Back to Journals » International Journal of General Medicine » Volume 16
Predictive Value of the Prothrombin Time-International Normalized Ratio to Albumin Ratio in the Prognosis of Patients with Hepatitis B Virus-Related Acute-on-Chronic Liver Failure
Authors Sheng Y ![]() , Zeng Y
, Zeng Y ![]() , Luo W, Zhang X, Wang H, Jiao J
, Luo W, Zhang X, Wang H, Jiao J ![]()
Received 9 August 2023
Accepted for publication 28 September 2023
Published 6 October 2023 Volume 2023:16 Pages 4565—4572
DOI https://doi.org/10.2147/IJGM.S434572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Yunjian Sheng,1,* Yu Zeng,1,* Wenling Luo,1 Xuemei Zhang,1 Hang Wang,2 Jiahuan Jiao3
1Department of Infectious Diseases, the Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China; 2Department of Gastroenterology, Dazhou Hospital of Integrated Traditional and Western Medicine, Dazhou, Sichuan, People’s Republic of China; 3Department of Infectious Diseases, the People’s Hospital of Leshan, Leshan, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunjian Sheng, Department of Infectious Diseases, the Affiliated Hospital of Southwest Medical University, No. 25 Taiping Street, Luzhou, Sichuan Province, People’s Republic of China, Email [email protected]
Background: Acute-on-chronic liver failure is a common clinical syndrome with high short-term mortality, and early assessment of its mortality risk is crucial, but the search for valid and accurate prognostic biomarkers is a challenging endeavor. The purpose of this study was to investigate the predictive value of the prothrombin time-international normalized ratio to albumin ratio (PTAR) for mortality in patients with hepatitis B virus-related acute-on-chronic liver failure (HBV-ACLF).
Patients and methods: A total of 354 patients with HBV-ACLF were included in the retrospective study. Patients were divided into survival and non-survival groups based on 90-day follow-up. Cox regression analysis was used to explore the relationship between PTAR and 90-day mortality in patients with HBV-ACLF. The area under the receiver operating characteristic curve was used to evaluate the effectiveness of PTAR in predicting mortality.
Results: PTAR was significantly higher in non-survivors than in survivors. The results of multivariate analysis showed that PTAR was a valid independent predictor of mortality in patients with HBV-ACLF. Its predictive ability for mortality was similar to that of the Child-Turcotte-Pugh score, the end-stage liver disease model (MELD) score, and the MELD-sodium score.
Conclusion: PTAR may be a simple and effective tool for predicting the prognosis of patients with HBV-ACLF.
Keywords: acute-on-chronic liver failure, hepatitis B virus, prothrombin time-international normalized ratio to albumin ratio, prognosis
Introduction
Acute-on-chronic liver failure (ACLF) is a unique syndrome occurring on the basis of chronic liver disease, characterized by the development of hepatic or extrahepatic organ failure, with a poor prognosis and high risk of death, and is one of the very serious types of end-stage liver disease commonly seen in clinical practice.1 Hepatitis B virus (HBV) infection is a major global public health problem, and China has a high prevalence of HBV infection. The most important cause of ACLF in China is the reactivation of HBV, and HBV-related acute-on-chronic liver failure (HBV-ACLF) is the most common type of liver failure in China.2,3 The main principles of current treatment of ACLF are diagnosis and treatment of the precipitating event and provision of supportive therapy. Liver transplantation is currently the only known and effective treatment option. However, there is a shortage of organs and high costs, thus resulting in a very limited number of patients who can be treated with liver transplantation.4,5 Other emerging therapies including granulocyte colony-stimulating factor, and cytarabine are promising alternatives to liver transplantation, but their safety and efficacy need to be further validated.5 Therefore, early assessment of the risk of death in patients with ACLF and selection of appropriate treatment modalities to prevent its development are crucial.
The prothrombin time-international normalized ratio to albumin ratio (PTAR), a new objective score, was first created by Haruki et al.6 They conducted a retrospective study of 199 patients with hepatocellular carcinoma after resection and demonstrated that the PTAR was a good predictor of prognosis in these patients and could also be used to assess liver function reserve after hepatectomy in patients with hepatocellular carcinoma.6 Like patients after hepatocellular carcinoma resection, HBV-ACLF patients also have hepatic dysfunction and diminished hepatic reserve function. Therefore, our study aimed to investigate the value of PTAR score as a method to predict 90-day mortality in patients with HBV-ACLF.
