Back to Journals » Journal of Pain Research » Volume 19
Predisposing Factors for Chronic Post-Surgical Pain After Thoracic Surgery: A Scoping Review with Quantitative Synthesis
Authors Bonilla Sierra P, Celi MA ![]() , Suárez Burneo C
, Suárez Burneo C ![]()
Received 31 July 2025
Accepted for publication 10 December 2025
Published 8 January 2026 Volume 2026:19 557361
DOI https://doi.org/10.2147/JPR.S557361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Patricia Bonilla Sierra, Manuel Antonio Celi, Carolina Suárez Burneo
Department of Health Sciences, Universidad Técnica Particular de Loja (UTPL), Loja, Ecuador
Correspondence: Carolina Suárez Burneo, Email [email protected]
Background: Chronic post-surgical pain (CPSP) is a frequent complication after thoracic and cardiothoracic surgery; however, reported risk factors remain heterogeneous and inconsistent.
Objective: To map and synthesize the factors associated with CPSP after thoracic and cardiac surgery and to determine the strength of evidence supporting each predictor category.
Methods: An exploratory review was conducted following PRISMA-ScR guidelines. Searches were performed in PubMed, Scopus, and Web of Science, identifying 20 eligible studies. A complementary qualitative synthesis was undertaken: statistically significant p-values (p < 0.05) were extracted, and predictors were categorized by evidence strength (strong, moderate, limited/inconsistent).
Results: Severe acute postoperative pain during the first postoperative days emerged as the strongest and most reproducible predictor of CPSP across designs and populations. Psychological distress, particularly anxiety, depression, and catastrophizing, also showed strong and consistent associations. Moderate evidence supported the influence of young age, female sex, low BMI, and pre-existing chronic pain. Surgical determinants such as operative duration, minimally invasive approaches, tissue trauma, and postoperative complications showed variable associations, as did anesthetic factors, especially high intraoperative remifentanil doses. Evidence for single-dose S-ketamine and regional blocks was limited or inconsistent. Preliminary findings related to inflammatory cytokines, microRNA phenotypes, and geriatric prediction models suggest additional biological contributors but remain exploratory.
Conclusion: CPSP after thoracic and cardiothoracic surgery results from interacting nociceptive, psychological, procedural, and biological factors. Although heterogeneity across studies requires cautious interpretation, this synthesis highlights early postoperative pain control and psychological vulnerability screening as priority strategies in perioperative care, and underscores the need for standardized, prospective, biomarker-informed research.
Keywords: chronic post-surgical pain, thoracic surgery, predisposing factors
Introduction
Long-term pain following thoracic surgery presents a significant clinical challenge, affecting more than 50% of patients and posing concerns for both individuals and healthcare providers. Thoracic surgeries encompass a diverse range of procedures, from lung resections to corrections of thoracic wall deformities, with the potential for patients to develop acute and chronic pain that significantly impacts their quality of life and recovery process.1
According to the International Association for the Study of Pain (IASP), chronic post-surgical pain (CPSP) is defined as pain that develops after a surgical procedure, persists for at least three months, cannot be explained by other causes such as infection or disease recurrence, and results in significant functional or psychological impact.2 Within this classification, the IASP specifically recognizes chronic post-thoracotomy pain syndrome as a distinct condition characterized by persistent pain in the thoracic or chest wall region following thoracic surgery. This review adopts these definitions as the conceptual framework for identifying and interpreting CPSP-related predictors in thoracic and cardiothoracic procedures.
The incidence of thoracic surgeries has been steadily rising due to factors such as population aging, the increasing prevalence of respiratory and cardiovascular diseases, and advancements in surgical techniques. Recent epidemiological data reveals a global increase in the incidence of thoracic surgeries, with procedures like lobectomy, pneumonectomy, and thoracoscopic surgeries becoming more commonplace. For example, in the United States alone, it is estimated that over 530,000 thoracic surgeries are performed annually.1 This trend is expected to continue with the aging population and the rising burden of thoracic diseases.3
However, this surge in surgical interventions also underscores the critical need for effective postoperative pain management to minimize patient suffering and facilitate optimal recovery.4 Inadequate pain control not only affects patient comfort but can also lead to complications such as respiratory compromise, delayed mobilization, prolonged hospital stays, and the development of chronic pain syndromes.5
Despite advances in thoracic surgery and perioperative management, a significant gap remains in understanding why some patients develop CPSP after thoracotomy. Available evidence shows that CPSP is a complex and multidimensional phenomenon involving interacting biological, emotional, and social factors, consistent with the biopsychosocial model described by Giusti et al.6 Similarly, recent reviews highlight that the transition from acute to chronic pain depends on a dynamic interaction between intense nociception, psychological vulnerability, and procedural characteristics.7 However, these authors agree that the evidence remains fragmented, particularly in thoracic surgery, where an integrative framework that systematically synthesizes these different domains is lacking. This review seeks to help close this gap through a broad and structured synthesis of the factors associated with CPSP in thoracic and cardiac surgery.
Therefore, a synthesis that systematically incorporates these determinants is needed to clarify how these domains combine to influence CPSP risk after thoracotomy. In this context, we formulated the following research question: Which factors have been associated with chronic post-surgical pain (CPSP) after thoracic and cardiac surgery, and what level of evidence supports each category of predictors? Accordingly, the objective of this scoping review was to map and synthesize the factors associated with CPSP after thoracic and cardiac surgery and to determine the strength of evidence for each predictor category. Addressing this question requires a methodological approach capable of encompassing the wide variability in procedures, CPSP definitions, factor domains, and study designs found in the current literature. For this reason, we chose to conduct a scoping review, as the evidence on CPSP after thoracic surgery is extensive yet highly heterogeneous, limiting the feasibility of a traditional quantitative synthesis and constraining direct comparability across studies.8
Materials and Methods
This review aimed to map and synthesize the factors associated with CPSP after thoracic and cardiac surgery and to determine the strength of evidence for each predictor category. The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR), ensuring a transparent and structured mapping of the existing evidence.9 A comprehensive secondary search was conducted across the PubMed, Scopus, and Web of Science databases.
