")
Back to Journals » International Journal of General Medicine » Volume 14
Predictors of Death from Complicated Severe Acute Malnutrition in East Ethiopia: Survival Analysis
Authors Oumer A , Mesfin L, Tesfahun E , Ale A
Received 6 September 2021
Accepted for publication 9 November 2021
Published 24 November 2021 Volume 2021:14 Pages 8763—8773
DOI https://doi.org/10.2147/IJGM.S337348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdu Oumer,1 Leul Mesfin,1 Esubalew Tesfahun,2 Ahmed Ale3
1Department of Public Health, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia; 2Department of Public Health, College of Medicine and Health Science, Debre Birhan, University, Debre Birhan, Ethiopia; 3School of Medicine, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia
Correspondence: Abdu Oumer
Department of Public Health, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia
Email [email protected]
Background: Severe acute malnutrition (SAM) is still the leading cause of global child morbidity and mortality, with a greater burden in sub-Saharan Africa. A facility-based treatment of SAM demands critical care for improved outcomes and survival of children. However, there is a need to understand predictors for time to death among SAM children for effective interventions.
Objective: To assess the predictors of death from complicated severe acute malnutrition among admitted children treated in East Ethiopia.
Methods: A 31-month retrospective cohort study was conducted among a total of 665 under-five children admitted with complicated SAM in Dilchora hospital, eastern Ethiopia. The data was extracted from the patient register and medical charts using the kobo tool. The life table, survival, and hazard curves were plotted. Kaplan–Meier with Log rank tests was used to estimate and compare the mean survival time. The bivariable and multivariable Cox proportional hazards models were used to identify predictors of time to death. Crude and adjusted hazard ratios with 95% confidence intervals and p-values were reported.
Results: A total of 665 full medical charts were reviewed with a total of 60 (9%; 95% CI: 6.8– 11.2%) deaths were observed, where most of the deaths occurred during the first two weeks of admission, while 74 (11%) and 449 (68%) were cured and recovered (stabilized and transferred to outpatient), respectively. Admitted children having good appetite (AHR=0.15; 95% CI: 0.64– 0.33), pneumonia (AHR=2.46, 95% CI: 1.436, 4.22), diarrhea (AHR=2.16, 95% CI: 1.16, 4.06), tuberculosis (AHR=2.86, 95% CI: 1.08, 7.63) and having a nasogastric tube inserted (AHR=2.33, 95% CI: 1.15, 4.72) were significant predictors of time to death among SAM children.
Conclusion: There is unacceptably high under-five mortality due to SAM, which is predicted by co-morbidities (pneumonia, diarrhea, and tuberculosis), with medical complications and nasogastric tubes.
Keywords: survival pattern, predictors, time to death, severe acute malnutrition, hospitals
Introduction
Acute malnutrition is characterized by a recent failure to receive adequate nutrition due to episodes of diarrhea and other acute illnesses.1,2 It can be classified as moderate acute malnutrition (MAM) and severe acute malnutrition (SAM) using weight for height (WFH) or mid-upper arm circumference (MUAC) cutoff points.3,4 SAM is diagnosed with low MUAC (MUAC <11.5 cm) and/or a WFH Z-score (less than −3). It is the most extreme and visible form of undernutrition that is characterized by profound wasting or edema, loss of appetite, comorbidities, and complications. It requires timely and appropriate management for the child to survive.1,3,5
Globally, an estimated 49 million (7.3%) children had acute malnutrition, with 16 million children being victims of SAM, accounting for estimated three million child deaths. The continent of Africa bears 28% of the global malnutrition burden.6 Estimated 3 million child deaths are attributable to SAM, with over 50% of child deaths occurring in developing countries attributable to undernutrition, in general.7 A forecast in 2014 showed that estimated 28.8 million children were victims of SAM and projected to decrease to 21.7 million by 2030. Despite a decline in the burden, additional 8 million new cases occur in sub-Saharan Africa each year.8 In sub-Saharan Africa, SAM affects about 3% of under-five children, with more than 400,000 child deaths each year.9 In addition, estimated 6.9 million child deaths are attributable to malnutrition in low- and middle-income countries.10
In Ethiopia, where the under-five child mortality rate is high (57 child deaths per 1000), malnutrition is a basic underlying cause, accounting for an estimated 57% of child mortality.11 Malnutrition, primarily due to SAM, costs approximately 16.5% of the national GDP.12 An estimated 9–40% of children are affected by acute malnutrition.13–18 SAM is the third leading cause of mortality, accounting for 8.1% of under-five deaths.19 It is also estimated that 4.8 million children need emergency nutrition support in 2019, which could aggravate the situation in Ethiopia.20
Children with complicated SAM need to be treated as inpatients to manage complications and improve child survival, since severe infections including pneumonia, diarrhea, sepsis, or HIV have a higher case fatality of up to 40%. Children with complicated SAM have a high ongoing risk of mortality throughout.21 The United Nations International Children’s Education Fund (UNICEF) reported that in Ethiopia, there are 152,413 cases of SAM being treated from January to May 2021.22 SAM could threaten the futures of millions of children worldwide.23,24 In Dire Dawa, an estimated 4.2% of children are affected by SAM, which is above the national average of 3%.13 In addition, being on the border with the neighboring countries in the horn, sporadic conflicts, and population displacement make the area more prone to the adverse consequences of SAM.