Methods
Patient Selection
354 patients with HBV-ACLF hospitalized in the Infection Department of the Affiliated Hospital of Southwest Medical University from June 2017 to February 2022 were retrospectively recruited. Inclusion criteria for HBV-ACLF were based on the consensus recommendations of the Asia Pacific Association for the Study of the Liver (APASL) and the Chinese Group on the Study of Severe Hepatitis B:3,7 (1) hepatitis B virus surface antigen positivity >6 months; (2) jaundice with serum bilirubin ≥ 5 mg/dl or ≥ 85μmol/l and coagulopathy with international normalized ratio (INR) ≥1.5 or prothrombin activity ≤ 40%; (3) complicated ascites and/or hepatic encephalopathy within 4 weeks. The exclusion criteria were as follows: (1) hepatocellular carcinoma or other tumors, liver transplantation; (2) co-infection with hepatitis A/C/D/E virus, human immunodeficiency virus (HIV) or other hepatitis viruses; (3) combination with alcoholic liver disease, autoimmune liver disease, drug-related liver damage; (4) patients with incomplete clinical data or lost to follow-up. The included patients all received comprehensive internal medicine treatment during their hospitalization. Patients were followed up for 90 days and divided into survival and death groups according to their clinical outcome.
Clinical Data and Laboratory Indicators
Record the patient’s sex, age, comorbidities, and initial laboratory indicators after admission: alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyl transpeptidase (GGT), albumin, total bilirubin (TBIL), direct bilirubin (DBIL), creatinine, white blood cell count (WBC), neutrophil count (NEU), hemoglobin, red blood cell distribution width (RDW), platelet, serum potassium (K), serum sodium (Na), prothrombin time (PT), INR. The formula for calculating PTAR was INR divided by Alb (g/dL), and the model for end-stage liver disease model (MELD) score was calculated according to the formula: MELD = 3.8 × ln(TBIL mg/dl) + 11.2 × ln(INR) + 9.6 × ln(creatinine mg/dl) + 6.4,8 MELD-sodium (MELD-Na) score = MELD + 1.59 × [135-Na (mmol/l)],9 and Child-Turcotte-Pugh (CTP) score was calculated according to the relevant criteria.10
Statistical Analysis
SPSS version 27 and MedCalc version 20.0.22 software were used for statistical analysis. Normally distributed continuous variables were expressed as mean ± standard deviation, and non-normally distributed continuous variables were expressed as median and interquartile range, and the t-test or Mann–Whitney U-test was used for comparison between groups of continuous variables. Categorical variables were expressed as frequencies and percentages, and the chi-squared test was used for comparison between groups. Spearman correlation analysis was used to evaluate the correlation between PTAR and CTP score, MELD score and MELD-Na score. The Kaplan-Meier method was used to construct 90-day survival probability curves and compared with the Log rank test. Univariate and multivariate analyses of prognostic factors were performed using cox regression models. The predictive accuracy of each model was analyzed using the area under the receiver operating characteristic (ROC) curve (AUC). Comparisons between AUCs were performed using the De-Long test. Differences were considered statistically significant when P < 0.05 for the two-tailed test.
Results
Patient Characteristics
Based on our inclusion and exclusion criteria, 354 patients with HBV-ACLF were finally included in the study (Figure 1). The mean age of the patients was 48.26 years and the majority were male (82.5%). Complications were ascites in 215 patients (60.7%), hepatic encephalopathy in 48 patients (13.8%), gastrointestinal bleeding in 7 patients (2%), and hepatorenal syndrome in 6 patients (1.7%). The patients were divided into 272 cases in the survival group and 82 cases in the death group. By comparison, it was found that ALT, GGT, albumin, hemoglobin, platelet, and Na were higher in the survival group than in the death group, and age, TBIL, DBIL, creatinine, PT, INR, WBC, NEU, RDW, PTAR, CTP score, MELD score, and MELD-Na score were lower in the survival group than in the death group, and the differences were statistically significant (all P < 0.05) (Table 1).
