Back to Journals » Clinical Ophthalmology » Volume 17
Preferred Practice Patterns of Congenital Nasolacrimal Duct Obstruction in Jordan
Authors Abu Serhan H ![]() , AlSamhori JF
, AlSamhori JF ![]() , Siddiq A
, Siddiq A ![]() , Hassan AR, Irshaidat S
, Hassan AR, Irshaidat S ![]() , Abu Serhan L, Alawadhi A, Abdelaal A, Al-Thawabieh W
, Abu Serhan L, Alawadhi A, Abdelaal A, Al-Thawabieh W
Received 12 May 2023
Accepted for publication 23 June 2023
Published 11 August 2023 Volume 2023:17 Pages 2309—2322
DOI https://doi.org/10.2147/OPTH.S421054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hashem Abu Serhan,1 Jehad Feras AlSamhori,2 Abdelmonem Siddiq,3 Abdul Rhman Hassan,4 Sara Irshaidat,5 Leen Abu Serhan,6 Abdullah Alawadhi,7 Abdelaziz Abdelaal,8 Wejdan Al-Thawabieh9
1Department of Ophthalmology, Hamad Medical Corporations, Doha, Qatar; 2Faculty of Medicine, University of Jordan, Amman, Jordan; 3Faculty of Pharmacy, Mansoura University, Mansoura, Egypt; 4Department of Ophthalmology, Visual and Anatomical Sciences, Wayne State University School of Medicine, Detroit, MI, USA; 5Department of Pediatrics, King Hussein Cancer Center, Amman, Jordan; 6Faculty of Medicine, Hashemite University, Zarqa, Jordan; 7Department of Ophthalmology, Islamic Hospital, Amman, Jordan; 8Harvard Medical School, Postgraduate Medical Education, Boston, MA, USA; 9Department of Ophthalmology, Dr. Sulaiman Al Habib Hospital, Riyadh, Saudi Arabia
Correspondence: Hashem Abu Serhan, Department of Ophthalmology, Hamad Medical Corporations, PO 3050, Doha, Qatar, Tel +974-77912335, Email [email protected]
Purpose: Congenital nasolacrimal duct obstruction (CNLDO) is fairly common in newborns. The main aim of this cross-sectional study is to assess the preferred practice patterns of CNLDO among ophthalmologists in Jordan.
Methods: This cross-sectional study was conducted across all ophthalmological practices in Jordan, using convenience sampling. An online questionnaire, designed through Google Forms, was distributed through social media. The survey contained four domains: baseline characteristics of participants and the diagnosis (7 items), medical management (3 items), and surgical management (11 items) of CNLDO. Descriptive statistics were conducted using SPSS (IBM SPSS Corp, SPSS Statistics ver. 26, USA).
Results: Eighty-three physicians responded to the survey, with an average age of 40.6 ± 8.6. More than half of the participants (53.0%, n = 44) were general ophthalmologists. Only 37.3% of our sample (n = 31) regularly evaluated the refraction of a child presenting with epiphora suggestive of CNLDO. Criggler’s nasolacrimal duct massage was recommended by 62.7% of respondents (n = 52) for up to 12 months. In addition, 72.3% of respondents (n = 60) recommended 12 months as the minimum age for primary probing of CNLDO. Silicon intubation was considered for primary probing starting at 24 months by 31.3% of ophthalmologists (n = 20). Monocanalicular stent was preferred by 42.2% of respondents (n = 27) while 31.3% (n = 20) preferred bicanalicular stent.
Conclusion: There is considerable variability in preferred practice patterns regarding the diagnosis and management of CNLDO in Jordan. Our findings highlight the gaps in optimum practices which need to be addressed for better management.
