Back to Journals » International Journal of General Medicine » Volume 18
Predictive Value of the Modified Comprehensive Immunoinflammatory Indices for Hemorrhagic Transformation in Ischemic Stroke Patients Undergoing Thrombolysis: A Retrospective Study
Authors Cai J, Rao H, Li X, Luo J, Wang Z, Liu D
Received 9 June 2025
Accepted for publication 1 October 2025
Published 21 October 2025 Volume 2025:18 Pages 6353—6363
DOI https://doi.org/10.2147/IJGM.S545665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Junzhi Cai,1 Hui Rao,2 Xiangyang Li,1 Jingwen Luo,1 Zhenchang Wang,1 Dezhong Liu1
1Department of Emergency Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Department of Laboratory Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Dezhong Liu, Department of Emergency Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China, Email [email protected]
Objective: Ischemic stroke is closely related to inflammation and immune balance. The purpose of this study was to investigate the relationship of modified comprehensive immunoinflammatory indices (modified pan-immune-inflammation-value (mPIV), modified systemic immune-inflammatory index (mSII), modified systemic inflammatory response index (mSIRI)) and hemorrhagic transformation (HT) of ischemic stroke.
Methods: 894 ischemic stroke patients treated in Meizhou People’s Hospital from January 2019 to May 2024 were retrospectively analyzed. Clinical characteristics were collected, and mPIV, mSII, and mSIRI were calculated. The optimal cutoff values of mPIV, mSII, and mSIRI were analyzed by receiver operating characteristic (ROC) curve analysis. The relationship between mPIV, mSII, mSIRI and HT of ischemic stroke was analyzed.
Results: There were 685 (76.6%) patients without HT and 209 (23.4%) with HT. The cases with HT had higher mPIV (1337.71 (698.79, 2511.19) vs 992.37 (599.30, 1884.53), p=0.001), mSII (3418.31 (1895.87, 7112.89) vs 2574.81 (1630.46, 4006.18), p< 0.001), and mSIRI level (963.60 (517.86, 1947.87) vs 698.75 (446.99, 1100.62), p< 0.001) than those without HT. In ROC analysis, the cutoff value of mPIV was 1302.4 (sensitivity 50.7%, specificity 64.7%, area under the ROC curve (AUC): 0.575), mSII cutoff value was 3186.5 (sensitivity 54.5%, specificity 63.8%, AUC: 0.605), and mSIRI cutoff value was 996.5 (sensitivity 49.8%, specificity 70.2%, AUC: 0.610). Logistic regression analysis showed that high mPIV (odds ratio (OR): 1.901, 95% confidence interval (CI): 1.381– 2.617, p< 0.001), high mSII (OR: 2.081, 95% CI: 1.517– 2.854, p< 0.001), and high mSIRI (OR: 2.290, 95% CI: 1.664– 3.151, p< 0.001) were significantly associated with HT.
Conclusion: High levels of mPIV, mSII, and mSIRI may be associated with hemorrhagic transformationin patients with ischemic stroke who received intravenous thrombolysis treatment.