The research question guiding this review was: Which factors have been associated with chronic postsurgical pain (CPSP) after thoracic and cardiac surgery, and what level of evidence supports each category of predictors?
Given the exploratory nature of the topic and the expected heterogeneity among studies in design, population, surgical and anesthetic techniques, and pain-assessment methods, a scoping-review design was selected as the most appropriate methodological approach. According to the Joanna Briggs Institute and PRISMA-ScR guidance, scoping reviews are particularly suitable for mapping broad and variable bodies of literature, identifying knowledge gaps, and organizing diverse factors when a meta-analysis is neither feasible nor appropriate.9,10 This design allowed us to comprehensively chart, categorize, and interpret the breadth of available evidence without restricting inclusion to methodologically homogeneous studies.
The search strategy used MeSH and DeCS terms: “thoracic surgery”, “postoperative”, “pain”, “chronic pain”, and “risk factors” (Table 1). Peer-reviewed, open-access, full-text articles published between 2019 and 2025, in English or Spanish, were included if they aligned with the study question and examined chronic postsurgical pain in adult or pediatric patients who had undergone thoracic or cardiothoracic surgery. These parameters were selected to ensure contemporaneity of evidence and methodological rigor; however, restricting the search to two languages may represent a limitation. Eligible study designs included prospective and retrospective observational studies, randomized controlled trials, secondary analyses of clinical trials, cross-sectional studies, systematic reviews, and analytical models, reflecting the exploratory nature of a scoping review and its goal of mapping a broad and heterogeneous evidence base.
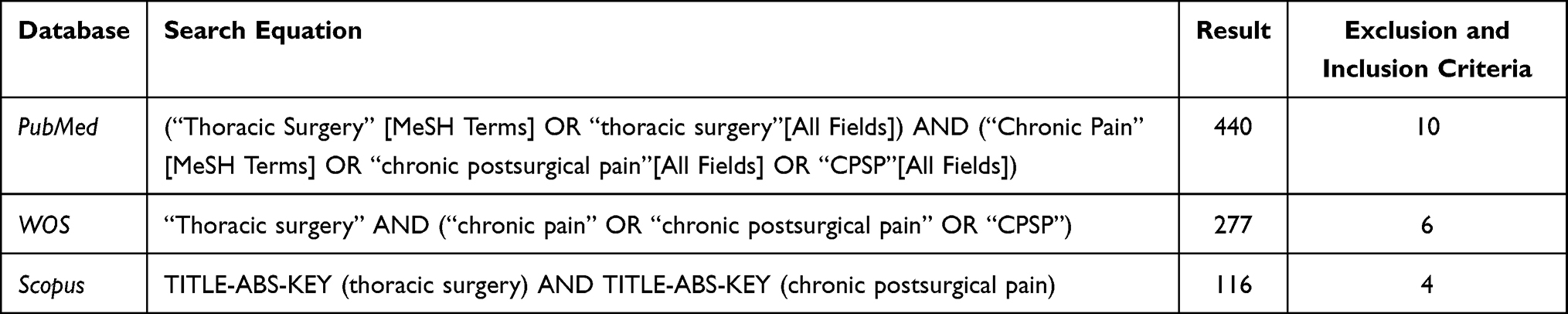 |
Table 1 Search Strategies |
Studies were excluded if they were opinion papers, editorials, letters to the editor, biographies, conference proceedings, non–peer-reviewed publications, or if they did not align with the study objectives (Figure 1), to ensure methodological rigor and consistency with PRISMA-ScR recommendations. The last search was performed in June 2025.
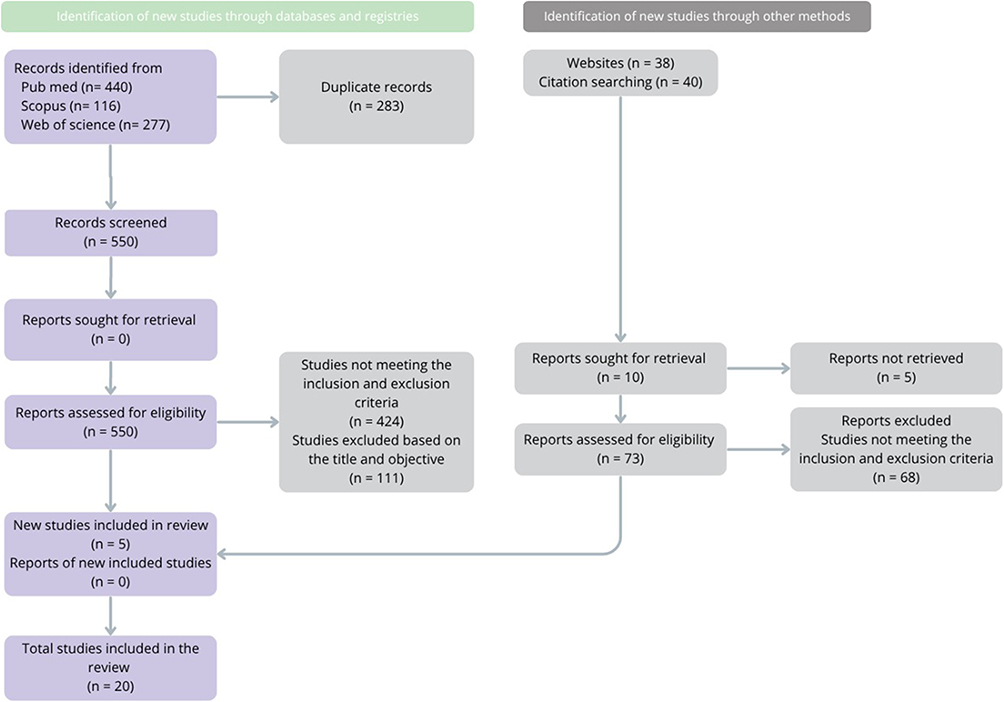 |
Figure 1 Diagram of extraction of selected articles. |
Two authors (Authors 2 and 3) independently conducted the search, removed duplicates, and screened titles and abstracts. Full-text selection and data extraction were also performed independently, with discrepancies resolved by a third author (Author 1). Extracted data included authorship, year, study design, country, sample size, interventions, and main findings. Zotero was used to identify duplicates, and Mendeley was employed for reference management.
