Back to Journals » Patient Preference and Adherence » Volume 16
Predictors of Vaccine Acceptance, Confidence, and Hesitancy in General, and COVID-19 Vaccination Refusal in the Province of Quebec, Canada
Authors Nizigiyimana A, Acharya D, Morillon GF ![]() , Poder TG
, Poder TG ![]()
Received 2 June 2022
Accepted for publication 5 August 2022
Published 18 August 2022 Volume 2022:16 Pages 2181—2202
DOI https://doi.org/10.2147/PPA.S376103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Alexis Nizigiyimana,1– 3,* Dilaram Acharya,1,4,* Gabin F Morillon,5,6 Thomas G Poder1,3,6
1Department of Management, Evaluation and Health Policy, School of Public Health, Université de Montréal, Montréal, QC, Canada; 2Centre de recherche en santé publique, Montréal, QC, Canada; 3Centre de Recherche de l’Institut Universitaire en Santé Mentale de Montréal, CIUSSS de l’Est-de-l’île-de-Montréal, Montréal, QC, Canada; 4Medical Affairs and Innovation, Héma-Québec, Montréal, QC, Canada; 5Faculté d’économie, Université de Montpellier, Montpellier, France; 6Centre interuniversitaire de recherche en analyse des organisations, Montréal, QC, Canada
*These authors contributed equally to this work
Correspondence: Thomas G Poder, Department of management, evaluation and health policy, School of Public Health, Université de Montréal, Montréal, QC, Canada, Email [email protected]
Introduction: A surge of COVID-19 variants is a major concern, and literatures that support developing an optimum level of herd immunity are meaningful. This study aimed to examine the factors associated with vaccine acceptance, confidence, and hesitancy in general, and COVID-19 vaccination refusal in the general population of Quebec, Canada.
Methods: A web-based cross-sectional survey was conducted in October and November 2020 among French-speaking participants above 18 years of age employing quota sampling technique. The questionnaire included socio-demographic and attitudinal variables towards vaccination. Logistic regression analyses were conducted to examine the association between independent and outcome variables.
Results: Of total 1599 participants, 88.9%, 87.5%, 78.5%, and 18.2%, respectively, indicated vaccine acceptance, high level of vaccine confidence, low level of vaccine hesitancy, and COVID-19 vaccination refusals. Participants having higher education, income, and fear of COVID-19 (FCV-19S) were more likely to get vaccinated, while smokers were less likely to get vaccinated. Similarly, age groups (40– 59, and ≥ 60 years), higher education, income, permanent resident in Canada, country of parents from Canada, ever faced acute disease in the family, higher sense of coherence, and FCV-19S scores were predictors of high levels of vaccine confidence. Higher education, income, sense of coherence and FCV-19S scores, and higher health-related quality of life (CORE-6D) produced lower levels of vaccine hesitancy. Conversely, those acting as caretaker, other essential worker, smoker, and those with financial losses were more likely to have higher vaccine hesitancy. Additionally, ≥ 60 years of age, higher education and income, country of parents from Canada, higher scores of willingness to take risk and FCV-19S were less likely to have high level of COVID-19 vaccination refusal.
Conclusion: Over three quarters of the participants indicated positive attitudes toward vaccination. Some socio-demographic and health-related quality of life factors were associated with the outcome variables, and these should be sought while designing interventions to improve COVID-19 vaccination rates.
Keywords: COVID-19, behaviour, health determinants, infectious diseases, public health, vaccination
Introduction
As of April 14, 2022, around 500 million confirmed cases including over 6 million deaths from COVID-19 have been reported worldwide, while Canada has registered 35 million confirmed cases including over38000deaths from COVID-19.1 In response to this major public health crisis, countries around the world have stepped up to manufacturing vaccines to reduce the morbidity and mortality related to COVID-19. Globally, around 65% of the global population, including 86.9% of Canadians have received at least one vaccine dose, while 59% of global population, including 82.2% of Canadians are fully vaccinated.2 A vaccine is seen as an effective choice to stop the pandemic, with more than one hundred COVID-19 vaccines in clinical development worldwide, including eight that have now been approved for human testing through clinical trials.3 For instance, since the onset of the delta variant, the United States’ Centers for Disease Control reported that unvaccinated people face 11 times more risk of death from delta variant than vaccinated people based on surveillance data.4 Although immunisation has historically successfully reduced the global burden of illness and death, public confidence in vaccines can be affected by various concerns. As such, vaccine hesitancy can lead to delays and refusals, and sometimes contribute to disease outbreaks.5 The approval of the various COVID-19 vaccines sent waves of excitement and relief across the world. However, some people remain hesitant about receiving a vaccine for COVID-19.6,7 Emerging international evidence on COVID-19 vaccine hesitancy suggests that there is a range of reasons for this reluctance, including doubts about the safety and efficacy of the vaccine, political or pharmaceutical mistrust, belief in natural immunity, and the belief that the virus is mild or not life-threatening.8,9 Vaccine confidence is an increasingly important global public health issue, with a decrease in confidence leading to well-documented cases of disease outbreaks, setbacks to global polio eradication as well as other immunization goals, and contentious political debates in high- and low-income countries alike.10,11 Amidst the sudden outbreak of COVID-19 variants which include delta, and omicron variants, a study from New Zealand estimated the threshold of herd immunity to stand at 97% of the population who need to be vaccinated to stop the spread of these new variants.12
As of April 14, 2022, the province of Quebec reported 90.2%, 83.01%, and 50.80% of people who, respectively, received their first, second, and third doses of COVID-19 vaccine.13 This underscores the need to identify the factors which would enable Quebec to increase the vaccine uptake to reach the recommended rate allowing herd immunity. To the best of our knowledge, there is a lack of recent data on the state of vaccine acceptance, confidence, and hesitancy during the pandemics in the province of Quebec. This information and its key drivers are prerequisites to understand the current vaccination situation and facilitate vaccination in a more efficient way. As such, it has the potential to provide evidence on vaccination strategies and to sustain vaccination coverage to an optimum level. Thus, our study aimed to examine the factors associated with vaccine acceptance, confidence, and hesitancy in general, and COVID-19 vaccination refusal in the general population of Quebec, Canada. Our findings would help to develop targeted behavior change strategies, communication interventions, and policy implications to increase the vaccine uptake in Quebec and beyond.
Methods
Study Design, Population, and Sampling
A web-based survey was conducted in Quebec, Canada, in October and November 2020 within French-speaking participants using quota sampling techniques according to age, gender and education. Of the total 3615 randomly contacted, 1980 accepted to participate and 1599 completed our survey, giving rise to a response rate of 44.23%. The survey company Dynata Inc. was involved in the recruitment of participants through their dynamic online platform (ie, members are invited to connect on the platform where various surveys are presented to them in an order based on an algorithm using their demographics, preferences, topics of previous surveys completed, etc.). To reach a statistical power of 95% with a first-species risk of 3% (ie, rejecting the null hypothesis when it is true) and a relevant population of 6.5 million, a minimum of 1067 individuals was needed.
Definition of Variables
The questionnaire included socio-demographic data such as gender, age, education level, household income, attitude towards vaccination including perception, confidence about vaccines, experience with the COVID-19, Fear-of-COVID19 Scale (FCV-19S), Sense of Coherence (SOC-3), and Health-Related Quality of Life (HRQoL) questionnaires. The survey also included a series of hypothetical scenarios describing vaccination strategies and asking people if they would accept to be vaccinated in such a scenario. In each scenario, two hypothetical vaccination strategies and an opt-out (ie, no vaccine program) were proposed. The main outcome variables we used in this study were as follows: vaccine acceptance, confidence, and hesitancy in general in a pandemic context, and refusal of COVID-19 vaccination (ie, corresponding to the hypothetical scenarios). We tested different ways to construct these four variables, using various modalities.
Regarding vaccine acceptance, we asked participants whether they generally accept most/all or some or whether they generally refuse most/all vaccines. Further, these three categories were dichotomized into two as follows: I refuse most or all of the vaccines, and I accept some, most or all of the vaccines. Concerning confidence about vaccine, we asked participants to respond to four questions, where each respondent was asked to choose yes or no, to the three following questions: “Do you consider vaccination to be important for the health of the population? Do you trust Quebec health institutions to recommend an effective and safe vaccine? Do you trust your doctor to recommend a safe and effective vaccine?”. For the fourth question, it was the same as for vaccine acceptance: “About vaccination, which one of the following situations corresponds to you?”. Responses to these four questions were summed, giving a score on a scale from 0 to 5, which were categorized as follows: 0–1 = low confidence, 2–3 = medium confidence, 4–5 = high confidence. Later, these scores were binarized into two groups: 0–2 = low confidence, 3–5 = high confidence. As for vaccine hesitancy, participants responded to eight questions which were summed to give a scale ranging from 0 to 32. Each respondent was asked to rate – on a five-point Likert scale: strongly agree, somewhat agree, do not know, somewhat disagree, strongly disagree – the extent to which they agreed with eight statements pertaining to vaccination: “I feel sufficiently informed about vaccination”, “I feel that there are risks for my health if my vaccination is delayed”, “I have already hesitated to be vaccinated”, “I consider that we receive too many vaccines”, “Overall, I am fearful of vaccines”, “I consider that vaccines are effective in preventing disease”, “I believe that vaccines may weaken my immune system”, “Overall, people around me are in favour of vaccination”. We then grouped hesitancy score into three categories (0–10 = low hesitancy, 11–21 = medium hesitancy, and 22–32 = high hesitancy). Further, these three categories were merged into dichotomous groups (0–16 = low hesitancy and 17–32 = high hesitancy). For COVID-19 vaccine refusal, participants were required to respond to twelve hypothetical scenarios as indicated earlier. A refusal to participate in the vaccination program was coded as 1, yielding a scale ranging from 0 to 12, allowing to create five groups (0 refusal = pro-vaccine, 1–6 = 50% of time or less chose no vaccine, 7–12 = more than 50% of time chose no vaccine, 0–11 = chose at least one time the vaccine program, 12 = anti-vaccine (100% of time chose no vaccine)). These categories were then dichotomized as follows: 0–6 = pro-vaccine, 7–12 = anti-vaccine. It is noteworthy to highlight here that we have tested two ways to construct these outcome variables using two modalities as described above (ie, binary or not). The binary outcome variables were created for the appropriate statistical analytical purposes as the proportion of participants in some category was very small. However, we reported each fragmented category and scores and additional statistical analyses in this regard as Supplementary Materials (Tables S1–S6).
