")
Back to Journals » Biologics: Targets and Therapy » Volume 17
Preliminary Assessment of Safety and Tolerability of Avacopan During the Early Access Program for ANCA-Associated Vasculitis
Authors van Leeuwen JR , Popov T, Obergfell A, Rabelink TJ, Teng YKO
Received 4 November 2022
Accepted for publication 19 January 2023
Published 25 January 2023 Volume 2023:17 Pages 11—14
DOI https://doi.org/10.2147/BTT.S394843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Doris Benbrook
Jolijn R van Leeuwen,1,* Tamara Popov,2,* Achim Obergfell,2 Ton J Rabelink,1 YK Onno Teng1
1Center of Expertise for Lupus-, Vasculitis- and Complement-Mediated Systemic Diseases (LuVaCs), Department of Internal Medicine - Nephrology Section, Leiden University Medical Center, Leiden, the Netherlands; 2Vifor Pharma Ltd, Glattbrugg, Switzerland
*These authors contributed equally to this work
Correspondence: YK Onno Teng, Department of Nephrology, Leiden University Medical Center (LUMC), P.O. Box 9600, 2300 RC, Leiden, the Netherlands, Tel +31-071-5262148, Fax +31-071-5266868, Email [email protected]
Introduction
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a heterogeneous group of rare, life-threatening, systemic autoimmune disorders characterized by necrotizing vasculitis that predominantly affects the small blood- to medium-sized vessels. Patients with ANCA vasculitis experience side effects from immunosuppression used to achieve disease remission, notably from long-term use of glucocorticoids.1 Both a Phase 2 trial (CLEAR) and a Phase 3 pivotal trial (ADVOCATE) have demonstrated the potential for avacopan to reduce steroid use in patients with newly diagnosed or relapsing severe ANCA-associated vasculitis while maintaining efficacy and safety.2,3 Avacopan is an orally administered small-molecule C5a receptor (C5aR) antagonist that selectively blocks the effects of C5a through the C5aR, including blocking neutrophil chemoattraction and activation.3 Most recently, avacopan has been approved by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) for the treatment of ANCA-associated vasculitis.4 In between the completion of the ADVOCATE study (2019) and the approval of regulatory agencies, 30 patients with a high unmet medical need have been treated with avacopan through the Early Access Program (EAP).5,6 Eligible for the EAP were patients with new or relapsing life- or organ-threatening ANCA-associated vasculitis, requiring an induction treatment, who also had a high risk of steroid-related complications.5
Methods
Here we describe the safety of avacopan within the EAP recorded in a global safety database between February 2, 2019, and November 30, 2021. Each patient qualified for inclusion in the managed access program when physicians confirmed patients’ informed consent after receiving all relevant information on the product and adverse event reporting. All data included in this analysis were conducted in accordance with the ethical principles that comply with the Declaration of Helsinki and are consistent with guidelines on good clinical practice (GCP) and applicable regulatory requirements.
All cases in this analysis are reported in the pharmacovigilance database and are received as solicited reports which are defined as those obtained from an organized data-collection method and were medically reviewed for clinical content, which includes medical history, concomitant medications, and possible causal relationship of AE to drug using the WHO-Uppsala Monitoring Centre Standardized Causality Assessment System. For the present report, definitions of adverse events (AEs) and serious adverse events (SAEs) were used according to the EMA guidelines.
Importantly, all physicians managing patients in the EAP had previous experience with avacopan in the ADVOCATE study and were experienced in recognizing AEs and adverse drug reactions (ADRs). All physicians agreed to report AEs and ADRs and received continuous updates on AEs from all avacopan studies as part of good clinical practice regulations. At the same time, additional measures were undertaken to minimize the risk of underreporting of SAEs including safety training and reminders.
Results
Overall, 30 patients with ANCA-associated vasculitis had avacopan exposure during 3 years of EAP. Supplementary Table 1 presents distribution of patients for sex, age, country, and exposure time. Average duration of avacopan treatment was 11.5 months, as assessed through the number of monthly dispensed bottles (total 346 ranging from 1 to 25 bottles per patient). Currently, 9 patients are still receiving avacopan under the EAP.
A total of 8 individual case safety reports (ICSRs) in 8 patients (27%) were retrieved from the global safety database with 24 events reported, while no adverse events were reported in 22 patients (73%). No deaths were reported. Fifteen events in 5 patients (16.7%) were considered SAEs and are listed per System Organ Class (SOC) in Table 1. A complete list of AEs, including SAEs is available in Supplementary Table 2. Focusing on SAEs, 4/15 were categorized as infection-related events occurring in 2 patients (6.7%) and resulting in 3 hospital admissions. Four renal SAEs were observed in 3 (10%) patients. This included one case of end-stage renal disease (ESRD) after 2 months of avacopan treatment in a patient who previously refused therapy with steroids and had hemodialysis noted in the medical history. This SAE was assessed as not related to avacopan by the treating physician. Only one SAE of special interest, as defined during the clinical trial program, occurred during the EAP (lymphopenia). This was assessed as unrelated to avacopan but rather to concomitant rituximab.
