Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Preoperative Immunotherapy in Hepatocellular Carcinoma: Current State of the Art
Authors Laschtowitz A, Roderburg C, Tacke F ![]() , Mohr R
, Mohr R ![]()
Received 28 September 2022
Accepted for publication 1 February 2023
Published 8 February 2023 Volume 2023:10 Pages 181—191
DOI https://doi.org/10.2147/JHC.S347944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Alena Laschtowitz,1 Christoph Roderburg,2 Frank Tacke,1 Raphael Mohr1
1Department of Hepatology and Gastroenterology, Charité – Universitätsmedizin Berlin, Campus Virchow Klinikum (CVK) and Campus Charité Mitte (CCM), Berlin, Germany; 2Clinic for Gastroenterology, Hepatology and Infectious Diseases, University Hospital Düsseldorf, Düsseldorf, Germany
Correspondence: Raphael Mohr, Department of Hepatology and Gastroenterology, Charité – Universitätsmedizin Berlin, Augustenburger Platz 1, Berlin, 13353, Germany, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is a malignancy that requires multidisciplinary evaluation to develop individualized and tailored treatment concepts. While liver resection and transplantation represent the mainstay of curative treatment in patients with early-stage HCC, disease recurrence remains an important burden. Immune checkpoint inhibitors (ICI) have become standard of care in the palliative setting, achieving promising response rates with overall good tolerability. Accordingly, ICIs are being evaluated in (neo)adjuvant concepts in order to improve survival. Nevertheless, neoadjuvant therapies are not recommended by current guidelines as they have not been proven to improve the outcome in large Phase III trials yet. Especially in the context of liver transplantation (LT), perioperative ICI usage is in need of a particularly critical risk–benefit assessment, as the immunotherapy may significantly increase the risk of rejection. In this review, we summarize available data on ICI-based perioperative treatment strategies in HCC. We discuss current drawbacks and challenges of this treatment concept and specifically highlight the risk of allograft rejection when ICI are given in patients (subsequently) considered for liver transplantation.
Keywords: hepatocellular carcinoma, immune oncology, checkpoint inhibitor, neoadjuvant
Introduction
The development of immune checkpoint inhibitors (ICI) has fundamentally changed the clinical management of hepatocellular carcinoma (HCC). While conventional chemotherapy had minimal effect on HCC, tyrosine-kinase inhibitors (TKI) have been the standard of care in HCC patients without curative treatment options during the past decades.1 The inhibition of programmed death receptor 1 (PD-1) or its ligand (PD-L1) in patients with advanced HCC showed clinical meaningful activity in several Phase I and II studies.2,3 The combination of the PD-L1 antibody atezolizumab with the vascular endothelial growth factor (VEGF) inhibitor bevacizumab improved overall survival (OS) and progression-free survival (PFS) when compared with the TKI sorafenib and was approved by the international guidelines as first-line therapy for advanced HCC.2,3 Most recently, phase III studies showed that the combination of PD-L1 inhibitor durvalumab with the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor tremelimumab, as well as the combination of PD-1 inhibitor camrelizumab with the TKI apatinib performed better than sorafenib in the setting of advanced HCC.4,5
For selected patients with early-stage HCC, surgical and ablative treatments are available in a (potentially) curative scenario while liver transplantation (LT) leads to improved long-term survival data in patients with cirrhosis compared to resected patients at the same tumor stage.6 Nevertheless, both de novo tumors and recurrence of HCC after LT may occur in 9–16% of cases.7 Thus, prevention of relapse remains an important goal in the management of HCC. TKI administration failed to show benefit in neoadjuvant randomized trials, and neither neoadjuvant nor adjuvant therapies are currently recommended by international guidelines as they have not been unequivocally demonstrated to improve the outcome. The excellent results of ICI trials in advanced HCC, on the one hand, and the high rates of recurrence after surgical treatment, on the other, support the evaluation of ICI usage in the intention of neoadjuvant or peri-interventional therapy concepts. Indeed, the clinical efficacy of preoperative ICI in other tumor entities has already led to FDA approvals.8–13 Nevertheless, only limited evidence is available on the usage of ICI as preoperative treatment, especially in the context of transplantation, and only small case series or individual case reports of transplanted patients have been published so far. Particularly in the context of LT, consideration of effectiveness and safety aspects must be taken into account regarding the possible risk of rejection.
In this review, we will briefly summarize, critically discuss and classify the current available evidence on the use of checkpoint inhibitors in neoadjuvant settings and give an outlook on future directions of immunotherapy in HCC.
Rationale and Biological Aspects of Neoadjuvant Immunotherapy
HCC is a malignancy that requires interdisciplinary evaluation to develop individualized and tailored treatment concepts. The reasonable combination of appropriate surgical approaches, interventional/locoregional treatment strategies and various lines of systemic therapy are required to achieve the best possible patient survival. Although surgery and LT will remain the mainstay of HCC therapy in patients at early disease stages, recent studies have identified major challenges. Many patients are not suitable for liver surgery and/or transplantation due to tumor macrovascular invasion, multifocal disease, large tumor mass, or impaired liver function. However, while in most patients surgical resection and transplantation are performed with curative intent, the recurrence rates peak up to 70% after HCC resection and about 50% of patients show early recurrence within the first two years which is associated with large tumor size or microvascular invasion.14,15 Neoadjuvant use of ICIs may therefore be intended as a downsizing strategy, making patients eligible for surgical treatment, but even more importantly to prevent relapses by eradication of micrometastasis.
“Immune checkpoints” are surface receptors. Under physiological conditions, their activation by the respective ligand regulates the balance between immune cell activation and immune cell quiescence, preventing normal tissues from being “attacked” by the immune system. Malignant tumors have the ability to upregulate those proteins, stimulating anti-inflammatory mechanisms, allowing the tumor to escape from being recognized by the patient’s immune system. In line, a high expression of the programmed death-ligand 1 by tumor cells or cells of the tumor microenvironment predict tumor recurrence after surgery.16 ICI block the inhibitory immune checkpoints, leading to a defense response toward the tumor tissue.