Consistent with JBI guidance, this study employed a descriptive analytical approach appropriate for a scoping review, whose purpose is to map and organize the available evidence rather than to statistically aggregate results.10 Accordingly, no meta-analysis was planned or conducted, as this technique is not compatible with the objectives or methodological foundations of a scoping review. To enhance the clinical utility of the findings, we incorporated a complementary simple quantitative synthesis, extracting and comparing the p-values (p < 0.05) reported in the included studies to identify which factors have been associated with chronic postsurgical pain (CPSP) after thoracic and cardiac surgery, and what level of evidence supports each category of predictors. To ensure clarity and facilitate interpretation, the results were first organized according to the strength of statistical evidence (high, moderate, or limited/inconsistent). Within each evidence tier, findings were further grouped thematically into demographic, psychological, surgical, anesthetic, postoperative pain, and immunological–genetic domains. This two-level structure allows for a clearer synthesis: the hierarchy reflects the robustness of the associations, while the thematic grouping highlights the multidimensional mechanisms underpinning CPSP. This structured descriptive approach, fully aligned with recommended practices for scoping reviews, allowed us to highlight patterns of consistency across the literature while preserving the exploratory and non-aggregative nature of this review.
Results
A total of 833 records were identified across databases. After removing 283 duplicates, 535 studies were excluded based on the inclusion and exclusion criteria, title, or objective. Following full-text screening, 45 articles were assessed, and 25 were excluded for not meeting the eligibility criteria. Finally, 20 studies encompassing 7559 patients were included in the scoping review (Figure 1).
Most of the included studies were conducted in Asia—particularly China—followed by Canada, Japan, Italy, the United States, and the United Kingdom, reflecting an uneven global distribution of evidence. This geographic pattern indicates that the current understanding of CPSP after thoracic and cardiac surgery is shaped predominantly by Asian and North American cohorts, with limited representation from other regions. Such imbalance may influence the generalizability of findings, as perioperative practices, analgesic protocols, and patient characteristics vary across healthcare systems. Study designs comprised 7 prospective observational studies, 4 randomized controlled trials, 3 retrospective studies, 2 secondary analyses, and 4 cross-sectional or analytical studies, including mediation analyses and propensity-score models (Table 2).
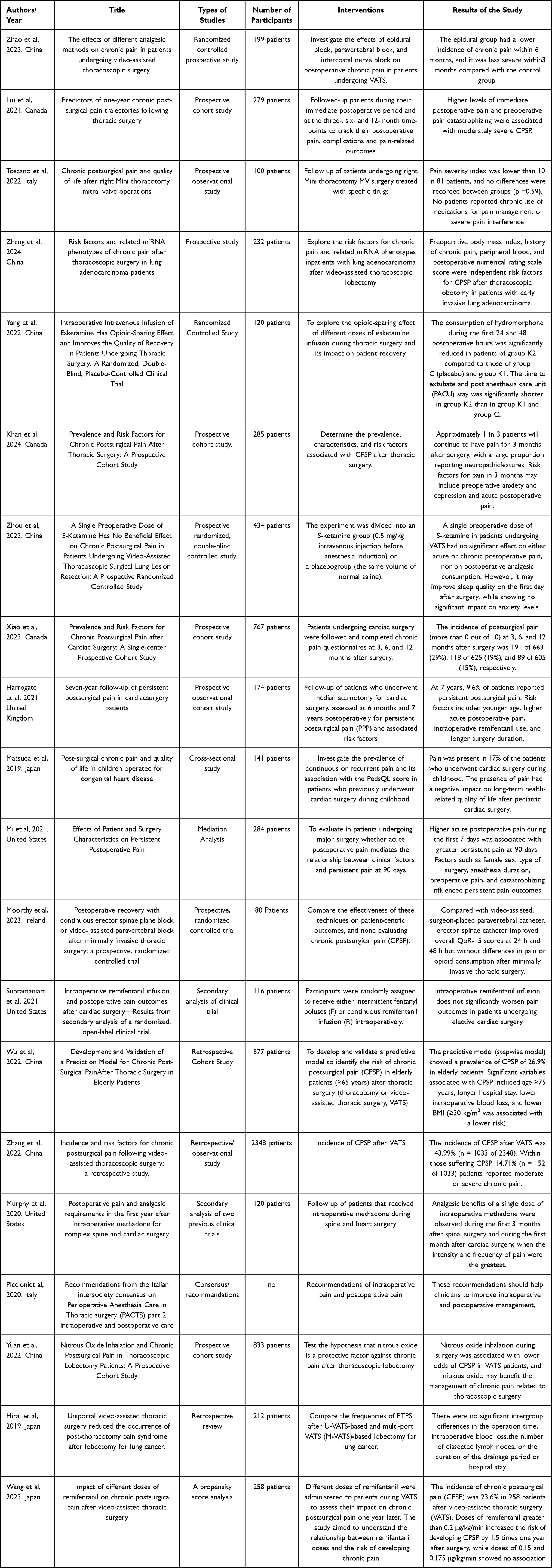 |
Table 2 Articles |
Factors with Strong and Consistent Statistical Associations
Acute Postoperative Pain (Most Consistent Predictor)
Acute postoperative pain emerged as the strongest and most consistently replicated predictor of CPSP across the included studies. High pain scores in the first 24–72 hours after surgery were repeatedly associated with chronic pain development, and all studies reporting this relationship demonstrated statistical significance (p < 0.05). Studies showed that elevated early postoperative pain predicted persistent pain at 3 months,4 while others found that higher acute pain remained a significant predictor even at 7-year follow-up.11 Similarly, Mi et al demonstrated that severe pain during the first postoperative week significantly mediated long-term pain trajectories, reinforcing the temporal link between early nociceptive intensity and chronicity.12 In VATS lobectomy patients, early postoperative NRS scores as independent and statistically significant predictors of CPSP (p < 0.05).13 Across all these studies, the direction and magnitude of effect were consistent, confirming that high acute postoperative pain is the most robust and statistically validated clinical driver of CPSP.
