")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Predictors of Influenza PCR Positivity in Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Authors Chen CYJ , Yew MS , Abisheganaden JA, Xu H
Received 22 September 2021
Accepted for publication 20 December 2021
Published 6 January 2022 Volume 2022:17 Pages 25—32
DOI https://doi.org/10.2147/COPD.S338757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Calvin You Jia Chen,1 Min Sen Yew,2 John Arputhan Abisheganaden,3 Huiying Xu3
1Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore; 2Department of Cardiology, Tan Tock Seng Hospital, Singapore, Singapore; 3Department of Respiratory and Critical Care Medicine, Tan Tock Seng Hospital, Singapore, Singapore
Correspondence: Huiying Xu
Department of Respiratory and Critical Care Medicine, Tan Tock Seng Hospital, 11 Jln Tan Tock Seng, Singapore
, 308433, Tel +65 6256 6011
Email [email protected]
Purpose: Influenza infection is an important cause of acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Clinical features predicting influenza PCR positivity are unknown. We aim to identify predictors of influenza PCR positivity in AECOPD.
Patients and Methods: A retrospective study of AECOPD cases admitted between 1st January 2016 to 30 June 2017 with combined nasal/throat swabs sent for influenza PCR (Xpert Xpress Flu/RSV) within 24 hours of admission was performed. Clinical parameters and investigations within 24 hours of admission were retrieved from electronic medical records.
Results: Influenza PCR were sent for 925 AECOPD cases (mean age 75 years, 87.9% male). There were 90 PCR positive cases (68 Influenza A, 22 Influenza B). Influenza PCR positive cases had higher temperatures, higher heart rates, lower white cell and lower eosinophil counts. Age, gender, COPD severity, comorbidities and smoking status were similar in both groups. There were no differences in blood pressure, oxygen status, neutrophil or lymphocyte counts, C reactive protein, procalcitonin or chest X-ray consolidation between groups. Higher temperature, higher heart rate, white cell count in the lowest quartile (Q1 < 8.1 x109/L) and non-eosinophilic exacerbations predicted influenza PCR positivity on univariate logistic regression and these factors remained significant after multivariate adjustment (temperature adjusted odds ratio [adj OR] 1.324 [1.009– 1.737], p = 0.043; heart rate adj OR 1.017 [1.004– 1.030], p = 0.011; white cell count Q1 adj OR 3.330 [1.690– 6.562], p = 0.001; eosinophilic exacerbations adj OR 0.390 [0.202– 0.756], p = 0.005).
Conclusion: Higher temperature, higher heart rate, low white cell count (especially when < 8.1 x109/L) and non-eosinophilic exacerbations are independent predictors of influenza PCR positivity in AECOPD cases.
Keywords: chronic obstructive pulmonary disease, exacerbation, influenza, eosinophil
Introduction
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) refers to the acute worsening of respiratory symptoms, such as increase in dyspnea, cough, sputum production and sputum purulence, that results in additional therapy.1 AECOPD is strongly associated with mortality, morbidity, disease progression, Emergency Department visits and hospitalizations.2 Viral infections such as rhinovirus, influenza and respiratory syncytial virus are often implicated in AECOPD.3,4 Recent data based on more sensitive and specific diagnostic methods such as polymerase chain reaction (PCR) reveal higher viral detection rates in AECOPD, suggesting that the role of viruses in AECOPD is more significant than previously reported.5 Furthermore, viral associated AECOPD are more severe6 and frequently associated with complications such as secondary bacterial infections.7 As such, predictors of viral etiology in AECOPD are of clinical importance, especially since they may guide early initiation of antiviral agents such as oseltamivir, which have been shown to reduce disease duration, disease severity and respiratory complications in COPD patients,8,9 especially if started within 12 hours of symptom onset.10 Current guidelines, such as the 2021 GOLD Report,11 2017 European Respiratory Society (ERS)/American Thoracic Society (ATS) Guideline12 and the 2018 NICE Guideline,13 do not provide recommendations on when or in whom to perform influenza PCR in the setting of AECOPD. Despite the potential benefits, indiscriminate influenza PCR testing of all patients presenting with AECOPD is of questionable yield and may not be cost effective. Given the uncertainty of influenza PCR testing in AECOPD, we performed this study with the aim of identifying predictors of influenza PCR positivity in AECOPD patients.