The current strategy for Community-based Management of Acute Malnutrition (CMAM) is a focused and holistic approach for better SAM case management. It aims to increase the capacity to manage SAM children properly for a better treatment outcome. The proper implementation of SAM management has the potential to reduce under-five mortality from 55% to under 20% in Ethiopia.1,40 However, a substantial number of deaths; 29%,14 8.4%,25 14.5%26 and 5.8%27 have been observed in Ethiopia, which is mainly related to facility readiness, staff capacity, and inter-regional differences related to clinical characteristics and severity of malnutrition.28
Inpatient therapeutic feeding units are faced with a lot of challenges in handling cases of SAM. Some of the challenges are limited in-patient capacity, lack of enough skilled staff in the hospitals, late presentation of children, the high default rate among children, and the serious risk of cross infections for immune-suppressed children, which totally increases the mortality rate.29 A mortality rate of below 10% is considered acceptable in humanitarian situations.30 However, these parameters are still not achieved in many of the developing countries due to many causes.3
In Ethiopia, majorities of children with SAM present to therapeutic feeding centers, but present with many medical complications, and many children are dying anyway.31 However, the major predicting factors affecting the time to death are not well understood, particularly in Dire Dawa, which needs to be understood for targeted intervention for improved child survival and treatment success.38 So, the purpose of this study was to identify the predictors of time to death from complicated SAM among under-five children managed at stabilization centers in Dire Dawa.
Materials and methods
Study area and design
This retrospective cohort study was conducted in Dire Dawa city administration in Eastern Ethiopia. In the city, there were two public hospitals providing care for complicated SAM patients. However, due to the current Covid-19 pandemic, one hospital providing SAM care was changed to a Covid-19 treatment center. Thus, the current study was conducted in Dilchora Hospital’s SAM unit (stabilization center), where the majority of the SAM cases are treated. Dire Dawa is one of the two city administrations in Ethiopia which is located 515 km away from Addis Ababa, the capital city. The city has an estimated total population of more than 506,936 as of 2019/20, with the majority of residents living in the rural part. There are two governmental hospitals, four private hospitals, five higher clinics, twelve medium clinics (private), 15 health centers, and 34 health posts with 100% health service coverage.32
Dilchora hospital gives inpatient management for complicated SAM children (13 beds) in a stabilization center, in accordance with the national SAM management guideline. The data was retrieved from records from July 1, 2020, to August 30, 2020.
Study population and eligibility criteria
The results of this study are applicable to all children aged 0–59 months with complicated SAM admitted to the Dilchora Hospital stabilization center. All eligible records of 0–59 months’ children with SAM admitted to the center from September 2017 to March 2020 were from the study population (as this may show the most recent burden of the problem). Records of SAM children with missing treatment outcomes, admission, and discharge date were not included in the study as these are the primary outcomes of the study to be addressed.
Sample size determination
The minimum sample size for detecting the predictors of time to death from complicated SAM was calculated using Stata version 14 (Stata Corp., STATA 14.0 for window) for sample, and power calculation module. The sample size for comparing the survival Cox model and comparing slope to the reference was used. In addition, samples were calculated for each predictor, and the maximum calculated sample was taken. By taking anemia as a predictor of time to death (AHR = 1.36), the ratio of exposed to non-exposed as 1, the probability of death (0.29),31 a significance level (0.05), and power (80%), the minimum sample size to identify predictors of time to death among SAM children became 666.
Sampling technique
Simple random sampling using the serial numbers of SAM children in the SAM registry was used to generate a table of random numbers. Then, the unique medical record number corresponding to the selected random serial number is identified. Then, using the unique medical record number, the medical charts of randomly selected children were retrieved from the card room, and data was collected.
Data collection method
A cross-checked data abstraction format prepared in line with the SAM registry and the medical charts of children was used to collect data. The data was collected from the medical records and the SAM treatment registry through cross-validation. Graduate nurses and health officers were used for collecting the data.
Data quality control
To assure data quality, the checklist was cross-checked with the SAM register and medical charts. Data collectors were trained for one day, on how to extract the data from the patient registry. During training, data collectors exercised the data collection on at least five medical charts of children with the supervision of the researchers. Daily checkups and feedback were given by the investigators and supervisors on the appropriateness, completeness, and consistency of the collected data by taking a random sample of the collected data. The data was entered into the Kobo tool for controlled and quality data collection.
Variables of the study
The dependent variable was time to death from SAM among children. Meanwhile, the independent variables were demographic characteristics (age, sex of the child, place of residence), clinical conditions (vomiting, dehydration, loss of appetite, and hypothermia), presence of nutritional edema, co-morbidities (pneumonia, HIV status, diarrhea, anemia, malaria, tuberculosis, and hypothermia), routine medication intake (intravenous (IV) fluid intake, IV antibiotic treatment, blood transfusion, folic acid, vitamin A supplementation, deworming, and presence of nasogastric tube), and level of anthropometric deficits at admission.
