Back to Journals » Journal of Inflammation Research » Volume 15
Preoperative White Blood Cell-Related Indicators Can Predict the Prognosis of Patients with Transurethral Resection of Bladder Cancer
Authors Gao M ![]() , Yang Q
, Yang Q ![]() , Xu H, Chen Z, Wang X
, Xu H, Chen Z, Wang X ![]() , Guo H
, Guo H
Received 19 May 2022
Accepted for publication 7 July 2022
Published 21 July 2022 Volume 2022:15 Pages 4139—4147
DOI https://doi.org/10.2147/JIR.S373922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Mingde Gao1 *, Qiuxing Yang2 *, Haifei Xu,1 Zhigang Chen,1 Xiaolin Wang,1 Haifeng Guo1
1Department of Urology, Affiliated Tumor Hospital of Nantong University & Nantong Tumor Hospital, Nantong, 226361, People’s Republic of China; 2Department of Central Laboratory, Affiliated Tumor Hospital of Nantong University & Nantong Tumor Hospital, Nantong, 226361, People’s Republic of China
* These authors contributed equally to this work
Correspondence: Xiaolin Wang; Haifeng Guo, Department of Urology, Affiliated Tumor Hospital of Nantong University & Nantong Tumor Hospital, Nantong, 226361, People’s Republic of China, Tel +86 159 5086 8500 ; +86 138 1360 3975, Email [email protected]; [email protected]
Introduction: Numerous studies, including bladder cancer (BLCA), have confirmed the relationship between conventional systemic inflammatory biomarkers and the prognosis of tumors. Leukocytes, as the most common factor in inflammatory indicators, have been reported to predict prognosis in other tumors. However, we have not seen this research in BLCA. Therefore, we aim to find new blood markers to predict the prognosis of patients with transurethral resection of bladder tumor (TURBT).
Methods: Two cohorts from the two different hospitals were used for the specific study. The best cutoff values of leukocytes-related indicators were determined according to the ROC curve. Univariate and multivariate Cox regression analysis were used to explore the impact of indicators and clinical features on prognosis for patients with TURBT. The KM curve was used to show the impact of indicators on the prognosis. According to the consequence of multivariate method, a risk model was established to evaluate the prognosis of patients with bladder cancer.
Results: The white blood cell-to-lymphocyte ratio (WLR), the white blood cell-to-hemoglobin ratio (WHR), the white blood cell-to-neutrophil ratio (WNR), the white blood cell-to-monocyte ratio (WMR) and the white blood cell-to-erythrocyte ratio (WRR) are related to the prognosis of BLCA. The new risk model consisted of WHR, WMR and platelet-to-lymphocyte ratio (PLR), and patients with TURBT in the high-risk group had a worse prognosis.
Conclusions: Leukocyte-related preoperative indicators could predict the prognosis of the patients with TURBT and provided some guidance for clinical workers.
Keywords: bladder cancer, BLCA, white blood cell-to-lymphocyte ratio, WLR, white blood cell-to-hemoglobin ratio, WHR, white blood cell-to-neutrophil ratio, WNR
Introduction
Bladder cancer (BLCA) is 1 of the 10 most common malignant tumors in the world, with approximately 540,000 new cases and 200,000 deaths every year.1,2 BLCA can be divided into muscle-invasive bladder cancer (MIBC) and non-muscle-invasive bladder cancer (NMIBC) according to whether there is a muscularis invading the bladder wall. NMIBC accounts for about 75% of BLCA and is characterized by high recurrence rate and high cost of treatment for patients.3 Clinical treatment of BLCA is still mainly surgical treatment.4 Nevertheless, the treatment outcome is not satisfactory, and other therapeutic strategies should be sought to improve the prognosis of patients. Therefore, we have decided to seek new markers that can predict the prognosis of patients with bladder cancer.