HRQoL was assessed by three questionnaires: Short-form 6-Dimension version 2 (SF-6Dv2), EuroQoL 5-Dimension 5-Level (EQ-5D-5L), and Clinical Outcomes in Routine Evaluation 6-Dimension (CORE-6D). All were designed for calculating Quality-Adjusted Life-Years (QALYs), with a score of 1 for full health and 0 for death. SF-6Dv2 was derived from SF-36v2 and assesses HRQoL on 6 dimensions: Physical Functioning (PF), Role Functioning (RF), Social Functioning (SF), Pain (PA), Mental Health (MH), and Vitality (VT); with 5–6 response levels.14 The EQ-5D-5L consists of 5 dimensions: Mobility (MO), Self-Care (SC), Usual Activities (UA), Pain/Discomfort (PD), and Anxiety/Depression (AD).15 A unique health state can be described using a 5-digit vector formed according to the responses to the 5 questions. The CORE-6D is a HRQoL questionnaire dedicated to mental health which consists of 6 items, each with 5 levels of response (ranging from not at all to most or all the time), tapping 2 conceptual domains: 5 emotional items, and a physical symptom item.16 We assessed the fear of COVID-19 using the French-Canadian version of the FCV-19S, where participants responded to seven questions by choosing “strongly disagree”, “disagree”, “neutral”, “agree”, and “strongly agree”.17 The SOC-3 Score is based on 3 questions and was grouped into 0–4 and 5–6, as recommended.18 The other independent variables were socio-demographic variables such as age, gender, education, income, occupation, residential and financial status (ie, loss as a result of COVID-19 situation), willingness to take risk, and other personal attributes.
Statistical Analysis
Data was collected in Excel and imported into Statistical Package for the Social Sciences version 27 (SPSS). Descriptive statistics were performed to summarize the frequencies and percentages for categorical variables, while mean and standard deviation (SD) for continuous variables. We tested different statistical models. The univariate analysis was conducted employing either non-parametric (Fisher’s exact test, chi-square) and parametric test (one-way analysis of variance) depending on the types of variables. The multivariable logistic regression analysis was followed to assess the independent associations between independent variables and outcomes of interest. We entered all variables with p ≤ 0.20 in univariate analyses into an initial multivariable model with backward selection. The adjusted odds ratio (AOR) with their 95% confidence intervals (95% CI) was reported, along with a p-value of less than 0.05, which was considered statistically significant. We tested different statistical models, and the additional statistical analyses have been provided in Supplementary Materials (Tables S1-S6). Based on a reviewer comment, considering the number of participant indicating a gender of intersex (n = 1), the statistical analysis recorded this participant as a female (ie, biological attribute).
Ethical Considerations
The procedure and all the questionnaires used in this survey were fully compliant with the indications of the Declaration of Helsinki. Participants’ consents, privacy, anonymity and confidentiality were fully maintained throughout the study and beyond. Informed consent was obtained from the study participants prior to the study commencement. The ethical approval was obtained from the ethics committee of the CIUSSS de l’Est de l’île de Montréal, Montreal, QC, Canada.