Psychological Distress (Anxiety, Depression, Catastrophizing)
Psychological vulnerability also showed a strong and reproducible statistical association with the development of CPSP. Preoperative anxiety and depression significantly predicted chronic pain at 3 months following thoracotomy,4 while pain catastrophizing demonstrated a consistent statistical relationship (p < 0.05) with moderate to severe pain trajectories up to 12 months.14 Catastrophizing similarly influenced persistent pain at 90 days in a heterogeneous surgical cohort.12 In our comparative statistical synthesis, these psychological factors repeatedly met significance criteria, underscoring psychological distress as a high-impact predictor that materially contributes to the transition from acute to chronic postoperative pain.
Demographic Factors (Younger Age, Female Sex, History of Chronic Pain)
Demographic characteristics demonstrated moderate-to-strong statistical consistency as predictors of CPSP. Younger age was significantly associated with persistent pain at both intermediate and long-term follow-up—up to 7 years after cardiac surgery,11 while female sex consistently correlated with greater pain persistence at 90 days.12 A preoperative history of chronic pain independently predicted CPSP after VATS lobectomy,13 reaching strong statistical significance (p < 0.05) in our synthesis. Taken together, these demographic variables reflect reproducible patient-level vulnerabilities that increase susceptibility to chronic pain.
Surgical Factors (Procedural Invasiveness and Perioperative Complications)
Surgical characteristics also contributed significantly to CPSP risk, with several factors demonstrating replicated statistical associations across studies. Increased operative duration and remifentanil exposure during cardiac surgery were associated with persistent pain at long-term follow-up.11 In thoracoscopic lobectomy cohorts, perioperative blood loss and postoperative wound infection emerged as independent predictors of CPSP,1,15 with p < 0.05 in both cases. Large retrospective data further confirmed the substantial incidence of CPSP after VATS, supporting the role of surgical trauma and postoperative complications as significant contributors to chronic pain development.1
Anesthetic and Analgesic Predictors (Opioid Exposure Patterns)
Anesthetic management, particularly intraoperative opioid administration, showed statistically significant associations with long-term pain risk. High-dose intraoperative remifentanil (>0.2 μg/kg/min) increased the likelihood of CPSP one year after VATS by approximately 1.5-fold,16 a finding consistent with evidence from cardiac cohorts demonstrating higher persistent pain with greater remifentanil exposure.11 These associations reached significance (p < 0.05) in our statistical synthesis, identifying opioid exposure patterns as meaningful modifiable predictors within the anesthetic domain.
Immunological and Genetic Factors (Emerging but Significant Predictors)
Emerging evidence from molecular and immunological studies revealed statistically significant associations between biological markers and CPSP. In VATS lobectomy patients with early invasive lung adenocarcinoma, peripheral blood markers and specific miRNA phenotypes were independently associated with chronic pain development,13 with significant p-values (p < 0.05) supporting their predictive value. Although these findings remain preliminary, they highlight potential biological pathways, particularly related to inflammation and gene regulation, that may influence susceptibility to chronic pain.
Factors with Moderate Evidence (Statistically Significant in Single Studies, Without Replication Yet)
Protective or Neutral Effects of Specific Analgesic Techniques
Several analgesic techniques demonstrated statistically significant effects in individual studies, suggesting potential, but not yet replicated influence on chronic postoperative pain. Epidural analgesia significantly reduced the incidence and severity of chronic pain up to 6 months after VATS (p < 0.05).17 Nitrous oxide inhalation during thoracoscopic lobectomy also showed a statistically significant protective effect, with lower odds of CPSP in VATS patients (p < 0.05).18 In contrast, while esketamine infusion reduced postoperative opioid consumption (p < 0.05),19 neither a single preoperative dose of S-ketamine nor erector spinae–guided blocks demonstrated significant long-term effects on CPSP (p > 0.05).20,21 These findings highlight analgesic strategies that may influence chronic pain risk but require further replication before being considered robust predictors.
Procedural Approach and Minimally Invasive Techniques
Procedure type showed variable associations with chronic pain. Uniportal versus multi-port VATS demonstrated a statistically significant difference in CPSP rates (p < 0.05),22 and patients undergoing right minithoracotomy without using a rib retractor had a lower incidence of CPSP 9).23 Nonetheless, other authors found no statistic difference on the incidence of CPSP during U-VATS and M-VATS,22 nor among other minimally invasive other surgical approaches.1
Predictive Models in Older Adults
A prediction model developed in elderly patients after thoracotomy or VATS identified several statistically significant predictors of CPSP: age ≥75 years, longer hospitalization, lower intraoperative blood loss, and BMI <30 kg/m2 (all p < 0.05).15 Although statistically robust within the cohort, these findings have not been replicated in other populations, placing them within the category of emerging but still moderate-level evidence.
Weak or Inconsistent Evidence
Methadone and Opioid-Based Analgesic Strategies
The long-term impact of intraoperative methadone on CPSP remains inconsistent. While early postoperative analgesic benefits were observed in spine and cardiac surgery patients,3 these improvements did not translate into reduced chronic pain at later timepoints. Similarly, secondary analysis comparing remifentanil versus fentanyl showed no significant differences in persistent pain outcomes.24 Overall, opioid-based intraoperative strategies demonstrated weak and non-replicated associations with CPSP prevention.
Regional Analgesia Techniques
Evidence regarding regional analgesia and chronic pain is inconsistent. Continuous erector spinae plane block improved early recovery metrics after minimally invasive thoracic surgery but did not reduce CPSP rates.21 Paravertebral approaches showed no significant long-term advantages when compared with surgeon-placed catheters. Collectively, regional blocks demonstrated limited evidence for influencing chronic pain trajectories.
Pediatric Populations
Studies in pediatric surgical cohorts produced inconclusive evidence regarding CPSP predictors. Although continuous or recurrent pain was present in 17% of children following cardiac surgery and was associated with lower health-related quality of life,25 no consistent demographic, surgical, or analgesic predictors were identified across studies. Thus, evidence in pediatric populations remains limited and insufficient for firm conclusions.
Single-Dose S-Ketamine and Miscellaneous Pharmacologic Interventions
A single preoperative dose of S-ketamine showed no significant effect on acute or chronic postoperative pain after VATS.20 While minor improvements in next-day sleep quality were observed, these findings were not related to CPSP risk reduction. Other isolated pharmacologic interventions also failed to demonstrate consistent long-term benefits, indicating weak evidence for their role in CPSP prevention.