Materials and Methods
Patient Population
This is a retrospective study conducted at Tan Tock Seng Hospital, Singapore, a 1700-bed acute general hospital, between 1st January 2016 to 30 June 2017. Patients admitted for AECOPD with an influenza multiplex real-time, reverse transcriptase PCR (Xpert Xpress Flu/RSV, Cepheid Innovation, California, USA) obtained from combined nasal/throat swab within 24 hours of admission were included. All patients must have a diagnosis of COPD fulfilling the Global Initiatives for Chronic Obstructive Lung Disease (GOLD) criteria14 either in the past, or newly diagnosed based on spirometry performed during the index admission after clinical stabilization if they were not known to have COPD previously. This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval, including a waiver of need for written informed consent, was obtained from the Domain Specific Review Board (DSRB) of the National Healthcare Group (IRB 2018/00237). The data accessed complied with all relevant data protection and privacy regulations.
Clinical Variables and Data Collection
Clinical parameters and investigations within 24 hours of admission were retrieved from medical records, analyzed, and stratified by influenza PCR positivity. Baseline characteristics such as age, sex, GOLD staging for COPD severity, smoking status, comorbidities (specifically diabetes mellitus, hypertension, and hyperlipidemia) and vital signs were recorded. Blood analyses including a full blood count, C reactive protein (CRP) and procalcitonin (PCT) were performed. We defined eosinophilic exacerbation as blood eosinophil count ≥ 300 cells/μL, which was shown to be a reliable marker for sputum eosinophilia15 and used by other studies on COPD exacerbation.16 The presence of pulmonary consolidation on chest radiography performed within 24 hours of admission were determined from review of finalized radiology reports.
Statistical Analysis
All continuous variables were reported either as mean with standard deviation (SD) or median with interquartile range whenever appropriate. Between the influenza PCR positive and negative groups, differences of continuous variables were analyzed with a t-test or Mann–Whitney U-test, while a chi-squared test or Fisher’s exact test was used for comparing differences of categorical variables. Predictors of influenza PCR positivity were identified by performing univariate and multivariate binary logistic regression, with results expressed as the odds ratio (OR) accompanied by the 95% confidence interval (95% CI). Multicollinearity of the model was assessed using the variance-independent factor (VIF). Statistical analysis was performed with the SPSS Statistics software (SPSS 26, SPSS Inc, Chicago, IL, USA) where P < 0.05 was considered significant.