Results
Participants’ Characteristics
Results on outcome variables were presented as binary variables (Table 1). Of the 1599 participants, most reported that they generally accept some, most or all recommended vaccines (88.9%), had high level of vaccine confidence (87.5%), low level of vaccine hesitancy (78.5%), and few indicated COVID-19 vaccination refusal (18.2%).
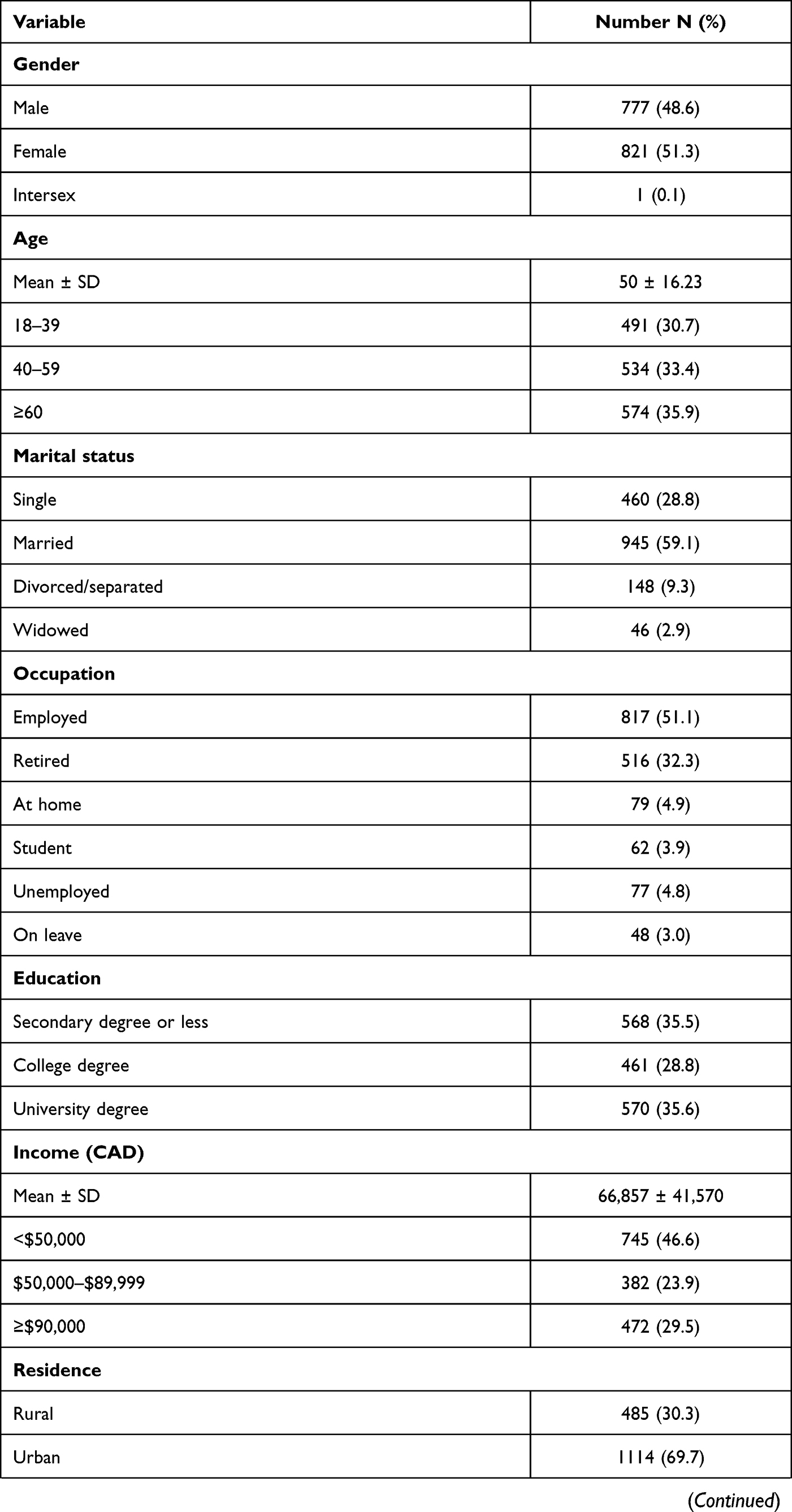 | 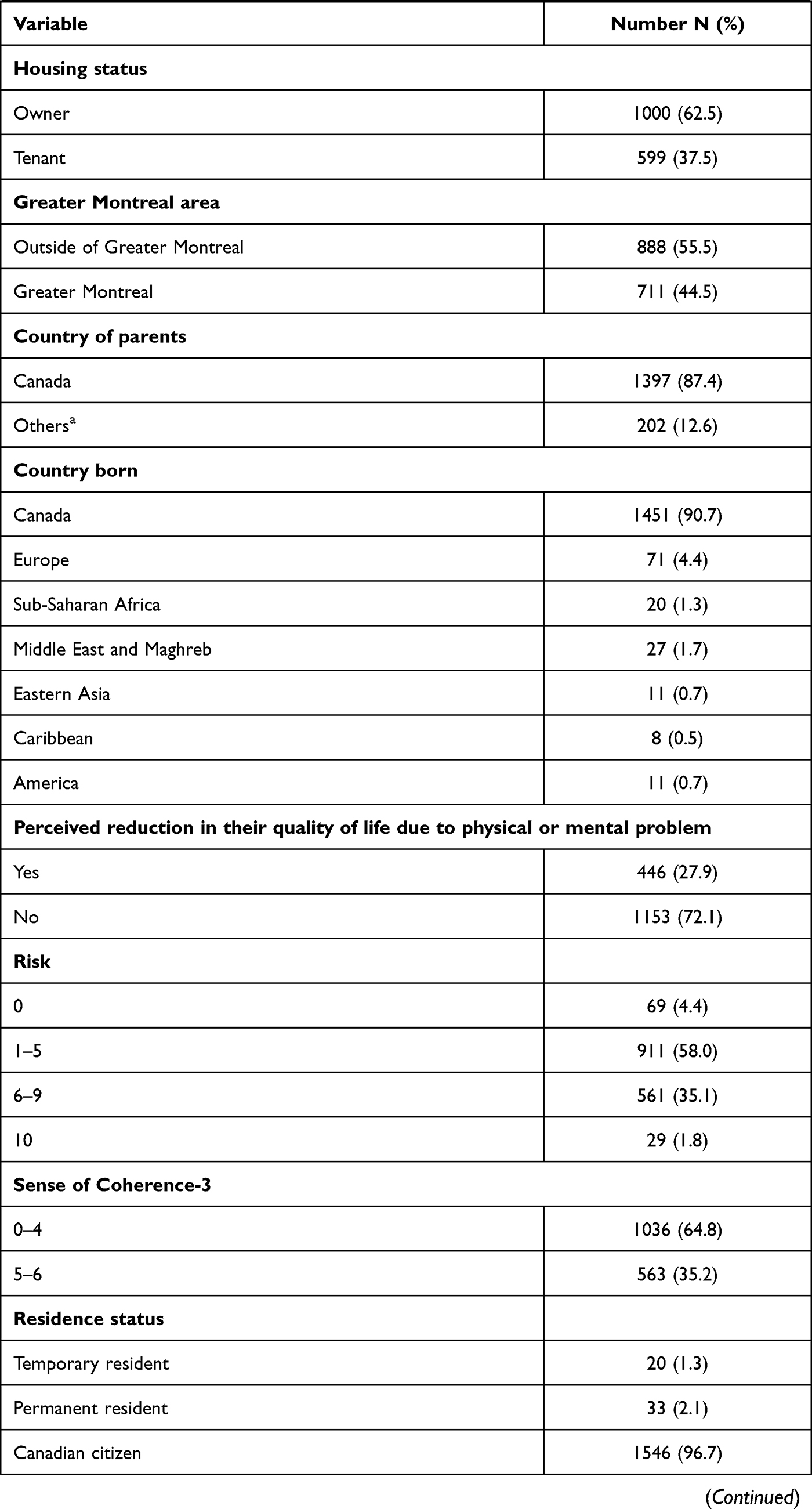 | 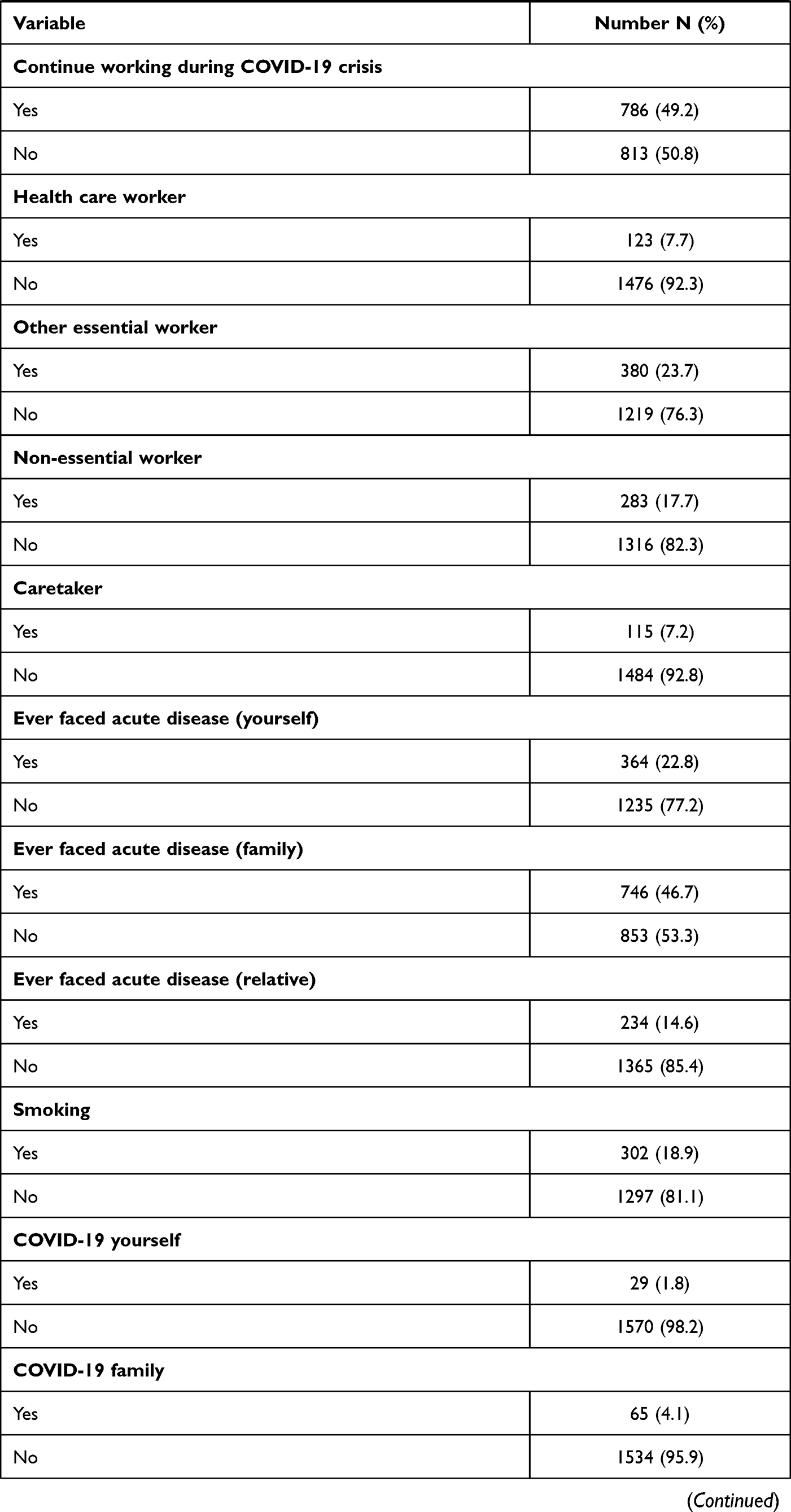 | 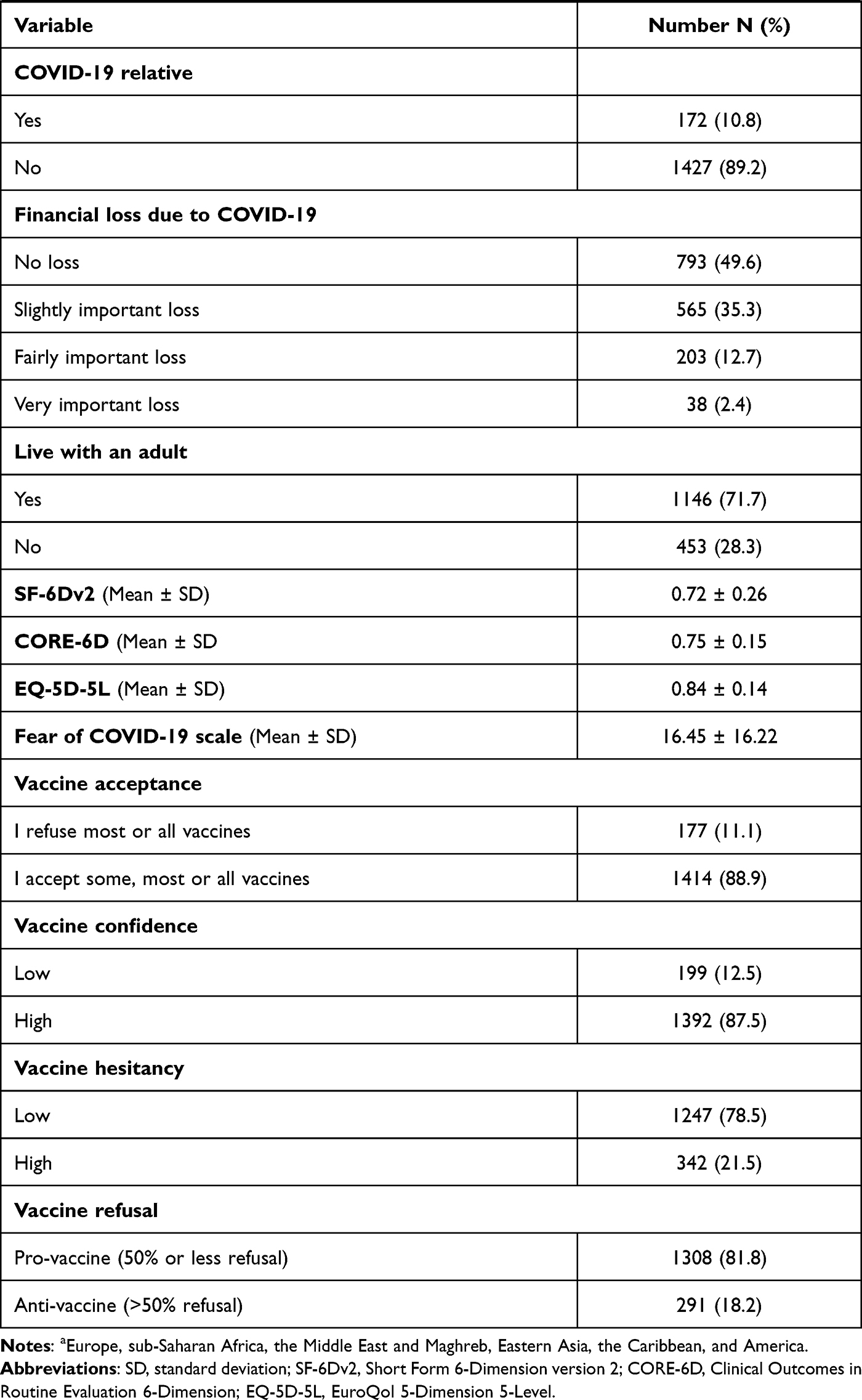 |
Table 1 Personal Characteristics of the Study Participants in the Province of Quebec, Canada, 2020 (N = 1599) |
Most study participants were born in Canada (90.7%), from Canadian parents (87.4%), were Canadian citizen (96.7%), non-smokers (81.1%), non-essential worker during the pandemics (82.3%), and not a health care worker (92.3%). Over 85% of the study participants indicated that themselves, their family or relatives did not suffer from COVID-19 at the time of the survey. Slightly more than half were female (51.3%) and employed (51.1%). Most of them were above 40 years of age (69.3%) (mean ±standard deviation (SD), 50 ± 16.23 years), married (59.1%), educated with a college degree or less (64.3%), urban resident (69.7%), living in their own house (62.5%), and were from outside of the Greater Montreal area (55.5%). Nearly half of them (46.6%) had an annual household income of less than CAD $50,000 (mean ± SD, CAD $ [66,857.41 ± 41,570.27]). Over a quarter of them reported a reduction in quality of life due to physical or mental problems (27.9%). Most of them reported a relatively low sense of coherence (64.8%). Almost half of the study participants (49.2%) indicated that they worked during the COVID-19 crisis, had no financial loss during this crisis (49.6). Mean ± SD score of SF-6Dv2, CORE-6D, EQ-5D-5L, and FCV-19S were 0.72 ± 0.26, 0.75 ± 0.15, 0.84 ± 0.14, and 16.45 ± 16.22, respectively. Most of these sociodemographic variables are representative of the general population in the province of Quebec as reported elsewhere19
Factors Associated with Vaccine Acceptance, Confidence, and Hesitancy in General, and COVID-19 Vaccination Refusal
The univariate analysis suggested that the marital status, education, income, smoking, financial loss, and FCV-19S were significantly associated with vaccine acceptance. Regarding vaccine confidence, a number of factors such as gender, age, marital status, occupation, education, income, residence, housing status, country of parents, residence status, smoking, financial loss, SOC-3 and FCV-19S were significantly associated in univariate analysis. Similarly, gender, age, marital status, education, income, housing status, work as other essential worker, caretaker, smoking, financial loss, SOC-3, CORE-6D, SF-6Dv2, FCV-19S, and EQ-5D-5L were significantly associated with vaccine hesitancy in univariate analysis. Likewise, gender, age, education, income, housing status, and perceived risk were significantly associated with vaccine refusal (Tables 2 and 3).