Discussion
Our findings indicate that the transition from acute postoperative pain to CPSP after thoracic surgery follows a predictable pattern repeatedly described in the literature. Consistent with the evidence reported, early postoperative acute pain emerges as the most robust predictor of CPSP.4,12 This is reinforced by other authors who identified immediate postoperative pain as a key determinant of long-term outcomes,26 and similarly reported that early pain intensity distinguishes patients who develop CPSP.27 This convergence across multiple study designs reinforces the importance of intensive pain control during the first postoperative days, establishing acute pain as a highly relevant and modifiable preventive target.
Preoperative pain was a significant predictor for those investigations that took it into account.1,4,12,13,28 Evidence suggests that the descending inhibitory system, a complex nervous network that functions to reduce the perception of pain to some extent, may become less effective in patients who have suffered pain for a long time.29 Therefore, in patients with a history of preoperative pain, this contributes to a greater sensitization of peripheral nociceptors, thereby increasing the risk of developing CPSP.29
Psychological factors, such as anxiety, depression, and negative affect, play a significant role in chronic pain, especially in women.30 Evidence from several studies indicates a direct relationship between symptoms like depression, anxiety and poor sleep quality scores and an elevated risk of chronic post-surgical, and influence in its prevalence.31–34 These findings align with other reviews, where they report a strong influence of preoperative factors, such as psychological, pain related, social/lifestyle, depression, anxiety, and pain catastrophizing.35,36
The relationship between psychological vulnerability and pain persistence aligns closely with findings from various authors, all of whom demonstrate that anxiety, depression, and especially pain catastrophizing significantly increases the likelihood of developing CPSP.12,14,33,37 Fear of pain and early postoperative pain can be identified as independent predictors, reinforcing the interaction between emotional states and nociceptive processing.26,33 Likewise, psychosocial mechanisms highlight how cognitive-emotional patterns, such as maladaptive attention, negative affect, and diminished reward responsiveness—facilitate the transition from acute to chronic pain.29,38 These findings align with observations from other authors who identified moderate–severe acute pain as a key determinant of persistent thoracic pain.27 Together, this body of evidence reinforces the contemporary biopsychosocial model and highlights a clear opportunity to integrate brief perioperative psychological interventions, targeting catastrophizing, enhancing coping strategies, and reducing emotional distress, to mitigate the progression toward CPSP.
Some studies identified age under 65 years as a risk factor for the development of CPSP.1,4,12 It is relevant to point out that pain perception is something purely subjective, and the responses given by patients may vary depending on the pain threshold/tolerance of each individual.39 The positive relationship between young patients and the development of chronic pain can be explained by two hypotheses.1 Younger individuals may be biologically more sensitive to painful stimuli and their nervous system reacts more effectively to these stimuli than an adult would. The other theory states that older adults tend to be reluctant patients who limit their reporting of their symptoms, and pain is one of them.34
Regarding the surgical factors, there were direct associations between blood loss and history of wound infections as risk factors for CPSP.1,15 The reason might be associated with a sensibilization of the central and peripheral nervous system after an infection, causing hyperalgesia, which might contribute to CPSP.40
The degree of tissue trauma, surgical duration, and postoperative complications appear to be more influential than the surgical approach itself. Some articles reported that the surgical approach was not associated with an increased risk of CPSP, finding no significant differences between U-VATS and M-VATS.22 Meanwhile, other studies observed a high CPSP risk even with minimally invasive techniques.1 In contrast, in the case of multiportal video-assisted thoracic surgery, the number of incisions increased the possibilities of intercostal nerve damage, increasing the risk of CPSP.23,41 Evidence suggests that the absence of a rib retractor decreases the risk of damaging the intercostal nerves, thus reducing the risk of CPSP after minithoracotomy procedures.23 These variable data suggests that minimizing effective tissue trauma, rather than merely reducing the number of ports or surgical approach, remains a critical target for future research.
A consistent finding across the literature is the potential harmful effect of high doses of remifentanil.16 However, evidence regarding protective anesthetic interventions remains contradictory. While some authors demonstrated that epidural analgesia reduced CPSP at 6 months,17 other studies demonstrate inconsistent benefits of regional anesthesia or enhanced recovery techniques, matching the variable evidence identified in our review for procedural and anesthetic predictors.21,42 No reduction in chronic pain was observed with advanced regional techniques or with preoperative S-ketamine.20,21 These discrepancies may be explained by variations in dose, timing, and CPSP definitions, underscoring the need for methodological standardization. Furthermore, variables associated with intraoperative anesthesia showed that rescue analgesia and fentanyl carried a higher risk of CPSP.1 In contrast, the use of single dose intraoperative methadone showed grater results at reducing CPSP one month after spine and cardiac surgery.3 Also, the administration of intravenous propofol indicate a lower risk of CPSP.3,42 New studies show that the use of nonsteroidal anti-inflammatory drugs (NSAIDs) during the postsurgical period reduces the incidence of CPSP. This effect is achieved by decreasing opioid consumption and interfering with the underlying pathophysiological mechanisms of CPSP.43 In the context of cardiac surgery, there are some contraindications regarding the use of NSAIDs. They have been associated with a higher risk for thrombotic events, acute kidney failure and bleeding complications.44 Additionally, some studies have reported that combining dexmedetomidine with ropivacaine in epidural blocks may enhance postoperative analgesia by reducing pain and prolonging the duration of its effects.45 Thoracic epidural anesthesia may also help reduce the incidence and severity of chronic postsurgical pain after thoracic and abdominal procedures, especially when used as part of a multimodal analgesia strategy.46 All of these strategies have recently been included under the concept of multimodal analgesia, which combines pharmacological and non-pharmacological approaches, applied individually according to each patient’s needs.47
Also, new research found that higher preoperative levels of IL-8 and increased postoperative levels of IL-6, IL-8, and IL-13 were associated with a lower risk of CPSP, suggesting a potential protective role and their value as prognostic biomarkers. The results suggest that immunomodulatory interventions enhancing IL-6, IL-8, and IL-13 or targeting pro-inflammatory cytokines could offer promising strategies for CPSP prevention.48
In addition, some studies found a genetic contribution to CPSP severity (~35% heritability) and found 77 significant SNPs across 24 loci. Also, the adaptive immune system, especially B cells, has an important role in pain resolution. Animal models confirmed that a higher number of B cells help to prevent prolonged post-surgical pain. These findings suggest B cells as potential targets for CPSP treatment.49
Taken together, the findings of this review are consistent with evidence reported by multiple authors, who repeatedly demonstrate that severe acute postoperative pain is the main driver in the transition to CPSP and remains the most clearly modifiable perioperative factor.1,12,14 Despite this convergence, the literature remains fragmented across surgical approaches, anesthetic techniques, and patient populations, which limits the ability to develop an integrated understanding of CPSP mechanisms and to standardize preventive strategies. Our work addresses this gap by integrating dispersed evidence from heterogeneous studies, into a cross-cutting framework that connects nociceptive mechanisms, psychological determinants, and procedural contributors to pain chronification1,4,12,14 In doing so, it provides the most comprehensive map to date of CPSP predictors in thoracic and cardiac surgery, something that previous literature had not synthesized in a coherent way.