So far, considerable research has been done to analyze the prognosis of BLCA. Clinicopathological characteristics, such as TNM staging, recurrence, body mass index (BMI), etc can be used as prognostic predictors for patients with BLCA.5 Current and past smoking increases the risk of recurrence and death in patients with BLCA.6 The expression of miR-143 in the serum of patients with BLCA is related to clinical stage, lymph node metastasis, distant metastasis and prognosis.7 The high expression level of PDK1 in tumor tissues represents a poor prognosis for patients with BLCA.8 However, the predictive power of some of the above markers for the prognosis of patients with BLCA is not concise, and we aim to find a clinically commonly used index to simply predict the prognosis of patients with NMIBC. In BLCA patients, some preoperative or postoperative blood test indicators explain the positive prognostic significance. The change in neutrophil-to-lymphocyte ratio (NLR) after BLCA surgery was a potential indicator for early diagnosis of BLCA recurrence.9 Pretreatment with platelet-to-lymphocyte ratio (PLR) could be used as a biomarker for predicting poor prognosis in patients with BLCA.10 There was an independent association between higher preoperative lymphocyte-to-monocyte ratio (LMR) and prognosis in patients with BLCA who underwent radical cystectomy (RC).11
White blood cells (WBCs), as a complete cell type in human blood, were rarely reported in BLCA. White blood cell-to-hemoglobin ratio (WHR) is very effective in predicting the prognosis of patients with gastric adenocarcinoma.12 The absolute count of WBCs has been confirmed to be unrelated to the prognosis in patients with BLCA.13 However, the research on other inflammatory indicators related to WBCs have not been reported in BLCA. Thus, we focused on studying the impact of leukocyte-related inflammation indicators on the prognosis of BLCA.
Methods
Patient Information Collection
The first cohort in the study consisted of 469 patients who underwent transurethral resection of bladder tumor (TURBT) from the Affiliated Hospital of Nantong University from January 1, 2014 to January 4, 2018. In accordance with the requirements of repeated patients, no serum data, and no life and death status, unnecessary data was deleted. The remaining 385 patients were included in the study cohort, and the follow-up time for this cohort ended on January 1, 2021. According to the above screening methods, the second cohort in the study consisted of 90 patients who underwent TURBT from the Affiliated Tumor Hospital of Nantong University, the most of which were from April 1, 2014 to December 31, 2019, and the follow-up time for this cohort ended on September 10, 2021. All patients included in the study were verified by the second contributor to verify the correctness of the collected information. All information collection was based on the patient’s last blood drawn before surgery.
Inflammation Biomarkers
All serum indicators mentioned in the text include white blood cell-to-lymphocyte ratio (WLR), WHR, white blood cell-to-neutrophil ratio (WNR), white blood cell-to-monocyte ratio (WMR) and white blood cell-to-erythrocyte ratio (WRR), NLR, LMR and PLR. All ratios were calculated by their absolute counts, respectively. The receiver operating characteristics (ROC) curve was utilized to determine the best cut-off value of each marker for the patient’s prognosis by the first cohort.
The best cut-off value for WLR was 3.6735; the best cut-off value for WHR was 0.0437; the best cut-off value for WNR was 1.5764; the best cut-off value for WMR was 14.8778; the best cut-off value for WRR was 1.6592; the best cut-off value for NLR was 2.3525; the best cut-off value for LMR was 4.8983; and the best cut-off value for PLR was 141.5387.
Statistical Analysis
All data statistics in the text were valid with a P value less than 0.05. The follow-up time started from the day of surgery and ended with death or the final follow-up termination time. The first cohort was defined as the training set, and the first cohort plus the second cohort was defined as the validation set. IBM SPSS Statistics 25, GraphPad Prism 8 and R Studio were performed to analyze all the data involved in the study.
Chi-square test (χ2 test) was used to detect the relationship between clinical characteristics (gender, age, BMI, recurrence, grade and adjuvant chemotherapy) and serum indicators. Univariate and multivariate Cox regression analysis was used to explore the significance of markers and clinical features on prognosis for patients with BLCA underwent TURBT. Kaplan–Meier’s (KM) curves, using Log rank test as a statistical method, were used to display indicators for the prognosis of BLCA patients. A new prognostic risk model (Risk = 0.6345*WHR-0.464*WMR+0.6063*PLR) was obtained from the results of multi-Cox analysis. The integrated prognostic ROC and KM curve plotting tool for the relationship between risk score and gene expression developed by R package “ggplot2”.
Results
Patient Information in the Training Set
A total of 385 patients were included in the training set, and the results are shown in Table 1. As the result showed that the expression level of WLR in the serum was significantly related to the tumor grade in BLCA (P = 0.0005, χ2 = 12). The expression level of WHR was significantly related to the tumor grade in BLCA (P = 0.005, χ2 = 7.72). The expression level of WNR was significantly related to the tumor grade in BLCA (P = 0.002, χ2 = 9.22). There was a significant correlation between the expression of WMR and gender (P = 0.01, χ2 = 6.658), age (P = 0.047, χ2 = 3.954), and grade (P = 0.032, χ2 = 4.62). The expression level of WRR was significantly related to the tumor grade in BLCA (P = 0.021, χ2 = 5.3). There was a significant correlation between the expression of NLR and age (P = 0.043, χ2 = 4.1), and grade (P = 0.0005, χ2 = 12). There was a significant correlation between the expression of LMR and gender (P = 0.0002, χ2 = 13.421), age (P = 0.003, χ2 = 8.868), and grade (P = 0.0002, χ2 = 14). In conclusion, there was a clear relationship between preoperative indicators and the grade of BLCA patients with TURBT, and there was no significant correlation with the patient’s recurrence and adjuvant chemotherapy methods.