Operational definitions
In this study, cure from SAM was achieved when the SAM child reached the discharge criteria; weight-for-height/length is ≥–2 Z-scores and they have had no edema for at least 2 weeks, or MUAC is ≥12.5 cm, and they have had no edema for at least 2 weeks without any acute medical complications. However, recovered (stabilized) is defined as when the child is treated for acute medical complications at a stabilization center and transferred to OTP (not cured yet) for continuous SAM treatment.30,33 Censored observations were defined as those SAM children who were defaulted, transferred, disappeared, recovered, or non-responded in which the primary outcome of interest (death) was not observed. Anemia was defined with a hemoglobin level below 11 gm/dl (hematocrit level less than 33%) at admission,33 while hypothermia is defined as when the body temperature is below 35.5°C.
Data processing and analysis
The collected data through the Kobo tool was exported to SPSS statistical software version 20 for data cleaning and analysis. The data were cleaned and checked for outliers and inconsistencies ahead of the statistical analysis. Frequency, percentage, mean, median, and standard deviation were used to present the data. The Kolmogorov–Smirnov test was done to check the distribution of ratio scale variables. Graphs and tables were presented. The life tables and survival curve were used to display the cumulative survival and survival function with different patient characteristics. The Kaplan–Meier test with a Log rank test was used to compare the mean or median survival time among different categories. The Cox-proportional hazard assumption was checked in Stata/SE 14.0 both graphically and statistically. After checking the Cox proportional hazard assumption, both bivariable and multivariable Cox proportional hazard regression analysis with crude and adjusted hazard ratio (CHR and AHR) and 95% Confidence interval (95% CI) were reported. The Cox proportional hazard assumption was tested using a global test in Stata Version 14.0. To test the proportional hazard estimate over time, both graphical (survival and Kaplan–Meier by categorical variables) and statistical (global test) methods were used. Predictor variables with a p-value below 0.2 in bivariable Cox regression were candidates for the multivariable Cox regression analysis. Predictor variables with a P-value below 5% was used to declare as statistically significant predictors of time to death from SAM.
Ethical considerations
An ethical support letter was obtained from the Dire Dawa University, College of Medicine and Health Science research and ethics review committee. The support letters were subsequently taken to the city administration health bureau and the hospital. Written informed consent was taken from the hospital administration on behalf of the clients that the information collected would be kept confidential and be used only for the proposed study. Specific personal identifiers of children were not collected to maintain the client’s private health issues like HIV status.
Results
Socio-demographic characteristics of SAM children
In this study, a total of 665 full medical records of children were reviewed, where, more than half, 363 (54.6%) were males. A total of 210 (31.6%) SAM children were aged below twelve months, and a mean age of 20 months (±15 months). Regarding residence, the majority of SAM children treated in the SAM unit, 385 (57.9%), were from rural areas.
Medical characteristics of admitted children
Concerning the admission history of children, about 426 (64.1%) and 217 (32.6%) were diagnosed with marasmus and kwashiorkor, respectively, being the common clinical forms of SAM, while only 22 (3.3%) of SAM children had Marasmic-Kwashiorkor at admission. About 417 (62.7%), 401 (60.3%), and 310 (46.6%) children were affected by vomiting, diarrhea, and dehydration, respectively. On the other hand, only 10 (1.5%) and 7 (1.1%) were victims of hyperthermia and hypothermia, respectively. About 651 (97.9%), 110 (16.5%), and 148 (22.3%) of admitted SAM children were given an intravenous antibiotic, a nasogastric tube (NG tube), and intravenous infusions, respectively. Meanwhile, a total of 91 (13.7%) of children received a blood transfusion during their hospital stay for treatment of anemia (Table 1).
 |
Table 1 Co-Morbidity and Medical Conditions of Children Admitted to Stabilization Center in Dire Dawa, from 2017 to 2020 (n = 665) |
Survival patterns of SAM children
Concerning the treatment outcomes of SAM children, the majority of children (67.5%) were recovered. Also, about 11.1%, 2%, and 10.4% of SAM children were cured, self-discharged without clinical improvement, and defaulted in the course of SAM treatment. A total of 60 (9%: 95% CI: 6.8–11.2%) deaths were observed among SAM children during treatment at a stabilization center within the hospital (Figure 1). The overall cumulative incidence density for mortality was found to be 0.022.
 |
Figure 1 Treatment outcomes of SAM children treated in stabilization center, Eastern Ethiopia. |
A life table, survival chart, and Kaplan Meier tests were done to explore and understand the survival patterns of SAM children. A total of 60 (9%; 95% CI: 6.8%–11.2%) deaths were observed among admitted SAM children in the hospital. The vast majority of them, 78.3% of children, died within ten days of being admitted to a hospital where medical complications and mismanagement are common (Table 2 and Figure 2). The median survival time of SAM children was 10 days, with a minimum and maximum hospital stay of 1 and 47 days, respectively. The survival patterns of children showed a significant decline and increased hazard of death during the early first weeks of admissions. Regarding the duration of the hospital stay, the average length of stay in the hospital was 12 days (SD ± 7.35 days).
