Back to Journals » Journal of Pain Research » Volume 19
Preferences and Participation Factors of a Web-Based Mind–Body Intervention for Chronic Orofacial Pain: A Qualitative Study
Authors Lovette BC ![]() , Levey N
, Levey N ![]() , Cliff KB, Bakhshaie J, Kulich R
, Cliff KB, Bakhshaie J, Kulich R ![]() , Cheng HT
, Cheng HT ![]() , He S, Vranceanu AM
, He S, Vranceanu AM ![]() , Greenberg J
, Greenberg J ![]()
Received 1 December 2025
Accepted for publication 10 February 2026
Published 23 February 2026 Volume 2026:19 585652
DOI https://doi.org/10.2147/JPR.S585652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Brenda C Lovette,1,2 Nadine Levey,1 Kozbi Bayne Cliff,1 Jafar Bakhshaie,1,2 Ronald Kulich,3 Hsinlin Thomas Cheng,2,4 Shuhan He,2,5 Ana-Maria Vranceanu,1,2 Jonathan Greenberg1,2
1Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA; 2Department of Psychiatry, Harvard Medical School, Boston, MA, USA; 3Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, MA, USA; 4Department of Neurology, Massachusetts General Hospital, Boston, MA, USA; 5Lab of Computer Science, Massachusetts General Hospital, Boston, MA, USA
Correspondence: Jonathan Greenberg, Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, One Bowdoin Square, Suite 648, Boston, MA, 02114, USA, Email [email protected]
Purpose: Chronic orofacial pain (COP) is associated with substantial pain interference and emotional distress. Psychosocial treatments for COP are scarce, rely on talking, which is often painful for this population, and require intensive resources. There is a clear need for a novel, scalable, accessible, “talk free” intervention to reduce pain interference and emotional distress among individuals with COP. This study explored people with COP’s perceptions of a novel mind-body web-based intervention targeting pain interference and emotional distress (Face-Forward-Web) to inform its development and optimization.
Patients and Methods: We conducted semi-structured focus groups (N=4 groups, 22 participants; 77% female; mean age 47 (SD = 15.9)) and used Rapid Data Analysis (RDA) to gauge perceptions of the intervention’s content structure, format, and barriers and facilitators to participation.
Results: Perception of the intervention was largely positive, and participants perceived its value for increasing engagement in life activities. They emphasized the importance of tailoring the intervention to the unique characteristics of COP. They expressed that the self-paced web-based format was ideal given unpredictable pain flares and variable needs. Concurrently, they desired social connection. They perceived the content and skills as helpful and relaxing. They identified barriers and facilitators to participation, including technical considerations, reminders and incentives, and providers setting up realistic expectations for outcomes.
Conclusion: This study elucidates insights that can inform psychosocial and mind-body interventions for people with COP. Findings give voice to the needs and perceptions of people with COP, guiding the development of tailored, patient-informed treatment approaches such as Face-Forward-Web.
Keywords: orofacial pain, qualitative analysis, intervention development, web-based intervention
Introduction
Orofacial pain (ie, pain of the hard or soft tissue of the face, neck, or head) is common1–3 and costly to both individuals and the healthcare system.4,5 Orofacial pain that lasts more than three months is known as chronic orofacial pain (COP)6 and is associated with high levels of pain interference in daily life,7 emotional distress (eg, depression and anxiety),7–12 suicidality,13 and maladaptive forms of coping such as pain catastrophizing and pain-related fear.14–16 While the etiologies of orofacial pain vary,17,18 psychosocial consequences such as activity limitations and reduced quality of life are consistent across underlying conditions and diagnoses17,18 and, when left unaddressed, can worsen over time.19 Despite increasing evidence of the important role psychosocial factors play in COP outcomes,20 such factors are often neglected in COP treatment.12 Addressing the often-overlooked psychosocial correlates of COP is essential to improve COP management and well-being in this patient population.21
Some psychosocial treatments, such as cognitive behavioral therapy (CBT)22–26 and other behavioral interventions,27–29 demonstrate potential in improving outcomes in COP. However, such interventions are resource-intensive (eg, require the availability of a live, trained clinician)30 and costly,31 limiting treatment accessibility. Asynchronous web-based platforms have the potential to circumvent these limitations by enhancing intervention accessibility,31 bypassing mental health stigma,32 and increasing scalability while maintaining effectiveness.21,33,34 Further, most psychosocial interventions take the form of “talk therapy”, which can be painful for individuals with COP and limit their treatment engagement.21,35 To our knowledge, there are no asynchronous, “talk free” web-platforms for COP.
To address the unmet needs of individuals with COP, we developed the prototype of Face-Forward-Web, a novel, web-based, mind-body intervention targeting pain interference, emotional distress, and maladaptive coping among in adults with COP. Face-Forward-Web is asynchronous, self-guided, and talk-free, avoiding pain triggered by speech. Conceptualization and iterative development of Face-Forward-Web is guided by human-centered design principles, a framework that emphasizes the needs of target users to maximize an intervention’s fit and acceptability. In our work, human-centered design elements include clear identification of patients’ needs and preferences, prototyping, and rapid iteration with active stakeholder involvement.36–38 As the first step of this process, qualitative methods offer a powerful means of leveraging the perspectives of people with COP to effectively integrate human-centered design throughout the development process.