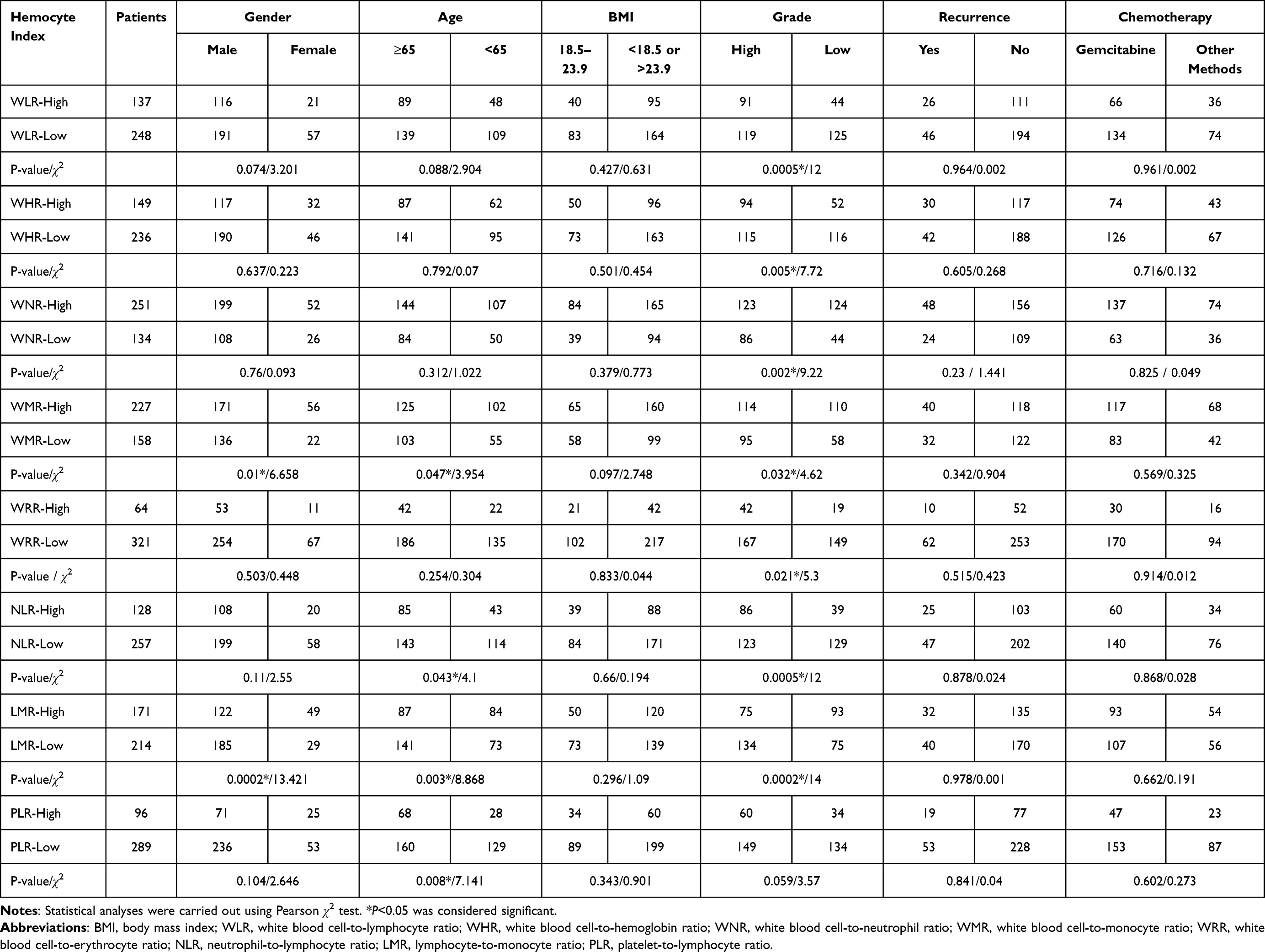 |
Table 1 Clinical Features of Bladder Cancer Patients Related to Hemocyte Index Involved in the Training Set |
WBC-Related Markers as the Independent Prognostic Factors in the Training Set
Univariate Cox regression analysis showed that age (P = 0.0001, HR = 2.244), tumor grade (P = 0.0003, HR = 2.106), WLR (P = 0.0011, HR = 1.818), WHR (P<0.0001, HR = 2.048), WNR (P = 0.0043, HR = 0.591), WMR (P = 0.0004, HR = 0.519), WRR (P<0.0001, HR = 2.686), NLR (P = 0.0004, HR = 1.914), LMR (P<0.0001, HR = 0.442) and PLR (P<0.0001, HR = 2.107) were the prognostic factors of BLCA patients underwent TURBT (Table 2). Multivariate Cox regression analysis showed that age (P = 0.0081, HR = 1.799), tumor grade (P = 0.0367, HR = 1.563), WHR (P = 0.0116, HR = 1.886), WMR (P = 0.0447, HR = 0.629) and PLR (P = 0.0039, HR = 1.834) were independent prognostic factors for patients with BLCA (Table 2). KM curve was made to exhibit the prognosis of the different expression level of WLR, WHR, WNR, WMR, WRR, NLR, LMR and PLR in BLCA (Figure 1A–H). As shown in the figure, the high expression of WLR, WHR, WRR, NLR and PLR represented the poor prognosis of patients with BLCA. However, the low expression level of WNR, WMR and LMR represented the poor prognosis of patients with BLCA.