Keywords: nasolacrimal duct obstruction, CNLDO, lacrimal system, practice patterns, congenital
Introduction
Congenital nasolacrimal duct obstruction (CNLDO) is a common disorder among children occurring in 6–20% of children with 80% of the cases are unilateral.1 The pathogenesis of the CNLDO is due to mechanical membranous obstruction at the valve of Hasner due to failure of recanalization, just before the nasolacrimal duct inserts in the nasal cavity.2 The mechanical obstruction could be also due to facial bone abnormality or stenosis of the distal part of the nasolacrimal duct at the inferior meatus.3 Genetic predisposition, intrapartum infection, prematurity, and exposure to radiation or certain medications are some of the risk factors for CNLDO.4,5 The nasolacrimal duct is essential for the drainage of tears. Tears are synthesized in the lacrimal gland with the physiological function of lubricating the eyes. They are normally drained from the lacrimal sac to the nasal cavity through the nasolacrimal duct at the inferior meatus of the nasal cavity. Therefore, CNLDO leads to an abnormal overflow of tears onto the face termed epiphora.6 Infections could occur on the top of CNLDO, presenting with mucinous discharge, eyelashes crusting, and eyelid dermatitis.7 Furthermore, the persistence of CNLDO can lead to chronic preseptal and orbital cellulitis as well as dacryocystitis.8
Diagnosis of CNLDO is clinical and can be confirmed using the fluorescein dye disappearance test.9 During their first year of life, 80–90% of CNDO resolve either spontaneously or with conservative management.10 Probabilities of spontaneous resolution by month until 12 months of age are 80–90% at 3 months of age, 68–75% at 6 months of age, and 36–57% at 9 months of age.11 Conservative measures include massaging the lacrimal sac using Criggler’s technique as well as antibiotics in the presence of bacterial infection of the stagnant tears. When conservative measures fail, probing of nasolacrimal duct is the first line of management. In children younger than 18 months old, success rates of 77% to 97% have been reported.12 However, the optimal timing of probing remains controversial. The main problem is that spontaneous resolution can occur after 13 months of age. Rates of spontaneous resolution of CNDO at 13–24 months of age are 60.0–79.3%. In addition, spontaneous resolution of CNDO with conservative therapies can occur up to 48 months of age. On the other hand, Young et al13 reported that the cure rate for cases with probing performed at 12–24 months of age was significantly higher than that for spontaneous resolution. Other available interventions are balloon catheter dilation and duct intubation, and external or endoscopic dacryocystorhinostomy (DCR).14,15
The main aim of this cross-sectional study is to assess the preferred practice patterns of CNLDO among ophthalmologists in Jordan. Building a consensus on the preferred management paradigm of CNLDO will help both physicians and patients. To our knowledge, this is the first study evaluating the preferred practice patterns of CNLDO among ophthalmologists in Jordan.
Methods
Study Design and Participants
This is a descriptive, cross-sectional study that was conducted using an online questionnaire targeting all ophthalmologists practicing in Jordan including public, private, and university hospitals. We followed the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) in conducting the questionnaire (Appendix 1).16 Data was collected using web-based questionnaire software (Google forms). Participants were recruited through social media (E-mail, Facebook, and WhatsApp) by sending an invitation to complete the questionnaire after providing a brief description of the study from September to December 2022. Participants were informed before starting the questionnaire that it is completely anonymous, and voluntary and that all data would be treated as confidential.
Items in the Survey
A 20-minute online survey on Google form that was based on current scientific literature by referring to the literature and included main ideas and primary items relevant to our topic was used in this study. The face and content validity of the questionnaire was established by reviewing the questionnaire by 5 experts in the field who provided their feedback and suggested necessary changes. The reliability of the questionnaire was established through pilot testing by collecting data from 20 general ophthalmologists who were asked to provide their feedback and these were not included in the study sample. The questionnaire was completely anonymous and did not contain any identifying information. To ensure that it was impossible to link responses with their providers, the Internet protocol address was omitted from individual responses at the time of analysis.
The survey consisted of four attributes. The first section is for demographic data of the participants who were asked to report their age, gender, specialty, years of experience, and type of practice. The second section included seven questions on the diagnostic approach of CNLDO. The third section included three questions investigating the medical management of CNLDO including Criggler’s massage, and probing. The last section included 11 questions targeting the surgical management of CNLDO including in-fracture of the inferior turbinate, silicon intubation, balloon catheter dilatation, and DCR. The questionnaire items are included in Appendix 2.