Results
Participants and Baseline Characteristics
There were 925 AECOPD cases included in this study. The baseline characteristics, COPD severity, comorbidities, vital signs on presentation, and investigation results stratified by influenza PCR positivity are shown in Table 1. The included patients were predominantly male (87.9%) with a mean age of 75 years. Most patients were in GOLD Stage II or III.
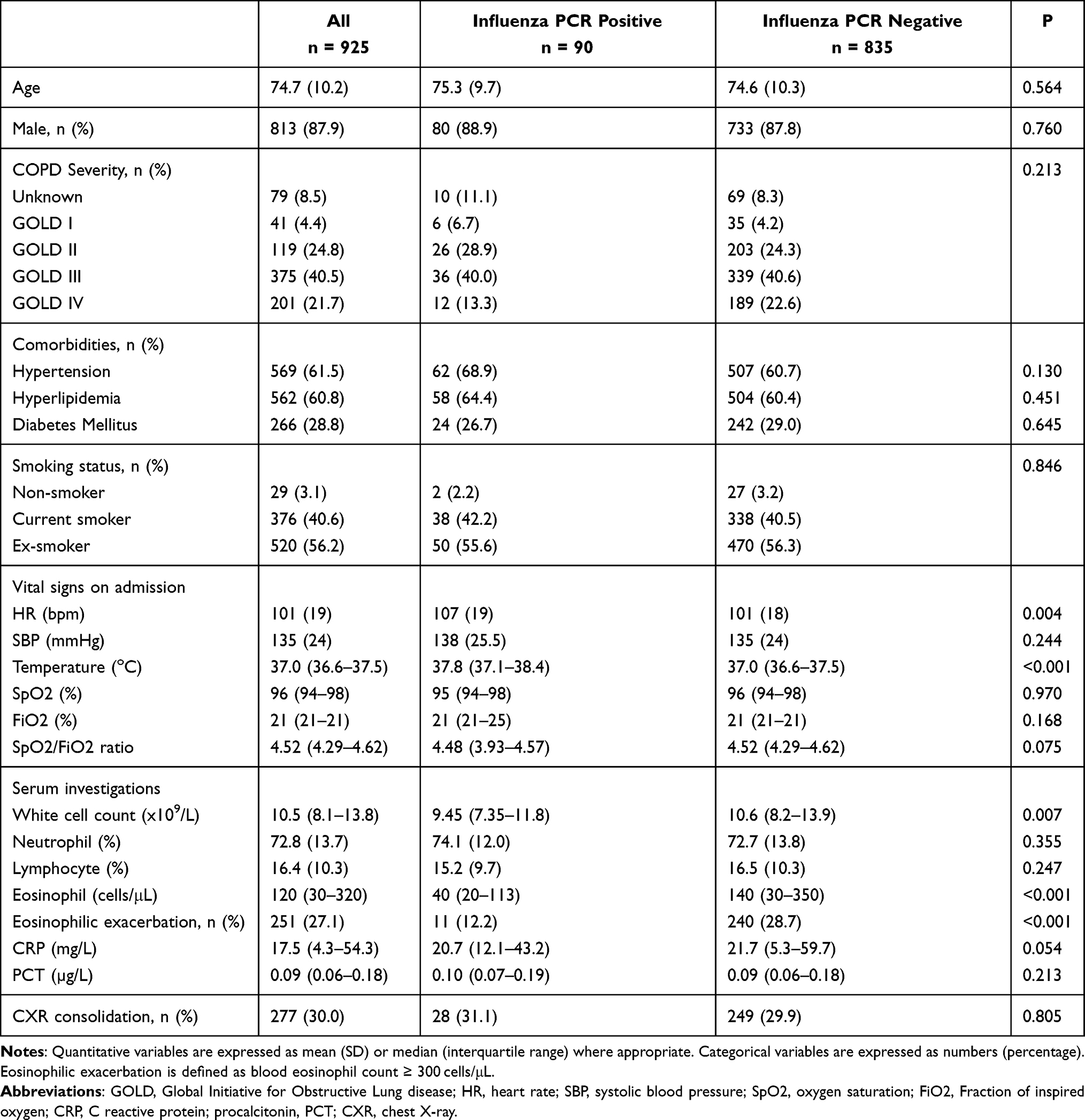 |
Table 1 Comparison of Clinical Variables in AECOPD Patients by Influenza PCR Positivity |
Influenza PCR Positivity
There were 90 (9.7%) Influenza PCR positive cases, of which 68 were Influenza A and 22 were Influenza B. The influenza PCR positive and negative groups had similar baseline characteristics, COPD severity and comorbidities. There were also no differences in blood pressure, oxygen status, neutrophil or lymphocyte counts, CRP, PCT or chest X-ray consolidation. The influenza PCR positive group had higher temperatures (37.8 [37.1–38.4] vs 37.0 [36.6–37.5] °C, p < 0.001), higher heart rates (107 [19] vs 101 [18] bpm, p = 0.004) and lower white cell counts (9.45 [7.35–11.8] vs 10.6 [8.2–13.9] x109/L, p = 0.007). There were also fewer patients with eosinophilic exacerbation in the influenza PCR positive group (11 [12.2%] vs 240 [28.7%], p < 0.001). Table 2 shows the univariate and multivariate analysis of clinical variables associated with influenza PCR positivity. We further divided the total white cell counts (WCC) into quartiles (Q), with the cutoff values as Q1 < 8.1, Q2 = 8.1–10.4, Q3 = 10.5–13.7 and Q4 > 13.7 (x109/L) for the purpose of binary logistic regression analysis. Higher temperature, higher heart rate, white cell count in the lowest quartile (Q1 < 8.1 x109/L) and non-eosinophilic exacerbations predicted influenza PCR positivity on univariate logistic regression and these factors remained significant after multivariate adjustment (temperature adjusted odds ratio [adj OR] 1.324 [1.009–1.737], p = 0.043; heart rate adj OR 1.017 [1.004–1.030], p = 0.011; white cell count Q1 adj OR 3.330 [1.690–6.562], p = 0.001; eosinophilic exacerbations adj OR 0.390 [0.202–0.756], p = 0.005). There was low multicollinearity among the predictors (temperature VIF = 1.067, heart rate VIF = 1.120, white cell count quartile VIF = 1.082, eosinophilic exacerbation VIF = 1.015).