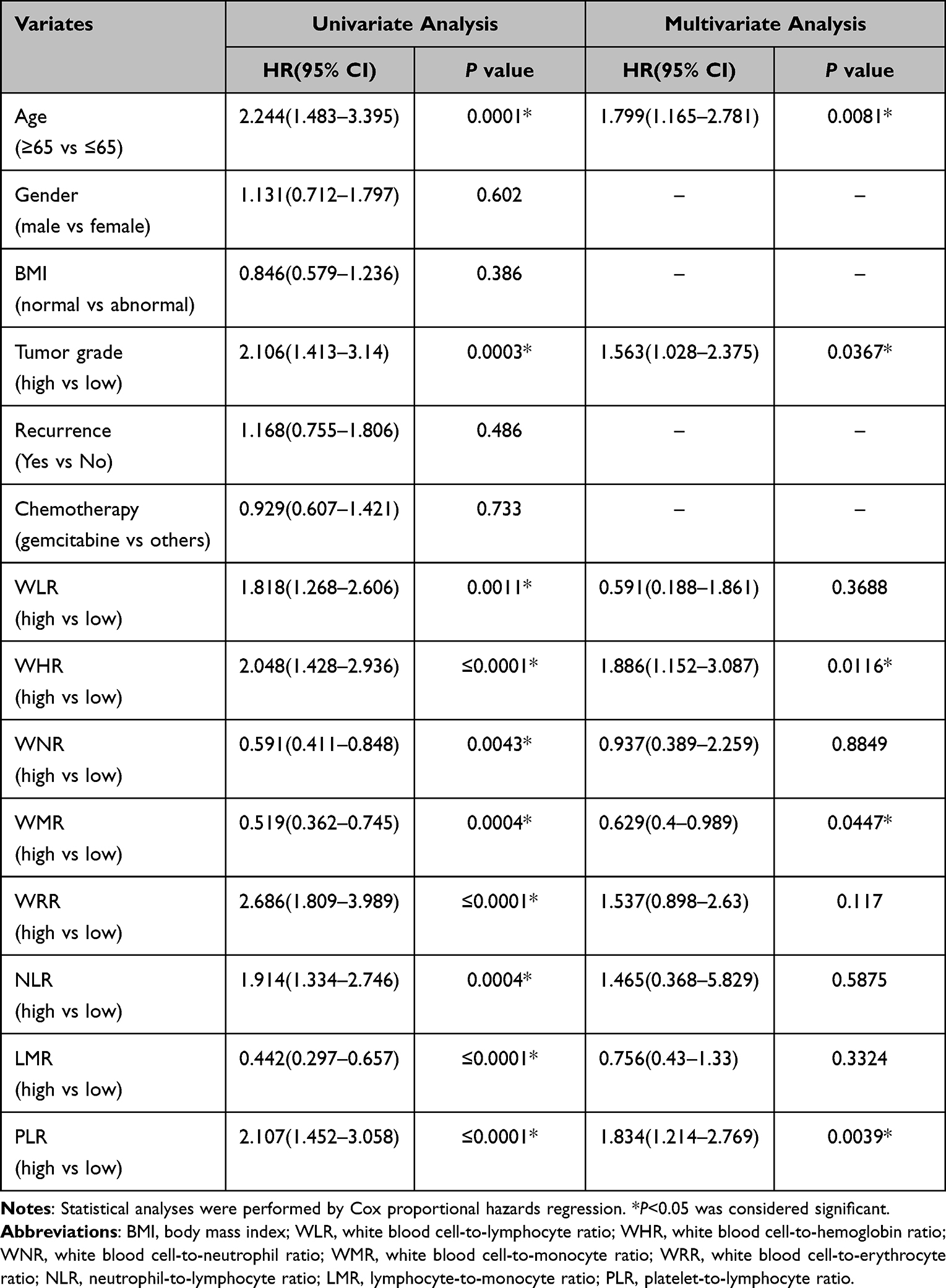 |
Table 2 Univariate and Multivariate Cox Regression Analysis for Prognosis of Patients with Bladder Cancer in the Training Set |
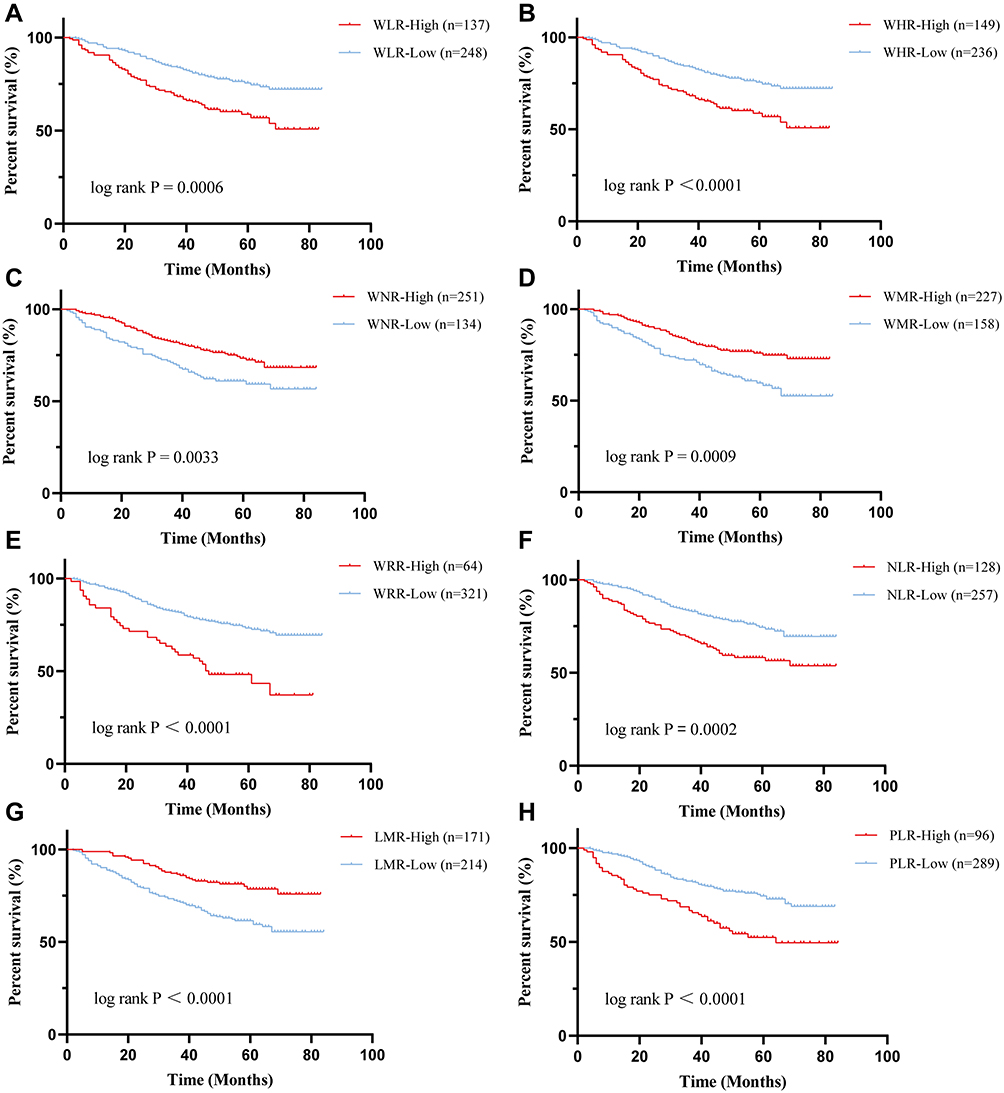 |
Figure 1 The KM curves of inflammatory marks for patients with BLCA in the training set. (A–H) KM curve was made to exhibit the prognosis of the different expression level of WLR, WHR, WNR, WMR, WRR, NLR, LMR and PLR, respectively. |
A New Risk Model for Patients in the Training Set
According to the results of Cox multivariate methods, we verified three serum indicators (WHR, WMR and PLR) with independent prognostic significance to construct a new risk model in the training set. Based on the ROC curve, the cut-off value (79.2223) of Risk was determined to divide into high-risk group and low-risk group (Figure 2A). The area under the curve (AUC) for 1,3,5-year survival rate was 0.79, 0.59 and 0.62, respectively (Figure 2B). The high-risk group had a worse prognosis for patients with BLCA than the lower expression group (Figure 2C, P<0.0001, HR = 1.01).