Keywords: ischemic stroke, hemorrhagic transformation, modified pan-immune-inflammation-value, modified systemic immune-inflammatory index, modified systemic inflammatory response index
Introduction
Cerebral infarction, also known as ischemic stroke, is a localized ischemic necrosis or softening of brain tissue caused by blood circulation disorders in the brain, resulting in ischemia and hypoxia.1 Its pathogenesis is complex, mainly including atherosclerosis, thrombosis, and embolism. These factors can lead to blockage of cerebral blood vessels, causing local brain tissue to lose blood supply and subsequently triggering neurological deficits.2,3 Clinically, patients often present with sudden limb weakness, slurred speech, facial numbness, visual impairment, and so on. In severe cases, coma or even death may occur.4,5 Epidemiological data show that cerebral infarction has become one of the main causes of death and disability worldwide.6
Intravenous thrombolysis is currently one of the most effective treatment methods for the early stage of acute cerebral infarction.7,8 Especially intravenous thrombolysis with recombinant tissue plasminogen activator (rt-PA), by activating plasminogen to convert into plasmin, dissolving thrombus, restoring blood perfusion of brain tissue in the infarcted area, and saving the ischemic penumbra, thereby improving the neurological function of patients.9,10 However, although thrombolytic therapy has brought new hope to patients with cerebral infarction, the clinical prognosis is still not optimistic. Relevant studies have shown that among patients who receive intravenous thrombolysis, only 30% to 50% can achieve good clinical outcomes.11–13
Hemorrhagic transformation (HT) after thrombolysis for cerebral infarction refers to the phenomenon where blood exudation or hematoma formation occurs in the infarcted area or surrounding tissues in patients with acute cerebral infarction after thrombolysis therapy.14 According to whether it is accompanied by neurological deterioration, HT can be classified into asymptomatic hemorrhage transformation (aHT) and symptomatic hemorrhage transformation (sHT).15 aHT may cause brain tissue edema to worsen and trigger inflammatory responses, leading to long-term decline in cognitive function and delayed recovery of neurological function in patients,16 while sHT patients often experience acute neurological deterioration such as impaired consciousness and aggravated limb paralysis, with a high mortality rate.17 The occurrence of HT is a complex pathological process mediated by the imbalance among ischemic injury, the effects of thrombolytic drugs, and vascular repair.18 After the occurrence of cerebral infarction, the ischemia and hypoxia in the brain tissue will first cause damage to the endothelial cells of the cerebral blood vessels.19 Excessive activation of the fibrinolytic system significantly reduces the local blood coagulation ability, making it difficult for damaged blood vessels to achieve self-repair through the coagulation mechanism.20 Reperfusion of blood flow will have a “flushing effect” on the damaged blood vessel walls, thereby exacerbating the damage to the vessels.21 The occurrence of hemorrhagic transformation after thrombolysis for cerebral infarction is influenced by multiple risk factors.14
After cerebral infarction occurs, the body immediately initiates an inflammatory response.19 This process plays a complex and crucial role in the pathological process of cerebral infarction and is closely related to the HT after thrombolysis.22 In the acute stage of cerebral infarction, ischemia and hypoxia trigger a local inflammatory cascade reaction. A large number of inflammatory cells, such as neutrophils and monocytes, rapidly recruit to the infarcted area and release pro-inflammatory cytokines such as tumor necrosis factor -α (TNF-α) and interleukin-6 (IL-6).23 These cytokines not only aggravate local brain tissue damage, but also disrupt the integrity of the blood-brain barrier, laying hidden dangers for HT.
The dynamic balance of inflammatory response, immune status, and nutritional status plays a crucial role in the occurrence, development and prognosis of cerebral vessel disease.24 And the thrombolytic treatment process can lead to inflammatory responses, coagulation dysfunction and changes in the patient’s nutritional status within their body.25,26 Some composite immune-inflammation indices integrate the counts of different immune cell subsets, coagulation-related parameters, or organ function indicators to more systematically capture the interaction between the immune system and inflammation in the body, providing a more comprehensive biological basis for disease risk assessment. A series of new inflammatory immune indices based on the combination of peripheral blood cell counts and laboratory indicators have emerged, such as the modified pan-immune-inflammation-value (mPIV), modified systemic immune-inflammatory index (mSII), and modified systemic inflammatory response index (mSIRI), have gradually become research hotspots.27,28 The pathological mechanisms of stroke and hemorrhagic transformation after thrombolysis (such as ischemia-reperfusion injury, disruption of the blood-brain barrier, and inflammatory-coagulation interaction activation) are highly consistent with the dimensions of the modified immune index (such as the synergistic effect of nutritional status - coagulation - inflammation).29–31 As new inflammatory immune indicators, at present, the predictive value of mPIV, mSII, and mSIRI in the hemorrhagic transformation of patients with ischemic stroke undergoing thrombolysis remains unclear. The purpose of this study is to solve this problem.