Through semi-structured qualitative focus groups, the present study aims to identify the treatment preferences of individuals with COP, as well as their perceived barriers and facilitators to participating in Face-Forward-Web. Results will inform the development and optimization of Face-Forward-Web.
Materials and Methods
This qualitative analysis was part of a larger mixed-methods study aimed at developing and testing Face-Forward-Web, a mind-body intervention for individuals with COP.39 Here, we report on data from qualitative focus groups (N=4) with adults living with COP to understand their treatment preferences, their perceptions of the intervention, and their perceived barriers and facilitators to participation to help inform the iterative process of refining the intervention. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Mass General Brigham (MGB) Institutional Review Board (IRB) approved all study procedures (#2024P001309) and determined that the study is exempt from written informed consent. All participants were presented with a study fact sheet and indicated their consent by clicking a button that they understood the study and agreed to participate.
Participants
We recruited 22 adults with COP through a newsletter distributed by the Facial Pain Association (FPA), provider referrals from the Facial Pain Clinic at MGB, flyer postings at MGB pain clinics, and an online platform which connects MGB researchers with potential patient participants (MGB Rally). Inclusion criteria were as follows: 1) adults over 18 years old, 2) experiencing chronic (lasting more than three months) orofacial pain, whose pain was 3) non-malignant, and 4) clinically significant, evidenced by scoring ≥4 on the Numerical Rating Scale,40 5) were fluent in English, and 6) had reliable access to the internet. Exclusion criteria were: 1) severe untreated mental health disorder (eg, psychosis), 2) any change in and psychotropic medication within six weeks prior to the study, 3) active suicidal ideation with plan or intent, 4) pregnancy, and 5) engagement in a regular mindfulness practice (ie, > 45 minutes/week) or participation in mind-body or cognitive behavioral therapy in the past three months.
Procedures
We developed a semi-structured interview script with open-ended questions and probes about participants’ treatment needs and preferences, their perceptions of the Face-Forward-Web intervention content, skills, and structure, and perceived barriers and facilitators to participation. The script included short breaks for staff to present participants with early stage “sketches” of the intervention. Study staff screened potential participants for eligibility. Staff presented eligible participants with a study fact sheet and obtained their consent for participation in the study. Both the fact sheet and the focus group script included explanation that participants’ verbatim statements will be recorded, deidentified, and used for research purposes. Upon enrollment, participants were scheduled for one of four focus groups and given an electronic demographic questionnaire to complete remotely via Research Electronic Data Capture (ie, REDCap),41 a secure HIPAA-approved survey platform hosted by MGB.
Two PhD-level researchers with training in qualitative interviewing facilitated the focus groups (BCL and JG), which were conducted over a HIPAA compliant version of Zoom. One research assistant (NL) attended each session to take structured field notes for Rapid Data Analysis (RDA) and to provide technical support as needed. Each of the four focus groups (N=7, 8, 4, and 3, respectively) lasted ~60 minutes. We audio-recorded all focus groups and later transcribed the interviews verbatim and de-identified the transcripts. Results of RDA demonstrated thematic saturation after the fourth focus group, thus data collection was concluded.
Data Analysis
For qualitative analysis, we engaged in RDA,42 a valid and reliable method for qualitative data analysis that is frequently used in the iterative development of digital health programs. In contrast to traditional qualitative analysis, which often takes months to complete, RDA is an efficient method which yields more timely actionable results. This approach allowed us to adapt our interview strategies and efficiently integrate major findings into our intervention prototype in real-time, supporting our aim for a user-centered design. Immediately after each focus group, one team member (NL), who has prior experience in qualitative research and analysis, used a template modeled after the interview script to generate a summary of findings including salient participant quotes. The facilitators (BCL and JG) then reviewed, edited and refined its content.43 To enhance rigor, we maintained all iterations of the summaries and matrix along with accompanying researcher notes to establish a comprehensive audit trail. Next, we used hybrid inductive-deductive thematic analysis to restructure results of the RDA matrix into a table that included key domains (deductive), themes (inductive) and corresponding participant quotes. When we needed additional specificity or nuance to refine our results, the research team consulted full transcripts to validate interpretations and enhance the trustworthiness of our findings.
Results
Participant demographic characteristics are presented in Table 1. We organized our qualitative analysis into four domains: general impressions of the intervention, perception of modality and structure, perception of content and skills, and barriers and facilitators to participation. Box 1 displays the themes and subthemes within each domain. Below, we describe the results and include participant quotes to exemplify our findings.