 |
Table 2 Life Table Showing the Survival and Hazards of SAM Children Treated in Stabilization Center, in Dire Dawa from 2017 to 2020, Ethiopia |
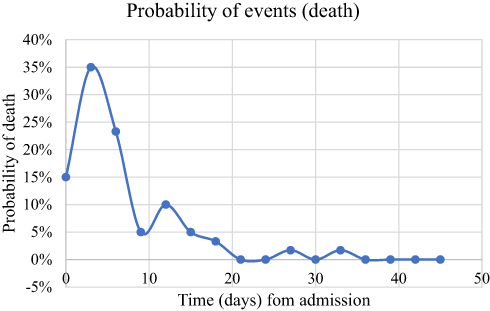 |
Figure 2 Hazard (1-survival) curve for admitted SAM children in stabilization center: from admission to outcome (death). |
Those SAM children with a failed appetite at admission had a significantly lower mean survival time (26.9 days) as compared to those with a passed appetite test (43.6 days) (p-value of log-rank = 0.0001). In addition, children with the diagnosis of tuberculosis had a significantly lower mean survival time as compared to their counterparts. Children with pneumonia and diarrhea at admission had a significantly shorter mean survival time than the others. Children who received routine medications (deworming and NG tube) had significantly shorter mean survival times than their counterparts.
Predictors of time to death among under-five children with SAM
Bivariable Cox proportional hazard regression was done to identify the potential predictors of time to death from complicated SAM among children. The risks of death were found to be lower among those over the age of two, males, and children of city dwellers. Those SAM children who were diagnosed with dehydration (CHR=2.0; 95% CI: 1.18–3.38) and pneumonia (CHR=2.68: 95% CI: 1.58–4.56) had a significantly increased risk of death from SAM. In addition, children with TB in the course of SAM treatment (CHR=2.85; 95% CI: 1.14–7.14) and those on IV fluid treatment (CHR=3.23; 95% CI: 1.94–5.36) had a significantly three-fold increased hazard of death. Children who were unable to swallow food and those who had the NGT implanted had a 13-fold increased risk of death (CHR=13.02; 95% CI: 7.54–22.48). Meanwhile, children who got vitamin supplements, deworming, and IV antibiotics had a lower hazard of death (Table 3).
 |
Table 3 Bivariable Cox Proportional Hazard Regression Model for Predictors of Death from SAM in Eastern Ethiopia |
The predictors of time to death from SAM were assessed using multivariable Cox proportional hazard regression. Failed appetite, comorbidities (diarrhea, pneumonia and tuberculosis), not taking deworming, and the presence of an NG tube were important predictors of time to death among admitted complicated SAM children. Children who had a good appetite (AHR=0.15; 95% CI: 0.64–0.34) and those who took deworming tablets (AHR=0.36; 95% CI: 0.20–0.64) had lower risks of death due to SAM. While children with pneumonia (AHR=2.43; 95% CI: 1.42–4.16) and diarrhea (AHR=1.96; 95% CI: 1.08–3.56), respectively, had a 2.4- and 2-fold increased risk of death from SAM, respectively. Furthermore, children with tuberculosis (AHR=2.86; 95% CI: 1.08–7.63) and those with nasogastric tubes inserted (AHR=2.32; 95% CI: 0.15–4.72) had a higher risk of death than their peers (Table 4).