Materials and Methods
Participants
A retrospective analysis was conducted on 894 patients with acute cerebral infarction who received intravenous thrombolysis and were continuously recorded in Meizhou People’s Hospital from January 2019 to May 2024. All the subjects received intravenous thrombolytic therapy within 5 hours. The intravenous thrombolysis method refers to the “Chinese Stroke Association guidelines for clinical management of ischaemic cerebrovascular diseases”.32
Inclusion criteria: (1) patients diagnosed with CI accordance with the criteria of the Chinese Guidelines for Ischemic Stroke;33 (2) age ≥18 years old; (3) patients who meet the indications for intravenous thrombolysis in the “Chinese Stroke Association guidelines for clinical management of ischaemic cerebrovascular diseases”32 (4) patients who underwent cranial CT or MRI reexamination after thrombolysis; and (5) the patients’ admission information were complete. Exclusion criteria: (1) patients who undergo arterial thrombolysis or arterial thrombectomy through cerebral vascular intervention; (2) patients received bridging therapy or surgical decompression; (3) patients without subsequent imaging or insufficient clinical data for analysis; and (4) patients whose laboratory indicators are significantly affected due to severe diseases or organ function impairment. This study was supported by the Ethics Committee of the Meizhou People’s Hospital. The flowchart of present study is shown in Figure 1.
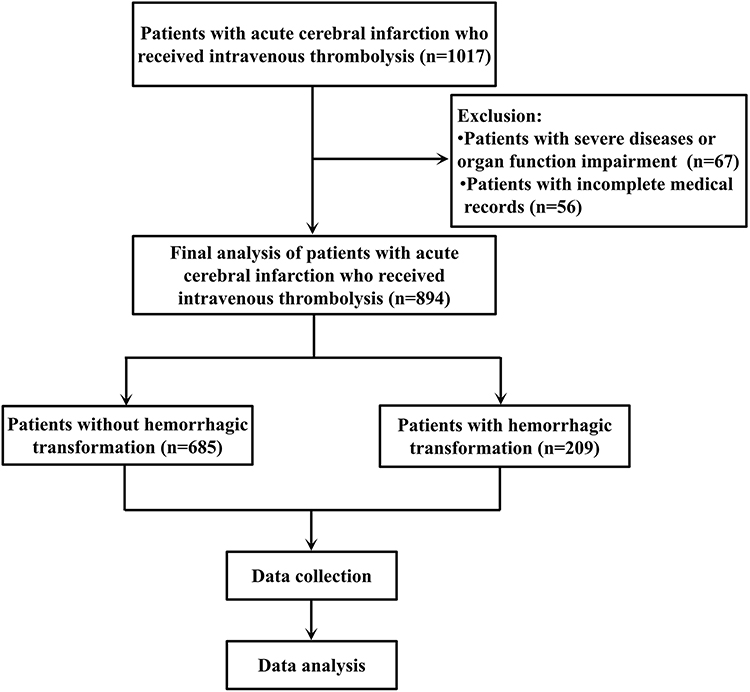 |
Figure 1 The flowchart of this study. |
Data Collection
The clinical data of the patients were collected, including gender, age, hypertension, diabetes mellitus, laboratory data (triglyceride, albumin, platelet, neutrophil, and lymphocyte) and imaging data.
The calculation of mPIV, mSII, and mSIRI:
mPIV=triglyceride×neutrophil×platelet/lymphocyte;
mSII=platelet×neutrophil/lymphocyte×ln(albumin);
mSIRI=platelet×neutrophil/lymphocyte.
Hemorrhagic transformation:34 No hemorrhage was found in the first head computed tomography (CT)/magnetic resonance imaging (MRI) after cerebral infarction, but intracranial hemorrhage was detected in the second head CT/MRI examination, or hemorrhagic infarction can be determined based on the first head CT/MRI.
Statistical Analysis
All statistical analysis were performed using SPSS statistical software version 26.0 (IBM Inc., USA). Continuous variables were compared using t-test or Mann–Whitney U-test. The comparison of categorical variables was conducted using the Chi-square test. The specificity and sensitivity of mPIV, mSII, and mSIRI were described using the receiver operating characteristic (ROC) curve analysis. The accuracy of mPIV, mSII, and mSIRI in differentiating HT was evaluated by calculating the area under the ROC curve (AUC), and the optimal cut-off values of mPIV, mSII, and mSIRI were determined using the Youden index. Logistic regression analysis was used to evaluate the relationship between mPIV, mSII, mSIRI and HT adjusting for other influencing factors, such as gender, age, hypertension, and diabetes mellitus p<0.05.