This scoping review also presents several important limitations that must be acknowledged to properly contextualize its findings. First, the methodological heterogeneity across studies, reflected in variable definitions of CPSP, inconsistent follow-up intervals, diverse pain measurement tools, and non-standardized reporting of effect sizes, limits the comparability of results and may have introduced interpretation bias. Second, the reliance on p-values extracted from individual studies, many of which did not report confidence intervals or adjusted analyses, restricts the ability to assess the precision and clinical relevance of the observed associations. Third, although the scoping design is appropriate for mapping broad and emerging fields, it inherently prevents causal inference and does not allow for quantitative synthesis or estimation of pooled effects. Fourth, the predominance of single-center cohorts from high-income countries raises concerns about external validity, particularly in settings with different perioperative protocols, analgesic resources, or population characteristics. Fifth, several studies had moderate to high risk of bias due to small sample sizes, retrospective designs, selective reporting, or substantial loss to follow-up. Finally, despite a comprehensive search strategy, publication bias cannot be excluded, especially regarding negative or null results related to analgesic interventions. Addressing these limitations will require large, multicenter prospective studies with standardized CPSP definitions, harmonized perioperative assessments, and integration of biological, psychological, and procedural predictors within robust analytical frameworks.
The clinical implications of this synthesis are clear: the prevention of CPSP should prioritize early control of acute postoperative pain and the timely identification of psychological vulnerability factors. Consistent with the findings of various authors, anxiety, depression, and pain catastrophizing modulate pain intensity and increase the likelihood of persistence, underscoring the need to incorporate brief psychological interventions into standard perioperative care.4,12,14 Likewise, evidence regarding the detrimental effects of high remifentanil doses, together with the inconsistent results of regional techniques and adjunctive therapies,1,11,16 suggests that prevention does not depend on a single anesthetic strategy but rather on coherent multimodal protocols tailored to individual risk profiles.3,19–21 While the conclusions of this review must be interpreted with caution given its methodological limitations, the synthesis highlights which predictors are consistently supported and which remain controversial, offering a practical, hierarchical framework to guide institutional protocol updates.
Conclusion
This scoping review identifies early acute postoperative pain and psychological vulnerability, particularly anxiety, depression, and catastrophizing as the most consistent and clinically relevant predictors of CPSP after thoracic and cardiac surgery. Moderate evidence also supports the influence of younger age, female sex, prior chronic pain, and high-dose intraoperative remifentanil, whereas minimally invasive approaches, regional techniques, and anesthetic adjuvants show inconsistent or context-dependent effects (Figure 2).
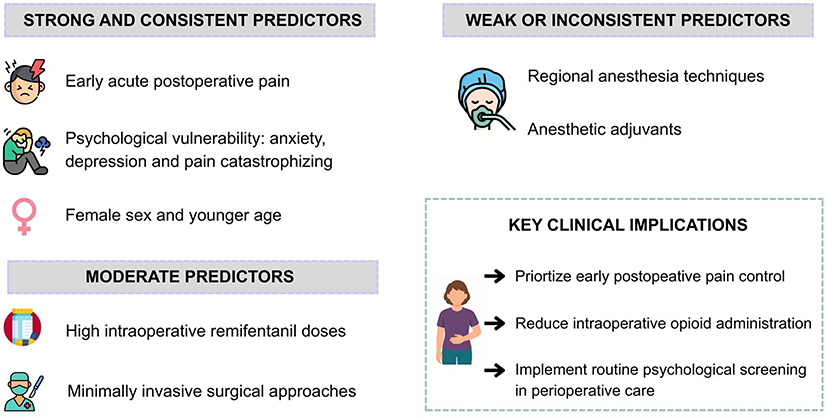 |
Figure 2 Predisposing factors for chronic post-surgical pain after thoracic surgery. |
By mapping these predictors according to the strength of evidence, this review provides a structured and clinically meaningful synthesis that clarifies which factors reliably increased risk and which remain uncertain. These findings emphasize the need to prioritize early postoperative pain control and psychological screening within multimodal perioperative pathways. Future studies should focus on a multimodal assessment of patients to better identify CPSP, as the factors involved extend beyond surgical or analgesic variables and include essential biopsychosocial components. Additionally, research should aim to include larger and more diverse populations, representing multiple socioeconomic backgrounds and ethnic groups.
Acknowledgments
The authors of this manuscript declare that Artificial Intelligence (AI) was used during the writing process solely to improve readability and refine the language. This use was carried out under strict human supervision and control. Following the application of AI technologies, the authors thoroughly reviewed and edited all outputs, taking full responsibility for the accuracy, coherence, and integrity of the content presented in this publication.