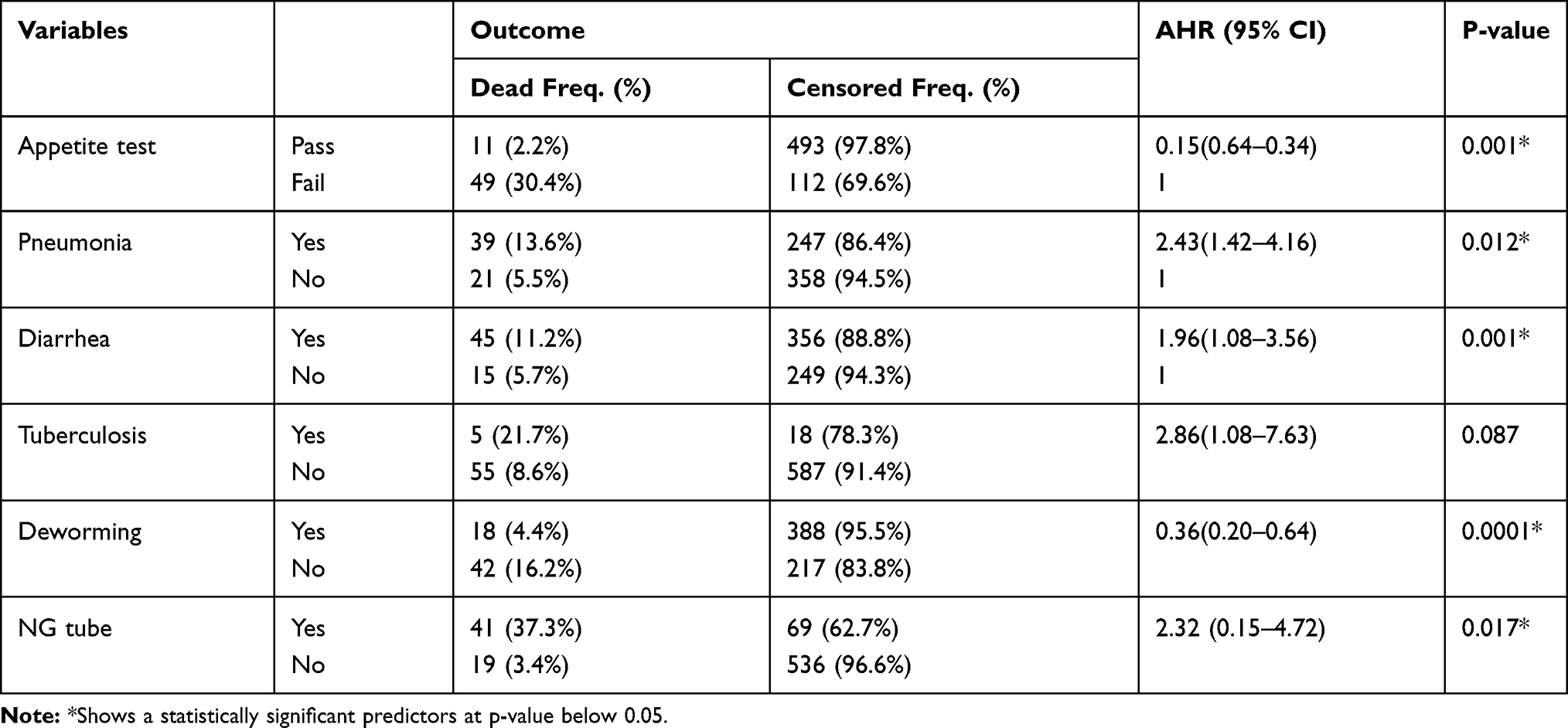 |
Table 4 Multivariable Cox-Proportional Hazard Regression Model for Predictors of Death from SAM |
Discussions
The purpose of this study was to identify the predictors of time to death from SAM among children treated in a stabilization center within the hospital, in Ethiopia. The findings of this study showed that a significantly higher number of deaths (9%: 95% CI: 6.8%–11.2%) were observed among admitted children. Despite the fact that Ethiopia is implementing a standard management protocol for complicated SAM management for children, the mortality is found to be high. Other similar studies also reported 7.6% in eastern Ethiopia,34 and the Wolaita Zone (8.8%),35 while it was higher than the result from North Ethiopia (3.8%).36 However, a higher mortality rate was observed in Yaoundé, Cameroon (15%),5 Zambia (46%),37 northern Ethiopia (29%) and southwest Ethiopia (14.5).26
The SPHERE minimum standard for humanitarian response states that the death rate should be below 10% as a target.30 However, as the situation is not in an emergency setting, but in a relatively stable setting, a higher mortality incidence that needs due attention is found. This may be related to the frequent occurrence of medical complications, such as diarrhea,38 pneumonia, and others impairing nutritional recovery,3,39 and prolong hospitalization, which negatively affects nutrient intake. In addition, since the cure is expected at outpatient therapeutic feeding, where children are transferred from hospitals, the current mortality rate may be increased. That means a significant number of children are dying in the early phase of hospital admission, which should be addressed for improved health care and effective treatment.40
In this study, the mean survival time was 40.43 days with most of the deaths occurring within the first two weeks of admission to the hospital. This might be due to the fact that children in the early stages of treatment are more prone to fatal medical complications and some mismanagement that may potentially increase the risk of death.41–44 In addition, the presence of respiratory complications that are commonly observed in children, like pneumonia, TB, and loss of appetite, accompanied by comorbidities, decreases child survival and shortens the mean survival time.33,45 This warrants careful identification, diagnosis, and management of such medical comorbidities in accordance with the national protocol.
A number of factors were found to be important predictors of child survival. A 2.4-fold increased hazard of death was observed among children with a diagnosis of pneumonia. In addition, a fourfold increased risk of death was also reported for pneumonia.46 Other studies conducted in Northwest and Northern Ethiopia showed that children with pneumonia have a 29% and 56% lower likelihood of recovering from SAM and have an increased risk of death, respectively.47,48,51 Furthermore, TB has the potential to increase the risk of death by three-fold (AHR=2.86; 1.08–7.63). Similarly, a study conducted at Sekota Hospital, northern Ethiopia (HR=2.88)49 and (AHR: 1.6)50 showed an increased risk of death by three and two folds. Frequent infections, particularly respiratory diseases, have the potential to limit dietary intake and child oxygenation, which may potentially increase the risk of early death.