Results
Clinical Features of the Ischemic Stroke Patients Performed Thrombolysis
A total of 894 ischemic stroke patients were included in this study, including 648 (72.5%) male and 246 (27.5%) female patients. Among them, 663 (74.2%), and 293 (32.8%) patients had hypertension, and diabetes mellitus, respectively. The mean levels of triglyceride, neutrophil count, platelet count, lymphocyte count, and albumin was 1.37 (0.96, 1.96) mmol/L, 5.80 (4.30, 7.76) ×109/L, 214.50 (179.00, 249.25) ×109/L, 1.63 (1.20, 2.21) ×109/L, and 40.90 (38.08, 43.60) g/L, respectively. The median levels of mPIV, mSII, and mSIRI was 1041.12 (617.55, 2073.74), 2657.62 (1703.10, 4524.08), and 722.37 (463.49, 1239.76) in all patients, respectively. There were 685 (76.6%) patients without HT and 209 (23.4%) with HT (Table 1).
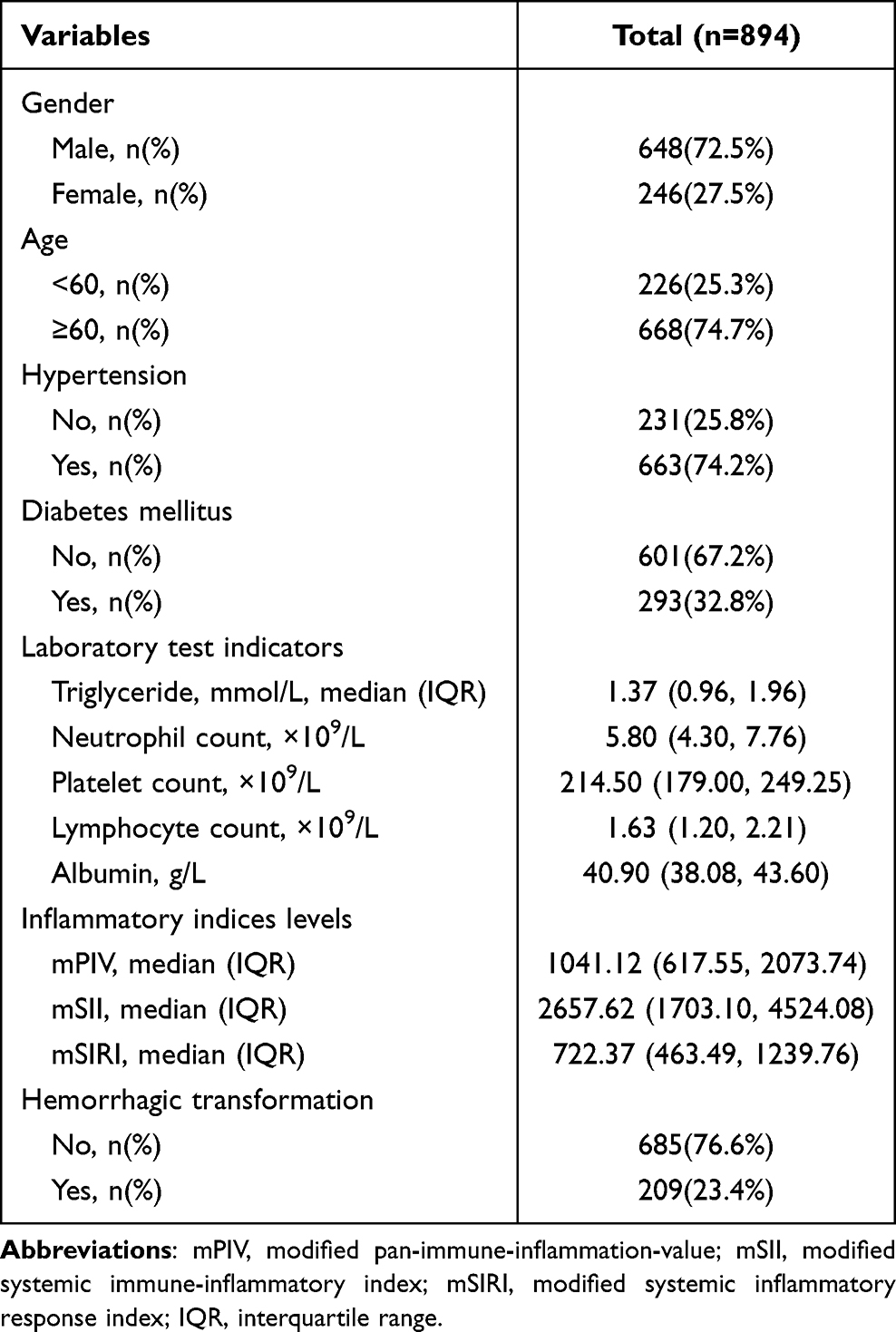 |
Table 1 The Clinical Features of the Ischemic Stroke Patients Performed Thrombolysis |
Comparison of Clinical Features Among HT and Non-HT Patients
The cases with HT had higher mPIV (1337.71 (698.79, 2511.19) vs 992.37 (599.30, 1884.53), p=0.001), mSII (3418.31 (1895.87, 7112.89) vs 2574.81 (1630.46, 4006.18), p<0.001), and mSIRI level (963.60 (517.86, 