Funding
The Universidad Técnica Particular de Loja, Ecuador, funded the open-access publication. This research did not receive a specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Zhang Y, Zhou R, Hou B, et al. Incidence and risk factors for chronic postsurgical pain following video-assisted thoracoscopic surgery: a retrospective study. BMC Surg. 2022;22(1). doi:10.1186/s12893-022-01522-1
2. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–13. doi:10.1097/j.pain.0000000000001384
3. Murphy GS, Avram MJ, Greenberg SB, et al. Postoperative pain and analgesic requirements in the first year after intraoperative methadone for complex spine and cardiac surgery. Anesthesiology. 2020;132(2):330–342. doi:10.1097/ALN.0000000000003025
4. Khan JS, Dana E, Xiao MZX, et al. Prevalence and risk factors for chronic postsurgical pain after thoracic surgery: a prospective cohort study. J Cardiothorac Vasc Anesth. 2024;38(2):490–498. doi:10.1053/j.jvca.2023.09.042
5. Hyland SJ, Brockhaus KK, Vincent WR, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare. 2021;9:333. doi:10.3390/healthcare9030333
6. Giusti EM, Lacerenza M, Manzoni GM, Castelnuovo G. Psychological and psychosocial predictors of chronic postsurgical pain: a systematic review and meta-analysis. Pain. 2021;162(1):10–30. doi:10.1097/j.pain.0000000000001999
7. Rosenberger DC, Pogatzki-Zahn EM. Chronic post-surgical pain – update on incidence, risk factors and preventive treatment options. BJA Educ. 2022;22(5):190–196. doi:10.1016/j.bjae.2021.11.008
8. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. doi:10.1186/s12874-018-0611-x
9. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
10. Pollock D, Peters MDJ, Khalil H, et al. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evid Synth. 2023;21(3):520–532. doi:10.11124/JBIES-22-00123
11. Harrogate SR, Cooper JA, Zawadka M, Anwar S. Seven-year follow-up of persistent postsurgical pain in cardiac surgery patients: a prospective observational study of prevalence and risk factors. Eur J Pain. 2021;25(8):1829–1838. doi:10.1002/ejp.1794
12. Mi X, Zou B, Rashidi P, et al. Effects of patient and surgery characteristics on persistent postoperative pain: a mediation analysis. Clin J Pain. 2021;37(11):803–811. doi:10.1097/AJP.0000000000000979
13. Zhang L, Chen Z, Xu L, Hu H. Risk factors and related miRNA phenotypes of chronic pain after thoracoscopic surgery in lung adenocarcinoma patients. PLoS One. 2024;19(3):e0297742. doi:10.1371/journal.pone.0297742
14. Liu CW, Page MG, Weinrib A, et al. Predictors of one year chronic post-surgical pain trajectories following thoracic surgery. J Anesth. 2021;35(4):505–514. doi:10.1007/s00540-021-02943-7
15. Wu XD, Zeng FF, Yu XX, et al. Development and validation of a prediction model for chronic post-surgical pain after thoracic surgery in elderly patients: a retrospective cohort study. J Pain Res. 2022;15:3079–3091. doi:10.2147/JPR.S368295
16. Wang X, Ida M, Uyama K, Naito Y, Kawaguchi M. Impact of different doses of remifentanil on chronic postsurgical pain after video-Assisted thoracic surgery: a propensity score analysis. Medicine. 2023;102(30):E34442. doi:10.1097/MD.0000000000034442
17. Zhao X, Xiao W, Zhang T, Xi M, Sun X. The effects of different analgesic methods on chronic pain in patients undergoing video-assisted thoracoscopic surgery. Videosurgery Miniinv. 2023;18:157–65 doi:10.5114/wiitm.2022.120572.
18. Yuan Y, Zhang L, Zhang Y, Shen L, Huang Y. Nitrous oxide inhalation and chronic postsurgical pain in thoracoscopic lobectomy patients: a prospective cohort study 2022. doi:10.21203/rs.3.rs-2345093/v1
19. Yuan J, Chen S, Xie Y, et al. Intraoperative intravenous infusion of esmketamine has opioid-sparing effect and improves the quality of recovery in patients undergoing thoracic surgery: a randomized, double-blind, placebo-controlled clinical trial. Pain Physician. 2022 25(9).
20. Zhou R, Zhang Y, Tang S, et al. A single preoperative dose of s-ketamine has no beneficial effect on chronic postsurgical pain in patients undergoing video-assisted thoracoscopic surgical lung lesion resection: a prospective randomized controlled study. J Cardiothorac Vasc Anesth. 2023;37(8):1433–1441. doi:10.1053/j.jvca.2023.02.046
21. Moorthy A, Ní Eochagáin A, Dempsey E, et al. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial. Br J Anaesth. 2023;130(1):e137–e147. doi:10.1016/j.bja.2022.07.051
22. Hirai K, Usuda J. Uniportal video-assisted thoracic surgery reduced the occurrence of post-thoracotomy pain syndrome after lobectomy for lung cancer. J Thorac Dis. 2019;11(9):3896–3902. doi:10.21037/jtd.2019.09.07
23. Toscano A, Barbero C, Capuano P, et al. Chronic postsurgical pain and quality of life after right minithoracotomy mitral valve operations. J Card Surg. 2022;37(6):1585–1590. doi:10.1111/jocs.16400
24. Subramaniam K, Ibarra A, Ruppert K, Mallikarjun K, Orebaugh S. Intraoperative remifentanil infusion and postoperative pain outcomes after cardiac surgery—results from secondary analysis of a randomized, open-label clinical trial. J Cardiothorac Vasc Anesth. 2021;35(2):458–466. doi:10.1053/j.jvca.2020.08.064
25. Matsuda M, Takemura H, Yamashita A, Matsuoka Y, Sawa T, Amaya F. Post-surgical chronic pain and quality of life in children operated for congenital heart disease. Acta Anaesthesiol Scand. 2019;63(6):745–750. doi:10.1111/aas.13346
26. Chen B, Shi, G, Gao, P. Risk factors for chronic postsurgical pain following thoracoscopic surgery for lung cancer. Am J Transl Res. 2024;16(12):7959–7971. doi:10.62347/NHTK3687