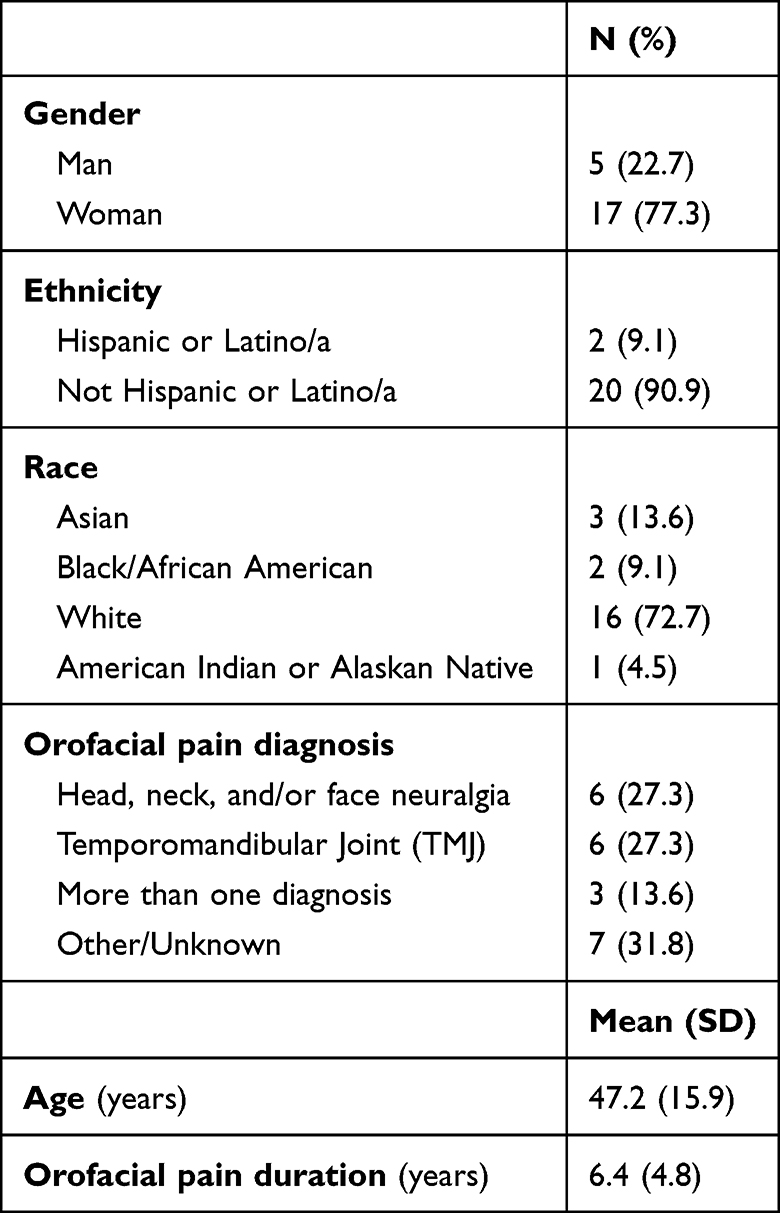 |
Table 1 Participant Demographic Characteristics |
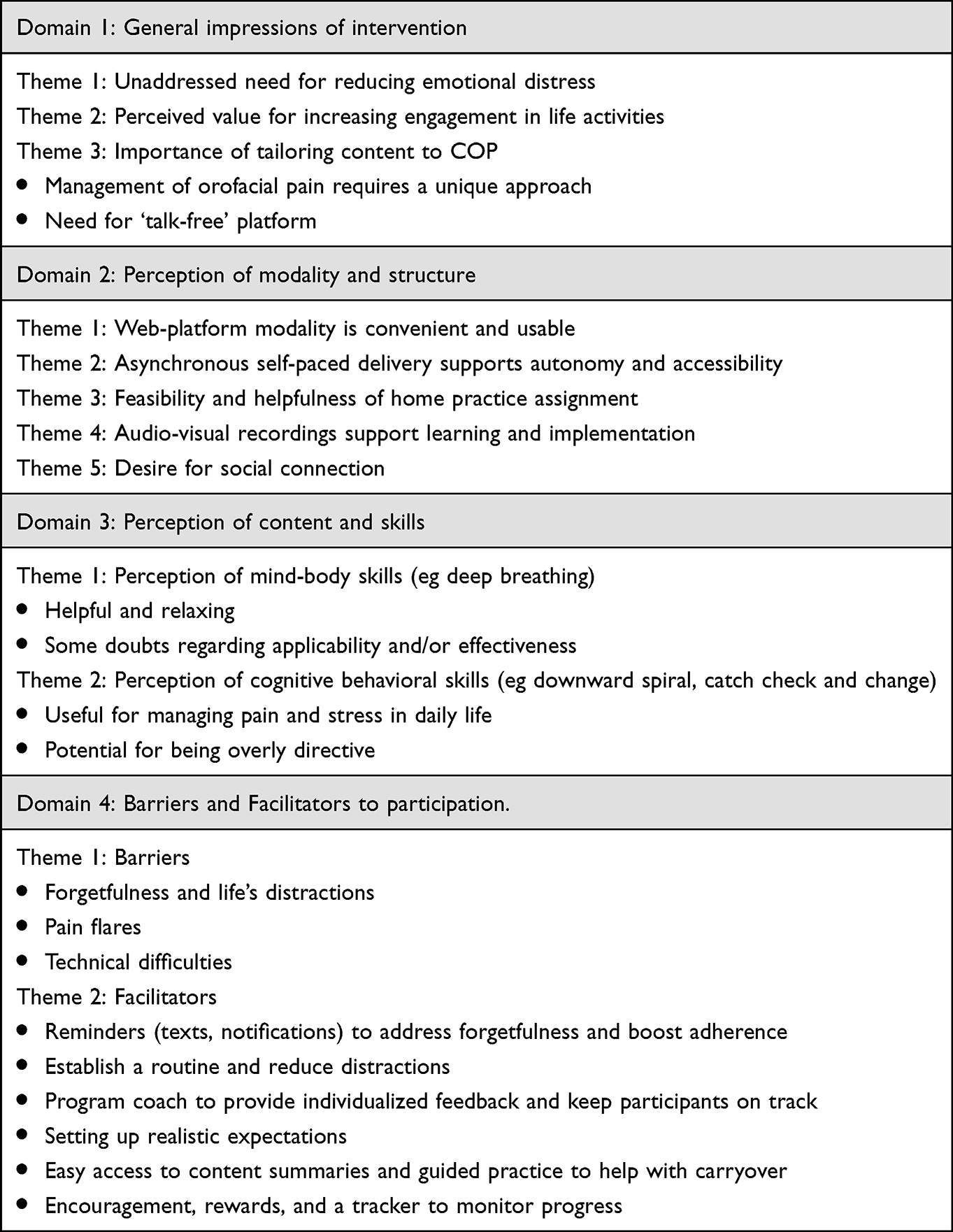 |
Box 1 Domains, themes, and subthemes |
Domain 1: General Impressions of the Intervention
Theme 1: Unaddressed Need for Reducing Emotional Distress
Participants expressed a need for professional intervention to address the “emotional fallout that comes with facial pain,” and emphasized the paucity of effective mental health treatment and education about COP and emotional distress. One participant shared “very few [providers] understand the science underlying chronic pain … Even when they’re kind of more up on it, they don’t necessarily handle it well”. Another participant described “how little information was provided to me about my mental health during all of this. So, I see [this intervention] as a really great opportunity”.
Theme 2: Perceived Value for Increasing Engagement in Life Activities
Participants endorsed that participating in this mind-body intervention could help increase participation in life activities that are important to them. Participants described how understanding the connection between mental health and COP would “save [them from] a lot of avoiding things I want to do in fear of making pain worse” and “be more active and happier with my life”.
Theme 3: Importance of Tailoring Content to COP
Participants emphasized the importance of tailoring the intervention content for the specific needs of people with COP. Findings included two subthemes.
First, participants indicated that management of orofacial pain requires a unique approach because “orofacial pain is a different ball of wax from other types of pain”. One participant indicated the intervention “would need to be pretty specific and specialized in order for me to be interested in it”. Another participant explained, “It was much easier for me to compartmentalize pain in an extremity than it is to compartmentalize pain that is right here [points to face/head] where I live. This is me. This, this is me. This is — it’s much harder”.