Sample Size and Sampling Technique
The sample size was calculated using epiinfoTM v.7.2.4.0 (epiinfoTM, version 7.2.4.0, a database and statistics program for public health professionals. CDC, Atlanta, GA, USA, 2011) considering a previous study performed in Jordan with an applied reliability of 0.749 (ie, Cronbach’s alpha).17 Using a cross-sectional study design, where n = required sample size (n = Z (α/2) 2 pq/d2), we calculated the sample size based on the following parameters:
Prevalence of 480 registered ophthalmologists,18 Cronbach’s alpha of 0.749, 99.99% confidence interval (CI), and 5% margin of error. We estimated 41 as the minimum sample size required to represent the true population. A total of 83 subjects were included in this study.
Data Analysis
The information was taken from Google Forms and converted to an Excel spreadsheet before being entered into the Statistical Package for Social Sciences (SPSS) version 27 (IBM SPSS Corp, SPSS Statistics ver. 26, USA). Descriptive analysis was used to display categorical variables as percentages and frequencies while presenting numerical variables as a mean and standard deviation to evaluate the data quantitatively. The significance of the data was determined using a categorical Chi-square test. All statistical tests were conducted with a 95% confidence interval and a 5% error margin. A p-value of less than 0.05 was considered statistically significant.
Ethical Approval
The Institutional Review Board committee of the Islamic Hospital, Amman, Jordan, considered this study to be exempt from IRB review and approval. All study procedures were conducted according to the principles of the World Medical Association Declaration of Helsinki and its amendments.19
Results
Demographic Characteristics of Participants