Mechanistically, ICI treatment is supposed to induce an improved priming of T cells that are directed against tumor neoantigens. In adjuvant settings, the priming is only induced by remaining micrometastasis, while in neoadjuvant settings more tumor mass is available for a stronger T cell response, underlining the benefit of ICI when used preoperatively. In line, data from melanoma and lung cancer showed the superiority of peri- versus postoperative immunotherapy.10,17 This concept has also been validated in animal models, where a preoperative PD-1 blockade led to improved survival and enhanced tumor-specific CD8+ T cell activation compared to postoperative PD-1 blockade.18 Furthermore, it seems intuitive that surgical intervention with removal of lymph nodes may negatively affect T cell expansion.
The principal concept of using ICI in a tumor mass reductive strategy making patients eligible for surgery is based on findings that liver-directed therapies are associated with sufficient local control and low LT waitlist dropout.19,20 Long-term outcomes showed 10-year survival and recurrence after downstaging of 52% and 20.4% compared to 60.5% and 14.3% for patients after liver transplantation without downstaging.21 In contrast to locoregional therapies, ICI harbor the risk of immune-related adverse events and severe allograft rejection in the transplant setting, as discussed further below. In this respect, the different metabolic half-lives of the several ICI agents which may lead to different prolonged T cell inductions need specific consideration.22,23
Available Data on Neoadjuvant Immunotherapy
For patients with preserved liver function and early-stage HCC, liver resection is the foremost curative strategy, with a 5-year overall survival (OS) of about 60%. But in spite of improving routine HCC surveillance to allow early detection of resectable HCC lesions, many patients present with tumors not eligible for primary resection. In this setting, ICI therapy may serve as a downstaging strategy to obtain secondary resectability while this practice already has relevant value in other tumor entities, such as for downstaging in advanced colon carcinoma.
Preoperative ICI in Initially Unresectable HCC
In HCC, this approach has been evaluated in one of the first published reports on preoperative ICI therapy in 15 patients primarily ineligible for curative resection due to high-risk features such as portal vein invasion, multifocality or advanced tumor size of more than 10 cm.24 After two weeks lead-in therapy with the TKI cabozantinib (40mg oral daily), an additional 4 cycles of the anti-PD-1 agent nivolumab (240mg Q2W) were applied. Restaging was performed after 10 weeks. In 12 out of 15 patients, margin-negative resection could be performed. Of note, one patient did not pursue surgical resection due to missing clinical response and insufficient hepatic reserve. In 5 out of 12 patients who underwent surgery, a pathological response with >90% of tumor necrosis was detected.
In the following, two further observational studies with heterogenous TKI/ICI regimes were administrated as neoadjuvant conversion therapy prior to surgery, as displayed in Table 1, but with markedly heterogenous combinatorial TKI/ICI treatment schedules, making it difficult to objectively compare different agents.25,26 Nevertheless, Zhang et al report on 10 patients with HCC and major vascular invasion that received different combinations of ICI and TKI with subsequent salvage surgery in 8 out of 10 patients and a 12-month recurrence-free survival rate of 75%.
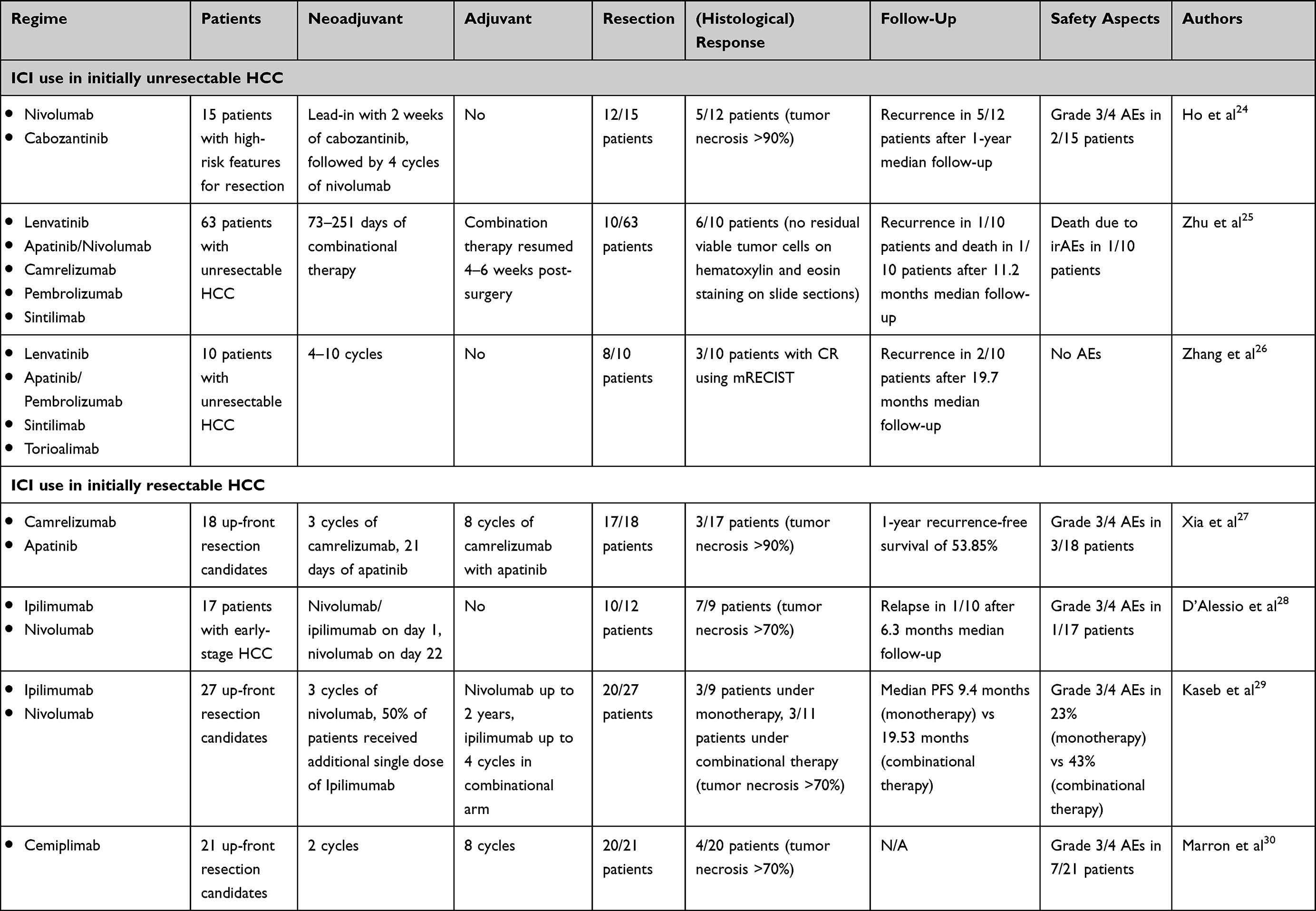 |
Table 1 Available Evidence for Preoperative Immunotherapy from Clinical Trials |
Preoperative ICI in Initially Resectable HCC
The three aforementioned studies used preoperative immunotherapy in a downstaging attempt to convert initially non-resectable tumors eligible for surgery. Another approach of neoadjuvant ICI treatment accounts to the high risk of recurrence in HCC, highlighted by recurrence rates as high as 70% at 5 years.14 Immunotherapy prior to resection aims to eradicate micrometastasis, that may lead to early recurrence, and thus to prolong recurrence-free survival. This concept has been evaluated in several Phase Ib/II trials for patients with up-front resectable tumors, as displayed in Table 1.