Second, participants expressed a need for “talk -free” platform. One participant appreciated that in this intervention, “you don’t need to talk through it like being in therapy. You’re talking, you know, more than anything else, which can create additional pain for us”. Another participant expressed, “I’m very excited about it. I think it’s great. And it’s something where you’re not going to have to talk if you’re having a lot of facial pain, you don’t have to smile, you don’t have to do any of that”.
Domain 2: Perception of Modality and Structure
Theme 1: Web-Platform Modality is Convenient and Usable
Participants reported confidence with using a web-based platform and expressed “I probably wouldn’t have too much trouble picking up and using something like that basically self-guided”. They appreciated the convenience of a web-platform, particularly given their unpredictable pain status, stating, “If you’re having a bad day, you can lay in bed and do it”. Participants perceived that the intervention would be usable and fit well into their life. One participant described “let’s say you’re sitting in the restroom and you’re like, doom scrolling. But then if there is this app which I can use, then maybe it’ll be the perfect thing”.
Theme 2: Asynchronous Self-Paced Delivery Supports Autonomy and Accessibility
Participants appreciated the ability to self-pace, both to promote autonomy and to support use during pain flares. One indicated that “being able to go at your own pace is a good advantage. I just like having the control of going through things myself. There are some things I may want to gloss over quicker, some things I may want to look at in more detail”. Participants described the importance of being able to access the intervention during pain flares. One expressed the benefit of “doing it…when you’re in pain or when you’re in less pain. The idea is you acquire the skills so that when the pain comes, you can use them. But you’ll be able to get to it anytime”.
Theme 3: Feasibility and Helpfulness of Home Practice Assignment
Participants endorsed the feasibility and benefit of home practice assignments. They indicated they could “definitely carve out 10 minutes” to practice. One participant noted that practicing the techniques would help with carryover and independence, stating, “How would you know if you would feel better if you haven’t actually tried to do the exercises that they recommend? So, I think that’s completely fair”.