Eighty-three physicians responded to the survey, with an average age of 40.6 ± 8.6. Males made up 63.9% (n = 53) of the total, while female respondents made up 36.1% (n = 30). The majority of participants (61.4%, n = 61) had less than ten years of experience. More than half of the participants (53.0%, n = 44) were general ophthalmologists. Thirty-six of them (43.4%) worked in private practice. Table 1 shows the demographic characteristics of participants.
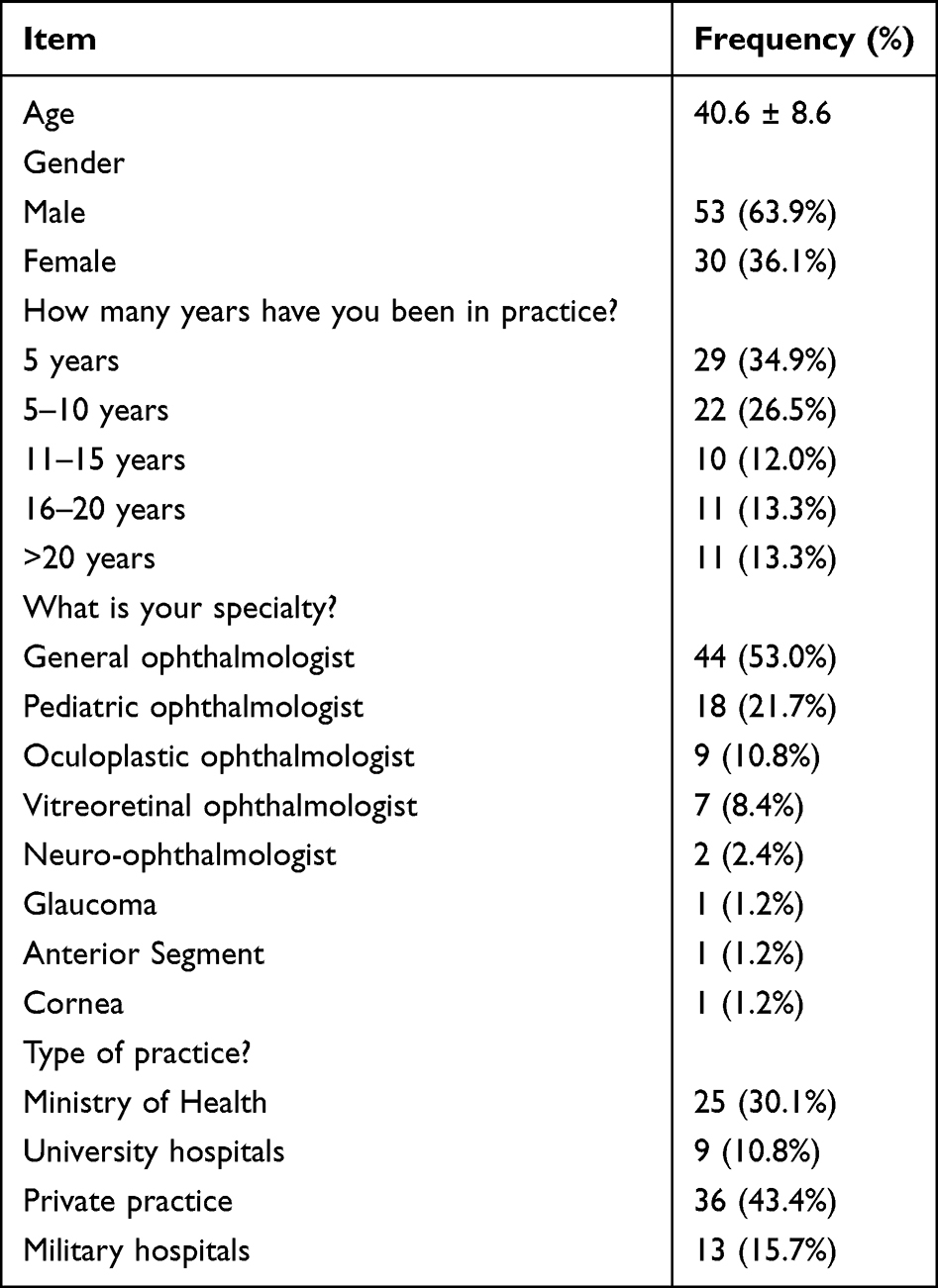 |
Table 1 Demographic Characteristics of the Participants |
Diagnostic Approach of Congenital Nasolacrimal Duct Obstruction
For a child presenting with epiphora suggestive of CNLDO, 49.4% of ophthalmologists (n = 41) used fluorescein dye to estimate the lacrimal lake and confirm the diagnosis. Chi-square test was conducted to evaluate the association between the usage of fluorescein dye and the usage of Dye Disappearance test (DDT) in the diagnosis of CNLDO. It was found that physicians who always used fluorescein dye would use DDT in aiding the diagnosis. (x2= 63.34, p-value <0.001). Furthermore, 50.6% of ophthalmologists (n = 42) inspect the inferior puncta at least to check for patency of lacrimal puncta for a child presenting with epiphora. Only 37.3% of our sample (n = 31) regularly evaluated the refraction of a child presenting with epiphora suggestive of CNLDO. Almost 44.6% of ophthalmologists (n = 37) would consider congenital glaucoma as one of the differential diagnoses for a child with epiphora. Table 2 shows the preferred practice patterns of the diagnostic approach of CNLDO.
 |
Table 2 Preferred Practice Patterns of the Diagnostic Approach of CNLDO |
Medical Management of Congenital Nasolacrimal Duct Obstruction
Criggler’s nasolacrimal duct massage was recommended by 62.7% of respondents (n = 52) for up to 12 months. In addition, 72.3% of respondents (n = 60) recommended 12 months as the minimum age for primary probing of CNLDO. In terms of surgical management of CNLDO, 37.3% of ophthalmologists (n = 31) would not treat CNLDO surgically. However, they would prefer to refer them for probing at or before the age of 18 months. Table 3 shows the preferred practice patterns of medical management of CNLDO.