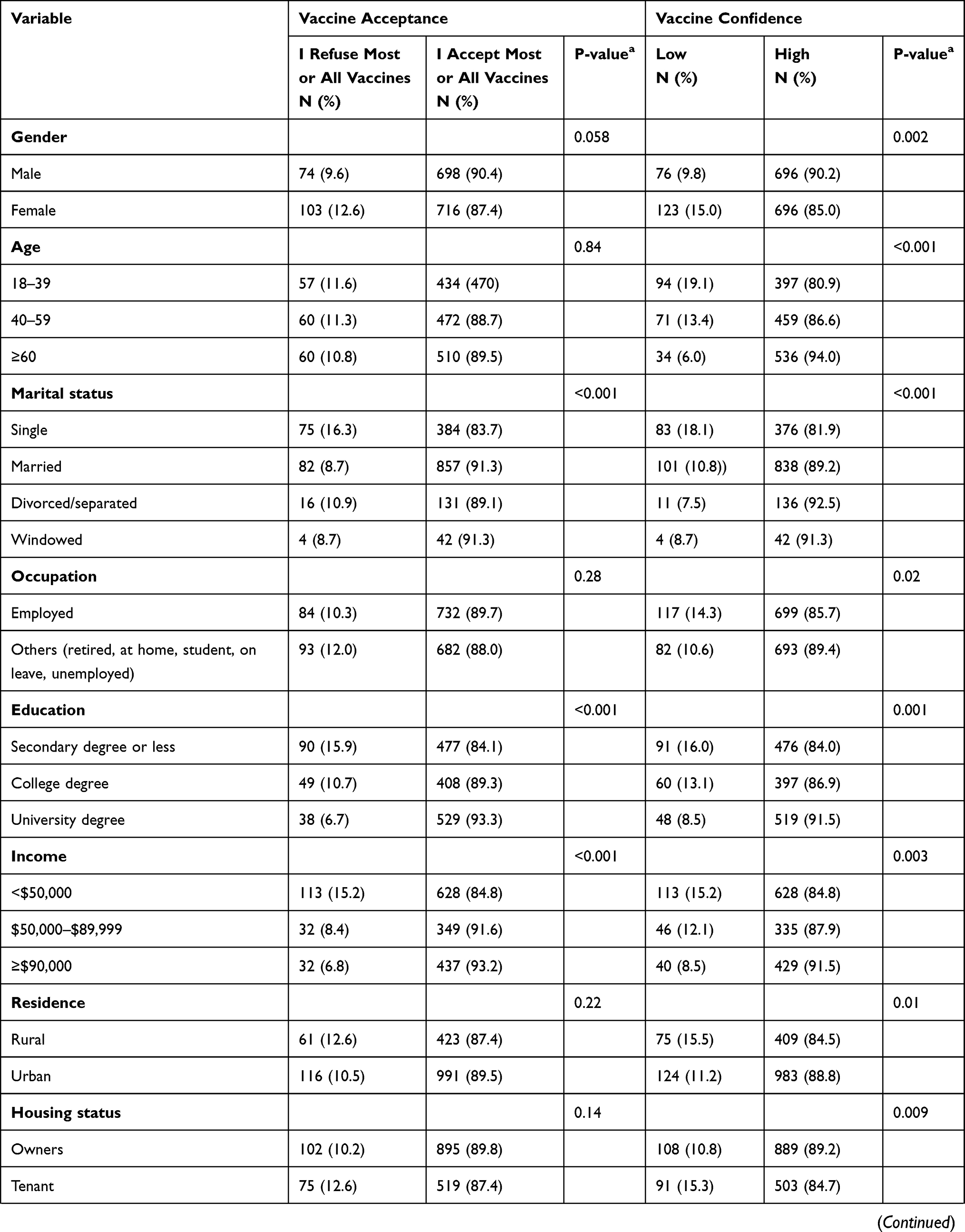 | 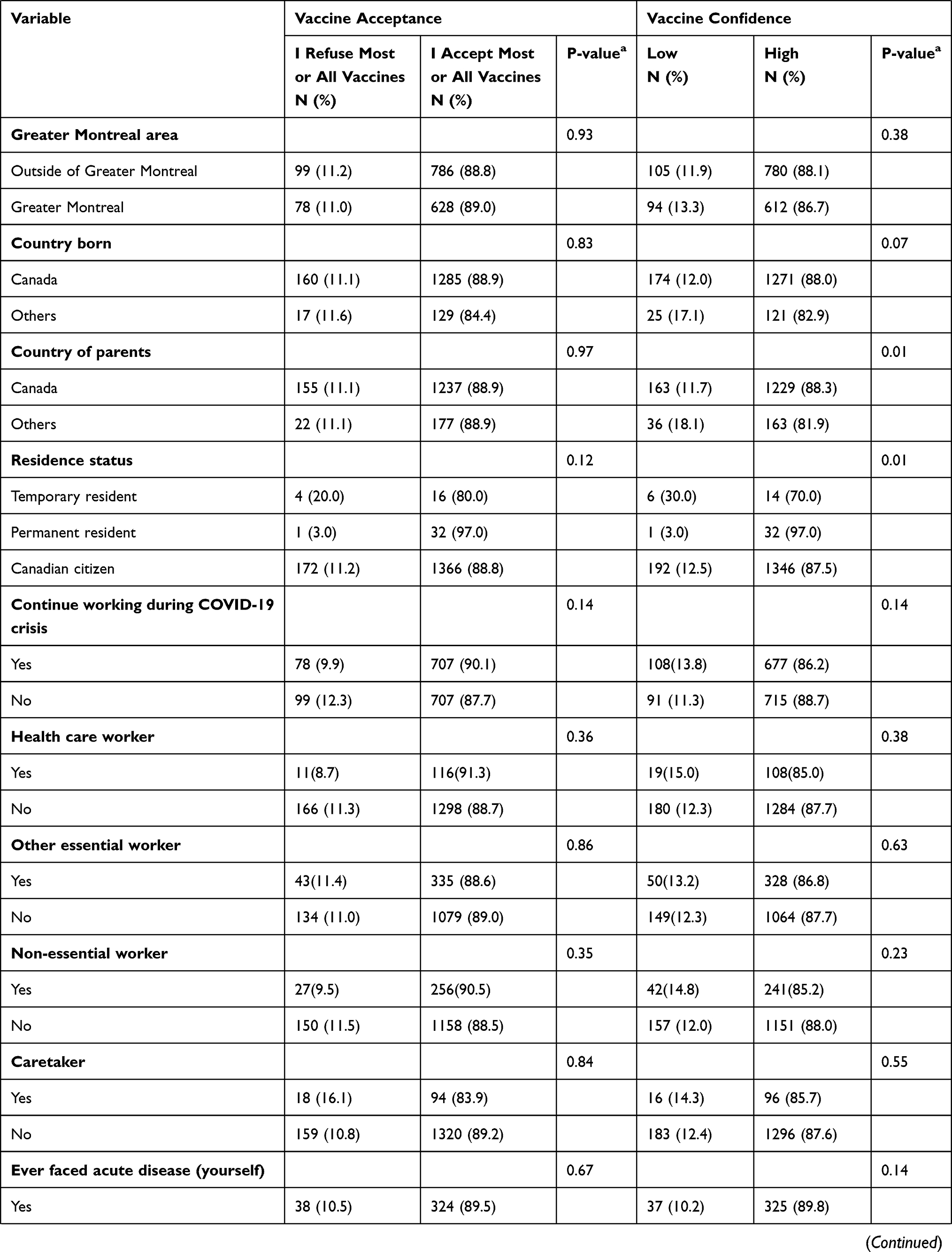 | 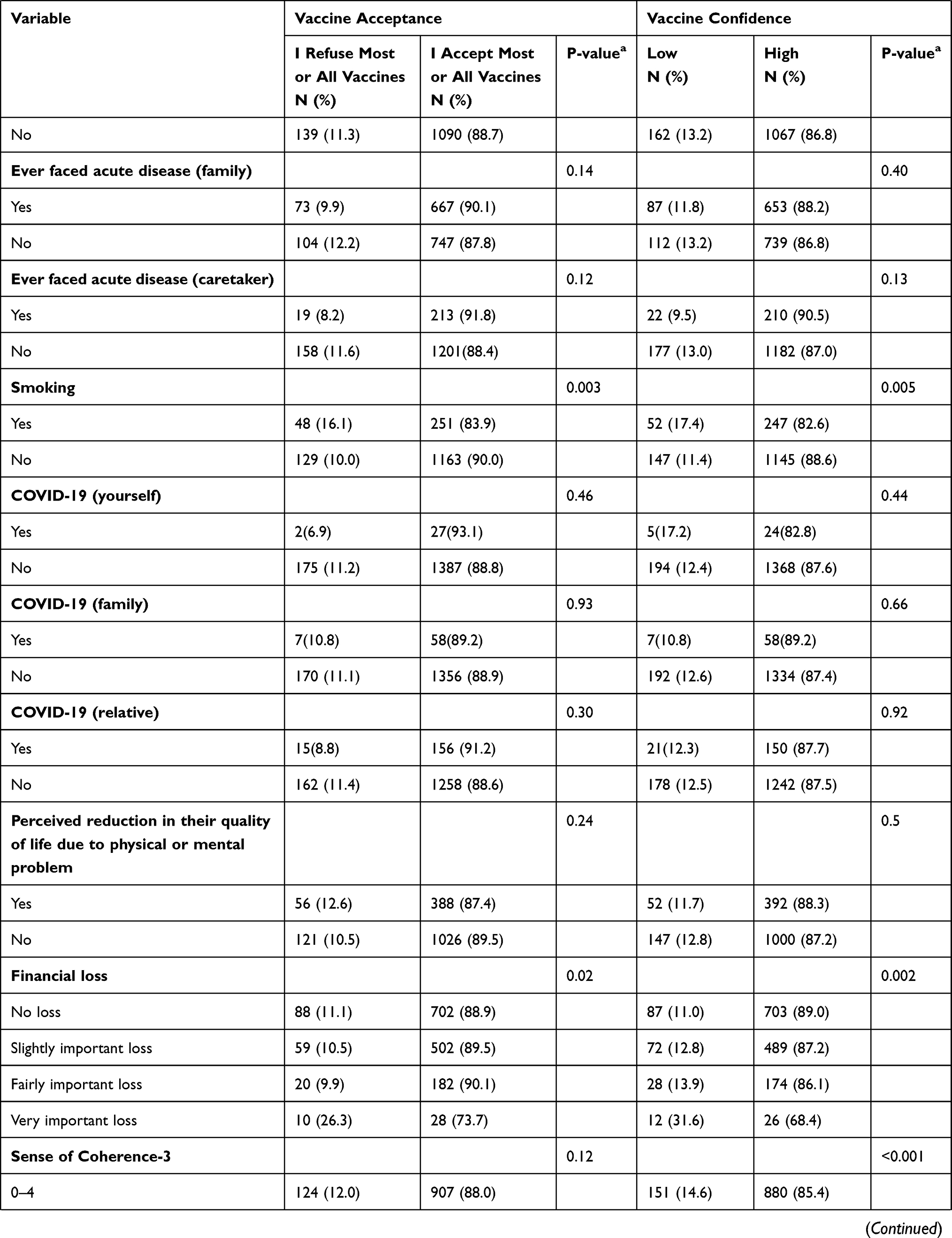 | 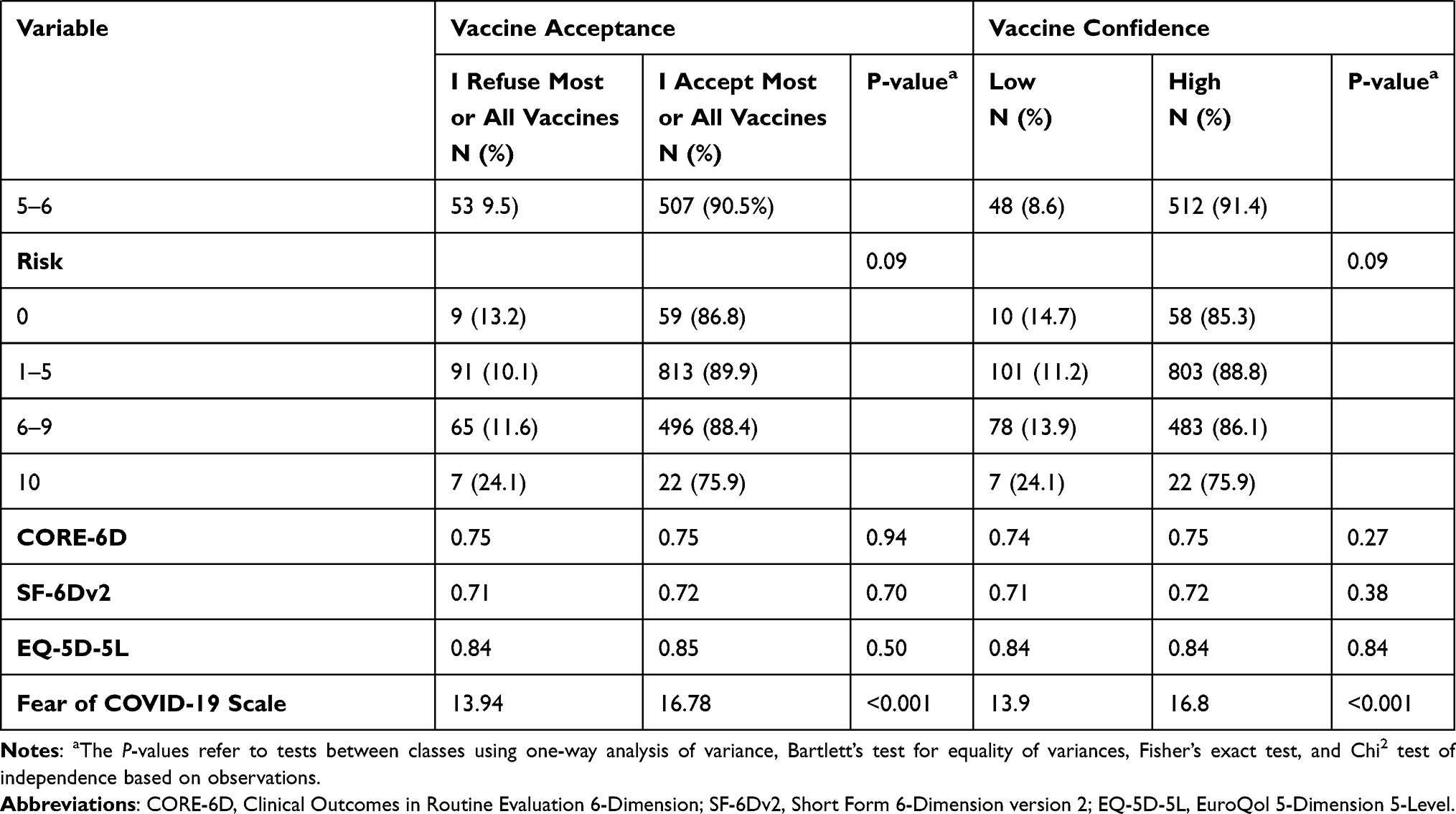 |
Table 2 Univariate Analysis of Factors Associated with Vaccine Acceptance, and Confidence, in General, in the Province of Quebec, Canada, 2020 |
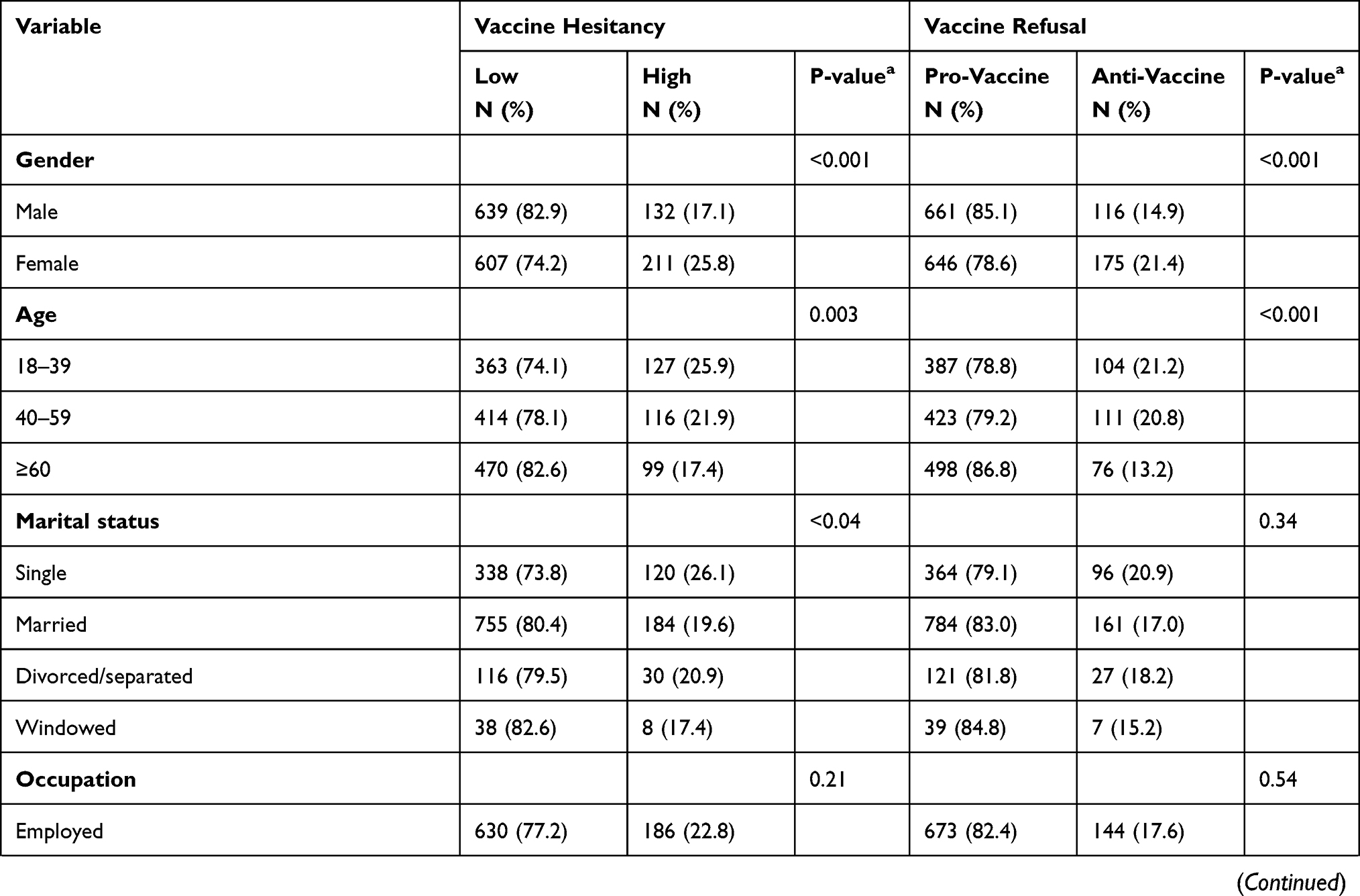 | 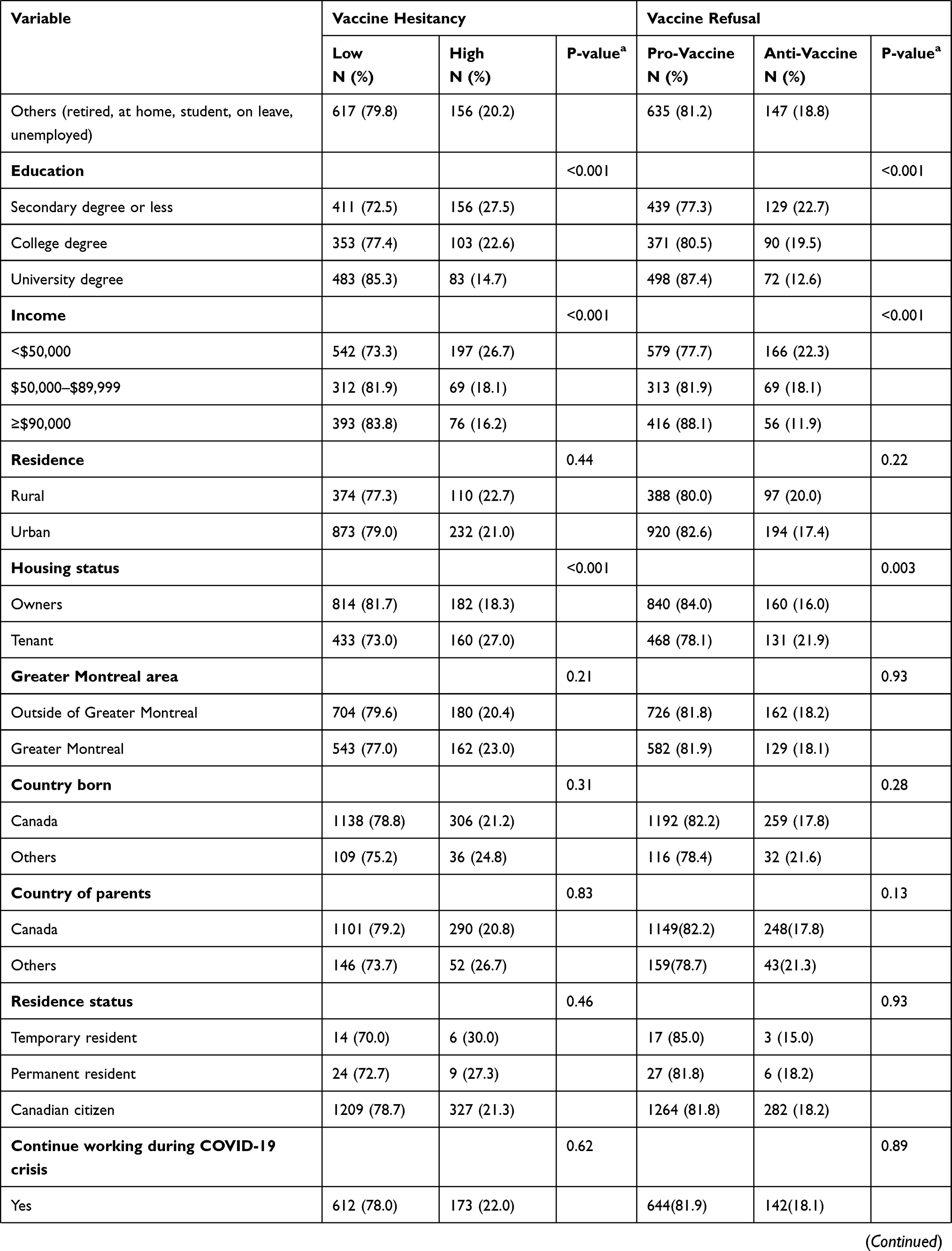 | 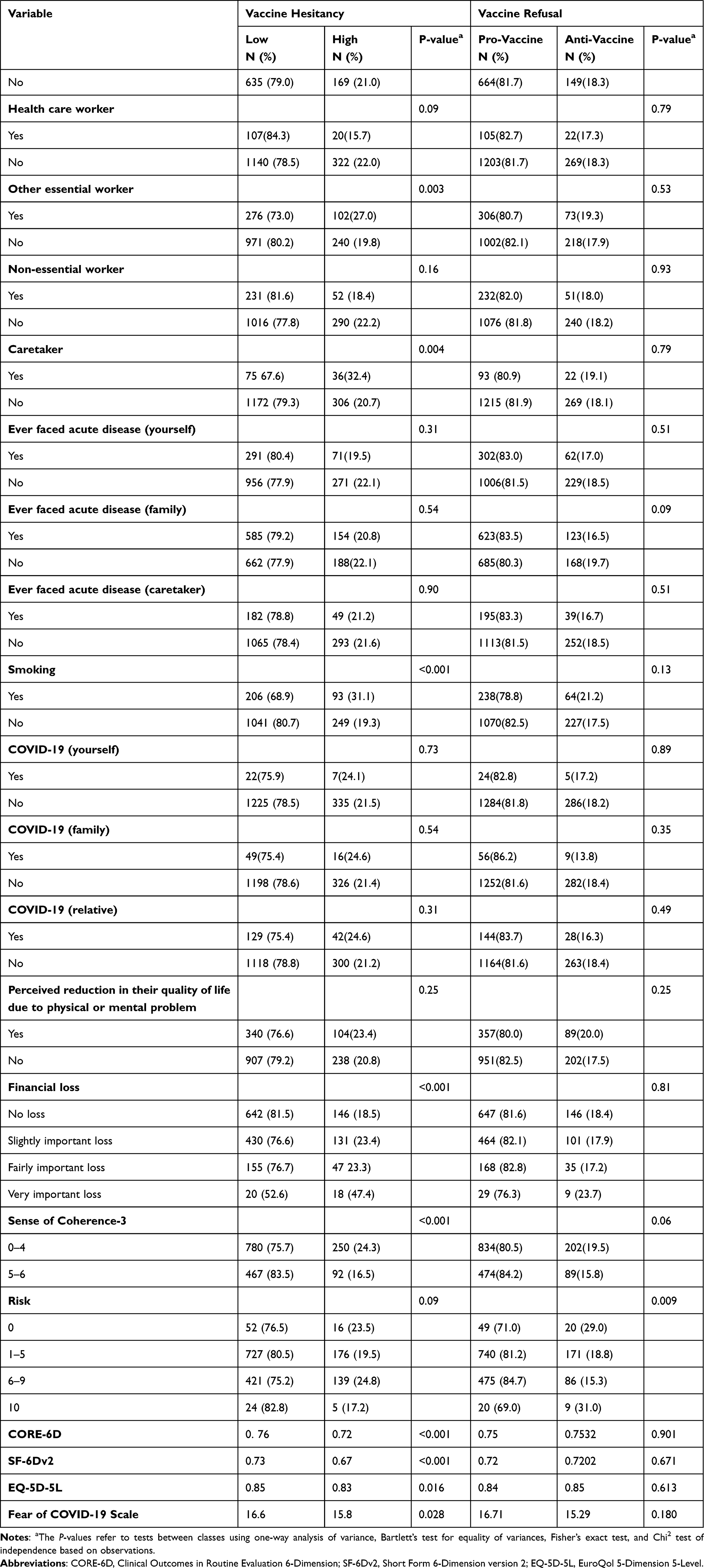 |
Table 3 Univariate Analysis of Factors Associated with Vaccine Hesitancy in General and COVID-19 Vaccination Refusal in the Province of Quebec, Canada, 2020 |
The final adjusted logistic regression model is presented in Tables 4 and 5. In this model, only four factors (education, income, smoking, and FCV-19S) appeared to be significantly associated with vaccine acceptance. Thus, participants