1947.87) vs 698.75 (446.99, 1100.62), p<0.001) than those without HT, respectively (Table 2 and Figure 2). There was no statistically significant difference in the distribution of gender, age, hypertension and diabetes between the two groups of patients (Table 2).
 |
Table 2 Comparison of Clinical Features Among Hemorrhagic Transformation (HT) and Non-HT Patients |
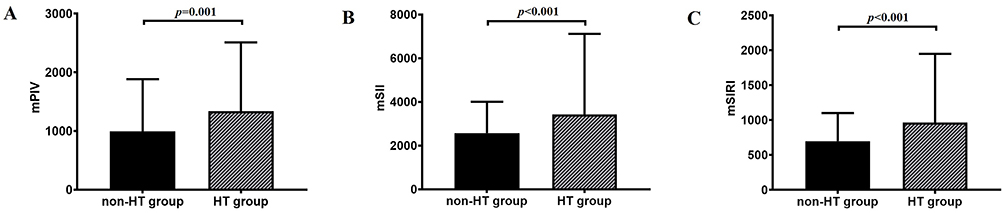 |
Figure 2 Comparison of mPIV (A), mSII (B), and mSIRI (C) in ischemic stroke patients with or without hemorrhagic transformation. Abbreviations: mPIV, modified pan-immune-inflammation-value; mSII, modified systemic immune-inflammatory index; mSIRI, modified systemic inflammatory response index. |
ROC Analysis
ROC analysis showed that the cutoff value of mPIV was 1302.4 (sensitivity 50.7%, specificity 64.7%, area under the ROC curve (AUC): 0.575) (95% confidence interval (CI), 0.529–0.620), the mSII cutoff value was 3186.5 (sensitivity 54.5%, specificity 63.8%, AUC: 0.605) (95% CI, 0.558–0.652), and the mSIRI cutoff value was 996.5 (sensitivity 49.8%, specificity 70.2%, AUC: 0.610) (95% CI, 0.563–0.657) when mPIV, mSII, and mSIRI were used as predictive indicators of HT (Figure 3).