 |
Table 3 Preferred Practice Patterns of Medical Management of CNLDO |
Surgical Management of Congenital Nasolacrimal Duct Obstruction
Simple probing was preferred as the first intervention for a child presenting with CNLDO by 39.1% of respondents (n = 25) at the age of 12 months. Most of respondents (64.1%, n = 41) do not have the experience to do infracture of inferior turbinate while 17.2% of them (n = 11) do it for cases with failed probing. Silicon intubation was considered for primary probing starting at 24 months by 31.3% of ophthalmologists (n = 20). Monocanalicular stent was preferred by 42.2% of respondents (n = 27) while 31.3% (n = 20) preferred bicanalicular stent. If silicon intubation (stent) was used during the procedure, 50.0% of them (n = 32) would wait 3 months before removal of stent while 37.5% (n = 24) would wait for 6 months to remove it. For the child presenting with epiphora suggestive of CNLDO with no history of any intervention, 40.6% (n = 26) of respondents would never perform DCR as a primary procedure. In case of a failed primary simple probing, 42.2% of them (n = 27) would repeat probing with silicon tube stenting regardless of the age, on contrary, 23.4% of them (n = 15) would refer failed cases to oculoplastic or pediatric ophthalmologists. Table 4 shows the preferred practice patterns of surgical management of CNLDO.
 |
Table 4 Preferred Practice Patterns of Surgical Management of CNLDO |
Effect of Specialty on the Preferred Practice Patterns of Congenital Nasolacrimal Duct Obstruction
Chi-square test was conducted to assess the effect of the specialty of the participants as general or pediatric/specialized ophthalmologists on their preferred practice patterns of CNLDO. For a child presenting with epiphora suggestive of CNLDO, there was significant difference between the practice of general and pediatric ophthalmologists. Pediatric ophthalmologists (54.2%, n = 13) were more capable to test refraction than general ophthalmologists (45.8%, n = 11) (p-value= 0.002). Furthermore, 80% of general ophthalmologists (n = 36) would recommend probing/surgical management of CNLDO at 12 months, on the other hand, only 20% of pediatric ophthalmologists (n = 9) would recommend it at 12 months (p-value=0.03). For a CNLDO with failed primary simple probing, 57.1% of general ophthalmologists (n = 8) would prefer repeating simple probing in comparison to 42.9% of pediatric ophthalmologists (n = 6) (p-value= 0.010). When comparing between general and specialized ophthalmologists in their preferred practice with infracture of inferior turbinate, 58.5% of general ophthalmologists stated that they never done it before (n = 24) while 41.5% of specialized ophthalmologists did not (n = 17) (p-value= 0.014). Table 5 shows the effect of specialty on the preferred practice patterns of CNLDO.
 |
Table 5 The Effect of Specialty on the Preferred Practice Patterns of CNLDO |
Discussion
Despite the fact that most cases of CNLDO resolve spontaneously within the first year of life, some could persist beyond this date and cause huge distress to both child and family. Therefore, a proper therapeutic strategy for CNLDO is essential. Management lines of CNLDO include observation, medical, and surgical management.20,21 Massaging the lacrimal sac using Criggler’s technique is usually the first preferred management line. Kushner B22 reported that Criggler’s technique speeds resolution of CNLDO through increasing the hydrostatic pressure, which leads to rupture of the membranous obstruction in the valve of Hasner with high success rates. In our study, 62.7% of respondents (n = 52) recommended Criggler’s nasolacrimal duct massage for up to 12 months. Probing is usually considered the first intervention performed for CNLDO failed conservative measures.10 Despite the fact that the cure rates for early probing reach 78–100% during the first 12 months of age, these are no different to rates for spontaneous resolution up to 12 months of age.11,23 Repka et al12 reported that primary probing in children with CNLOD success rates were 78% overall and was 78% for subjects aged 6 to <12 months, 79% for subjects aged 12–36 months, and 56% for subjects aged 36–48 months. Also, they reported that success rates were lower in eyes operated in an office setting compared with in an operating theatre (ARR = 0.88 [95% CI = 0.80 to 0.96]). Furthermore, they found that success rates were lower in eyes of subjects with bilateral CNLDO (ARR = 0.88 [95% CI = 0.81 to 0.95]).12 Nevertheless, probing may injure the nasolacrimal duct epithelium leading to cicatricial fibrosis and thus preventing the spontaneous resolution of CNLDO.11 Resolution rates of second probing are largely reduced.24 Kakizaki et al25 reported that the cure rates of primary probing were 92% in the first year, 84.5% in the second year, 65% in the third year, and 63.5 in the fourth and fifth years of age. Furthermore, probing could be complicated with bleeding and canalicular obstructions, which occurs in 20% and 44% of cases, respectively.25 Hence, a “wait-and-see” approach with conservative measures is recommended to prevent such iatrogenic complications. Honavar et al26 recommended that early probing before 12 months of age should be withheld if symptoms such as dacryocystitis or severe blepharitis are absent.