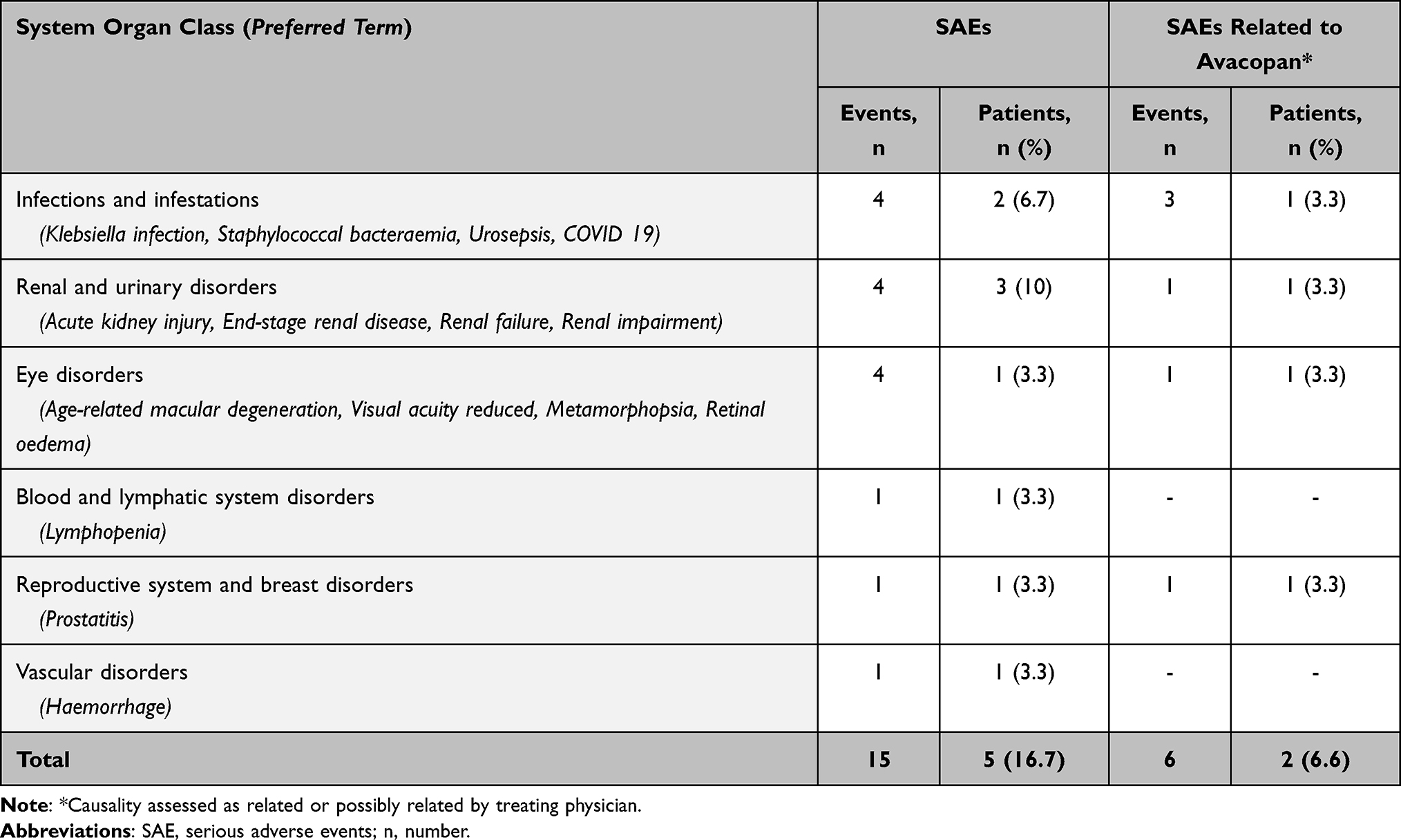 |
Table 1 Serious Adverse Events (SAEs) and SAEs Related or Possibly Related to Avacopan During the EAP |
Five SAEs in 1 patient were assessed as related to avacopan by the treating physician and included acute kidney injury, Klebsiella infection, prostatitis, staphylococcal bacterial infection and urosepsis during one hospitalization. Confounding factors were the patient’s history with bladder carcinoma and urinary infections. One SAE (worsening of previously diagnosed age-related macular degeneration) and two AEs (erythematous rash and dysgeusia) were assessed as possibly related to avacopan by the treating physician. Of these (possibly) related (S)AEs, only dysgeusia led to discontinuation of avacopan within 3 months after the (S)AE. Four patients discontinued avacopan due to (S)AEs unrelated to avacopan (ESRD, lymphopenia, inability to swallow, malaise). In one patient, avacopan was temporarily discontinued during hospitalization for a COVID-19 infection.
Focusing on four of six patients with an avacopan treatment duration of less than 3 months: Reasons for discontinuation were lymphopenia, end-stage renal disease, inability to swallow and dysgeusia. As mentioned, only dysgeusia was assessed as possibly related to avacopan by the treating physician. For the other two patients without AEs reported the reason for discontinuation is unknown.