The efficacy and safety of camrelizumab, an anti-PD1-antibody, plus the TKI apatinib was recently evaluated in an open-label, single-arm Phase II trial enrolling 18 patients with up-front resectable HCC.27 Neoadjuvant treatment with three doses of camrelizumab (200mg Q2W) in combination with apatinib (250mg oral daily) for 21 days was continued after HCC resection for a further 8 adjuvant cycles. Following neoadjuvant treatment, 3 and 6 out of 18 patients showed an overall response based on RECIST or mRECIST criteria, respectively. While one patient did not receive surgical resection due to disease progression, 3 out of 17 patients showed >90% tumor necrosis and 1 out of 17 patients achieved a pathologically complete response. Five patients were excluded from adjuvant therapy due to external reasons. The 1-year recurrence-free survival (RFS) rate amongst the remaining 13 patients was 53.9% (95% CI: 24.8–76.0), while the RFS rate was tendentially higher in patients with a tumor necrosis of >90%.
In line with these findings are the results from the most recently published Phase Ib study evaluating the combination of nivolumab (3 mg/kg, day 1 and day 22) plus ipilimumab (1 mg/kg, day 1 only) as a neoadjuvant therapy in 17 patients undergoing early-stage HCC resection.28 Median tumor diameter was 3.4 cm (interquartile range [IQR] 2.4–4.0), and median number of lesions was 1 (range 1–3). After a median follow-up of 6.3 months (IQR 1.9–23.0), one disease relapse was recorded 20.8 months after treatment initiation. Pathological response was achieved in 78% of patients eligible for pathological evaluation (7 out of 9 patients), including 2 patients (22%) with complete response, while percentage of tumor necrosis was not available from published preliminary results. In contrast, when radiologically assessed, the ORR was only 23%. No severe immune-related adverse events were induced and neoadjuvant immunotherapy did not defer resection. These results underline the discrepancy between radiological and pathological tumor response and highlight the need for further evaluation of appropriate endpoints.
A Phase II trial including 27 patients with resectable HCC evaluated the administration of preoperative nivolumab (240mg Q2W, up to 3 cycles) +/- ipilimumab (1mg/kg, single dose), followed by an adjuvant therapy of nivolumab (480mg Q4W, up to 2 years) +/- ipilimumab (1mg/kg Q4W, up to 4 cycles).29 Grade 3–4 adverse events (AEs) were higher in the nivolumab plus ipilimumab (n=14) group than in nivolumab monotherapy (n=13), with 43% vs 23%, respectively. Twenty out of 27 patients underwent resection. In all 7 cases, surgery was cancelled due to tumor progression but not because of treatment-related AEs. Estimated median progression-free survival (PFS) and median time to progression were each 9.4 vs 19.5 months with nivolumab and nivolumab plus ipilimumab, respectively. Significant pathological response, defined as >70% of tumor necrosis, was found in 3 out of 9 patients under nivolumab monotherapy and in 3 out of 11 patients under combinational therapy with ipilimumab. Notably, after a 2-year follow up no recurrences in patients with pathological response were observed, while half of the non-responders developed recurrence.
A potential predictive role of preexisting immune infiltrates is underlined by the evidence of a Phase II trial where tumor tissue of pre- and post-ICI-treatment was evaluated.30 Two cycles of cemiplimab (350mg Q3W) were administered as preoperative monotherapy in 21 patients with resectable HCC. One week after the last cemiplimab administration liver resection in curative intention was performed and was followed by an additional 8 postoperative cycles of cemiplimab. Twenty out of 21 patients received successful resection, whereof 20% of patients achieved a significant pathological response, defined as >70% tumor necrosis. Seven out of 20 patients were classified responders, defined as having >50% of tumor necrosis. Significant immune infiltrations were seen in responders compared to non-responders. Notably, increased immune infiltrates were also detected before treatment initiation among responders, indicating a potential predictive value for immune infiltrates as biomarker for rapid response to ICI therapy.