There are several treatment options for CNLDO if a primary probing failed. These include inferior turbinate fracture, repeated probing, balloon catheter dilation, silicone tube intubation and dacryocystorhinostomy (DCR). Monocanalicular silicone intubation offers high success rates for CNLDO. Engel et al15 reported 97% success rate when performed in children younger than 24 months of age. However, bicanalicular silicone intubation has been used more frequently because it is generally more tolerated by the cornea.27 Andalib et al’s28 study showed no difference in outcomes between monocanalicular and bicanalicular stenting. In addition to that, they found that monocanalicular stenting is easier in tube removal without sedation in the office.28 In our study, monocanalicular stent was preferred by 42.2% of respondents (n = 27) while 31.3% (n = 20) preferred bicanalicular stent. Dacryocystorhinostomy is considered the last resort and usually indicated for failure of standard probing, balloon dilation and/or stents.29 External DCR is the more common modality; nonetheless, due to technological advances, endoscopic DCR has recently gained popularity.30 The success rates of DCR in children are high reaching 88–96% for external and 82–92% endoscopic approaches.31 However, continuous changing anatomy in children, poor-defined anatomy and extensive development of fibrosis have all been proposed as variables that limit surgical outcomes of DCR in children.32
Interestingly, untreated CNLDO has been identified as a risk factor for the development of amblyopia.33 Silbert et al34 reported 22% prevalence of amblyopia in patients with CNLDO. This could be explained that excessive tearing in CNLDO causes blurred vision and form-deprivation amblyopia during the sensitive period of visual development.35 In our study, only 37.3% of respondents (n = 31) regularly evaluated the refraction of a child presenting with epiphora suggestive of CNLDO. Thus, children with symptoms of CNLDO required a thorough eye examination including a cycloplegic refraction and subsequent follow-up to prevent amblyopia. This is especially critical for general ophthalmologists since they reported less practice to evaluate the refraction for a child with CNLDO.
This study is considered to be a guide to identify the preferred practice patterns of ophthalmologists regarding the management of CNLDO in order to be able to identify the knowledge gap and faulty practice that can be corrected with clear guidelines setting. In addition, to provide general ophthalmologists better insights regarding their practice for children with CNLDO. Limitations of the study are the small number of participants which may create a risk for selection bias as the data of who responded will be different from other who do not respond to the questionnaire. Moreover, these are considered self-reported practice preferences of ophthalmologists in Jordan and not the results of a randomized clinical trial. Thus, interpretation of our findings should be with caution and limited to what is more commonly accepted in the international levels without implying that less common practices are necessarily incorrect.
Conclusions
Congenital nasolacrimal duct obstruction (CNLDO) is a common disorder among children. There is considerable variability in preferred practice patterns regarding the diagnosis and management of CNLDO in Jordan. Our findings highlight the gaps in optimum practices which need to be addressed for better management. Larger prospective studies are recommended to establish a consensus on the best approach for patients with CNLDO.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
The study was conducted according to the Helsinki Declaration principles and was reviewed and the Institutional Review Board committee of the Islamic Hospital, Amman, Jordan, considered this study to be exempt from IRB review and approval.
Consent to Participate Statement
Informed consent was obtained from all participants included in the study.