with college degree (OR = 1.58, 95% CI: 1.06–2.33), university degree (OR = 2.21, 95% CI: 1.43–3.40), annual income of CAD $50,000-$89,999 (OR = 1.85, 95% CI: 1.21–2.85) and ≥CAD $90,000 (OR = 2.49, 95% CI: 1.60–3.88), and high FCV-19S (OR = 1.11, 95% CI: 1.07–1.14) were more likely, while smokers (OR = 0.58, 95% CI: 0.40–0.86) were less likely to be willing to get vaccinated than their counterparts.
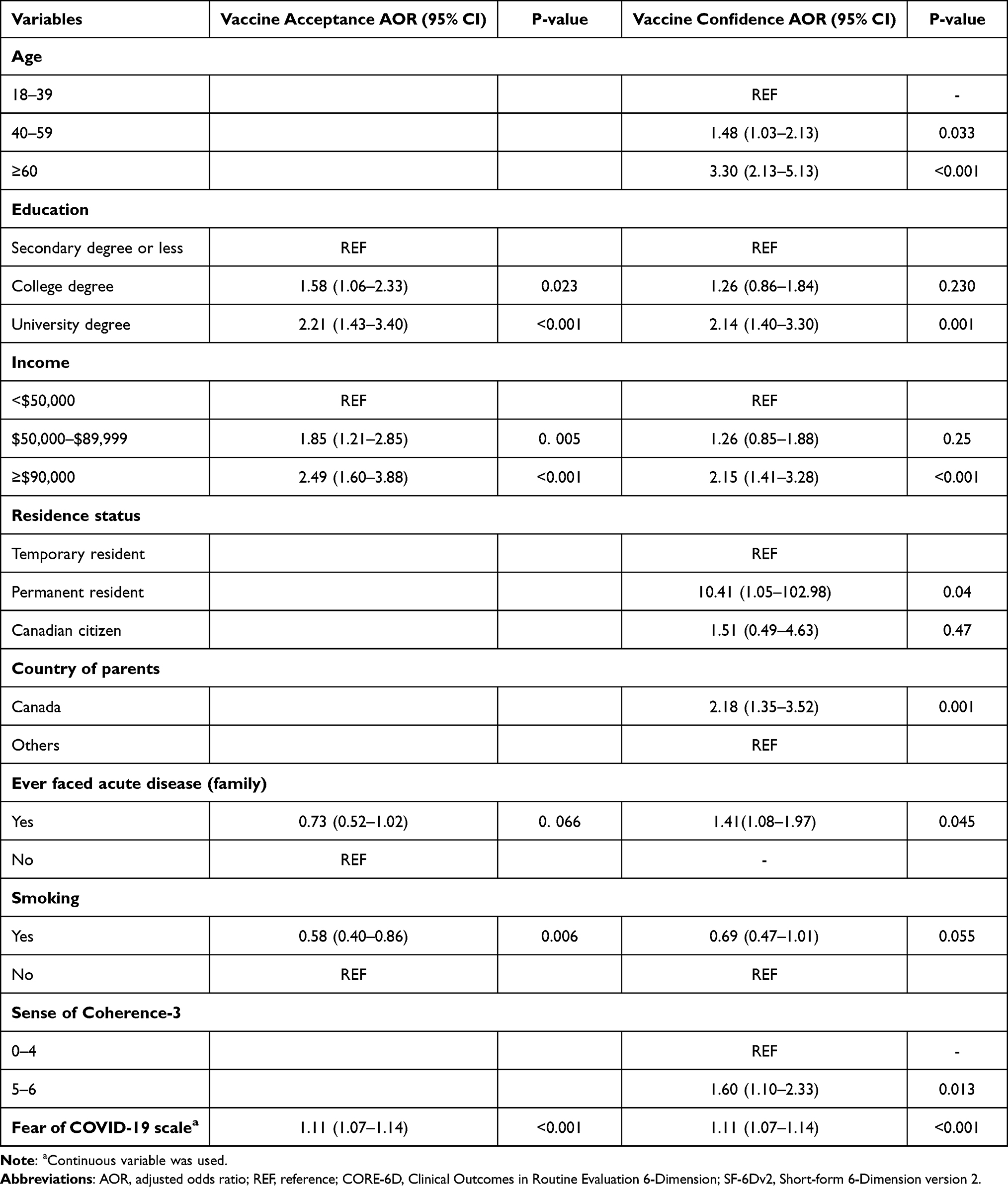 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with Vaccine Acceptance and Confidence, in General, in the Province of Quebec, Canada, 2020 |
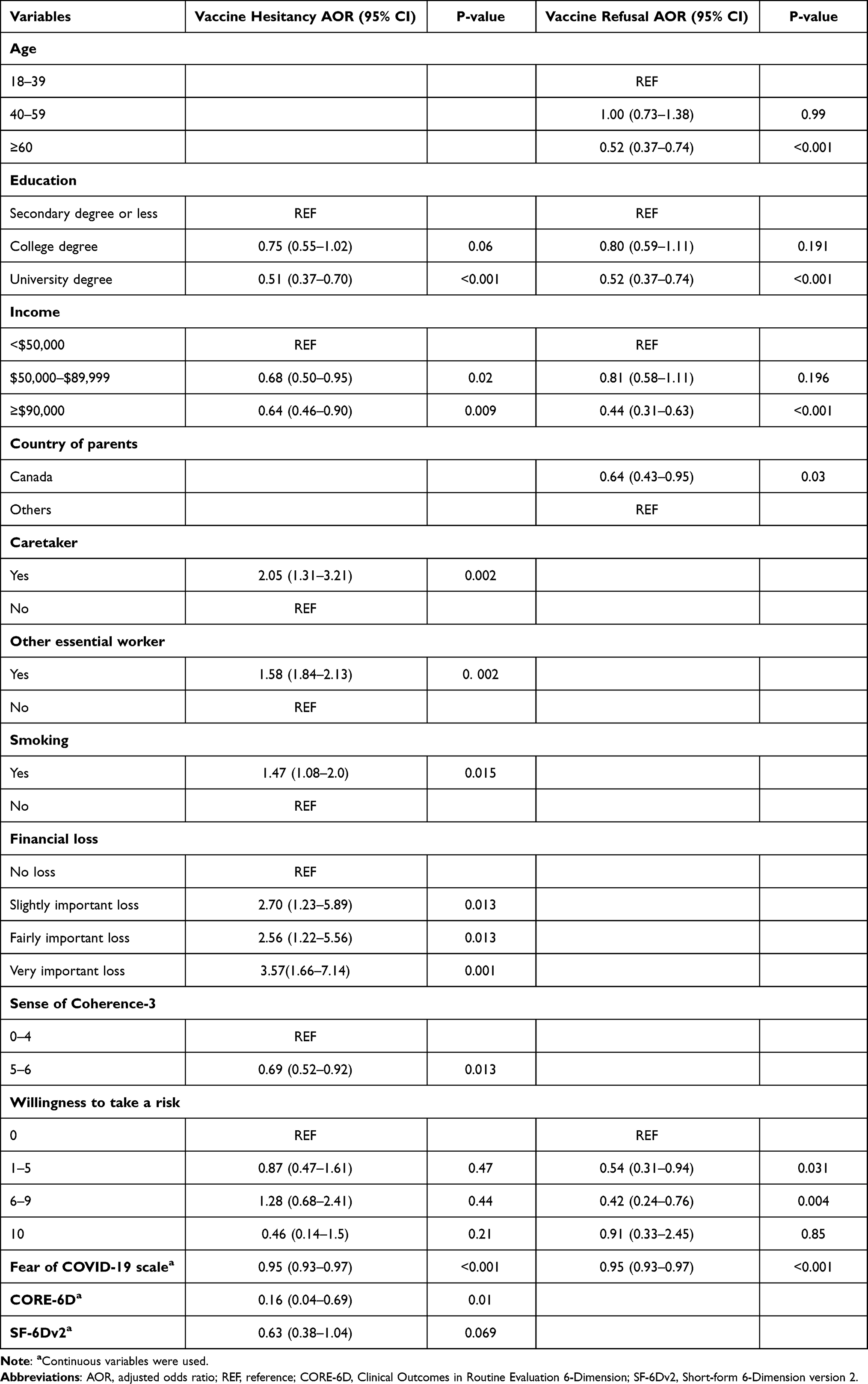 |
Table 5 Multivariable Logistic Regression Analysis of Factors Associated with Vaccine Hesitancy in General and COVID-19 Vaccination Refusal in the Province of Quebec, Canada, 2020 |
Regarding vaccine confidence, age, education, income, residence status, country of parents, ever faced acute disease in the family, SOC-3, and FCV-19S remained significantly associated with high level of vaccine confidence. Accordingly, age group 40–59 years (OR = 1.48, 95% CI: 1.03–2.13), ≥60 years (OR = 3.30, 95% CI: 2.13–5.13), university degree (OR = 2.14, 95% CI: 1.40–3.30), annual income ≥CAD $90,000 (OR = 2.15, 95% CI: 1.41–3.28), permanent resident in Canada (OR = 10.41, 95% CI: 1.05–102.98), country of parents from Canada (OR = 2.18, 95% CI: 1.35–3.52), ever faced acute disease in the family (OR = 1.41, 95% CI: 1.08–1.97), higher SOC-3 (OR = 1.60, 95% CI: 1.10–2.33), and being afraid of COVID-19 (FCV-19S) (OR = 1.11, 95% CI: 1.07–1.14) were significantly positively associated with high level of vaccine confidence.