Theme 4: Audio-Visual Recordings Support Learning and Implementation During Pain Flares
Participants overall had a positive perception of the audio-visual recordings and felt that the guided exercises were helpful, particularly to use during a pain flare. One participant described, “When I’m having an episode, I get very tense and upset and worked up, and I cannot relax. I need somebody to talk me through it”.
Theme 5: Desire for Social Connection
Participants expressed a desire for social connection within the intervention, both with a provider and with other individuals with COP. One expressed concern that “it can be a little dehumanizing to do things one-on-one with a computer where you’ve got little to no interaction with the provider”. Participants also expressed a desire to share the experience with others with COP. One noted the invention is “a module without people that are connected to each other …— and I don’t know if you have the means — to add a personal connection to it”.
Domain 3: Perception of Content and Skills
Theme 1: Perception of Mind-Body Skills
We probed for participants’ perceptions of the mind-body skills, such as deep breathing, which participants practiced through a sample of an instructional video. We identified two subthemes.
First, largely participants’ impressions of the skill were positive. They indicated that the deep breathing was helpful and relaxing and appreciated the guided instructions. One participant noted, “I can just relax my body and let somebody else tell me when to breathe”. On the other hand, a minority of participants expressed doubts regarding the applicability and/or effectiveness of the technique. Still, these participants tended to endorse that the skills might work for others. One stated, “We’re all different … if the breathing works for you, then do the breathing. If it doesn’t, skip that part and go on to the next”.
Theme 2: Perception of Cognitive Behavioral Skills
We asked participants about their perceptions of the cognitive behavioral skills, such as the “downward spiral”, which conveys how COP interacts with negative thoughts, emotions, and actions, and “catch check and change negative thoughts,” which teaches cognitive reframing. Results yielded two subthemes.
Participants found the skills useful for managing pain and stress in daily life. One participant described how the skill “actually gives you something to do… each time you’re in pain”. Another expressed, “It’s just, like, great advice. This advice is applicable in any difficulty in your life…I actually use these in real life”. Conversely, one participant suggested the skill could be overly directive, stating, “it just felt very directive, felt very dealing with conscious thought, and there’s a lot of unconscious thought that leads us and … it was one of those things that’s like’Nahh, not for me’”.
Domain 4: Barriers and Facilitators to Participation
Theme 1: Barriers
We asked participants what might prevent them from completing or benefiting from the intervention, and they expressed three perceived barriers. First, they identified forgetfulness and distractions as a barrier. Second, they indicated that pain flares could get in the way of completing sessions. Finally, they stated, “If there were a lot of like technical difficulties, that [would] make me not want to continue”.
Theme 2: Facilitators
When asked what would help them adhere to and benefit from the intervention, participants identified six potential facilitators: First, they stated that reminders (eg, texts, push notifications) could address forgetfulness and boost adherence. Second, they suggested that establishing a routine and reducing distractions would help them complete the intervention. Third, they expressed a desire for a program coach to provide individualized feedback and keep participants on track. Fourth, they emphasized the value of setting up realistic expectations, knowing the commitments, and adjusting mindset around outcomes. One participant shared, “There’s no magic pill, there’s no magic website or anything that’s going to go - blink, it’s done. It’s gone, you know”. Fifth, they described that easy access to content summaries and guided practice would help with carryover. Finally, sixth, they suggested encouragement, rewards, and a tracker to monitor progress. Participants suggested graphs, progress logs, and pop-ups with encouragement. One stated, “I think just a quick pop-up to reaffirm ‘thanks for doing it’, is going to make me more likely to want to keep doing it”.
Discussion
People with COP experience substantial pain interference and emotional distress, yet psychosocial treatments for this population are limited. We developed a novel web-based, “talk-free” mind-body intervention to meet the unique needs of people with COP. Through these focus groups with people with COP we gained insights into their perceptions of the intervention, its structure, content, skills, and barriers and facilitators for engagement to guide development and refinement.
Generally, participants were enthusiastic about the program, recognizing its potential to meet a critical unaddressed need for managing the psychosocial contributors to COP, consistent with other work highlighting the shortcomings of standard biomedical care for COP.44 Participants confirmed that an intervention that helped them see the connection between thoughts, emotions, and pain would help boost their activity participation, echoing the pattern of confrontation and recovery described in the fear avoidance model19 and in prior research pointing to the connection between mental health and pain for people with COP.45 Participants emphasized the uniqueness of their experience and its separation from other forms of chronic pain, including the need for a “talk-free” intervention. This emphasizes the need for a tailored approach, explicitly addressing orofacial pain and reflecting their unique experiences and challenges, which will remain a key focus throughout the development of Face-Forward-Web.