 |
Table 1 Comparisons of Baseline Characteristics Between Survivors and Non-Survivors |
 |
Figure 1 Flow chart of study participants. |
Univariate and Multivariate Cox Regression Analysis of 90-Day Prognosis in Patients with HBV-ACLF
Univariate cox regression analysis was performed for the parameters with statistical significance in Table 1. Multivariable cox regression analysis was performed for indicators with significant variation (P < 0.05) in univariate analysis, which included age, TBIL, DBIL, creatinine, PT, INR, WBC, NEU, RDW, ALT, GGT, albumin, hemoglobin, platelet, Na, and PTAR. The results of multivariate cox regression analysis showed that PTAR (OR: 4.388, 95% CI: 2.833–6.796), Na (OR: 0.947, 95% CI: 0.905–0.992), TBIL (OR: 1.004, 95% CI: 1.002–1.005), age (OR: 1.027, 95% CI: 1.008–1.045) were considered as independent prognostic factors for 90-day mortality in patients with HBV-ACLF (Table 2).
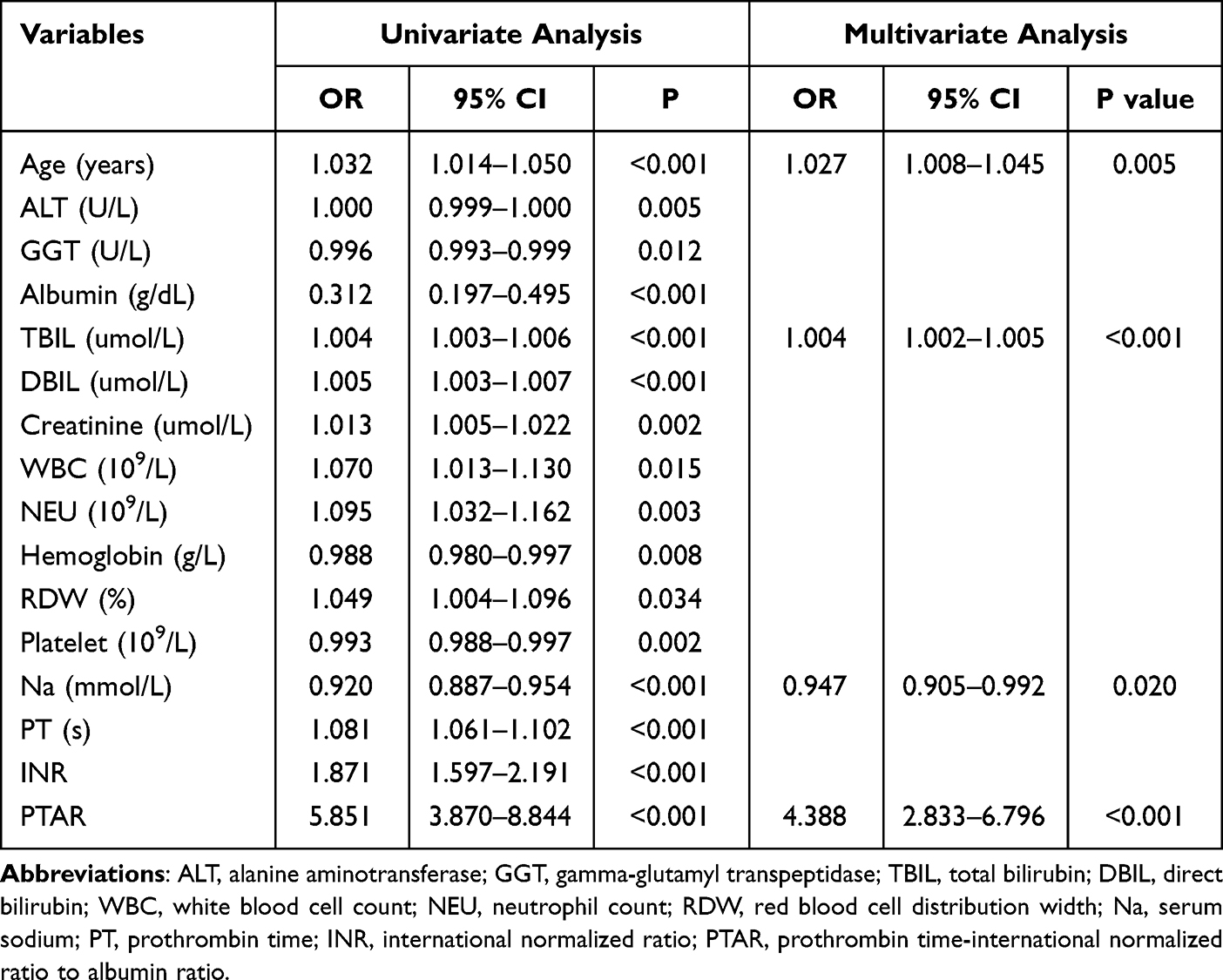 |
Table 2 Cox Regression Analysis of Factors Associated with 90-Day Mortality in Patients with HBV-ACLF |
Correlation of PTAR with Other Scores and Survival Curve Analysis
PTAR was positively correlated (P < 0.001) with CTP score (r = 0.69), MELD score (r = 0.733), and MELD-Na score (r = 0.584), suggesting that PTAR may be closely related to the prognosis of HBV-ACLF patients. We plotted Kaplan-Meier survival curves based on the cut-off value of patients’ PTAR. The results showed that patients with PTAR >0.67 had a worse prognosis (log rank P < 0.001) (Figure 2).