Similarly, the final multivariate analysis model also demonstrated several predictors such as education, income, acting as caretaker, other essential worker, smoking, financial loss, SOC-3, FCV-19S, and CORE-6D, for vaccination hesitancy. Study participants educated with university degree (OR = 0.51, 95% CI: 0.37–0.70), annual income of CAD $50,000-$89,999 (OR = 0.68, 95% CI: 0.50–0.95) and ≥CAD $90,000 (OR = 0.64, 95% CI: 0.46–0.90), higher SOC-3 (OR = 0.69, 95% CI: 0.52–0.92), FCV-19S (OR = 0.95, 95% CI: 0.93–0.97), and CORE-6D (OR = 0.16, 95% CI: 0.04–0.69), had lower odds of having high level of vaccine hesitancy, while those who were acting as caretaker (OR = 2.05, 95% CI: 11.31–3.21), other essential workers (OR = 1.58, 95% CI: 11.84–2.13), smokers (OR = 1.47, 95% CI: 1.08–2.0) and those having slightly important financial loss (OR = 2.70, 95% CI: 1.23–5.89), fairly important financial loss (OR = 2.56, 95% CI: 1.22–5.56), and very important financial loss (OR = 3.57, 95% CI: 1.66–7.14), had higher odds of having high level of vaccine hesitancy. Likewise, our adjusted multivariate analysis demonstrated a number of associates of COVID-19 vaccine refusal such as age, education, income, country of parents, willingness to take risk about vaccination, and FCV-19S. Study participants of age group ≥60 years (OR = 0.52, 95% CI: 0.37–0.74), educated with university degree (OR = 0.52, 95% CI: 0.37–0.74), annual income of ≥CAD $90,000 (OR = 0.44, 95% CI: 0.31–0.63), country of parents from Canada (OR = 0.64, 95% CI: 0.43–0.95), a score of1–5 willingness to risk (OR = 0.54, 95% CI: 0.31–0.94) and score of6–9 willingness to risk (OR = 0.42, 95% CI: 0.24–0.76), and high FCV-19S (OR = 0.95, 95% CI: 0.93–0.97) were less likely to have high level of COVID-19 vaccination refusal. We tested different categorization for the outcomes of interest in order to confirm the above-mentioned results (Supplementary Materials, Tables S2–S6) and they were not very different from the current results for outcome variables.
Discussion
In the present study, out of 1599 study participants, 88.9%, 87.5%, 78.5%, and 18.2%, respectively, indicated their acceptance of some, most or all vaccines, had high level of vaccine confidence, low level of vaccine hesitancy in general, and COVID-19 vaccine refusals. Vaccine acceptance rate was almost similar to what was found in another study in Canada (88.9% vs 82%).20 There could be inter-and-intra country differences in vaccine acceptance rates based on types of vaccines and individual perception of vaccination. It has been reported to have almost 90% (in China) to less than 55% (in Russia) COVID-19 vaccine acceptance rates amidst COVID-19 pandemics.21 In a recent Canadian study conducted among 9252 Saskatchewan adults (≥18 years), 76%, 13% and 11% of the participants, respectively, indicated to be vaccinated or willing to, hesitant and refusal with COVID-19 vaccination22 which is comparable to our current study findings although we observed higher rates for all three dimensions of vaccine acceptance, hesitancy, and refusals, given that we did not use the same methodology to construct these variables and that their data were collected over a longer period. However, these lower rates of outcome of interest found in Saskatchewan adults may be considered in a perspective where Canadians in central provinces such as Saskatchewan and Alberta have been more protesting against COVID-19 vaccine mandates.23
Our study found that higher education attainment and higher income were significantly positively associated with vaccine acceptance, which is consistent with several other previous study findings.21,24 We also found that having a higher fear of COVID-19 (FCV-19S) was positively associated with willingness to have vaccine acceptance. We assume that increased fear of such emerging disease might have created the participants to be of more health concern. Similar to our study findings, previous studies supported the notion of being afraid of COVID-19 to influence participants to accept vaccination.25,26 This could be explained in a way that the growing sense of realization about risk of acquiring disease might influence people to adopt preventive strategies. Identification of the risk perception towards specific health intervention is therefore necessary, especially during pandemic situation.27
Higher vaccine confidence level could impact vaccination status, and it has been demonstrated a positive association between vaccine confidence and vaccine uptake.28 However, there are several factors associated with vaccine confidence such as the vaccine safety and effectiveness among many others that are of major concern.29 We found several sociodemographic factors in the study participants such as an older age group, higher education achievement, and income, being permanent resident in Canada, having parents born in Canada, ever faced acute disease in the family, and FCV-19S, to produce higher odds of having of a high level of vaccine confidence. These findings seem to like what have been found in the literature throughout the COVID-19 pandemic times especially for those studies related to COVID-19 vaccine confidence.24,29 The possible reasons are obvious as people at this moment are highly concerned with the fatalities associated with COVID-19. Nonetheless, this does not always seem true for vaccination in general, for example, a global study being held in 2016 to assess the general vaccine confidence that included a 67-country survey uncovered that higher educational attainment, good access to health services and socio-economic status had an inverse relation with vaccine confidence.30 Nonetheless, the vaccine confidence level could be dynamic as it could be determined by many other factors such as the importance of vaccination, vaccine safety concerns and effectiveness.28,30 Hence, periodic follow-up study should be recommended.
Vaccine hesitancy is a complex issue associated with a variety of context-specific factors. Decreasing vaccine confidence is considered as one of the potential contributors to the reduced vaccine coverage rates.31 A large-scale global study being conducted among 32,028 subjects from eight different countries around the world reported an overall 27% of the participants who demonstrated vaccine hesitancy with intercountry variation (France, 47.3% vs Brazil, 9.6%) between March 2020 and January 2021.32 In our study, we observed that more than three fourth of the study participants had low level of vaccine hesitancy. Higher educational achievement and income, as well as higher FCV-19S and HRQoL (CORE-6D) scores, were less likely to have high level of vaccine hesitancy, while those acting as caretakers and other essential workers had higher odds of having high level of vaccine hesitancy. Comparable to our study finding, Muhajarine et al found that not being afraid of COVID-19 were significantly associated with increased likelihood of vaccine hesitancy.22 In addition, we suppose that the reason behind having lower vaccine hesitancy to those of having higher HRQoL could be due to our study participants being younger who are supposed to have less fatality or to be hospitalized compared to elderly people.33 Elderly people who have chronic conditions expressed low HRQoL and are at higher risk to get COVID-19 than healthy people, which make them afraid of the virus and subsequently decrease their vaccine hesitancy.34 It might be possible that the other essential workers (eg, truckers) were more hesitant to COVID-19 vaccine because most of them have low education level which was associated with high vaccine hesitancy in our results.35 There are also possibly religious and cultural beliefs and personal values (freedom) which opposed the enforcement of vaccine by the government in different countries and subsequently increased their mistrust and less confidence in vaccine.36 Other studies showed the detrimental effect of socio-economic gradients on higher level of vaccine hesitancy.37,38 Our study also revealed that those with slightly important financial loss, fairly important financial loss, and very important financial loss were more likely to have high level of vaccine hesitancy indicating the influence of financial losses on incremental vaccine hesitancy. Increasing vaccine uptake strategy should therefore target socioeconomically disadvantaged group who are more at risk of having vaccine-preventable diseases.38
In addition, more interestingly, our analyses demonstrated that participants having a higher sense of coherence were more likely to have both higher vaccine confidence and lower level of vaccine hesitancy, while smokers were less willing to have vaccine acceptance, and higher vaccine hesitancy. Other studies have highlighted the higher sense of coherence in terms of healthcare and healthcare utilization benefits.39,40 We presume that the higher sense of coherence in participants might have increased the perceived need and positive attitudes towards vaccine acceptance. In line with our study findings, studies from the UK and the USA also observed that smokers were uncertain and unwilling to be vaccinated for COVID-19.41,42 This could be argued that smokers do have a negative attitude towards vaccine, were unknown about the future effects of vaccination and/or believed in natural immunity.41 Smoking cessation interventions would therefore potentially be beneficial to improve vaccine uptake, besides reducing the risk of infection and spread of COVID-19.43
Our study more specifically identified the key drivers of COVID-19 vaccine refusals. Study participants of age group ≥60 years, university degree education, annual income of ≥CAD $90,000, country of parents from Canada, a higher score (1–5 and 6–9) for willingness to take a risk, and high fear of COVID-19 were less likely to have a high level of COVID-19 vaccination refusal. Muhajarine et al found that lower education level, being born outside Canada, and not being afraid of COVID-19 were significantly associated with a higher likelihood of vaccine refusal, which is similar to our study findings.22 The increased vaccine refusal among immigrants may be explained by the fact that most of them have religious and cultural beliefs which are against vaccine uptake.44 Another cross-sectional study led among women in the UK found that ethnic minority women were twice more likely to reject COVID-19 vaccine when not pregnant, pregnant, and for their babies compared with white ethnic women.45 Soares et al also reported that vaccine refusal was higher among young people, those who had a loss of income during the pandemic and those having low confidence in the COVID-19 vaccine.46
We recommend considering these predictors while initiating interventions to improve the COVID-19 vaccination rates to develop the optimum level of herd immunity in the province of Quebec. This study is meaningful in the context of current COVID-19 pandemic situation with a surge of new variants and has some important strengths to mention about. Firstly, this study involved a representative sample that might allow extrapolation of study outcome in the province of Quebec, Canada, and other similar settings. Secondly, although the study was based on online survey questionnaires, it has a high response rate of 44.23%. Thirdly, we employed validated study instruments in collecting relevant information. Lastly, we conducted robust statistical analyses with various statistical modeling in order to confirm the consistency of the results presented. However, the study should be interpreted in the light of some specific inherent limitations. Indeed, our study participants were only French Speakers and those who could not access the online survey questionnaire because of physical health and other concerns were left behind. This could obviously have external validity threat to use the study outcome beyond French speaker participants and those not reached online. In addition, our study results of vaccine acceptance, confidence and hesitancy might have been influenced by contextual factors since we conducted the study just before the beginning of the COVID-19 vaccination campaign in Quebec (ie, December 2020). Finally, we cannot suggest cause-and-effect relationships as this is a cross-sectional study. However, our study revealed the proportion of participants with COVID-19 vaccination refusal behavior and its associated factors using specific questionnaires. Local area research could provide essential data needed for area-specific interventions. Further studies should focus on the key drivers of low level of vaccine acceptance, confidence, and high level of hesitancy in the context of fulfillment of recommended doses and booster doses for COVID-19 vaccination.