Regarding modality and structure, participants perceived that the web-based asynchronous modality as ideal, given their desire to access it at their own time including during unpredictable and sometimes debilitating pain flares.21 Concurrently, they expressed a desire for social connection and human interaction, aligning with previous studies with people with chronic conditions including COP.46,47 This highlights the need to balance factors increasing intervention accessibility and scalability (eg, self-placed, talk-free intervention that is available 24/7) with a desire for an intervention that has more human and supportive features. In an effort to optimize this balance, Face-Forward-Web includes audio-visual recording of a dedicated human therapist and used a conversational and personal tone throughout. We also included vignette examples of people with COP, painting a picture with relatable characters. Finally, we offer support from a human staff member as needed for questions, information, and/or technical support.
Regarding perception of intervention content, participants expressed largely positive views of the mind-body skills and the cognitive behavioral skills. They found the deep breathing exercise to be helpful and relaxing, and the skill to “catch, check and change negative thoughts” to be applicable in real life. The perception of skills was not unanimously positive, however, and participants expressed a desire to “pick and choose” techniques and concepts that resonated with them to further personalize and tailor their experience. To help accommodate these preferences, Face-Forward-Web includes diverse skills and encourages participants to choose what and when to practice in accordance with their changing needs and circumstances. Additionally, we include an acknowledgment that some practices might feel more personally useful than others and encouraged participants to give each element and skill a chance. Participants also have the freedom to choose their preferred skills to practice between sessions.
Participants discussed several barriers to participation. The most notable barrier was pain flares, reiterating the importance of providing people with COP with simple and practical tools, opportunities to practice, and easy-to-access therapeutic resources to utilize during episodes of severe pain. Though participants expressed overall confidence regarding their ability to use a web-platform-based intervention, they indicated that potential technical difficulties could hinder their participation. In an effort to minimize such difficulty, we designed Face-Forward-Web with simplicity and ease of navigation in mind. We include an orientation session to familiarize participants with the platform’s structure and enable them to ask questions and troubleshoot challenges. Finally, Face-Forward-Web offers technical support from a live staff member as needed. Aligned with human-centered design principles, we also added a “beta testing” phase prior to testing the feasibility of Face-Forward-Web. The Beta testing phase will include a subset of participants who will complete the intervention with a study staff observing to identify and solve any technical or design-related user challenges that may arise.
Participants identified several facilitators for participation, which may be helpful to consider when treating people with COP. Notably, they emphasized the importance of setting realistic expectations, acknowledging the challenges in living with and treating COP,10,21,44 and recognizing that while symptoms can improve, they may not resolve fully. They indicated that structure and routine would facilitate their participation, rewards and incentives would boost adherence and a sense of accomplishment, and easy access to summaries of key information would help accessibility during pain flares. In response, we are developing an interactive calendar that visually renders each user’s progress and remaining participation commitment. We designed progress trackers and added “pain management practice badges” that are awarded for consistent home practice of skills and instill a sense of progress and achievement. We also included session summaries and bookmarks to enable easy access to important content and skills.
Limitations of this study should be considered. First, participants’ diagnoses were self-reported. However, most participants were recruited via referrals from COP medical providers and advocacy groups, instilling reasonable confidence regarding participants’ experience of COP. Second, our analytic approach utilized RDA, which may not be as thorough as full thematic analysis. However, RDA is established, evidence-based, and provides the critical advantage of supporting timely intervention adaptation. Finally, the sample was predominantly white and female. Future research should elicit perceptions from diverse samples.
Conclusion
This study provides insights that can inform scalable, accessible psychosocial and mind-body interventions suitable for the unique needs of people with COP. Findings give voice to the needs and perceptions of people with COP, guiding the development of tailored, patient-informed treatment approaches such as Face-Forward-Web. Results give us specific changes. Future research should include beta testing and feasibility studies to refine and test the intervention.
Acknowledgments
Ana-Maria Vranceanu and Jonathan Greenberg shared senior authorship for this study. We would like to thank the Facial Pain Association for their contribution to data collection in this study.
Funding
This study was funded by the National Institute of Dental and Craniofacial Research (NIDCR) (grant 1R21DE033502-01A1) and awarded to JG and AMV and K23AT01065301A1 to JG.
Disclosure
SH is employed by Mass General Physician Organization/ Mass General Institute of Health Professions; reports consulting fees from Franchise Medicine. SH is also an unpaid volunteer at Health Tech Without Borders and Conductscience.org. The authors report no other conflicts of interest in this work.
References
1. Horst OV, Cunha-Cruz J, Zhou L, Manning W, Mancl L, DeRouen TA. Prevalence of pain in the orofacial regions in patients visiting general dentists in the Northwest Practice-based REsearch Collaborative in Evidence-based DENTistry research network. J Am Dent Assoc. 2015;146(10):721–728.e3. doi:10.1016/j.adaj.2015.04.001
2. Macfarlane TV, Blinkhorn AS, Davies RM, Kincey J, Worthington HV. Oro-facial pain in the community: prevalence and associated impact. Oral Epidemiol. 2002;30(1):52–10. doi:10.1034/j.1600-0528.2002.300108.x
3. Zieliński G, Pająk-Zielińska B, Ginszt M. A Meta-Analysis of the Global Prevalence of Temporomandibular Disorders. J Clin Med. 2024;13(5):1365. doi:10.3390/jcm13051365
4. Durham J, Breckons M, Vale L, Shen J. DEEP Study: modeling Outcomes and Costs of Persistent Orofacial Pain. JDR Clin Transl Res. 2023;8(1):16–26. doi:10.1177/23800844211063870
5. National Institute of Dental and Craniofacial Research. Facial Pain. 2018. Available from: https://www.nidcr.nih.gov/research/data-statistics/facial-pain.