Immunotherapy in the Context of Liver Transplantation
While immunotherapies can lead to clinically significant antitumor immune responses by activating immune cells, such therapies may also induce alloreactions and even autoimmune processes against organ transplants that are usually well controlled by drugs. For LT, it could be shown that the PD-1/PD-L1 interaction plays an important role in the inhibition of rejection reactions.31 Therefore, ICI treatment in the context of organ transplantation harbors the risk of graft rejection with ultimately graft loss and possibly patient death. There is broad consensus that any ICI-based therapy in patients potentially eligible for liver transplantation or in patients after liver transplantation (eg, in conditions of HCC recurrence or development of an extrahepatic malignancy such as melanoma) demands a careful and thorough risk–benefit assessment.32 Little data are published on ICI use in the context of organ transplantation, but rejection appears to occur in 30–40% of patients.33–38 A recent review on 25 LT cases described rejection in 36% of patients, which is associated with a rejection-related mortality rate of 20% of treated patients.39
In addition to the potential risk of rejection, a lower efficacy of ICI-based therapies in immunosuppressed patients after transplantation has to be considered. No biomarkers have been identified yet to predict rejection. However, there are findings of the histological evidence of PDL1- expression in the graft prior to initiation of ICI treatment being associated with a high risk of rejection.40 On pretransplant ICI treatment, there is also currently little data, as displayed in Table 2. Safety remains a significant concern, with definite interest in timing of withdrawal of different ICI agents, while small retrospective studies in which ICI therapy was continued until shortly before LT reported no increased rate of rejection.41,42
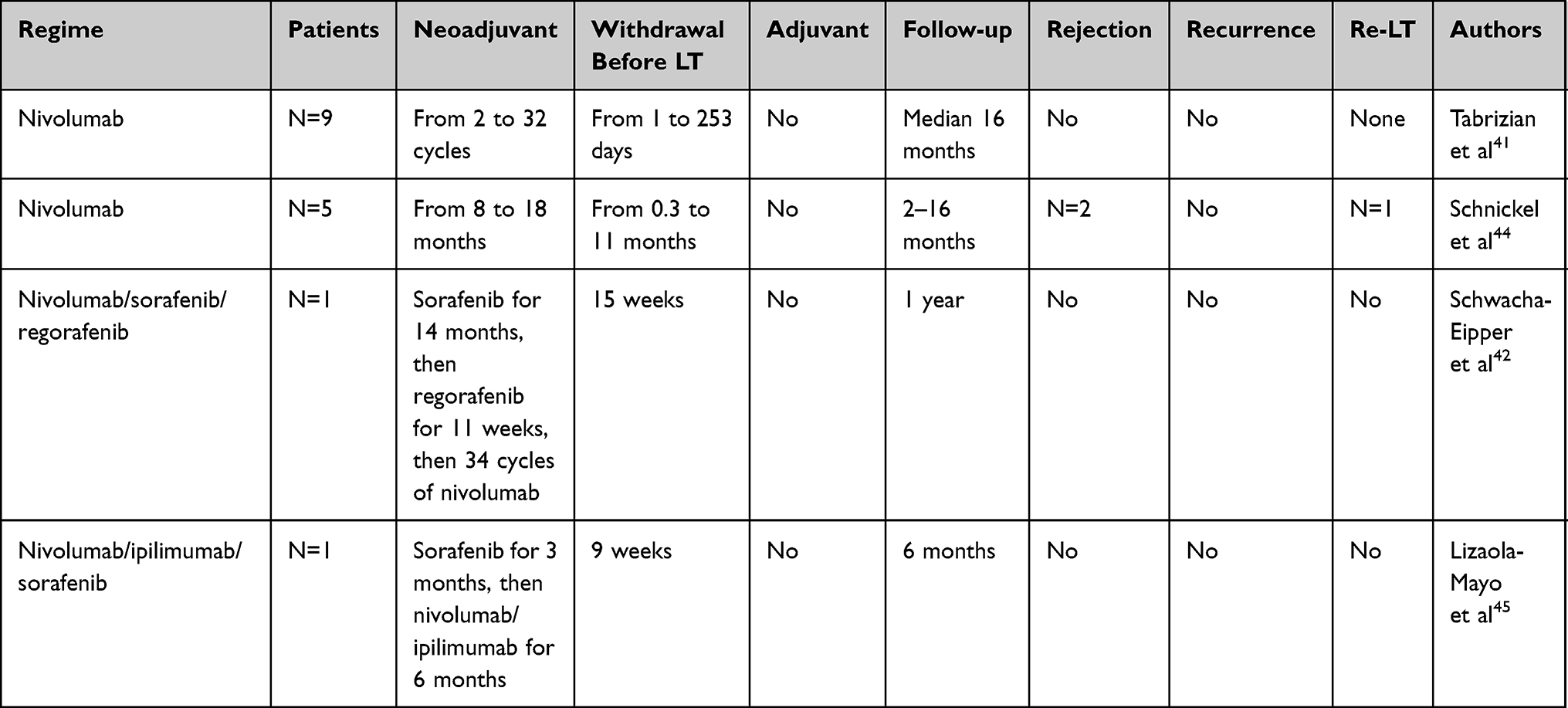 |
Table 2 Available Evidence for Immunotherapy in the Context of Liver Transplantation |
In clinical practice, the benefits and risks of preoperative immunotherapy need evaluation primarily as part of a multimodality therapeutic approach and subsequently in different scenarios. In patients with advanced tumors for whom liver transplantation is not a primary therapeutic option, an excellent response to immunotherapy may secondarily lead to the LT option in a downstaging approach. In those patients with an initial stage beyond transplantation criteria, studies have already shown a comparable outcome after LT in terms of overall survival and tumor-free survival when downstaging by locoregional measures compared to those with initial transplant eligibility.19 Indeed, future studies have to evaluate whether this also holds true in the setting of ICI therapy as a downstaging agent, taking into account the potentially increased risk of rejection or liver failure in subsequent liver transplantation, as previously reported.43
ICI therapy might be a future “bridging” concept in patients eligible for transplantation while being on the waiting list. This concept aims to avoid loss of the waiting list position due to tumor progression by mostly using locoregional treatment. But to date, due to multiple alternative strategies, ICI, with its increased allograft rejection risk, is nowadays not recommended as a bridging concept.
