RS, Peters-Strickland T, Savage GM. Digital medicines: clinical review on the safety of tablets with sensors. Expert Opin Drug Saf. 2018;17(9):849–852. doi:10.1080/14740338.2018.1508447
23. Belknap R, Weis S, Brookens A, et al. Feasibility of an ingestible sensor-based system for monitoring adherence to tuberculosis therapy. PLoS One. 2013;8(1):e53373. doi:10.1371/journal.pone.0053373
24. Nicholas JHK, Larsen ME, Basu A, Batterham PJ, Shaw F, Sendi S. Issues for eHealth in psychiatry: results of an expert survey. J Med Internet Res. 2017;19(2):e55. doi:10.2196/jmir.6957
25. International R. Behavioral health roundtable: using information technology to integrate behavioral health and primary care.
26. Hatch A, Hoffman JE, Ross R, Docherty JP. Expert consensus survey on digital health tools for patients with serious mental illness: optimizing for user characteristics and user support. JMIR Mental Health. 2018;5(2):e46. doi:10.2196/mental.9777
27. Cao J, Lim Y, Sengoku S, Guo X, Kodama K. Exploring the shift in international trends in mobile health research from 2000 to 2020: bibliometric analysis. JMIR mHealth auHealth. 2021;9(9):e31097. doi:10.2196/31097
28. Harbeck N. Digitalization in medicine: it is our chance and responsibility now to shape the digital future of breast cancer management. Breast Care. 2019;14(3):128–129. doi:10.1159/000501185
29. Association AM. AMA digital health research - physicians’ motivations and requirements for adopting digital health - adoption and attitudinal shifts from 2016 to 2019. American Medical Association; 2020.
30. (FDA) USFaDA. What is digital health?; 2020. Available from: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health.
31. Bruce CR, Harrison P, Nisar T, et al. Assessing the impact of patient-facing mobile health technology on patient outcomes: retrospective Observational Cohort Study. JMIR mHealth auHealth. 2020;8(6):e19333. doi:10.2196/19333
32. Gagnon M-P, Ngangue P, Payne-Gagnon J, Desmartis M. m-Health adoption by healthcare professionals: a systematic review. J Am Med Inf Assoc. 2015;23(1):212–220. doi:10.1093/jamia/ocv052
33. Gilmer TP, Dolder CR, Lacro JP, et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am J Psychiatry. 2004;161(4):692–699. doi:10.1176/appi.ajp.161.4.692
34. Zhang X, Guo X, Lai KH, Guo F, Li C. Understanding gender differences in m-health adoption: a modified theory of reasoned action model. Telemed j e-Health. 2014;20(1):39–46. doi:10.1089/tmj.2013.0092
35. Illiger K, Hupka M, von Jan U, Wichelhaus D, Albrecht UV. Mobile technologies: expectancy, usage, and acceptance of clinical staff and patients at a university medical center. JMIR mHealth auHealth. 2014;2(4):e42. doi:10.2196/mhealth.3799
36. Pecci A. Female physicians more likely to adopt telehealth; 2020. Available from: https://www.healthleadersmedia.com/innovation/female-physicians-more-likely-adopt-telehealth.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.