6. Schmidt JE, Hawkins JM. Orofacial Pain. In: Handbook of Psychosocial Interventions for Chronic Pain.
7. Rollman GB, Gillespie JM. The role of psychosocial factors in temporomandibular disorders. Curr Rev Pain. 2000;4(1):71–81. doi:10.1007/s11916-000-0012-8
8. Crandall JA. An Introduction to Orofacial Pain. Orofac Pain. 2018;62(4):511–523. doi:10.1016/j.cden.2018.05.001
9. Durham J, Raphael KG, Benoliel R, Ceusters W, Michelotti A, Ohrbach R. Perspectives on next steps in classification of oro-facial pain – part 2: role of psychosocial factors. J Oral Rehabil. 2015;42(12):942–955. doi:10.1111/joor.12329
10. Wolf E, Petersson K, Birgerstam P, Maria N. Nonspecific Chronic Orofacial Pain: studying Patient Experiences and Perspectives with a Qualitative Approach. J Oral Facial Pain Headache. 2008;22(4):349–358. doi:10.11607/jofph.22.4.09
11. Gustin SM, Wilcox SL, Peck CC, Murray GM, Henderson LA. Similarity of suffering: equivalence of psychological and psychosocial factors in neuropathic and non-neuropathic orofacial pain patients. PAIN. 2011;152(4):825–832. doi:10.1016/j.pain.2010.12.033
12. Peters S, Goldthorpe J, McElroy C, et al. Managing chronic orofacial pain: a qualitative study of patients’, doctors’, and dentists’ experiences. Br J Health Psychol. 2015;20(4):777–791. doi:10.1111/bjhp.12141
13. Fishbein NS, Bakhshaie J, Greenberg J. Suicidal Ideation and Self-Injury in Trigeminal Neuralgia. J Pain Res. 2025;18:2003–2010. doi:10.2147/JPR.S493649
14. Davis CE, Stockstill JW, Stanley WD, Wu Q. Pain-related worry in patients with chronic orofacial pain. J Am Dent Assoc 1939. 2014;145(7):722–730. doi:10.14219/jada.2014.37
15. Turner JA, Brister H, Huggins K, Mancl L, Aaron LA, Truelove EL. Catastrophizing is associated with clinical examination findings, activity interference, and health care use among patients with temporomandibular disorders. J Orofac Pain. 2005;19(4):291–300.
16. Jang HH, Kim ME, Kim HK. Pain Catastrophizing Mediates the Effects of Psychological Distress on Pain Interference in Patients with Orofacial Pain: a Cross-Sectional Study. J Oral Facial Pain Headache. 2018;32(4):409–417. doi:10.11607/ofph.2067
17. P Svensson, A Michelotti, R Benolie, et al. International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia. 2020;40(2):129–221. doi:10.1177/0333102419893823
18. Woda A, Tubert-Jeannin S, Bouhassira D, et al. Towards a new taxonomy of idiopathic orofacial pain. PAIN. 2005;116(3):396–406. doi:10.1016/j.pain.2005.05.009
19. Crombez G, Eccleston C, Van Damme S, Vlaeyen JWS, Karoly P. Fear-avoidance model of chronic pain: the next generation. Clin J Pain. 2012;28(6):475–483. doi:10.1097/AJP.0b013e3182385392
20. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
21. Lovette B, Bannon S, Spyropoulos D, Vranceanu AM, Greenberg J. “I Still Suffer Every Second of Every Day”: a Qualitative Analysis of the Challenges of Living with Chronic Orofacial Pain. J Pain Res. 2022;15:2139–2148. doi:10.2147/JPR.S372469
22. Aggarwal VR, Tickle M, Javidi H, Peters S. Reviewing the evidence: can cognitive behavioral therapy improve outcomes for patients with chronic orofacial pain? J Orofac Pain. 2010;24(2):163–171.