27. Rivera-Ramos H, Larrañaga-Altuna L, García-Olivera M, Armengol-Gay M, Soldevilla-García M, Bermejo-Martínez S. Incidence and risk factors of chronic post-thoracic surgery pain: a retrospective study. Rev Esp Anestesiol Reanim. 2025;72(1):101644. doi:10.1016/j.redare.2024.101644
28. Xiao MZX, Khan JS, Dana E, et al. Prevalence and risk factors for chronic postsurgical pain after cardiac surgery: a single-center prospective cohort study. Anesthesiology. 2023;139(3):309–320. doi:10.1097/ALN.0000000000004621
29. Batoz H, Semjen F, Bordes-Demolis M, Bnard A, Nouette-Gaulain K. Chronic postsurgical pain in children: prevalence and risk factors. A prospective observational study. Br J Anaesth. 2016;117(4):489–496. doi:10.1093/bja/aew260
30. Franqueiro AR, Wilson JM, He J, et al. Prospective study of preoperative negative affect and postoperative pain in patients undergoing thoracic surgery: the moderating role of sex. J Clin Med. 2024;13(19):5722. doi:10.3390/jcm13195722
31. Lim J, Chen D, McNicol E, et al. Risk factors for persistent pain after breast and thoracic surgeries: a systematic literature review and meta-analysis. Pain Lippincott Williams Wilkins. 2022;163(1):3–20. doi:10.1097/j.pain.0000000000002301
32. Ghadimi, D, Looha, M, Akbari, M et al Predictors of postoperative pain six months after breast surgery. Sci Rep. 2023;13(1). doi:10.1038/s41598-023-35426-8
33. Chen D, Yang H, Yang L, et al. Preoperative psychological symptoms and chronic postsurgical pain: analysis of the prospective China surgery and anaesthesia cohort study. Br J Anaesth. 2024;132(2):359–371. doi:10.1016/j.bja.2023.10.015
34. Aternali A, Slepian PM, Clarke H, et al. Presurgical distress about bodily sensations predicts chronic postsurgical pain intensity and disability 6 months after cardiothoracic surgery. Pain. 2022;163(1):159–169. doi:10.1097/j.pain.0000000000002325
35. Sydora BC, Whelan LJ, Abelseth B, et al. Identification of presurgical risk factors for the development of chronic postsurgical pain in adults: a comprehensive umbrella review. J Pain Res Dove Medical Press Ltd. 2024;17:2511–2530. doi:10.2147/JPR.S466731
36. Jin D, Zhang Y, Zheng H, et al. The epidemiology of chronic postsurgical pain after video-assisted thoracic surgery (VATS-CPSP) in China: a multicentre prospective study. J Thorac Dis. 2025;17(5):2802–2812. doi:10.21037/jtd-2024-2220
37. Li R, Rogers AH, Sujan AC, et al. Psychosocial mechanisms underlying the transition from acute to chronic postsurgical pain in youth following spinal fusion: a 6-month longitudinal study. Pain. 2025;166(10):e447–e459. doi:10.1097/j.pain.0000000000003631
38. Williams G, Howard RF, Liossi C. Persistent postsurgical pain in children and young people: prediction, prevention, and management. Pain Rep. 2017;2(5). doi:10.1097/PR9.0000000000000616
39. Gitkind AI, Olson TR, Downie SA. Vertebral artery anatomical variations as they relate to cervical transforaminal epidural steroid injections. Pain Med. 2014;15(7):1109–1114. doi:10.1111/pme.12266
40. Cazzaniga S, Real G, Finazzi S, Lorini LF, Forget P, Bugada D. How to modulate peripheral and central nervous system to treat acute postoperative pain and prevent pain persistence. Curr Neuropharmacol. 2023;22(1):23–37. doi:10.2174/1570159x21666230810103508
41. Wang X, Wang Y, Cao M, et al. Perioperative comparison of uniportal versus multiportal video-assisted thoracoscopic surgery for complex segmentectomy of the lower lung lobe. BMC Surg. 2025;25(1). doi:10.1186/s12893-025-02944-3
42. Piccioni F, Droghetti A, Bertani A, et al. Recommendations from the Italian intersociety consensus on perioperative anesthesa care in thoracic surgery (PACTS) part 2: intraoperative and postoperative care. Perioperative Med. 2020;9(1):31. doi:10.1186/s13741-020-00159-z
43. Parisien M, Lima LV, Dagostino C, et al. Acute inflammatory response via neutrophil activation protects against the development of chronic pain. Sci Transl Med. 2022;14(644). doi:10.1126/scitranslmed.abj9954
44. Huette P, Moussa M, Diouf M, et al. Effect of non-steroidal anti-inflammatory drugs on the management of postoperative pain after cardiac surgery: a multicenter, randomized, controlled, double-blind trial (KETOPAIN Study). Trials. 2024;25(1). doi:10.1186/s13063-024-08326-z
45. Tang R, Lu WS, Zhong HL, Wu F, Liu YQ. Comparison of different adjuvant analgesia for paravertebral block in video-assisted thoracoscopic surgery: a double-blind randomized controlled trial. PLoS One. 2025;20(5 May). doi:10.1371/journal.pone.0322589
46. Pöpping DM, Gogarten W. Epidural anesthesia in thoracic and abdominal surgery: current perspectives and practical implications. Anaesthesiologie. 2025;74(7):411–420. doi:10.1007/s00101-025-01528-3
47. Hwang W. Multimodal analgesia strategies for optimized pain management in thoracic surgery. J Korean Med Associ. 2025;68(1):16–23. doi:10.5124/jkma.2025.68.1.29
48. Chidambaran V, Duan Q, Pilipenko V, et al. The role of cytokines in acute and chronic postsurgical pain after major musculoskeletal surgeries in a quaternary pediatric center. Brain Behav Immun. 2024;122:596–603. doi:10.1016/j.bbi.2024.08.056
49. Parisien M, van Reij RRI, Khoury S, et al. Genome-wide association studies with experimental validation identify a protective role for B lymphocytes against chronic post-surgical pain. Br J Anaesth. 2024;133(2):360–370. doi:10.1016/j.bja.2024.04.053
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Prediction Model for Chronic Post-Surgical Pain After Thoracic Surgery in Elderly Patients: A Retrospective Cohort Study
Wu XD, Zeng FF, Yu XX, Yang PP, Wu JP, Xv P, Wang HT, Pei YM
Journal of Pain Research 2022, 15:3079-3091
Published Date: 29 September 2022