In patients with excellent responses to ICI therapy, individual possibilities of LT with a transplant organ offered outside of organ allocation or living donation require individual evaluation in specialized centers.32
Ongoing Preoperative Clinical Trials
Checkpoint inhibitors have the potential to achieve significantly higher tumor response rates than TKI. Thus, immunotherapy may serve as a downstaging strategy to achieve secondary resectability. Case series and the first available data from Phase I/II trials showed pathological tumor response rates up to 50%, but also occurrence of tumor progression under therapy leading to patients no longer being candidates for curative surgery. Numerous clinical trials are currently investigating the role of different ICI regimes and combinations in a neoadjuvant setting. An overview of ongoing clinical trials is given in Table 3. Key questions being addressed, besides efficacy and safety, are length and insensitivity (agent selection and combinations) of preoperative treatment.
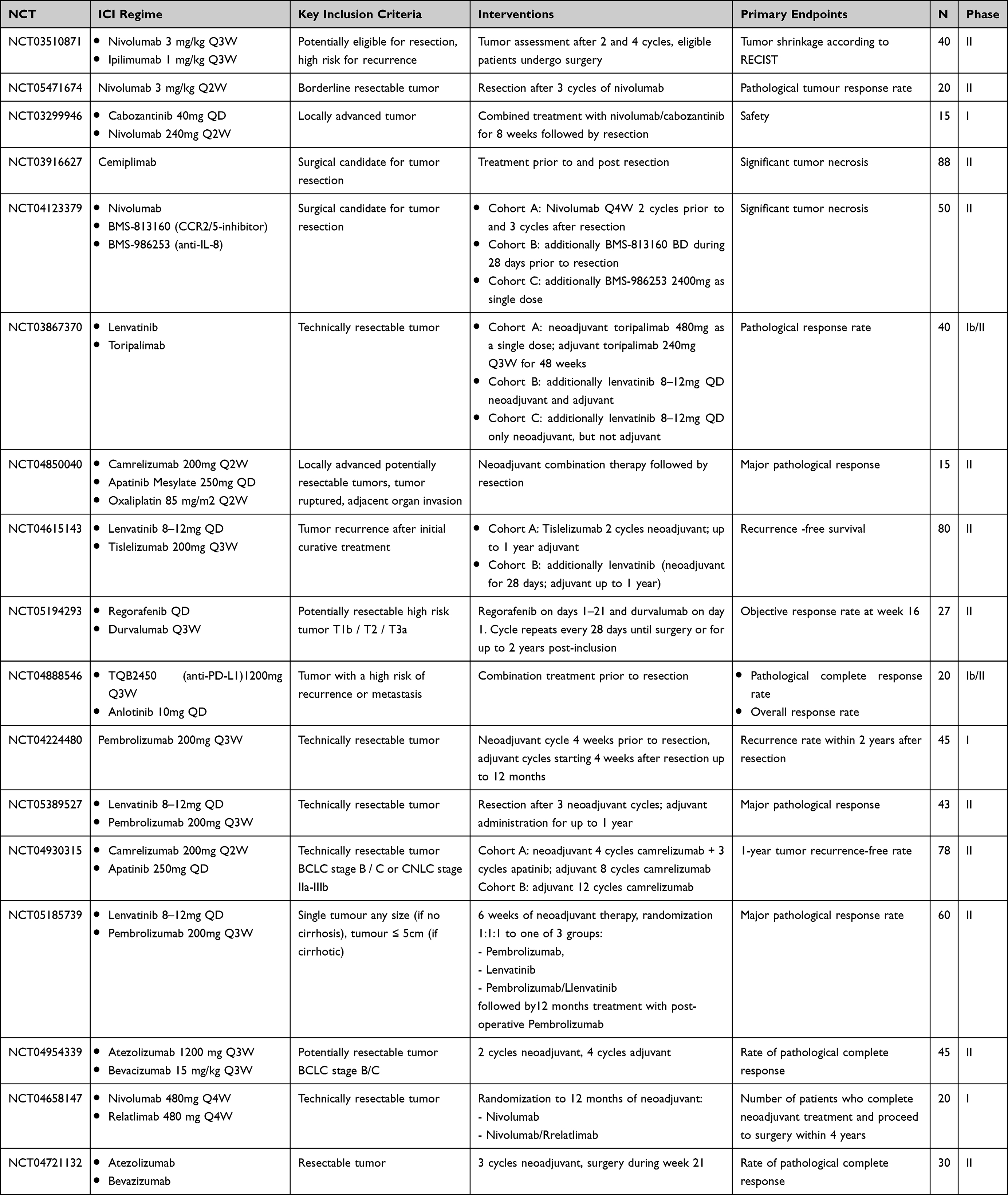 |
Table 3 Ongoing Clinical Trials for Preoperative Immunotherapy |
Discussion
As the majority of HCC is diagnosed at intermediate or advanced stages, there is a high clinical need for multimodal therapeutic approaches. While preoperative TKI administration failed to demonstrate benefit in HCC, the convincing efficacy of immunotherapy in the palliative setting raises new hopes to expand systemic therapy to earlier tumor stages and make downstaging and a prolongation of recurrence-free survival feasible. Nevertheless, neoadjuvant therapies are not yet recommended by current guidelines, as data from Phase III trials are lacking.