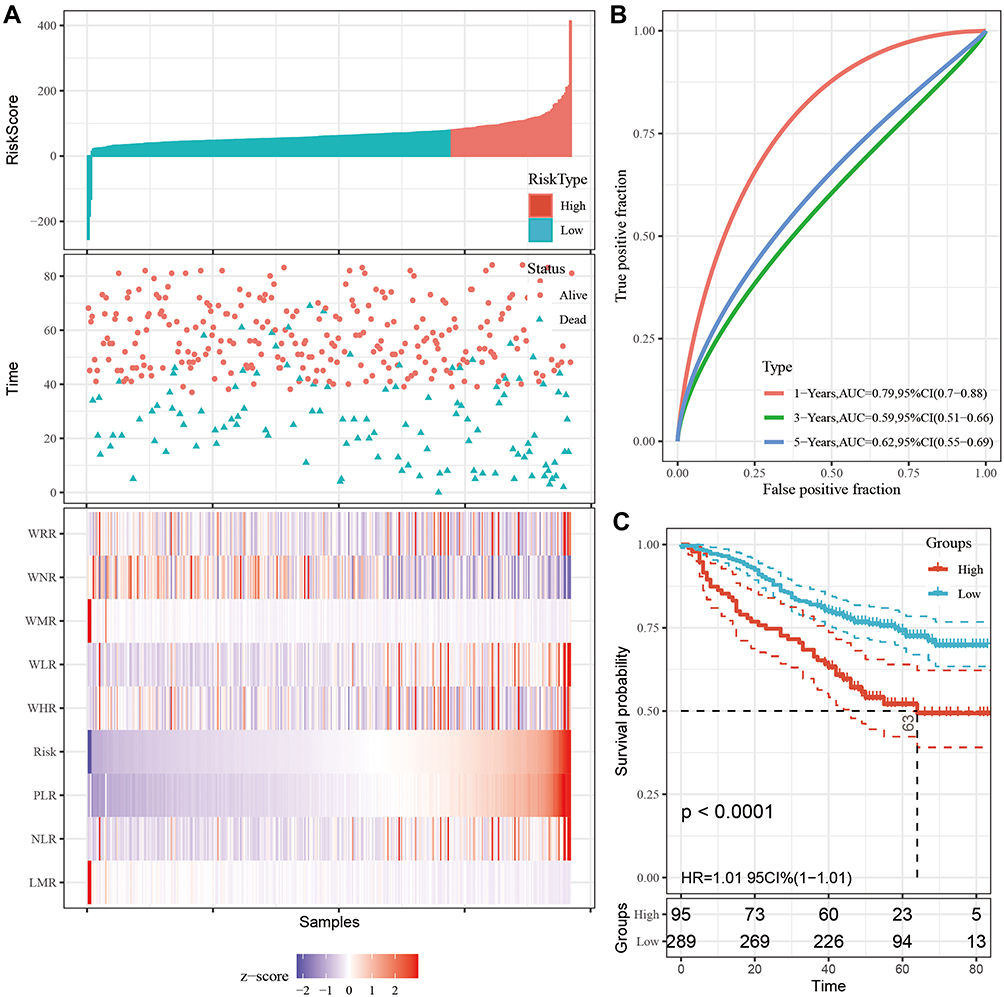 |
Figure 2 The new risk model was established to detect the OS of patients with BLCA in the training set. All patients were distinguished into high and low risk based on the risk score (A), upper; the relationship between survival time and prognosis of patients in the two corresponding groups (A), middle; the heatmap of inflammatory marks between the two groups (A), lower. Receiver operating characteristic (ROC) curve analysis of the new prognostic model at 1, 3, 5 years (B). Kaplan–Meier curves showing OS of groups with different risk (C). |
Patient Information in the Validation Set
In order to verify the authenticity and practicability of the research we constructed, we chose a new cohort as the verification set. Considering the data error caused by the small number of patients in the Affiliated Cancer Hospital of Nantong University, we combined it with the patients in the Affiliated Hospital of Nantong University as a validation set. As shown in Supplementary Table 1, all meaningful results in the training set were confirmed in the validation set. In addition, we found it that the expression level of WLR in the serum was significantly related to age in BLCA (P = 0.002, χ2 = 9.205). The expression level of PLR was significantly related to the tumor grade in BLCA (P = 0.035, χ2 = 4.466). The expression level of WLR was significantly related to the adjuvant chemotherapy methods in BLCA (P = 0.044, χ2 = 4.042). The expression level of NLR was significantly related to the adjuvant chemotherapy methods in BLCA (P = 0.023, χ2 = 5.165). Moreover, the Risk was also related to the age (P = 0.001, χ2 = 10.444) and grade (P = 0.031, χ2 = 4.641) in patients with BLCA who underwent TURBT.