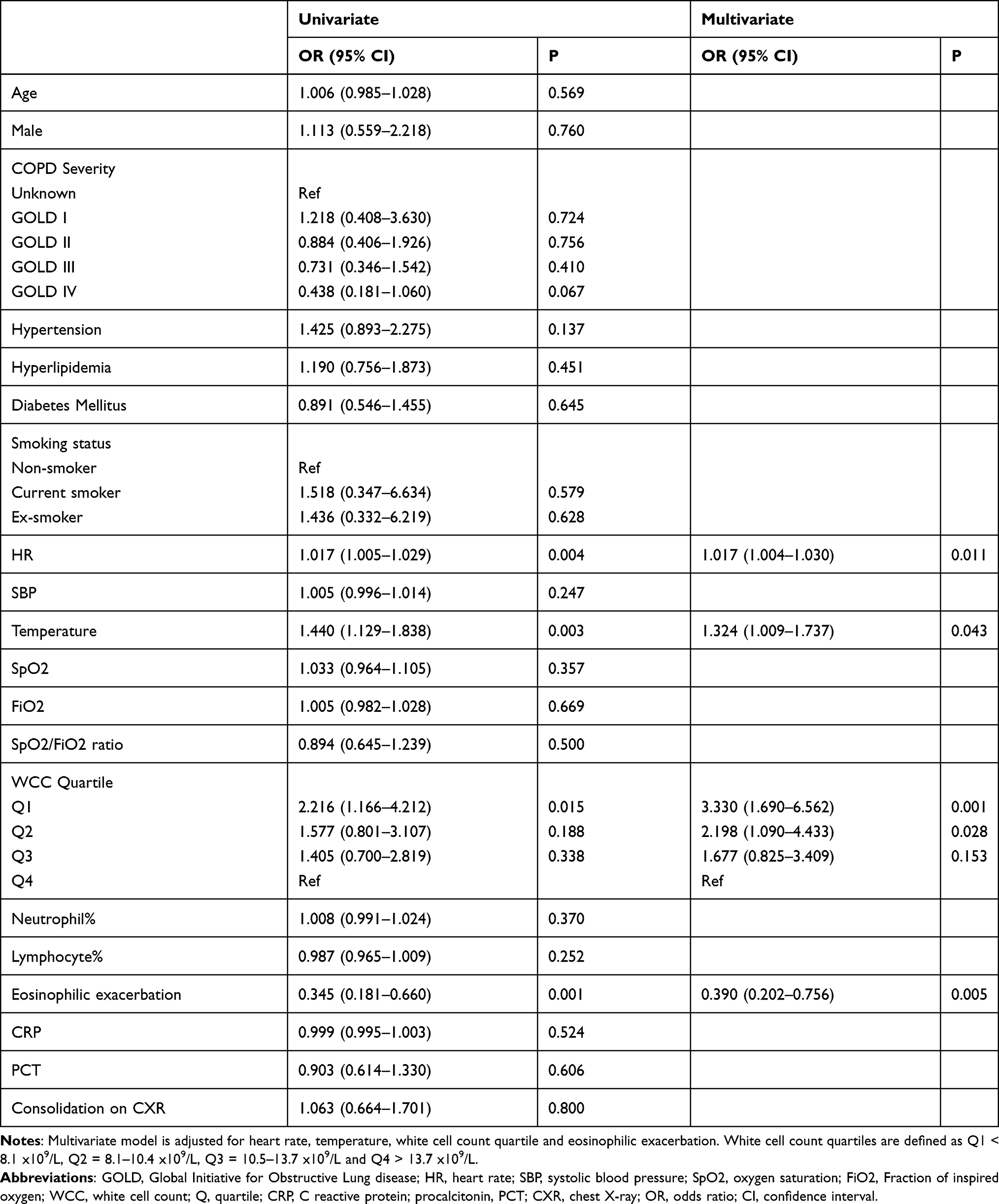 |
Table 2 Predictors of Influenza PCR Positivity in AECOPD Patients Based on Multivariate Logistic Regression Analysis |
Discussion
Respiratory tract infections, particularly of viral origin, are very important causes of AECOPD.11 A meta-analysis of 28 studies by Jafarinejad et al showed that influenza is the second most prevalent respiratory virus identified during AECOPD17 although some reports have identified it as the most common virus isolated in certain settings.18 In our study, influenza PCR positivity was seen in 9.7% of AECOPD patients with influenza PCR sent within 24 hours of hospital presentation, a figure consistent with other Asian studies.19–21
Although many studies have demonstrated the link between higher temperatures and viral associated AECOPD in general,4 very few studies have assessed this relationship specifically in influenza associated AECOPD. Neuzil et al reported that fever was associated with influenza infection in a cohort of vaccinated COPD patients.22 The link between fever and influenza infection in AECOPD is likely related to an exaggerated airway inflammatory response triggered by influenza through a variety of cytokine pathways.23
Similarly, sympathetic nervous system activation, resulting in modulation of proinflammatory cytokines and severe systemic and myocardial inflammation,24,25 has been implicated as the cause of an abnormal cardiovascular response to influenza infection. These effects range from abnormal electrocardiogram findings such as tachycardia,26 atrial fibrillation,24,27 or even life threatening ventricular arrhythmias25 and adverse cardiac events.28 Taken in combination, these findings may explain why tachycardia can be a predictor of influenza infection. Of note, one study reported that during influenza infection, electrocardiogram confirmed tachycardia resolves by Day 2 of infection,26 hence limiting the use of this marker to early presentations only.