It is known that reduced metabolic adaptation in SAM children usually makes the typical symptoms of comorbidities absent. This might lead to atypical presentations of children despite the fact that they have medical complications, but not clinically evident. But children may come up with a loss of appetite, an important clinical indicator of inherent medical complications. This study also found that children with loss of appetite had higher hazards of death. One study found that it increases the risk of death by almost threefold (AHR=2.7).34 Thus, clinicians need to be careful about the possibility of hiding a serious infection and should routinely give presumptive antibiotics as per the guideline.33,41
In addition, diarrhea was shown to increase the risk of death by 2.16 folds (AHR: 2.16; 1.16–4.06) compared to those who did not have diarrhea. Previous studies also pointed out that it increased the risk of death by 2.52.34 Furthermore, taking a deworming medication can reduce the risk of death by 64% when compared to those who did not take a deworming medication (AHR: 0.36, 0.21–0.66). Also, altered pulse rate due to various clinical conditions, including diarrhea, significantly increased the risk of death (AHR = 2.44, p-value <0.001).26 The presence of a nasogastric tube indicates that the child is unable to feed himself or herself consciously. Those children with NG tubes are more likely to be victims of medical complications and infections that warrant serious medical follow-up for a better clinical outcome. In addition, NG tube feeding in the presence of other complications increase child’s risk of death by 26%.48
This study indicated that a higher number of child deaths are observed, with important factors that determine child survival being identified. However, the findings of this study should be thought of in the light of some inherent limitations. Since the nature of the data is secondary data, the information for some children is lost and may be related to the outcome in that the current estimate may be underestimated. On the other hand, this study pinpoints important predictors for high mortality using appropriate statistical methods. This evidence will inform the hospital and others to focus on the most important areas to focus on for improved child survival. Further, there should be evidence on the facility readiness and quality of care for children that may contribute to increased risk of mortality, in addition to the clinical presentation of SAM children.
Conclusions and recommendations
In general, a higher child mortality rate and lower child survival were found among admitted SAM children in the hospital. In addition, loss of appetite at admission, the presence of medical complications (pneumonia, TB, and diarrhea), not getting deworming tablets, and being on NG tube feeding were important predictors of early death among SAM children. Implementation research on the level of implementation, quality of care, health professional’s readiness, skills, and other infrastructures should be thought about for a better understanding of the causes of higher mortality, besides medical conditions of the child. In addition, there should be an enhanced outreach program for malnutrition screening to identify SAM and acute malnutrition earlier before medical complications happen, reducing late presentations. There should be a targeted intervention in accordance with the national protocol for the management of SAM within hospitals.
Abbreviations
CI, confidence interval; HR, hazard ratio; MAM, moderate acute malnutrition; MUAC, mid-upper arm circumference; NG, nasogastric tube; SAM, severe acute malnutrition; TB, tuberculosis; UNICEF, United Nation International Children Education Fund; WFH, weight for height; WHO, World Health Organization.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The research was reviewed and ethically adopted by Dire Dawa University, College of Medicine and Health Science research and ethics review committee. Then, a written informed consent to collect data was obtained from the hospital manager on behalf of the SAM children's record. All possible ethical cares were respected throughout the conduct of the research project. All relevant ethical principles under the Helsinki declaration were followed and respected.
Acknowledgments
The authors would like to acknowledge Dire Dawa University for giving this opportunity to conduct this study. We would like to thank our data collectors, card retrievers, and staff of the Dilchora hospital for their valuable help and support for the accomplishment of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was obtained.
Disclosure
All the authors declare that they have no conflicts of interest in this work.
References
1. Collins S, Sadler K, Dent N, et al. Key issues in the success of community-based management of severe malnutrition. Food Nutr Bull. 2006;27(3_suppl3):S49–S82. doi:10.1177/15648265060273S304
2. World Health organization. Acute Malnutrition Summary Sheet, in Global Acute Malnutrition; 2012:1–2
3. Bhutta ZA, Das JK, Rizvi A, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013;382(9890):452–477. doi:10.1016/S0140-6736(13)60996-4
4. World Health organization. Update on Management of Severe Acute Malnutrition in Infants and Children, in Guideline 2013. Geneva: World Health organization; 2013:14–46.
5. Chiabi A, Malangue B, Nguefack S, et al. The clinical spectrum of severe acute malnutrition in children in Cameroon: a hospital-based study in Yaounde, Cameroon. Translational Pediatrics. 2017;6(1):32. doi:10.21037/tp.2016.07.05
6. UNICEF. Levels and Trends in Child Malnutrition UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2019 Edition. United Nations International Children Education Fund. 2–8. 2019.
7. Achadi E, Alvarez JL, Michael Anderson F, et al. Global Nutrition Report: shining a light to spur action on nutrition, in Global Nutrition Report 2018. Lancet. 2018:10–40.