WBC-Related Markers as the Independent Prognostic Factors in the Validation Set
The results of univariate Cox regression analysis obtained in the validation set were consistent with the conclusion in the training set (Supplementary Table 2). The Risk was also an independent prognostic factor for the validation set (P<0.001, HR = 2.005). KM curve was performed to display the prognosis of the different expression level of WLR, WHR, WNR, WMR, WRR, NLR, LMR and PLR in BLCA (Supplementary Figure 1A–H), and the result was consistent with the training set. According to the Risk above, we verified three serum indicators (WHR, WMR and PLR) with independent prognostic significance to construct a new risk model in the validation set. Based on the cut-off value mentioned above, Risk was divided into high-risk group and low-risk group (Supplementary Figure 2A). The AUC for 1,3,5-year survival rate was 0.73, 0.61 and 0.64, respectively (Supplementary Figure 2B). The high-risk group had a poor prognosis for patients with BLCA than the lower expression group (Supplementary Figure 2C, P<0.0001, HR = 1.01).
Discussion
The prognosis of the tumor by inflammatory microenvironment could be a positive intervention or a negative intervention,14 of course, this also including BLCA.15 When we mention the impact of inflammation-related indicators of BLCA patients on the prognosis, the most familiar ones were NLR,15 PLR and LMR, which have been studied in previous reports.16,17 These indicators were all related to the prognosis of patients with BLCA.
However, the function of the prognosis of WBCs, as an overall concept of inflammation indicators, was poorly understood in previous studies in BLCA. The total WBCs count often increased during infection and is a non-specific marker of inflammation. Although the absolute count of WBCs has no effect on the prognosis in BLCA (data not shown), we combined some other common blood cells as the research object. It was found that the combination of WBCs and other cells can be a good predictor for monitoring the prognosis of patients with BLCA who underwent TURBT. WLR, WHR, WNR, WMR and WRR could play a role of predicting the prognosis of BLCA patients. Previous studies seem to have overlooked the overall cell type of WBCs. In this study, we also explored whether there was a way to combine the new indicators and the previously famous indicators to explore the impact on the prognosis. A new prognostic model of combined serum indicators was born. WHR, WMR and PLR were combinedly chosen to form a new biomarker.
There is no doubt about the convenience of these indicators for clinically predicting the prognosis of patients with BLCA. However, whether these markers have high authenticity remains to be discussed. Prospective studies have shown that NLR has nothing to do with the prognosis of BLCA.18 This requires more research and larger sample data in the future to support the authenticity and validity of our findings. However, based on the current conclusions, it is very convenient to predict the prognosis of the patient with only the routine blood test before the operation. It is simple to carry out relevant interventions on the patient in advance to influence the prognosis of the patient.
Conclusions
We analyzed preoperative leukocyte-related indicators to predict the prognosis of patients with TURBT in this research. The results showed that WLR, WHR, WNR, WMR and WRR could play an important role of predicting the prognosis of BLCA patients. A new prognostic risk model of combined serum indicators exhibited that WHR, WMR and PLR were crucial. The results indicated that the simple and available serum indexes could provide some guidance for clinical workers. In the future, we hope to conduct research on the advanced BLCA patients and also wish to perform prospective and large sample experiments to verify our conclusions.