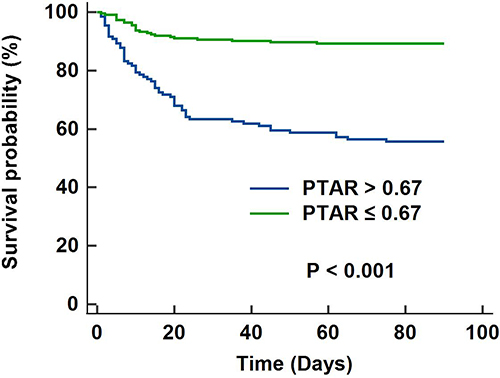 |
Figure 2 Survival curves of groups with PTAR > 0.67 and PTAR ≤ 0.67 by Kaplan-Meier survival analysis. Abbreviation: PTAR, prothrombin time-international normalized ratio to albumin ratio. |
Predictive Value of PTAR for 90-Day Prognosis in Patients with HBV-ACLF
The ROCs for PTAR, CTP score, MELD score and MELD-Na score are shown in Figure 3. The AUC values were 0.788 (95% CI: 0.734–0.842) for PTAR, 0.841 (95% CI: 0.794–0.887) for CTP score, 0.794 (95% CI: 0.743–0.845) for MELD score, and 0.777 (95% CI: 0.721–0.833) for MELD-Na score. The AUC of PTAR in determining poor prognosis was not statistically significant from the other three groups (P > 0.05). The sensitivity and specificity were 0.71 and 0.74, respectively, and the positive and negative predictive values were 0.45 and 0.89, respectively, when using the best cut-off value of PTAR of 0.67 to predict 90-day mortality. Details are shown in Table 3.
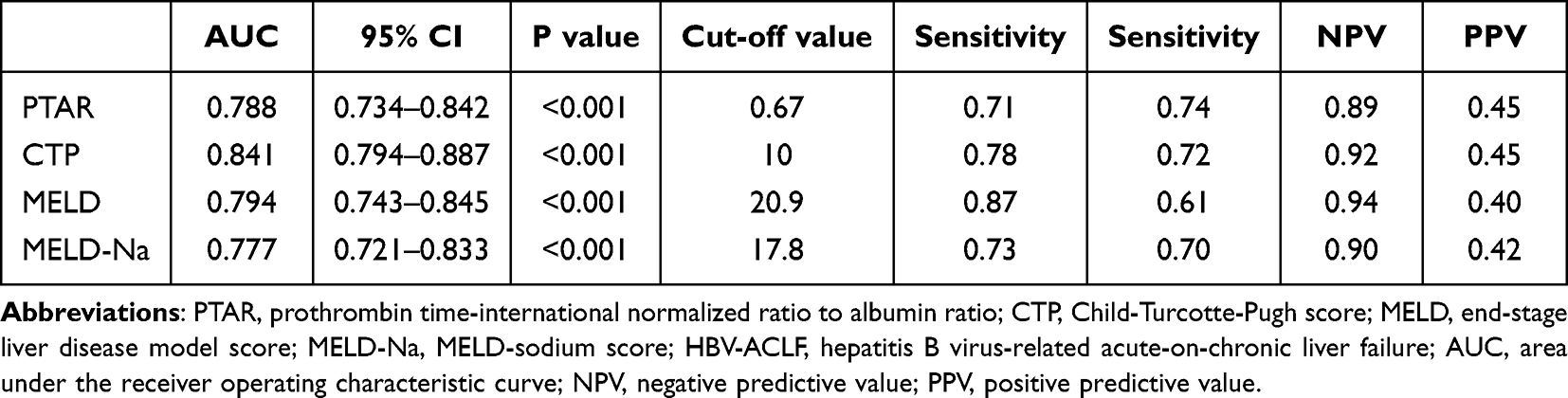 |
Table 3 Predictive Value of PTAR, CTP, MELD, and MELD-Na for 90-Day Mortality in Patients with HBV-ACLF |
 |
Figure 3 Receiver operating characteristics curves of PTAR, CTP, MELD, and MELD-Na for predicting 90-day mortality in patients with hepatitis B virus-related acute-on-chronic liver failure. Abbreviations: PTAR, prothrombin time-international normalized ratio to albumin ratio; CTP, Child-Turcotte-Pugh score; MELD, end-stage liver disease model score; MELD-Na, MELD-sodium score. |
Discussion
HBV-ACLF is a common clinical syndrome with an acute onset, rapid development of organ failure, and high short-term mortality. The pathogenesis of ACLF is complex and not fully understood, and some studies have shown that the core of the pathogenesis is an immune imbalance, which initially manifests as an excessive inflammatory response, and this hyperinflammatory state impairs the host defense mechanisms of immune cells, leading to immune hypofunction or even failure later in the course of the disease. And the severity of systemic inflammation is closely related to the severity of ACLF and the duration of hospitalization.11–13 To improve the outcome of patients with ACLF, predicting the risk of death and carefully selecting therapeutic interventions is crucial, but predicting the risk of death in patients with ACLF is currently challenging. In our study, PTAR was found to be a good predictor for assessing the prognosis of patients with HBV-ACLF.
There have been several studies on the relationship between PTAR and patient prognosis.14–17 Wang et al through a retrospective study of 4536 patients with sepsis found that PTAR scores could predict the prognosis of patients with sepsis and may help to rapidly identify patients with liver injury and dysfunction.14 Sreeraj’s study also found that the PTAR scoring system could be used to predict the prognosis of patients with cirrhosis combined with sepsis.15 Gao et al showed that the PTAR scoring system could be used to predict the prognosis of critically ill patients with hepatic sclerosis through a study of 865 patients.16 PTAR has also been identified as a prognostic predictor of mortality in patients with hepatitis B virus-associated decompensated cirrhosis.17