8. Moyer JD, Bohl DK, Petry C, et al. The persistent global burden of severe acute malnutrition: cross-country estimates, models and forecasts. Global Transitions. 2020;2:167–179. doi:10.1016/j.glt.2020.07.004
9. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. lancet. 2013;382(9890):427. doi:10.1016/S0140-6736(13)60937-X
10. United Nations Children Education Fund (UNICEF), World Health organization (WHO) and The World Bank. Levels and Trends in Child Malnutrition, Nutrition. UNICEF. 1–12. 2019.
11. FMOH. National Strategy for Child Survival in Ethiopia. Addis Ababa: FMOH; 2005:1–5.
12. Ethiopian Federal Ministry of Health. The Cost of HUNGER in Ethiopia: Implications for Implications for the Growth and the Growth and Transformation of Ethiopia, the Social and Economic Impact of Child Undernutrition in Ethiopia Child Undernutrition in Ethiopia: Summary Report. Addis Ababa; 2012:3–8
13. Central Statistical Agency (CSA). Ethiopia Mini Demographic and Health Survey. Central Statistical Agency; 2014.
14. Kebede S. Survival Status and Predictors of Mortality among Children Aged 0–59 Months with Severe Acute Malnutrition Admitted to Stabilization Center at Sekota Hospital Waghemra Zone. J Nutr Disorders Ther. 2015;5(2):160–171.
15. Zelalem T, Tsinuel G, Ayalew T. Treatment outcome of severe acute malnutrition in children with and without HIV infection: a Historical cohort study in South-West Ethiopia. Ethiopian J Pediatrics Child Health. 2010;6(6):145.
16. Tefera C, Lemessa O, Gudina E, Eskezyiaw A. Treatment outcome and associated factors among under-five children with severe acute malnutrition admitted to therapeutic feeding unit in woldia hospital. North Ethiopia J Nutr Food Sci. 2014;4(6):548.
17. Habtemu J, Abdulhalik W, Fessahaye A. Survival status and predictors of mortality in severely malnourished children admitted to Jimma University Specialized Hospital from 2010 to 2012, Jimma, Ethiopia: a retrospective longitudinal study. BMC Pediatr. 2015;15:76. doi:10.1186/s12887-015-0398-4
18. Melaku G, Afework MB, Mache T. Treatment Outcomes and Associated Risk Factors of Severely Malnourished under Five Children Admitted to Therapeutic Feeding Centers of Mekelle City, Northern Ethiopia. Open Access Lib J. 2014;1(4):1–9.
19. Health, FMOH. Federal Ministry of Health Health and Health Related Indicators 2005 E. C (2012/2013); 2014:EFY
20. UNICEF. Ethiopia: humanitarian Situation Report 2019:January to December 2019; 2020. Available from: https://www.unicef.org/ethiopia/reports/ethiopia-humanitarian-situation-report-2019#:~:text=Over%204.89%20million%20children%20required,disease%20outbreaks%20drove%20humanitarian%20needs.
21. Williams PC, Berkley JA. Severe Acute Malnutrition Update: Current WHO Guidelines and the WHO Essential Medicine List for Children. Geneva, Switzerland: World Health Organization; 2016.
22. United Nation Children Education Fund (UNICEF). UNICEF Ethiopia Humanitarian Situation Report: may 2021. UNICEF Ethiopia Humanitarian Situation Report 2021. [
23. Achadi E, Ahuja A, Bendech MA, et al. Global Nutrition Report: from promise to impact: Ending malnutrition by 2030. International Food Policy Research Institute; 2016
24. Sathyamala C. Global nutrition report: towards a global governance in nutrition. Dev Change. 2017;48(5):1227–1242. doi:10.1111/dech.12332
25. Desyibelew HD, Baraki AG, Dadi AF. Mortality rate and predictors of time to death in children with severe acute malnutrition treated in Felege-Hiwot Referral Hospital Bahir Dar, Northwest Ethiopia. BMC Res Notes. 2019;12:409. doi:10.1186/s13104-019-4467-x
26. Girum T, Muktar E, Worku A. Comparative Analysis of the Survival Status and Treatment Outcome of Under-five Children Admitted with Severe Acute Malnutrition Among Hospital-based and Health Center Based Stabilization Centers, South Ethiopia. Open Public Health J. 2018;11:209–220. doi:10.2174/1874944501811010209
27. Ashine YE, Ayele BA, Aynalem YA, Yitbarek GY. Time to Death and its Predictor Among Children Under Five Years of Age with Severe Acute Malnutrition Admitted to Inpatient Stabilization Centers in North Shoa Zone, Amhara Region, Ethiopia. Nutr Dietary Supplements. 2020;12:167–177. doi:10.2147/NDS.S249045
28. Kabalo MY, Shanka MM. Seasonal variations of admission and survival status of children treated for severe acute malnutrition (SAM) at outpatient therapeutic program (OTP) in Wolaita Zone, Southern Ethiopia. Int J Collab Res Internal Med Public Health. 2016;8(9):1254.