Acknowledgment
The publication of this article was funded by the Qatar National Library.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Olitsky SE. Update on congenital nasolacrimal duct obstruction. Int Ophthalmol Clin. 2014;54(3):1–7. doi:10.1097/IIO.0000000000000030
2. Petersen RA, Robb RM. The natural course of congenital obstruction of the nasolacrimal duct. J Pediatr Ophthalmol Strabismus. 1978;15(4):246–250. doi:10.3928/0191-3913-19780701-14
3. Moscato EE, Kelly JP, Weiss A. Developmental anatomy of the nasolacrimal duct: implications for congenital obstruction. Ophthalmology. 2010;117(12):2430–2434. doi:10.1016/j.ophtha.2010.03.030
4. Aldahash FD, Al-Mubarak MF, Alenezi SH, et al. Risk factors for developing congenital nasolacrimal duct obstruction. Saudi J Ophthalmol. 2014;28(1):58–60. doi:10.1016/j.sjopt.2013.09.007
5. Schellini SA, Ariki CT, Sousa RLF, et al. Management of congenital nasolacrimal duct obstruction--Latin American study. Ophthalmic Plast Reconstr Surg. 2013;29(5):389–392. doi:10.1097/IOP.0b013e31829bb162
6. MacEwen CJ, Young JD. Epiphora during the first year of life. Eye. 1991;5(Pt 5):596–600. doi:10.1038/eye.1991.103
7. Lorena SH, Silva JA, Scarpi MJ. Congenital nasolacrimal duct obstruction in premature children. J Pediatr Ophthalmol Strabismus. 2013;50(4):239–244. doi:10.3928/01913913-20130423-01
8. Bekmez S, Eriş E, Altan EV, et al. The role of bacterial etiology in the tear duct infections secondary to congenital nasolacrimal duct obstructions. J Craniofac Surg. 2019;30(7):2214–2216. doi:10.1097/SCS.0000000000005798
9. Schellini SA, Hoyama E, Rocha MC, et al. Evaluation of lacrimal system outflow in the newborn by dye tests. Orbit. 2000;19(3):137–142. doi:10.1076/orbi.19.3.137.2662
10. Takahashi Y, Kakizaki H, Chan WO, et al. Management of congenital nasolacrimal duct obstruction. Acta Ophthalmol. 2010;88(5):506–513. doi:10.1111/j.1755-3768.2009.01592.x
11. Kakizaki H, Takahashi Y, Kinoshita S, Shiraki K, Iwaki M. The rate of symptomatic improvement of congenital nasolacrimal duct obstruction in Japanese infants treated with conservative management during the 1st year of age. Clin Ophthalmol. 2008;2(2):291–294. doi:10.2147/OPTH.S2582
12. Repka MX, Chandler DL, Beck RW, et al. Primary treatment of nasolacrimal duct obstruction with probing in children younger than 4 years. Ophthalmology. 2008;115(3):577–584.e3.
13. Young JD, MacEwen CJ, Ogston SA. Congenital nasolacrimal duct obstruction in the second year of life: a multicentre trial of management. Eye. 1996;10(Pt 4):485–491. doi:10.1038/eye.1996.107
14. Saniasiaya J, Abdullah B, Husain S, et al. Primary endoscopic endonasal dacryocystorhinostomy for pediatric nasolacrimal duct obstruction: a systematic review. Am J Rhinol Allergy. 2017;31(5):328–333. doi:10.2500/ajra.2017.31.4464
15. Engel JM, Hichie-Schmidt C, Khammar A, et al. Monocanalicular silastic intubation for the initial correction of congenital nasolacrimal duct obstruction. J Aapos. 2007;11(2):183–186. doi:10.1016/j.jaapos.2006.09.009
16. Eysenbach G. Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34. doi:10.2196/jmir.6.3.e34
17. Alsaad M, Shehadeh A. Knowledge, attitude, and practice of different specialties about congenital nasolacrimal duct obstruction: a cross- sectional study in Jordan. Int Med J. 2019;24:1.
18. Alkilany M. Jordanian ophthalmologists plan regional YO chapter; 2020. Available from: https://www.aao.org/young-ophthalmologists/yo-info/article/jordanian-yos-plan-regional-chapter.
19. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
20. Bansal O, Bothra N, Sharma A, et al. Congenital nasolacrimal duct obstruction update study (CUP study): paper I-role and outcomes of Crigler’s lacrimal sac compression. Eye. 2021;35(6):1600–1604. doi:10.1038/s41433-020-01125-1
21. Bothra N, Ali MJ. Congenital nasolacrimal duct obstruction update study (CUP Study): paper 4-Infantile Acute Dacryocystitis (InAD)-presentation, management, and outcomes. Ophthalmic Plast Reconstr Surg. 2022;38(3):270–273. doi:10.1097/IOP.0000000000002077
22. Kushner BJ. Congenital nasolacrimal system obstruction. Arch Ophthalmol. 1982;100(4):597–600. doi:10.1001/archopht.1982.01030030599010
23. Rees MG, Woo CL, Optom B. Pediatric eye disease investigator group amblyopia treatment review. Am Orthopt J. 2007;57:99–103. doi:10.3368/aoj.57.1.99
24. Kapadia MK, Freitag SK, Woog JJ. Evaluation and management of congenital nasolacrimal duct obstruction. Otolaryngol Clin North Am. 2006;39(5):959–77, vii. doi:10.1016/j.otc.2006.08.004
25. Kashkouli MB, Kassaee A, Tabatabaee Z. Initial nasolacrimal duct probing in children under age 5: cure rate and factors affecting success. J Aapos. 2002;6(6):360–363. doi:10.1067/mpa.2002.129041
26. Honavar SG, Prakash VE, Rao GN. Outcome of probing for congenital nasolacrimal duct obstruction in older children. Am J Ophthalmol. 2000;130(1):42–48. doi:10.1016/S0002-9394(00)00388-3
27. Komínek P, Červenka S, Pniak T, et al. Monocanalicular versus bicanalicular intubation in the treatment of congenital nasolacrimal duct obstruction. Graefes Arch Clin Exp Ophthalmol. 2011;249(11):1729–1733. doi:10.1007/s00417-011-1700-2
28. Andalib D, Gharabaghi D, Nabai R, et al. Monocanalicular versus bicanalicular silicone intubation for congenital nasolacrimal duct obstruction. J Aapos. 2010;14(5):421–424. doi:10.1016/j.jaapos.2010.08.003
29. Michael A, Kipp RCA. Congenital Nasolacrimal duct obstruction (NLDO); 2023. Available from: https://www.aao.org/education/oculoplastics-center/congenital-nasolacrimal-duct-obstruction-nldo.
30. Grover AK. Management of nasolacrimal duct obstruction in children: how is it changing? Indian J Ophthalmol. 2017;65(10):910–911. doi:10.4103/ijo.IJO_719_17
31. Leibovitch I, Selva D, Tsirbas A, et al. Paediatric endoscopic endonasal dacryocystorhinostomy in congenital nasolacrimal duct obstruction. Graefes Arch Clin Exp Ophthalmol. 2006;244(10):1250–1254. doi:10.1007/s00417-006-0273-y
32. Nowinski TS, Flanagan JC, Mauriello J. Pediatric Dacryocystorhinostomy. Arch Ophthalmol. 1985;103(8):1226–1228. doi:10.1001/archopht.1985.01050080138035
33. Ramkumar VA, Agarkar S, Mukherjee B. Nasolacrimal duct obstruction: does it really increase the risk of amblyopia in children? Indian J Ophthalmol. 2016;64(7):496–499. doi:10.4103/0301-4738.190101
34. Silbert DI, Matta NS, Quintanal A, et al. Incidence of amblyopia risk factors in children with nasolacrimal duct obstruction. J AAPOS. 2013;17(6):618. doi:10.1016/j.jaapos.2013.06.019
35. Ellis JD, MacEwen CJ, Young JD. Can congenital nasolacrimal-duct obstruction interfere with visual development? A cohort case control study. J Pediatr Ophthalmol Strabismus. 1998;35(2):81–85. doi:10.3928/0191-3913-19980301-05
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.