 |
Figure 3 ROC analysis of mPIV, mSII, and mSIRI used in the prediction of hemorrhagic transformation in ischemic stroke patients performed thrombolysis. Abbreviations: mPIV, modified pan-immune-inflammation-value; mSII, modified systemic immune-inflammatory index; mSIRI, modified systemic inflammatory response index. |
Logistic Regression Analysis of the Relationship Between mPIV, mSII, mSIRI and Hemorrhagic Transformation
Univariate analysis showed that high mPIV (odds ratio (OR): 1.884, 95% confidence interval (CI): 1.377–2.577, p<0.001), high mSII (OR: 2.115, 95% CI: 1.545–2.894, p<0.001), and high mSIRI (OR: 2.335, 95% CI: 1.701–3.206, p<0.001) were significantly associated with hemorrhagic transformation. Multivariate logistic regression analysis showed that high mPIV (OR: 1.901, 95% CI: 1.381–2.617, p<0.001), high mSII (OR: 2.081, 95% CI: 1.517–2.854, p<0.001), and high mSIRI (OR: 2.290, 95% CI: 1.664–3.151, p<0.001) were significantly associated with hemorrhagic transformation (Table 3).
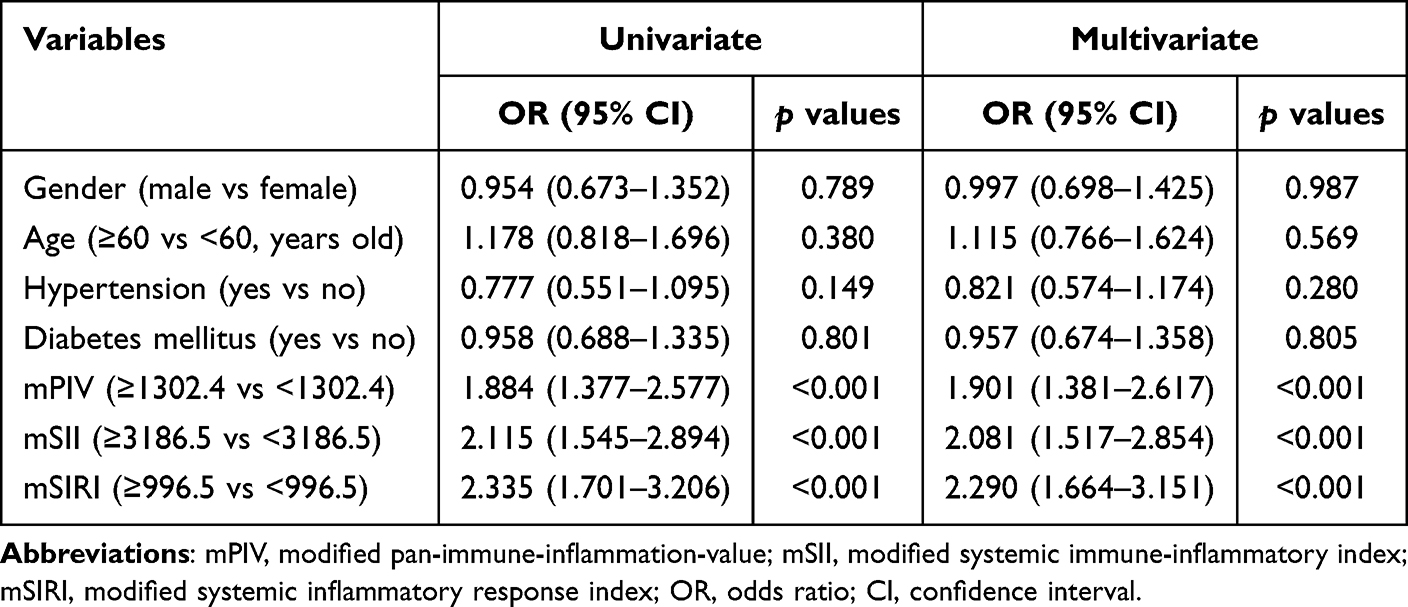 |
Table 3 Logistic Regression Analysis of the Relationship Between mPIV, mSII, mSIRI and Hemorrhagic Transformation |
Discussion
These modified immunoinflammatory indices is a comprehensive indices that combines nutritional status, coagulation, and inflammation. This study aimed to explore the associations between mPIV, mSII, mSIRI and hemorrhagic transformation in patients with acute ischemic stroke who received thrombolytic therapy. And the results found that the cases with HT had higher mPIV, mSII, and mSIRI levels than those without HT. After adjusting for other influencing factors, such as gender, age, hypertension, and diabetes mellitus, this study found that mPIV, mSII, and mSIRI still maintained their independent predictive value for HT, and there were significant interaction effects among these factors. It provides a new perspective for clinical risk assessment.