Discussion
Here we describe the first safety summary of avacopan use in patients with ANCA-associated vasculitis outside clinical trials. No new or elevated safety signal was observed. Per the experience from the clinical trials of avacopan in patients with ANCA-associated vasculitis, the most frequently reported SAEs were infections and renal disorders. Due to the nature of an early access program, clinical data are lacking and would require an observational cohort study with accompanied consent of patients and physicians. As such, the present study focused on physician-reported safety and could not correct for confounders including concomitant medications and the activity status and underlying history of ANCA-associated vasculitis. This also impedes a thorough assessment of the causality between avacopan and an AE afterwards. As so, we used the assessment of the treating physicians, whom all had experience with avacopan and concomitant medications and whom received regular updates of global safety reports on the use of avacopan.
Currently, the only available published safety data on avacopan usage can be derived from the phase 2 CLEAR and CLASSIC studies and phase 3 ADVOCATE study.2,3,7 When comparing safety results between the EAP and these clinical trials, the differences between the nature of these studies should be considered. One needs to consider the inherent limitations of an EAP, where the lack of monitoring of AE reporting can result in limited medical information on AEs and potential under-reporting of (S)AEs. Given these limitations, post approval studies which can assess complete medical data of a large group of patients are essential to increase knowledge on safety and efficacy of avacopan. However, since all participating physicians in the EAP were ADVOCATE investigators with previous avacopan experience and safety training, including recognizing AEs, we assume the underreporting of SAEs, hospitalizations and AEs leading to discontinuation of avacopan is minimal. In this regard, the observed SAEs in the EAP (16.7%) were not elevated compared to the previously reported CLEAR (25%), CLASSIC (17%) and ADVOCATE (42.2%) studies. Discontinuation of avacopan was comparable in the EAP (16.7%) and the CLEAR (2.3%), CLASSIC (14%) and ADVOCATE (15.7%) studies. Also, no increase in patients with hospitalizations (6.7%) was reported despite less strict exclusion criteria for the EAP, which could have resulted in more vulnerable patients.
Conclusion
Collectively, based on the 30 patients over almost 3 years in the avacopan EAP, we describe a safety profile that is consistent with the clinical trial experience. However, given the limitations of an EAP, the small number of patients and short observation period, it is important that pharmacovigilance surveillance remains ongoing when avacopan gains global market access as treatment for ANCA-associated vasculitis.
Acknowledgments
All authors declare that the results presented in this paper have not been published previously in whole or part, except in abstract format. The abstract was presented at the ASN kidney week 2022: https://www.asn-online.org/education/kidneyweek/2022/program-abstract.aspx?controlId=3769111.
Disclosure
Achim Obergfell is a shareholder of Vifor Pharma. YK Onno Teng has received an unrestricted research grant and consultancy fees from Vifor Pharma. The work of YK Onno Teng is supported by the Dutch Kidney Foundation (17OKG04) and by the Arthritis Research and Collaboration Hub (ARCH) foundation. ARCH is funded by Dutch Arthritis Foundation (ReumaNederland). The authors report no other conflicts of interest in this work.
References
1. Yates M, Watts R. ANCA-associated vasculitis. Clin Med. 2017;17(1):60–64. doi:10.7861/clinmedicine.17-1-60
2. Jayne DRW, Bruchfeld AN, Harper L, et al. Randomized trial of C5a receptor inhibitor avacopan in ANCA-associated vasculitis. J Am Soc Nephrol. 2017;28(9):2756–2767. doi:10.1681/ASN.2016111179
3. Jayne DRW, Merkel PA, Schall TJ, Bekker P. Avacopan for the treatment of ANCA-associated vasculitis. N Engl J Med. 2021;384(7):599–609. doi:10.1056/NEJMoa2023386
4. Vifor Pharma press releases. VFMCRP receives EU approval for Tavneos® for the treatment of ANCA associated vasculitis; 2022. Available from: https://www.viforpharma.com/sites/vifor-corp/files/media/vifor-pharma-press-release-tavneos-granted-eu-approval-190122.pdf.
5. van Leeuwen JR, Bredewold OW, van Dam LS, et al. Compassionate use of avacopan in difficult-to-treat antineutrophil cytoplasmic antibody-associated vasculitis. Kidney Int Rep. 2022;7(3):624–628. doi:10.1016/j.ekir.2021.11.036
6. Gabilan C, Pfirmann P, Ribes D, et al. Avacopan as first-line treatment in antineutrophil cytoplasmic antibody-associated vasculitis: a steroid-sparing option. Kidney Int Rep. 2022;7(5):1115–1118. doi:10.1016/j.ekir.2022.01.1065
7. Merkel PA, Niles J, Jimenez R, et al. Adjunctive treatment with avacopan, an oral C5a receptor inhibitor, in patients with antineutrophil cytoplasmic antibody-associated vasculitis. ACR Open Rheumatol. 2020;2(11):662–671. doi:10.1002/acr2.11185
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.