Both INR and albumin reflect the synthetic function of the liver. Human serum albumin, a protein synthesized in the liver, is the most abundant plasma protein, accounting for approximately 50% of the total protein content (3.5–5 g/L). Albumin is mostly used to maintain colloid osmotic pressure and is also considered a negative acute phase protein that may affect microvascular integrity and aspects of the inflammatory response.18 Albumin may block inflammatory signaling pathways through intracellular internalization into endocytic vesicles and may reverse plasma-mediated immune dysfunction by binding and inactivating prostaglandin E2. Albumin is emerging as a potent modulator of the innate immune system and can be used in the management of ACLF.19,20 Serum albumin is produced exclusively by the liver and can reflect hepatic function, which is an important indicator to assess hepatic synthetic function and hypoproteinemia.21 In our study, we found that serum albumin was significantly lower in the death group compared to the survival group. Therefore, low serum albumin levels may partially reflect the inflammatory status and hepatic synthetic function in HBV-ACLF patients. In addition, changes in coagulation-related parameters are hallmarks of advanced liver disease, and PT and INR are inextricably linked to the prognosis and progression of liver disease. The progression of protein synthesis dysfunction is also inevitably associated with the progression and prognosis of liver disease, both in acute liver failure and in chronic liver disease. The inclusion of INR in the prognostic mortality equation of various liver diseases such as MELD score, MELD-Na score and chronic liver failure sequential organ failure assessment (CLIF-SOFA) score is evidence that INR is closely associated with hepatic synthetic dysfunction.22 And, among the factors that constitute the MELD score, the INR has been reported to have the greatest impact on the score.23 In the present study, we found that although the results of univariate analysis showed that albumin and INR were risk factors for mortality, neither was considered an independent predictor of mortality in patients with HBV-ACLF in the results of multifactorial analysis. This discrepancy may arise because PTAR, which is a ratio of albumin and INR, would be more stable than either indicator, whereas individual indicators may change depending on multiple factors such as blood sample handling or degree of hydration.