Preoperative immunotherapy is a promising approach for up-front resectable and borderline resectable HCC. Primary goal is to induce an immune response against micrometastasis and thus decrease the risk of disease recurrence. In this respect, it seems likely that substances with higher antitumoral activity (eg higher response rates) will achieve better survival than those with rather low activity. Recent data suggested higher response rates for drug combinations than for single substances.2,28,29 In line with this hypothesis, the combination of nivolumab and opilimumab was associated with pathological response rates of up to 78% when used in a neoadjuvant setting. While head-to-head studies comparing different treatments are missing, it seems likely that future studies addressing the potential of immunotherapy in the neoadjuvant setting will focus on drug combinations harbouring the risk of increased immune-related toxicities.
A major drawback in the process of regulatory approval of preoperative agents in HCC is the lack of a validated endpoint. Whereas the nivolumab/cabozantinib and the camrelizumab/apatinib trials chose a pathological response of >90% tumor necrosis, the nivolumab/ipilimumab and the cemiplimab trials chose >70%. Conventional radiologic response assessments may be inapt to record changes within short time intervals, differentiate between tumor progress vs pseudoprogression through immune infiltration, and may underestimate the magnitude of tumor response. As in the nivolumab/ipilimumab trial, a pathological response was achieved in 78%, whereas the radiologic ORR was only 23%.
Another key question is the required duration of preoperative therapy. Longer treatment may enhance tumor response but harbors the risk of inducing immune-related adverse events. This was the case in the cemiplimab trial, where an ICI-related pneumonitis delayed one patient’s resection significantly. Data from preclinical mouse models of metastatic malignancies reported that only a relatively short duration (in this case 4–5 days) between the first ICI administration to surgery was necessary for optimal outcome, while both shortening and delaying led to decreased efficacy (in this case 2 or 10 days, respectively).46 But interestingly, even an additional 4 cycles to the basic 2 cycles of neoadjuvant ICI therapy did not improve tumor-free survival, underlining the need for more detailed data.
In the context of liver transplantation with the risk of allograft organ loss, not only the duration of preoperative ICI therapy but also the timing of withdrawal remain major challenges. Existing data showed a sustained mean occupancy of majority of PD-1 molecules on T cells even 2 months after ICI administration and regardless of application doses.47 Moreover, a discrepancy in the pharmacological and biological half-lives of ICI agents has to be taken into consideration.48 In view of the very limited data available, no definitive recommendation concerning the duration of ICI therapy prior to LT can be given.32 Overall, a period of at least 3 months is considered advisable (3–5 half-life periods) to reduce the risk of rejection after LT. Nevertheless, in individual cases, a rejection after a 3-month ICI abstinence has also been described, indicating appropriate monitoring. More data is urgently needed on optimized withdrawal timing to prevent ICI-induced organ rejection. However, in real life, timing of withdrawal remains particularly challenging regarding the inability to anticipate and time organ offerings.
To improve the assessment of risk and benefits of ICI use, biomarkers may help to predict ICI response. Aside from the aforementioned possible role of PD-L1 expression in the transplant as a predictive biomarker for rejection, the study of Marron et al indicates a role for pre-existing immune infiltrates as being predictive for rapid ICI response. Accordingly, pretherapeutic liver biopsies could be implemented in the decision-making process.
A further possible factor for the prediction of ICI efficiency is the underlying etiology based on findings in NASH-HCC mice. Here, an accumulation of CD8+PD1+ T cells were detected, which surprisingly was associated with more severe hepatic tissue damage and HCC progression under PD-1 blockade, thus being different to non-NASH-HCC mice that showed tumor regression.30,49,50 However, whether biomarkers and/or underlying etiology have an influence on the decision of using perioperative immunotherapy requires further investigation.
Given the high efficacy of ICI-based combination therapies, this systemic therapy for HCC will be increasingly used in the future in patients with earlier HCC stages, and thus also in patients before transplantation. While in the context of resection several trials are ongoing, there is a dire need for randomized, prospective trials for transplant candidates.
Conclusion
More and more evidence is accumulating indicating that immunotherapy is a powerful tool in the multimodal treatment approach for HCC. In early-stage tumors where resection is feasible, neoadjuvant immunotherapy may increase the chances of definitive cure by reducing the risk of micrometastases and tumor recurrence. For patients with borderline tumor burden at diagnosis, immunotherapy may provide a downstaging strategy converting these patients into candidates for resection. Recent data suggest higher response rates for drug combinations but with an increasing risk of immune-related toxicities. Taking into account the considerations outlined above, individualized concepts of preoperative ICI therapy are possible, also in the context of LT, until data from Phase III trials and corresponding recommendations are published in the guidelines. However, individualized concepts should only be performed in highly specialized centers and the risk of organ failure has to be critically discussed with the patient. In addition, the need for further biomarkers to identify patients with an increased risk of rejection is becoming clear. For a better risk assessment in future, data from randomized trials are required to identify the optimal combination of agents and duration of therapy, as well as to determine subsets of patients that benefit from neoadjuvant strategies.
Abbreviations
AE, adverse event; CPR, complete pathological response; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; FDA, US Food and Drug Administration; HCC, hepatocellular carcinoma; ICI, immune checkpoint inhibitor(s); irAE, immune-related adverse event; IQR, interquartile range; LT, liver transplantation; mRECIST, modified response evaluation criteria in solid tumors; ORR, objective response rate; OS, overall survival; PD-1, programmed death receptor 1; PD-L1, programmed death receptor 1 ligand; PFS, progression-free survival; RECIST, response evaluation criteria in solid tumors; RFS, recurrence-free survival; Th 2 cell, T-helper cell 2; TKI, tyrosine-kinase inhibitors; VEGF, vascular endothelial growth factor.