Lower white cell counts predicted influenza PCR detection in AECOPD patients. Influenza, being a viral infection, is known to cause leukopenia and lymphopenia.29,30 Patients with influenza infection or undergoing vaccination with a live attenuated virus experience T-cell depression prior to the onset of clinical illness.31 Of note, the T cell depression persisted during the course of the illness but returns to normal with recovery, again highlighting the importance of correlating the white cell count values to the timing of illness.
There is much interest in blood eosinophil count as a biomarker in COPD, particularly in its ability to predict risk of severe exacerbation,32 clinical response to inhaled corticosteroid (ICS) therapy or other anti-eosinophilic therapy,33–35 and outcomes.36–38 However, the role of blood eosinophil count in predicting a specific etiology in AECOPD is not well studied. Jang et al reported that low eosinophil count in the setting of AECOPD suggests viral infection in general.19 Blood eosinophil count of <50 cells/µL was also shown to be associated with infectious AECOPD as defined by viral PCR positivity or CRP levels.39 On the contrary, an eosinophilic COPD exacerbation is characteristic of non-infectious inflammation and responds better to steroid therapy.40 Although the exact mechanism for this association is unknown, it has been recently reported that eosinophils exert an immunomodulatory function in the airway epithelium against influenza A.41 It is therefore possible that patients with eosinophilic exacerbations are able to mount a stronger protective response against influenza, and hence be PCR negative for influenza. The results of our study add on to existing literature demonstrating an inverse relationship between eosinophils and influenza PCR positivity, although further research is needed to better study this association.
Despite systemic inflammation being a likely contributor to our findings, CRP and PCT did not emerge as significant predictors of influenza PCR positivity. This is consistent with many prior studies demonstrating CRP and PCT as poor predictors of virus detection in AECOPD.18,42 While viruses are known to generate an intense host inflammatory response in AECOPD patients which serum biomarkers such as CRP are indicative of,43 CRP can also be raised in stable COPD patients,44,45 which may confound any associations drawn.
Identification of influenza in AECOPD patients is of clinical relevance given the availability of effective antiviral therapy. In practice however, clinical features alone do not reliably identify influenza-infected AECOPD patients as symptoms poorly distinguish influenza from non-influenza illness amongst patients with chronic lung diseases.22 Major societal guidelines currently do not offer definite recommendations on when or in whom to perform influenza PCR testing. Routine and indiscriminate PCR testing of all AECOPD cases is likely to be of low yield and poor cost effectiveness given an influenza PCR positivity rate of under 10% in our cohort. We identified higher temperature, higher heart rate, lower white cell count, and non-eosinophilic exacerbation (<300 cells/µL) as independent predictors of influenza PCR positivity in AECOPD. Although several of these factors may be seen in general respiratory viral infections, our study is one of the few in the literature to establish an independent relationship between them and influenza specifically. These predictors, especially in combination, may have a role in guiding the clinician in identifying AECOPD patients in whom influenza PCR testing is appropriate. This will ideally enable early diagnosis and treatment with antivirals, which has been shown to reduce the severity and duration of AECOPD8,9 and potentially improve health-related quality of life.46 In addition, these predictors are of interest in infection control as they can potentially be used to identify AECOPD patients with suspected influenza infection for initial isolation and air-borne precautions to prevent in-hospital spread47 while awaiting PCR confirmation.