The univariate results of this study showed a significant increase in PTAR in those who died compared to those who survived. And PTAR was positively correlated with CTP score, MELD score and MELD-Na score. In addition, it was further demonstrated by multivariate analysis that PTAR was an independent predictor of 90-day mortality in HBV-ACLF patients, and the higher the PTAR score, the worse the prognosis of patients. Although several models such as CTP score and MELD score exist for risk prediction of prognosis of HBV-ACLF patients, the complexity of calculation makes their application in daily clinical practice somewhat limited. In addition, clinical assessments such as hepatic encephalopathy are somewhat subjective, which may affect the accuracy of the models. Compared with these models, the PTAR score requires only simple and rapid calculation of two easily available laboratory parameters, which has the advantage of simplicity, objectivity and convenience, and its predictive accuracy remains high.
This study has some limitations. First, it is a single-center study with a limited number of included patient cases and cannot represent all regions of HBV-ACLF patients. Second, this is a retrospective study without dynamic observation of changes in relevant indicators, so further large-scale prospective clinical trials may be needed to validate the current results.
Conclusion
In conclusion, this study suggests that PTAR is a simple and effective adjunctive marker for predicting 90-day prognosis in patients with HBV-ACLF. The mortality predictive ability of PTAR is similar to that of the CTP score, the MELD score, and the MELD-Na score, and it has the advantages of being easy to obtain, simple, and objective. However, further studies are needed to evaluate and validate its applicability.
Data Sharing Statement
The data used to support the results of this study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The study was approved by the Clinical Trial Ethics Committee of the Affiliated Hospital of Southwest Medical University (approval number: KY2023060). Given the retrospective nature of this study, the committee waived the requirement for informed consent. We declare that patient information will be kept confidential and that the principles of the Declaration of Helsinki will be adhered to.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moreau R, Gao B, Papp M, Bañares R, Kamath PS. Acute-on-chronic liver failure: a distinct clinical syndrome. J Hepatol. 2021;75(1):S27–S35. doi:10.1016/j.jhep.2020.11.047
2. Wang H, Men P, Xiao Y, et al. Hepatitis B infection in the general population of China: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):811. doi:10.1186/s12879-019-4428-y
3. Sarin SK, Choudhury A, Sharma MK, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update. Hepatol Int. 2019;13(4):353–390. doi:10.1007/s12072-019-09946-3
4. Zhao RH, Shi Y, Zhao H, Wu W, Sheng JF. Acute-on-chronic liver failure in chronic hepatitis B: an update. Expert Rev Gastroenterol Hepatol. 2018;12(4):341–350. doi:10.1080/17474124.2018.1426459
5. Kumar R, Mehta G, Jalan R. Acute-on-chronic liver failure. Clin Med. 2020;20(5):501–504. doi:10.7861/clinmed.2020-0631
6. Haruki K, Shiba H, Saito N, et al. Risk stratification using a novel liver functional reserve score of combination prothrombin time-international normalized ratio to albumin ratio and albumin in patients with hepatocellular carcinoma. Surgery. 2018;164(3):404–410. doi:10.1016/j.surg.2018.02.022
7. Wu T, Li J, Shao L, et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut. 2018;67(12):2181–2191. doi:10.1136/gutjnl-2017-314641
8. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464–470. doi:10.1053/jhep.2001.22172