Disclosure
AL is supported by the Digital Clinician Scientist Program of the Berlin Institute of Health. FT reports grants from Gilead, BMS, and Inventiva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Vogel A, Bathon M, Saborowski A. Advances in systemic therapy for the first-line treatment of unresectable HCC. Expert Rev Anticancer Ther. 2021;21:621–628. doi:10.1080/14737140.2021.1882855
2. Finn RS, Qin S, Ikeda M, et al. IMbrave150: updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J Clin Oncol. 2021;39:267. doi:10.1200/JCO.2021.39.3_suppl.267
3. Vogel A, Martinelli E, Cervantes A, et al. Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO clinical practice guidelines. Ann Oncol. 2021;32:801–805. doi:10.1016/j.annonc.2021.02.014
4. Abou-Alfa GK, Chan SL, Kudo M, et al. Phase 3 randomized, open-label, multicenter study of tremelimumab (T) and durvalumab (D) as first-line therapy in patients (pts) with unresectable hepatocellular carcinoma (uHCC): HIMALAYA. J Clin Oncol. 2022;40:379. doi:10.1200/JCO.2022.40.4_suppl.379
5. OncologyPRO. Camrelizumab (C) plus rivoceranib (R) vs. sorafenib (S) as first-line therapy for unresectable hepatocellular carcinoma (uHCC): a randomized, phase; 2023. Available from: https://oncologypro.esmo.org/meeting-resources/esmo-congress/camrelizumab-c-plus-rivoceranib-r-vs.-sorafenib-s-as-first-line-therapy-for-unresectable-hepatocellular-carcinoma-uhcc-a-randomized-phase.
6. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76:681–693. doi:10.1016/j.jhep.2021.11.018
7. Gül-Klein S, Kästner A, Haber PK, et al. Recurrence of hepatocellular carcinoma after liver transplantation is associated with episodes of acute rejections. J Hepatocell Carcinoma. 2021;8:133–143. doi:10.2147/JHC.S292010
8. Schmid P, Cortes J, Dent R, et al. VP7-2021: KEYNOTE-522: phase III study of neoadjuvant pembrolizumab + chemotherapy vs. placebo + chemotherapy, followed by adjuvant pembrolizumab vs. placebo for early-stage TNBC. Ann Oncol. 2021;32:1198–1200. doi:10.1016/j.annonc.2021.06.014
9. Topalian SL, Bhatia S, Amin A, et al. Neoadjuvant nivolumab for patients with resectable merkel cell carcinoma in the CheckMate 358 trial. In Journal of Clinical Oncology. American Society of Clinical Oncology; 2020:2476–2487.
10. Blank CU, Rozeman EA, Fanchi LF, et al. Neoadjuvant versus adjuvant ipilimumab plus nivolumab in macroscopic stage III melanoma. Nat Med. 2018;24:1655–1661. doi:10.1038/s41591-018-0198-0
11. Forde PM, Anagnostou V, Sun Z, et al. Durvalumab with platinum-pemetrexed for unresectable pleural mesothelioma: survival, genomic and immunologic analyses from the Phase 2 PrE0505 trial. Nat Med. 2021;27:1910–1920. doi:10.1038/s41591-021-01541-0
12. Chalabi M, Fanchi LF, Dijkstra KK, et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. 2020;26:566–576. doi:10.1038/s41591-020-0805-8
13. Powles T, Kockx M, Rodriguez-Vida A, et al. Clinical efficacy and biomarker analysis of neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. Nat Med. 2019;25:1706–1714. doi:10.1038/s41591-019-0628-7
14. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Prim. 2021;7:1–28. doi:10.1038/s41572-020-00234-1
15. Zheng J, Chou JF, Gönen M, et al. Prediction of hepatocellular carcinoma recurrence beyond milan criteria after resection. In: Annals of Surgery. Lippincott Williams and Wilkins; 2017:693–701.
16. Calderaro J, Rousseau B, Amaddeo G, et al. Programmed death ligand 1 expression in hepatocellular carcinoma: relationship With clinical and pathological features. Hepatology. 2016;64:2038–2046. doi:10.1002/hep.28710
17. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med. 2018;378:1976–1986. doi:10.1056/NEJMoa1716078
18. Liu J, Blake SJ, Yong MCR, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov. 2016;6:1382–1399. doi:10.1158/2159-8290.CD-16-0577
19. Yao FY, Mehta N, Flemming J, et al. Downstaging of hepatocellular cancer before liver transplant: long-term outcome compared to tumors within Milan criteria. Hepatology. 2015;61:1968–1977. doi:10.1002/hep.27752
20. Mazzaferro V, Citterio D, Bhoori S, et al. Liver transplantation in hepatocellular carcinoma after tumour downstaging (XXL): a randomised, controlled, phase 2b/3 trial. Lancet Oncol. 2020;21:947–956. doi:10.1016/S1470-2045(20)30224-2
21. Israelsen MB, Trošt K, Madsen BS, et al. Oral abstracts (Abstracts 1–288). Hepatology. 2019;70:1–187. doi:10.1002/hep.30940
22. Hurkmans DP, Basak EA, Van Dijk T, et al. A prospective cohort study on the pharmacokinetics of nivolumab in metastatic non-small cell lung cancer, melanoma, and renal cell cancer patients. J Immunother Cancer. 2019;7. doi:10.1186/s40425-019-0669-y
23. Su C, Wang H, Liu Y, et al. Adverse effects of anti-PD-1/PD-L1 therapy in non-small cell lung cancer. Front Oncol. 2020;10. doi:10.3389/fonc.2020.554313
24. Ho WJ, Zhu Q, Durham J, et al. Neoadjuvant cabozantinib and nivolumab convert locally advanced hepatocellular carcinoma into resectable disease with enhanced antitumor immunity. Nat Cancer. 2021;2:891–903. doi:10.1038/s43018-021-00234-4
25. Zhu XD, Huang C, Shen YH, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and anti-PD-1 antibody combinations. Liver Cancer. 2021;10:320–329. doi:10.1159/000514313
26. Zhang W, Hu B, Han J, et al. Surgery after conversion therapy with PD-1 inhibitors plus tyrosine kinase inhibitors are effective and safe for advanced hepatocellular carcinoma: a pilot study of ten patients. Front Oncol. 2021;11:215.