23. Bergdahl J, Anneroth G, Perris H. Cognitive therapy in the treatment of patients with resistant burning mouth syndrome: a controlled study. J Oral Pathol Med. 1995;24(5):213–215. doi:10.1111/j.1600-0714.1995.tb01169.x
24. Noma N, Watanabe Y, Shimada A, et al. Effects of cognitive behavioral therapy on orofacial pain conditions. J Oral Sci. 2020;63(1):4–7. doi:10.2334/josnusd.20-0437
25. Litt MD, Shafer DM, Kreutzer DL. Brief cognitive-behavioral treatment for TMD pain: long-term outcomes and moderators of treatment. Pain. 2010;151(1):110–116. doi:10.1016/j.pain.2010.06.030
26. Wang J, Jian F, Chen J, et al. Cognitive behavioral therapy for orthodontic pain control: a randomized trial. J Dent Res. 2012;91(6):580–585. doi:10.1177/0022034512444446
27. Tan G, Glaros A, Sherman R, Wong C. Integrative Approaches to Orofacial Pain: role of Biofeedback and Hypnosis. In: Orofacial Disorders: Current Therapies in Orofacial Pain and Oral Medicine; 2017:317–324. doi:10.1007/978-3-319-51508-3_27
28. Bae Y, Park Y. The Effect of Relaxation Exercises for the Masticator Muscles on Temporomandibular Joint Dysfunction (TMD). J Phys Ther Sci. 2013;25(5):583–586. doi:10.1589/jpts.25.583
29. Carlson CR, Bertrand PM, Ehrlich AD, Maxwell AW, Burton RG. Physical self-regulation training for the management of temporomandibular disorders. J Orofac Pain. 2001;15(1):47–55.
30. Wang D, Cao X, Huang X. Equity of Accessibility to Health Care Services and Identification of Underserved Areas. Chin Geogr Sci. 2021;31(1):167–180. doi:10.1007/s11769-021-1181-0
31. Schatman ME. The Role of the Health Insurance Industry in Perpetuating Suboptimal Pain Management. Pain Med. 2011;12(3):415–426. doi:10.1111/j.1526-4637.2011.01061.x
32. Wahl OF. Mental Health Consumers’ Experience of Stigma. Schizophr Bull. 1999;25(3):467–478. doi:10.1093/oxfordjournals.schbul.a033394
33. Dear BF, Gandy M, Karin E, et al. The Pain Course: a randomised controlled trial examining an internet-delivered pain management program when provided with different levels of clinician support. PAIN. 2015;156(10):1920–1935. doi:10.1097/j.pain.0000000000000251
34. Onken LS, Carroll KM, Shoham V, Cuthbert BN, Riddle M. Reenvisioning clinical science: unifying the discipline to improve the public health. Clin Psychol Sci. 2014;2(1):22–34. doi:10.1177/2167702613497932
35. Melchior M, Mazzetto M, Magri L. Relation of painful TMD with the speech function: what are the possible characteristics of mandibular movements and the main symptoms reported? CoDAS. 2019;31:1. doi:10.1590/2317-1782/20182018161
36. Garrett J. The Elements of User Experience: User-Centered Design for the Web and Beyond. 2010.
37. Walden A, Garvin L, Smerek M, Johnson C. User-centered design principles in the development of clinical research tools. Clin Trials. 2020;17(6):174077452094631. doi:10.1177/1740774520946314
38. Dopp A, Parisi K, Munson S, Lyon A. Aligning implementation and user-centered design strategies to enhance the impact of health services: results from a concept mapping study. Implement Sci Commun. 2020;1:1. doi:10.1186/s43058-020-00020-w
39. Lovette BC, Bakhshaie J, Kulich R, et al. Development of a Novel Web-Based Intervention Targeting Pain-Related Outcomes in Individuals With Chronic Orofacial Pain: protocol for a Mixed Methods Study. JMIR Res Protoc. 2025;14(1):e71839. doi:10.2196/71839
40. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. PAIN. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
41. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
42. Vindrola-Padros C, Johnson GA. Rapid Techniques in Qualitative Research: a Critical Review of the Literature. Qual Health Res. 2020;30(10):1596–1604. doi:10.1177/1049732320921835
43. Schexnayder J, Perry KR, Sheahan K, et al. Team-Based Qualitative Rapid Analysis: approach and Considerations for Conducting Developmental Formative Evaluation for Intervention Design. Qual Health Res. 2023;33(8–9):778–789. doi:10.1177/10497323231167348
44. Grunberg VA, Reichman M, Lovette BC, Vranceanu AM, Greenberg J. “No One Truly Understands What We Go through and How to Treat It”: lived Experiences with Medical Providers among Patients with Orofacial Pain. Int J Environ Res Public Health. 2022;19(16):10396. doi:10.3390/ijerph191610396
45. LaRowe LR, Bakhshaie J, Vranceanu AM, Greenberg J. Anxiety, pain catastrophizing, and pain outcomes among older adults with chronic orofacial pain. J Behav Med. 2024;47(3):537–543. doi:10.1007/s10865-024-00473-7
46. Pester BD, Tankha H, Caño A, et al. Facing Pain Together: a Randomized Controlled Trial of the Effects of Facebook Support Groups on Adults With Chronic Pain. J Pain. 2022;23(12):2121–2134. doi:10.1016/j.jpain.2022.07.013
47. Thompson DM, Booth L, Moore D, Mathers J. Peer support for people with chronic conditions: a systematic review of reviews. BMC Health Serv Res. 2022;22(1):427. doi:10.1186/s12913-022-07816-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.