This study has several limitations. Despite being one of the largest studies specifically assessing influenza PCR positivity in AECOPD patients, our single center study in a predominantly Asian population may not be generalizable to other patient populations. Unlike temperate countries, tropical Singapore lacks a defined influenza season, but local epidemiological data has shown a bimodal increase in influenza incidence observed between April to July and between November to January.48 To overcome this seasonal variation, our study period spanned 1.5 years in order to include as many patients possible from the periods with high influenza incidence. The retrospective nature of the study meant that it was highly reliant on accurate and comprehensive electronic medical records. As such, we did not have reliable data on prior influenza vaccination as many patients could have had influenza vaccinations administered at primary care settings or other institutions which we did not have medical records for. We could not control for variables such as time between onset of clinical illness and hospital presentation, or the exact timing of the influenza PCR and other investigations performed upon hospital admission. Finally, in the absence of a reliable alternative marker, we assumed that the presence of influenza PCR positivity indicated active influenza infection, although it has been shown that PCR may detect minute quantities of viral DNA or RNA which may not indicate the presence of live virus.49
Conclusion
While influenza is an important cause of AECOPD, it is not commonly detected amongst AECOPD patients in our cohort. Clinical features of higher temperature, higher heart rate, a lower total white cell count and non-eosinophilic exacerbation are predictors of influenza PCR positivity. These may guide appropriate influenza PCR testing and early treatment in AECOPD patients for better outcomes.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; CI, confidence interval; CRP, C reactive protein; CXR, chest X-ray; DSRB, Domain Specific Review Board; FiO2, Fraction of inspired oxygen; GOLD, Global Initiatives for Chronic Obstructive Lung Disease; HR, heart rate; OR, odds ratio; PCR, polymerase chain reaction; PCT, Procalcitonin; Q, quartile; SBP, systolic blood pressure; SD, standard deviation; SpO2, oxygen saturation; VIF, variable inflation factor.
Data Sharing Statement
The data analyzed is available upon reasonable request.
Acknowledgments
The authors would like to acknowledge the work of Dr Tan Joo Hor for his contributions to the data collection. The abstract of this paper was presented at the 2020 ERS International Congress, in session “Respiratory viruses in the ‘pre COVID-19’ era”. The poster’s abstract was published in “Poster Abstracts” in European Respiratory Journal 2020; 56: Suppl. 64, 2377: https://imsva91-ctp.trendmicro.com:443/wis/clicktime/v1/query?url=https%3a%2f%2ferj.ersjournals.com%2fcontent%2f56%2fsuppl%5f64%2f2377andumid=662F7BB1-CC01-3605-A6A0-56ABECDA2304andauth=6e3fe59570831a389716849e93b5d483c90c3fe4-1769fe133454a776c20fda9365c7d77c8ca88fdb
Disclosure
The authors do not have any relevant conflict of interests to declare. The authors did not receive funding for this study.
References
1. Kim V, Aaron SD. What is a COPD exacerbation? Current definitions, pitfalls, challenges and opportunities for improvement. Eur Respir J. 2018;52(5):1801261. doi:10.1183/13993003.01261-2018
2. MacIntyre N, Huang YC. Acute exacerbations and respiratory failure in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):530–535. doi:10.1513/pats.200707-088ET
3. Varkey JB, Varkey B. Viral infections in patients with chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2008;14(2):89–94. doi:10.1097/MCP.0b013e3282f4a99f
4. Mohan A, Chandra S, Agarwal D, et al. Prevalence of viral infection detected by PCR and RT-PCR in patients with acute exacerbation of COPD: a systematic review. Respirology. 2010;15(3):536–542. doi:10.1111/j.1440-1843.2010.01722.x
5. Mallia P, Johnston SL. Influenza infection and COPD. Int J Chron Obstruct Pulmon Dis. 2007;2(1):55–64. doi:10.2147/copd.2007.2.1.55
6. Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(9):1618–1623. doi:10.1164/ajrccm.164.9.2105011
7. Mallia P, Footitt J, Sotero R, et al. Rhinovirus infection induces degradation of antimicrobial peptides and secondary bacterial infection in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(11):1117–1124. doi:10.1164/rccm.201205-0806OC
8. Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med. 2003;163(14):1667–1672. doi:10.1001/archinte.163.14.1667
9. Lin J-T, Yu X-Z, Cui D-J. A multicentre, randomized, controlled trial of oseltamivir in the treatment of influenza in a high-risk Chinese population. Curr Med Res Opin. 2006;22(1):75–82. doi:10.1185/030079906X80297
10. Wesseling G. Occasional review: influenza in COPD: pathogenesis, prevention, and treatment. Int J Chron Obstruct Pulmon Dis. 2007;2(1):5–10. doi:10.2147/copd.2007.2.1.5
11. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 report); Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
12. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3):1600791. doi:10.1183/13993003.00791-2016
13. National Clinical Guideline Centre (UK). Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London: Royal College of Physicians (UK); 2010. Available from: http://www.ncbi.nlm.nih.gov/books/NBK65039/.
14. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
15. Negewo NA, McDonald VM, Baines KJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. COPD. 2016;11(1):1495–1504. doi:10.2147/COPD.S100338
16. Jabarkhil A, Moberg M, Janner J, et al. Elevated blood eosinophils in acute COPD exacerbations: better short- and long-term prognosis. Eur Clin Respir J. 2020;7(1):1757274. doi:10.1080/20018525.2020.1757274
17. Jafarinejad H, Moghoofei M, Mostafaei S, Salimian J, Azimzadeh Jamalkandi S, Ahmadi A. Worldwide prevalence of viral infection in AECOPD patients: a meta-analysis. Microb Pathog. 2017;113:190–196. doi:10.1016/j.micpath.2017.10.021
18. Kawamatawong T, Apiwattanaporn A, Siricharoonwong W. Serum inflammatory biomarkers and clinical outcomes of COPD exacerbation caused by different pathogens. Int J Chron Obstruct Pulmon Dis. 2017;12:1625–1630. doi:10.2147/COPD.S132132
19. Jang JG, Ahn JH, Jin HJ. Incidence and prognostic factors of respiratory viral infections in severe acute exacerbation of chronic obstructive pulmonary disease. COPD. 2021;16:1265–1273. doi:10.2147/COPD.S306916
20. Ko FWS, Ip M, Chan PKS, et al. Viral etiology of acute exacerbations of COPD in Hong Kong. Chest. 2007;132(3):900–908. doi:10.1378/chest.07-0530
21. Choi J, Oh JY, Lee YS, et al. Bacterial and viral identification rate in acute exacerbation of chronic obstructive pulmonary disease in Korea. Yonsei Med J. 2019;60(2):216–222. doi:10.3349/ymj.2019.60.2.216
22. Neuzil KM, O’Connor TZ, Gorse GJ, Nichol KL. Recognizing influenza in older patients with chronic obstructive pulmonary disease who have received influenza vaccine. Clin Infect Dis. 2003;36(2):169–174. doi:10.1086/345668
23. Tu YH, Guo Y, Ji S, Shen JL, Fei GH. The Influenza A Virus H3N2 Triggers the Hypersusceptibility of Airway Inflammatory Response via Activating the lncRNA TUG1/miR-145-5p/NF-κB Pathway in COPD. Front Pharmacol. 2021;12:604590. doi:10.3389/fphar.2021.604590
24. Verma N, Knight BP. The flu and atrial fibrillation: nothing to sneeze at. Heart Rhythm. 2016;13(6):1195–1196. doi:10.1016/j.hrthm.2016.01.025
25. Madjid M, Connolly AT, Nabutovsky Y, Safavi-Naeini P, Razavi M, Miller CC. Effect of high influenza activity on risk of ventricular arrhythmias requiring therapy in patients with implantable cardiac defibrillators and cardiac resynchronization therapy defibrillators. Am J Cardiol. 2019;124(1):44–50. doi:10.1016/j.amjcard.2019.04.011
26. Ison MG, Campbell V, Rembold C, Dent J, Hayden FG. Cardiac findings during uncomplicated acute influenza in ambulatory adults. Clin Infect Dis. 2005;40(3):415–422. doi:10.1086/427282
27. Chang TY, Chao TF, Liu CJ, et al. The association between influenza infection, vaccination, and atrial fibrillation: a nationwide case-control study. Heart Rhythm. 2016;13(6):1189–1194. doi:10.1016/j.hrthm.2016.01.026
28. Gopal R, Marinelli MA, Alcorn JF. Immune mechanisms in cardiovascular diseases associated with viral infection. Front Immunol. 2020;11:570681. doi:10.3389/fimmu.2020.570681
29. Lee IK, Liu JW, Wang L, Yang KD, Li CC, Eng HL. 2009 pandemic influenza A (H1N1): clinical and laboratory characteristics in pediatric and adult patients and in patients with pulmonary involvement. Influenza Other Respir Viruses. 2012;6(6):e152–161. doi:10.1111/j.1750-2659.2012.00410.x
30. Cate TR. Clinical manifestations and consequences of influenza. Am J Med. 1987;82(6A):15–19. doi:10.1016/0002-9343(87)90555-9
31. Scheinberg M, Blacklow NR, Goldstein AL, Parrino TA, Rose FB, Cathcart ES. Influenza: response of T-cell lymphopenia to thymosin. N Engl J Med. 1976;294(22):1208–1211. doi:10.1056/NEJM197605272942204
32. Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen general population study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
33. Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117–126. doi:10.1016/S2213-2600(18)30006-7
34. Cheng SL. Blood eosinophils and inhaled corticosteroids in patients with COPD: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:2775–2784. doi:10.2147/COPD.S175017
35. Siddiqui SH, Pavord ID, Barnes NC, et al. Blood eosinophils: a biomarker of COPD exacerbation reduction with inhaled corticosteroids. Int J Chron Obstruct Pulmon Dis. 2018;13:3669–3676. doi:10.2147/COPD.S179425
36. Holland M, Alkhalil M, Chandromouli S, Janjua A, Babores M. Eosinopenia as a marker of mortality and length of stay in patients admitted with exacerbations of chronic obstructive pulmonary disease. Respirology. 2010;15(1):165–167. doi:10.1111/j.1440-1843.2009.01651.x
37. Wu HX, Zhuo KQ, Cheng DY. Peripheral blood eosinophil as a biomarker in outcomes of acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:3003–3015. doi:10.2147/COPD.S226783
38. Couillard S, Larivée P, Courteau J, Vanasse A. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest. 2017;151(2):366–373. doi:10.1016/j.chest.2016.10.003
39. MacDonald MI, Osadnik CR, Bulfin L, et al. Low and high blood eosinophil counts as biomarkers in hospitalized acute exacerbations of COPD. Chest. 2019;156(1):92–100. doi:10.1016/j.chest.2019.02.406
40. Wu CW, Lan CC, Hsieh PC, Tzeng IS, Wu YK. Role of peripheral eosinophilia in acute exacerbation of chronic obstructive pulmonary disease. World J Clin Cases. 2020;8(13):2727–2737. doi:10.12998/wjcc.v8.i13.2727
41. Tiwary M, Rooney RJ, Liedmann S, LeMessurier KS, Samarasinghe AE. Eosinophil Responses at the Airway Epithelial Barrier during the Early Phase of Influenza A Virus Infection in C57BL/6 Mice. Cells. 2021;10(3):509. doi:10.3390/cells10030509
42. Kherad O, Kaiser L, Bridevaux PO, et al. Upper-respiratory viral infection, biomarkers, and COPD exacerbations. Chest. 2010;138(4):896–904. doi:10.1378/chest.09-2225
43. Rohde G, Borg I, Wiethege A, et al. Inflammatory Response in Acute Viral Exacerbations of COPD. Infection. 2008;36(5):427–433. doi:10.1007/s15010-008-7327-5
44. Torres JP, Cordoba-Lanus E, López-Aguilar C, et al. C-reactive protein levels and clinically important predictive outcomes in stable COPD patients. Eur Respir J. 2006;27(5):902–907. doi:10.1183/09031936.06.00109605
45. Dahl M, Vestbo J, Lange P, Bojesen SE, Tybjaerg-Hansen A, Nordestgaard BG. C-reactive protein as a predictor of prognosis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;175(3):250–255. doi:10.1164/rccm.200605-713OC
46. Seemungal T, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5):1418–1422. doi:10.1164/ajrccm.157.5.9709032
47. Stuart RL, Cheng AC, Marshall CL, Ferguson JK. ASID (HICSIG) position statement: infection control guidelines for patients with influenza-like illnesses, including pandemic (H1N1) influenza 2009, in Australian health care facilities. Med J Aust. 2009;191(8):667. doi:10.5694/j.1326-5377.2009.tb03373.x
48. Chow A, Ma S, Ling AE, Chew SK. Influenza-associated Deaths in Tropical Singapore. Emerg Infect Dis. 2006;12(1):114–121. doi:10.3201/eid1201.050826
49. Beasley V, Joshi PV, Singanayagam A, Molyneaux PL, Johnston SL, Mallia P. Lung microbiology and exacerbations in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:555–569. doi:10.2147/COPD.S28286
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.