Data Sharing Statement
All data generated involved in the research are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by The Ethics Committee of the hospital (Nantong, China). Written informed consent was obtained from all individual participants included in the study. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by [Clinical medicine program of Nantong University] grant number [2019JY018] and the article processing charges (APC) was funded by [Jiangsu Commission of Health (M2021005)]. This article has been supported by the above funding and has received funding to cover publishing costs.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Cumberbatch M, Jubber I, Black PC, et al. Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018;74(6):784–795. doi:10.1016/j.eururo.2018.09.001
3. Lenis AT, Lec PM, Chamie K. Bladder cancer. JAMA. 2020;324(19):2006. doi:10.1001/jama.2020.17601
4. Tran L, Xiao JF, Agarwal N, Duex JE, Theodorescu D. Advances in bladder cancer biology and therapy. Nat Rev Cancer. 2021;21(2):104–121. doi:10.1038/s41568-020-00313-1
5. Westhoff E, Witjes JA, Fleshner NE, et al. Body mass index, diet-related factors, and bladder cancer prognosis: a systematic review and meta-analysis. Bladder Cancer. 2018;4(1):91–112. doi:10.3233/BLC-170147
6. Hou L, Hong X, Dai M, et al. Association of smoking status with prognosis in bladder cancer: a meta-analysis. Oncotarget. 2017;8(1):1278–1289. doi:10.18632/oncotarget.13606
7. Liu X, Zhao W, Wang X, Zhu Y, Zhou Z, Shi B. Expression of mir-143 in serum of bladder cancer patients and its correlation with clinical features and prognosis. J BUON. 2019;24(2):791–796.
8. Zhu J, Zheng G, Xu H, Jin X, Tang T, Wang X. Expression and prognostic significance of pyruvate dehydrogenase kinase 1 in bladder urothelial carcinoma. Virchows Arch. 2020;477(5):637–649. doi:10.1007/s00428-020-02782-z
9. Zhang Q, Lai Q, Wang S, Meng Q, Mo Z. Clinical value of postoperative neutrophil-to-lymphocyte ratio change as a detection marker of bladder cancer recurrence. Cancer Manag Res. 2021;13:849–860. doi:10.2147/CMAR.S289986
10. Wang X, Ni X, Tang G. Prognostic role of platelet-to-lymphocyte ratio in patients with bladder cancer: a meta-analysis. Front Oncol. 2019;9:757. doi:10.3389/fonc.2019.00757
11. Wang R, Yan Y, Liu S, Yao X. Comparison of preoperative neutrophil-lymphocyte and platelet-lymphocyte ratios in bladder cancer patients undergoing radical cystectomy. Biomed Res Int. 2019;2019:3628384. doi:10.1155/2019/3628384
12. Zheng HL, Lu J, Xie JW, et al. Exploring the value of new preoperative inflammation prognostic score: white blood cell to hemoglobin for gastric adenocarcinoma patients. BMC Cancer. 2019;19(1):1127. doi:10.1186/s12885-019-6213-0
13. Ku JH, Kang M, Kim HS, Jeong CW, Kwak C, Kim HH. The prognostic value of pretreatment of systemic inflammatory responses in patients with urothelial carcinoma undergoing radical cystectomy. Br J Cancer. 2015;112(3):461–467. doi:10.1038/bjc.2014.631
14. Fridman WH, Pagès F, Sautès-Fridman C, Galon J. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306. doi:10.1038/nrc3245
15. Lucca I, Jichlinski P, Shariat SF, et al. The neutrophil-to-lymphocyte ratio as a prognostic factor for patients with urothelial carcinoma of the bladder following radical cystectomy: validation and meta-analysis. Eur Urol Focus. 2016;2(1):79–85. doi:10.1016/j.euf.2015.03.001
16. Rajwa P, Życzkowski M, Paradysz A, Bujak K, Bryniarski P. Evaluation of the prognostic value of LMR, PLR, NLR, and dNLR in urothelial bladder cancer patients treated with radical cystectomy. Eur Rev Med Pharmacol Sci. 2018;22(10):3027–3037. doi:10.26355/eurrev_201805_15060
17. Yıldız HA, Değer MD, Aslan G. Prognostic value of preoperative inflammation markers in non-muscle invasive bladder cancer. Int J Clin Pract. 2021;75(6):e14118. doi:10.1111/ijcp.14118
18. Ojerholm E, Smith A, Hwang WT, et al. Neutrophil-to-lymphocyte ratio as a bladder cancer biomarker: assessing prognostic and predictive value in SWOG 8710. Cancer. 2017;123(5):794–801. doi:10.1002/cncr.30422
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dynamic Characteristics of Lymphocyte Subsets and Their Predictive Value for Disease Progression and Prognosis in Primary Infection and Unvaccinated COVID-19 Patients
Zhang X, Chen Z, Zheng J, Feng C, Zhao B, Lan L, Liu D
International Journal of General Medicine 2024, 17:4559-4577
Published Date: 10 October 2024
Biomarkers for Pediatric Acute Respiratory Distress Syndrome: A Systematic Review
Yang F, Zou J, Zheng L, Zeng C, Xu H, Yang J
Journal of Inflammation Research 2026, 19:581773
Published Date: 30 June 2026