29. Chamois S, Golden M, Grellety Y. Ethiopia Protocol for the management of Severe Acute Malnutrition (2007). 2007.
30. Thurstans S. Minimum Standards in Food Security and Nutrition: Management of Acute Malnutrition and Micronutrient Deficiencies, in the Sphere Project Humanitarian Charter and Minimum Standards in Humanitarian Response. The sphere project; 2011:168–169.
31. Wagnew F, Dessie G, Takele WW. A meta-analysis of inpatient treatment outcomes of severe acute malnutrition and predictors of mortality among under-five children in Ethiopia. BMC Public Health. 2019;19(1):1175. doi:10.1186/s12889-019-7466-x
32. Dire Dawa Administration Health Bureau. D.D.H., (self communication); information on Health care delivery 2020. 2020
33. FMOH. Training Course on the Management of Severe Acute Malnutrition. Addis Ababa, Ethiopia: FMOH; 2013:10–72.
34. Oumer A, Mesfin F, Demena M. Survival Status and Predictors of Mortality among Children Aged 0–59 Months Admitted with Severe Acute Malnutrition in Dilchora Referral Hospital, Eastern Ethiopia. East African J Health Biomed Sci. 2016;1(1):125.
35. Admasu A, Tadesse E, Moshago T, Mekonnen N. Survival Status and Its Associated Factors Among Under-Five Children Admitted with Complicated Severe Acute Malnutrition in Hospitals of Wolaita Zone. South Ethiopia: Retrospective Cohort Study; 2017.
36. Guesh G, Degu G, Abay M, et al. Survival status and predictors of mortality among children with severe acute malnutrition admitted to general hospitals of Tigray, North Ethiopia: a retrospective cohort study. BMC Res Notes. 2018;11(1):832. doi:10.1186/s13104-018-3937-x
37. Munthali T, Jacobs C, Sitali L, Dambe R, Michelo C. Mortality and morbidity patterns in under-five children with severe acute malnutrition (SAM) in Zambia: a five-year retrospective review of hospital-based records (2009–2013). Arch Public Health. 2015;73(1):23. doi:10.1186/s13690-015-0072-1
38. Collins S. Treating severe acute malnutrition seriously. Arch Dis Child. 2007;92(5):453–461. doi:10.1136/adc.2006.098327
39. Black R, Victora CG, Walker SP. Maternal and child undernutrition and overweight in low-income and middle income countries. Lancet. 2013;382(9890):427–451.
40. Aguayo VM, Agarwal V, Agnani M, et al. Integrated program achieves good survival but moderate recovery rates among children with severe acute malnutrition in India. Am J Clin Nutr. 2013;98(5):1335–1342. doi:10.3945/ajcn.112.054080
41. Bruno S. Effects of infections on severely malnourished children in Kilifi-Mombasa and Dar es Salaam: a comparative study. Dar Es Salaam Med Students J. 2006;14(1):27–35.
42. Nzioki C, Irimu G, Musoke R, English M. Audit of Care for Children Aged 6–59 Months Admitted with Severe Acute Malnutrition at Kenyatta National Hospital. Kenya Int Health. 2009;1:91–96. doi:10.1016/j.inhe.2009.06.008
43. Keane E. Integrating Severe Acute Malnutrition into the Management of Childhood Diseases at Community Level in South Sudan. Malaria Consortium; 2013:1–36.
44. World Health organization. Maternal, Infant and Young Child Nutrition in East and Southern African Countries: Moving to National Implementation, in Report of a World Health Organization Workshop. Entebbe, Uganda: Geneva, WHO; 2014:7–12.
45. Ashworth A. Efficacy and Effectiveness of Community-Based Treatment of Severe Malnutrition. Nutrition and Public Health Intervention Research; 2005:1–10.
46. Chanchal R, Koonwar S, Gupta S. PREDICTORS OF MORTALITY IN CHILDREN WITH SEVERE ACUTE MALNUTRITION (SAM): a PROSPECTIVE OBSERVATIONAL STUDY IN NORTHERN INDIA. Int J Sci Res. 2020;9(1):458.
47. Derseh B, Mruts K, Demie T, Gebremariam T. Co-morbidity, treatment outcomes and factors affecting the recovery rate of under-five children with severe acute malnutrition admitted in selected hospitals from Ethiopia: retrospective follow up study. Nutr J. 2018;17(1):116. doi:10.1186/s12937-018-0423-1
48. Chane T, Oljira L, Atomesa GE, Agedew E. Treatment outcome and associated factors among under-five children with severe acute malnutrition admitted to therapeutic feeding unit in Woldia hospital, North Ethiopia. J Nutr Food Sci. 2014;4(6):1. doi:10.4172/2155-9600.1000329
49. Desta K. Survival status and predictors of mortality among children aged 0–59 months with severe acute malnutrition admitted to stabilization center at Sekota Hospital Waghemra Zone. J Nutr Disord Ther. 2015;5:160.
50. Wagnew F, Dejenu G, Eshetie S, et al. Treatment cure rate and its predictors among children with severe acute malnutrition in northwest Ethiopia: a retrospective record review. PLoS One. 2019;14(2):e0211628. doi:10.1371/journal.pone.0211628
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.