Conclusions
Our study reported that more than three fourth of the study participants indicated the acceptance of some, most or all vaccines, high level of vaccine confidence, low level of vaccine hesitancy in general, and nearly one in five indicated COVID-19 vaccine refusals in 2020. Since some socio-demographic and health-related quality of life factors were associated with the outcome variables, those factors should be sought while designing interventions to improve COVID-19 vaccination rates to develop the optimum level of herd immunity in the province of Quebec, Canada, and in similar settings. Additional studies should be performed to investigate the key drivers of compliance to recommended doses of COVID-19 vaccination including booster doses.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work. Alexis Nizigiyimana and Dilaram Acharya have contributed equally to this work and share first authorship.
Funding
This study was funded by the Fondation de l’IUSMM and supported by the CIRANO.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. World Health Organization. WHO Coronavirus (COVID-19) Dashboard; 2022. Available from: https://covid19.who.int/.
2. Our World in data. Coronavirus (COVID-19) Vaccinations; 2022. Available from: https://ourworldindata.org/covid-vaccinations.
3. Leng A, Maitland E, Wang S, et al. Individual preferences for COVID-19 vaccination in China. Vaccine. 2021;39(2):247–254. doi:10.1016/j.vaccine.2020.12.009
4. Dyer O. Covid-19: unvaccinated face 11 times risk of death from delta variant, CDC data show. BMJ. 2021;374:n2282. doi:10.1136/bmj.n2282
5. Heidi JL, David S, Pauline P, et al. Measuring vaccine confidence: analysis of data obtained by a media surveillance system used to analyse public concerns about vaccines. Lancet Infect Dis. 2013;13(7):606–613. doi:10.1016/S1473-3099(13)70108-7
6. Detoc M, Bruel S, Frappe P, Tardy B, Botelho-Nevers E, Gagneux-Brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine. 2020;38(45):7002–7006. doi:10.1016/j.vaccine.2020.09.041
7. Harrison EA, Wu JW. Vaccine confidence in the time of COVID-19. Eur J Epidemiol. 2020;35(4):325–330. doi:10.1007/s10654-020-00634-3
8. Griffith J, Marani H, Monkman H. COVID-19 vaccine hesitancy in Canada: content analysis of tweets using the theoretical domains framework. J Med Internet Res. 2021;23(4):e26874. doi:10.2196/26874
9. Taylor S, Landry CA, Paluszek MM, Groenewoud R, Rachor GS, Asmundson GJG. A proactive approach for managing COVID-19: the importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front Psychol. 2020;11:575950. doi:10.3389/fpsyg.2020.575950
10. Brown KF, Kroll JS, Hudson MJ, et al. Factors underlying parental decisions about combination childhood vaccinations including MMR: a systematic review. Vaccine. 2010;28(26):4235–4248. doi:10.1016/j.vaccine.2010.04.052
11. Larson HJ, Cooper LZ, Eskola J, Katz SL, Ratzan S. Addressing the vaccine confidence gap. Lancet. 2011;378(9790):526–535. doi:10.1016/S0140-6736(11)60678-8
12. Meier C. Covid-19: new data suggests herd immunity unachievable in New Zealand; 2022.
13. Gouvernement du Québec. COVID-19 vaccination data; 2022. Available from: https://www.quebec.ca/en/health/health-issues/a-z/2019-coronavirus/situation-coronavirus-in-quebec/covid-19-vaccination-data.
14. Brazier JE, Mulhern BJ, Bjorner JB, et al. Developing a new version of the SF-6D health state classification system from the SF-36v2. Medical Care. 2020;58:6.
15. Xie F, Pullenayegum WE, Gaebel K, et al. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98–105. doi:10.1097/MLR.0000000000000447
16. Mavranezouli I, Brazier JE, Rowen D, Barkham M. Estimating a preference-based index from the clinical outcomes in routine evaluation-outcome measure (CORE-OM): valuation of CORE-6D. Med Decis Making. 2013;33(3):381–395. doi:10.1177/0272989X12464431
17. Attieh R, Koffi K, Toure M, Parr-Labbe E, Pakpour AH, Poder TG. Validation of the Canadian French version of the fear of COVID-19 scale in the general population of Quebec. Brain Behav. 2022;12:e32550. doi:10.1002/brb3.2550
18. Schumann A, Hapke U, Meyer C, Rumpf H-J, John U. Measuring sense of coherence with only three items: a useful tool for population surveys. Br J Health Psychol. 2003;8(4):409–421. doi:10.1348/135910703770238275
19. Poder TG, Carrier N. Quebec health-related quality of life population norms in adults using the SF-6Dv2: decomposition by sociodemographic data and health problems. Med Care. 2022;60(7):545–554. doi:10.1097/MLR.0000000000001730
20. Crawshaw J, Konnyu K, Castillo G, et al. Factors affecting COVID-19 vaccination acceptance and uptake among the general public. Living Behavioural Science Evidence Synthesis; 2021.
21. Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–228. doi:10.1038/s41591-020-1124-9
22. Muhajarine N, Adeyinka DA, McCutcheon J, Green KL, Fahlman M, Kallio N. COVID-19 vaccine hesitancy and refusal and associated factors in an adult population in Saskatchewan, Canada: evidence from predictive modelling. PLoS One. 2021;16(11):e0259513. doi:10.1371/journal.pone.0259513
23. CRISIS24. Canada: protests planned in multiple locations to oppose COVID-19 vaccine mandates and other measures; 2021. Available from: https://crisis24.garda.com/alerts/2021/09/Canada-protests.
24. Joshi A, Kaur M, Kaur R, Grover A, Nash D, El-Mohandes A. Predictors of COVID-19 vaccine acceptance, intention, and hesitancy: a scoping review. Front Public Health. 2021;9:698111. doi:10.3389/fpubh.2021.698111
25. Bendau A, Plag J, Petzold MB, Ströhle A. COVID-19 vaccine hesitancy and related fears and anxiety. Int Immunopharmacol. 2021;97:107724. doi:10.1016/j.intimp.2021.107724
26. Bono SA, Faria de Moura Villela E, Siau CS, et al. Factors affecting COVID-19 vaccine acceptance: an international survey among low- and middle-income countries. Vaccines. 2021;9(5):515.
27. Wise T, Zbozinek TD, Michelini G, Hagan CC, Mobbs D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R Soc Open Sci. 2020;7(9):200742. doi:10.1098/rsos.200742
28. de Figueiredo A, Simas C, Karafillakis E, Paterson P, Larson HJ. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet. 2020;396(10255):898–908. doi:10.1016/S0140-6736(20)31558-0
29. Ruiz JB, Bell RA. Predictors of intention to vaccinate against COVID-19: results of a nationwide survey. Vaccine. 2021;39(7):1080–1086. doi:10.1016/j.vaccine.2021.01.010
30. Larson HJ, de Figueiredo A, Xiahong Z, et al. The state of vaccine confidence 2016: global insights through a 67-country survey. EBioMedicine. 2016;12:295–301. doi:10.1016/j.ebiom.2016.08.042
31. Larson HJ, Jarrett C, Eckersberger E, Smith DMD, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. 2014;32(19):2150–2159. doi:10.1016/j.vaccine.2014.01.081
32. Stojanovic J, Boucher VG, Gagne M, et al. Global trends and correlates of COVID-19 vaccination hesitancy: findings from the iCARE study. Vaccines. 2021;9(6):661. doi:10.3390/vaccines9060661
33. Zimmermann P, Curtis N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV- 2 infections. Arch Dis Child. 2020;106:429–439.
34. Centers for Diseases Control and Prevention. People with Certain Medical Conditions; 2022. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
35. Dubinski K. Trucker convoy against vaccine mandates rolls through Ontario en route to Ottawa. Canadian Broadcasting Corporation(CBC); 2022. Available from: https://www.cbc.ca/news/Canada/london/trucker-protest-convoy-southwestern-ontario-1.6329118.
36. Dubinski K. Trucker convoy against vaccine mandates rolls through Ontario en route to Ottawa. CBC News; 2022.
37. Bertoncello C, Ferro A, Fonzo M, et al. Socioeconomic determinants in vaccine hesitancy and vaccine refusal in Italy. Vaccines. 2020;8(2):276. doi:10.3390/vaccines8020276
38. Chaudhary FA, Ahmad B, Khalid MD, Fazal A, Javaid MM, Butt DQ. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum Vaccin Immunother. 2021;17(10):3365–3370. doi:10.1080/21645515.2021.1944743
39. Kimhi S, Eshel Y, Zysberg L, Hantman S, Enosh G. Sense of coherence and socio-demographic characteristics predicting posttraumatic stress symptoms and recovery in the aftermath of the Second Lebanon War. Anxiety Stress Coping. 2010;23(2):139–152. doi:10.1080/10615800902971513
40. Elyasi M, Abreu LG, Olsen C, et al. Parent’s sense of coherence and children’s oral health-related behaviors: is there an association? Pediatr Dent. 2018;40(1):23–29.
41. Jackson SE, Paul E, Brown J, Steptoe A, Fancourt D. Negative vaccine attitudes and intentions to vaccinate against COVID-19 in relation to smoking status: a population survey of UK adults. Nicotine Tob Res. 2021;23(9):1623–1628. doi:10.1093/ntr/ntab039
42. Masson CL, McCuistian C, Straus E, et al. COVID-19 vaccine trust among clients in a sample of California residential substance use treatment programs. Drug Alcohol Depend. 2021;225:108812. doi:10.1016/j.drugalcdep.2021.108812
43. Paul Bramadat P, Benjamin L, N MacDonald, et al. COVID −19 VACCINE: religion, trust and vaccine acceptance. Royal Sociiety of Canada; 2021. Available from: https://rsc-src.ca/en/voices/covid-19-vaccine-religion-trust-and-vaccine-acceptance.
44. Paul Bramadat BLB, MacDonald N. COVID −19 vaccine: religion, trust and vaccine acceptance; 2021.
45. Skirrow H, Barnett S, Bell S, et al. Women’s views on accepting COVID-19 vaccination during and after pregnancy, and for their babies: a multi-methods study in the UK. BMC Pregnancy Childbirth. 2022;22(1):33. doi:10.1186/s12884-021-04321-3
46. Soares P, Rocha JV, Moniz M, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccines. 2021;9:3.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.