27. Xia Y, Tang W, Qian X, et al. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J Immunother Cancer. 2022;10:4656. doi:10.1136/jitc-2022-004656
28. D’Alessio A, Pai M, Spalding D, et al. Preliminary results from a phase Ib study of neoadjuvant ipilimumab plus nivolumab prior to liver resection for hepatocellular carcinoma: the PRIME-HCC trial. J Clin Oncol. 2022;40:4093. doi:10.1200/JCO.2022.40.16_suppl.4093
29. Kaseb AO, Hasanov E, Cao HST, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7:208–218. doi:10.1016/S2468-1253(21)00427-1
30. Marron TU, Fiel MI, Hamon P, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7:219–229. doi:10.1016/S2468-1253(21)00385-X
31. Shi XL, Mancham S, Hansen BE, et al. Counter-regulation of rejection activity against human liver grafts by donor PD-L1 and recipient PD-1 interaction. J Hepatol. 2016;64:1274–1282. doi:10.1016/j.jhep.2016.02.034
32. Vogel A, Sterneck M, Vondran F, et al. The use of immuno-oncologic therapy in hepatocellular carcinoma in the context of liver transplantationAn interdisciplinary benefit/risk assessment. Z Gastroenterol. 2022;60:184–191. doi:10.1055/a-1649-8643
33. DeLeon TT, Salomao MA, Aqel BA, et al. Pilot evaluation of PD-1 inhibition in metastatic cancer patients with a history of liver transplantation: the Mayo Clinic experience. J Gastrointest Oncol. 2018;9:1054–1062. doi:10.21037/jgo.2018.07.05
34. Gassmann D, Weiler S, Mertens JC, et al. Liver allograft failure after nivolumab treatment—A Case report with systematic literature research. Transplant Direct. 2018;4. doi:10.1097/TXD.0000000000000814
35. Tsung I, Worden FP, Fontana RJ. A pilot study of checkpoint inhibitors in solid organ transplant recipients with metastatic cutaneous squamous cell carcinoma. Oncologist. 2021;26:133–138. doi:10.1002/onco.13539
36. Friend BD, Venick RS, McDiarmid SV, et al. Fatal orthotopic liver transplant organ rejection induced by a checkpoint inhibitor in two patients with refractory, metastatic hepatocellular carcinoma. Pediatr Blood Cancer. 2017;64:189.
37. Zhuang L, Mou HB, Yu LF, et al. Immune checkpoint inhibitor for hepatocellular carcinoma recurrence after liver transplantation. Hepatobiliary Pancreat Dis Int. 2020;19:91–93. doi:10.1016/j.hbpd.2019.09.011
38. Tio M, Rai R, Ezeoke OM, et al. Anti-PD-1/PD-L1 immunotherapy in patients with solid organ transplant, HIV or hepatitis B/C infection. Eur J Cancer. 2018;104:137–144. doi:10.1016/j.ejca.2018.09.017
39. Delyon J, Zuber J, Dorent R, et al. Immune checkpoint inhibitors in transplantation—a case series and comprehensive review of current knowledge. Transplantation. 2021;105:67–78. doi:10.1097/TP.0000000000003292
40. Shi GM, Wang J, Huang XW, et al. Graft programmed death ligand 1 expression as a marker for transplant rejection following anti–programmed death 1 immunotherapy for recurrent liver tumors. Liver Transplant. 2021;27:444–449. doi:10.1002/lt.25887
41. Tabrizian P, Florman SS, Schwartz ME. PD‐1 inhibitor as bridge therapy to liver transplantation? Am J Transplant. 2021;21:1979–1980. doi:10.1111/ajt.16448
42. Schwacha-Eipper B, Minciuna I, Banz V, Dufour JF. Immunotherapy as a downstaging therapy for liver transplantation. Hepatology. 2020;72:1488–1490. doi:10.1002/hep.31234
43. Nordness MF, Hamel S, Godfrey CM, et al. Fatal hepatic necrosis after nivolumab as a bridge to liver transplant for HCC: are checkpoint inhibitors safe for the pretransplant patient? Am J Transplant. 2020;20:879–883.
44. Schnickel GT, Fabbri K, Hosseini M, et al. Liver transplantation for hepatocellular carcinoma following checkpoint inhibitor therapy with nivolumab. Am J Transplant. 2022;22:1699–1704. doi:10.1111/ajt.16965
45. Lizaola-Mayo BC, Mathur AK, Borad MJ, et al. Immunotherapy as a downstaging tool for liver transplantation in hepatocellular carcinoma. Am J Gastroenterol. 2021;116:2478–2480. doi:10.14309/ajg.0000000000001391
46. Liu J, O’Donnell JS, Yan J, et al. Timing of neoadjuvant immunotherapy in relation to surgery is crucial for outcome. Oncoimmunology. 2019;8:e1581530. doi:10.1080/2162402X.2019.1581530
47. Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28:3167–3175. doi:10.1200/JCO.2009.26.7609
48. Centanni M, Moes DJ, Trocóniz IF, Ciccolini J, van Hasselt JGC. Clinical pharmacokinetics and pharmacodynamics of immune checkpoint inhibitors. Clin Pharmacokinet. 2019;58:835–857. doi:10.1007/s40262-019-00748-2
49. Pfister D, Núñez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592:450–456. doi:10.1038/s41586-021-03362-0
50. Dudek M, Pfister D, Donakonda S, et al. Auto-aggressive CXCR6+ CD8 T cells cause liver immune pathology in NASH. Nature. 2021;592:444–449. doi:10.1038/s41586-021-03233-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Myasthenia Gravis-Like Symptoms Following Immune Checkpoint Inhibitor Therapy for Hepatocellular Carcinoma: A Case Report
Ha F, Wang H, Cai J, Liang J, Liu H
Cancer Management and Research 2025, 17:1819-1823
Published Date: 27 August 2025