9. Biggins SW, Kim WR, Terrault NA, et al. Evidence-based incorporation of serum sodium concentration into MELD. Gastroenterology. 2006;130(6):1652–1660. doi:10.1053/j.gastro.2006.02.010
10. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646–649. doi:10.1002/bjs.1800600817
11. Clària J, Stauber RE, Coenraad MJ, et al. Systemic inflammation in decompensated cirrhosis: characterization and role in acute-on-chronic liver failure. Hepatology. 2016;64(4):1249–1264. doi:10.1002/hep.28740
12. Laleman W, Claria J, Van der Merwe S, Moreau R, Trebicka J. Systemic Inflammation and Acute-on-Chronic Liver Failure: too Much, Not Enough. Can J Gastroenterol Hepatol. 2018;2018:1027152. doi:10.1155/2018/1027152
13. Casulleras M, Zhang IW, López-Vicario C, Clària J. Leukocytes, Systemic Inflammation and Immunopathology in Acute-on-Chronic Liver Failure. Cells. 2020;9(12):2632. doi:10.3390/cells9122632
14. Wang S, Ding S, Luo H, Chai X. International Normalized Ratio to Albumin Ratio (PTAR): an Objective Risk Stratification Tool in Patients with Sepsis. Int J Gen Med. 2021;14:1829–1841. doi:10.2147/IJGM.S305085
15. S S. Assessment of INR to Albumin Ratio in Predicting Outcome During Hospital Stay in Patients with Cirrhosis of Liver with Sepsis. J Assoc Physicians India. 2022;70(4):11–12.
16. Gao F, Cai MX, Lin MT, et al. Prognostic value of international normalized ratio to albumin ratio among critically ill patients with cirrhosis. Eur J Gastroenterol Hepatol. 2019;31(7):824–831. doi:10.1097/MEG.0000000000001339
17. Cai M, Han Z, He X, Zhang J. Usefulness of International Normalized Ratio to Albumin Ratio for Evaluation of Mortality in Hepatitis B Virus-Associated Decompensated Cirrhosis. Biomed Res Int. 2021;2021:6664574. doi:10.1155/2021/6664574
18. Quinlan GJ, Martin GS, Evans TW. Albumin: biochemical properties and therapeutic potential. Hepatology. 2005;41(6):1211–1219. doi:10.1002/hep.20720
19. Arroyo V, Clària J. Acute-on-Chronic Liver Failure, Human Serum Albumin, and Immune Modulation: the Beginning of an Exciting Adventure. Clin Gastroenterol Hepatol. 2018;16(5):633–636. doi:10.1016/j.cgh.2017.12.008
20. China L, Maini A, Skene SS, et al. Albumin Counteracts Immune-Suppressive Effects of Lipid Mediators in Patients With Advanced Liver Disease. Clin Gastroenterol Hepatol. 2018;16(5):738–747.e7. doi:10.1016/j.cgh.2017.08.027
21. Bernardi M, Maggioli C, Zaccherini G. Human albumin in the management of complications of liver cirrhosis. Crit Care. 2012;16(2):211. doi:10.1186/cc11218
22. Northup PG, Caldwell SH. Coagulation in liver disease: a guide for the clinician. Clin Gastroenterol Hepatol. 2013;11(9):1064–1074. doi:10.1016/j.cgh.2013.02.026
23. Porte RJ, Lisman T, Tripodi A, Caldwell SH, Trotter JF; Coagulation in Liver Disease Study Group. The International Normalized Ratio (INR) in the MELD score: problems and solutions. Am J Transplant. 2010;10(6):1349–1353. doi:10.1111/j.1600-6143.2010.03064.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Design for a Multicentre Prospective Cohort for the Assessment of Platelet Function in Patients with Hepatitis-B-Virus-Related Acute-on-Chronic Liver Failure
Jiang X, Chai S, Huang Y, Huang Z, Tan W, Gao Y, Lu X, Meng Z, Zhou H, Kong W, Tang X, Tang Y, Qi T, Liao C, Gan Q, Xiang X, Zhang Y, Wang S, Chen Y, Chen J
Clinical Epidemiology 2022, 14:997-1011
Published Date: 24 August 2022
Analysis of Clinical Characteristics and Long-Term Prognosis in Young Patients with Hepatitis B Cirrhosis: A Propensity Score Matched Study
Zhang P, Zhang W, Chen X, Guo H, Cai X, Tao C, Hong X, Zhang Z
Infection and Drug Resistance 2026, 19:569500
Published Date: 21 January 2026