During thrombolytic therapy for ischemic stroke, the interaction between inflammation and thrombosis constitutes an important pathological basis for the occurrence and development of hemorrhagic transformation.35,36 When embolism occurs in the cerebral blood vessels, local tissue ischemia and hypoxia rapidly activate the inflammatory response.37 A large amount of pro-inflammatory cytokines are released, such as TNF-α and IL-6,38,39 promoting the expression of adhesion molecules by vascular endothelial cells,40 attracting the aggregation of inflammatory cells such as neutrophils and monocytes,41,42 and destroying the integrity of the blood-brain barrier.43 The injury of the blood-brain barrier makes the blood components in the recanalized blood vessels after thrombolysis more likely to leak out, directly increasing the risk of HT.18,44
The dynamic process of thrombosis and dissolution in ischemic stroke further exacerbates the imbalance of the inflammatory response. In the early stage of thrombosis, platelets are activated and release substances such as thromboxane A2 and adenosine diphosphate,45 which not only promote the progression of thrombosis but also activate the complement system and trigger an inflammatory cascade reaction.46–48 After thrombolytic therapy, plasminogen is activated and converted into fibrinolytic protein, and fibrinolytic protein dissolves blood clots and generates fibrin degradation products (FDP) with anticoagulant effects.49 At the same time, it can also stimulate inflammatory cells to secrete more pro-inflammatory factors, leading to a vicious cycle between the coagulation-fibrinolysis system and the inflammatory system,50 and ultimately promoting HT at the originally stable thrombi site.
Neutrophils and platelets, as core participants in the inflammatory and coagulation processes,51 play a key role in the predictive mechanism of mPIV. Neutrophils can release toxic substances such as myeloperoxidase (MPO) and neutrophil elastase (NE), directly damaging the vascular basement membrane.52 Simultaneously activate the complement system, induce the inflammatory cascade reaction, and create pathological conditions for HT.53,54 Platelets play a procoagulant role in the early stage of thrombosis formation. However, their excessive activation can lead to the consumption of coagulation factors and hyperfibrinolysis, and reperfusion injury is prone to occur after thrombolysis.55 In this study, the elevated mPIV, mSII, and mSIRI suggested an enhanced synergistic pro-inflammatory and pro-coagulant effect between neutrophils and platelets, indicating a significant increase in the risk of hemorrhagic transformation.
Lymphocytes, as important cells for immune regulation in the body, a decrease in their quantity reflects the state of suppressed immune function.56 During the pathological process of ischemic stroke, impaired lymphocyte function can lead to insufficient anti-inflammatory response and fail to effectively curb vascular damage caused by excessive inflammation.57 The inclusion of lymphocyte count in mPIV can inversely evaluate the anti-inflammatory repair ability of the body. When the relative value of lymphocytes decreases, the elevated mPIV, mSII, and mSIRI value, further highlighting the intensification of the risk of hemorrhagic transformation.
In this study, mPIV, as a novel parameter integrating lipid metabolism and inflammatory immune indicators, has shown unique value in predicting bleeding transformation in thrombolytic patients with ischemic stroke. Triglycerides (TG) in the mPIV index reflect the lipid metabolism status of the body. High levels of TG can aggravate the dysfunction of vascular endothelial cells and disrupt the integrity of the blood-brain barrier through pathways such as activating protein kinase C and promoting the release of inflammatory factors.58 After thrombolytic therapy, the damaged vascular wall is more prone to blood extravasation, thereby increasing the risk of bleeding transformation. It explains the correlation between the TG component in mPIV and bleeding transformation. Albumin is not only a key indicator reflecting the nutritional status of individual,59 but also an important vascular endothelial protective factor.60 Albumin has the functions of antioxidation, anti-inflammation and maintaining the integrity of the vascular wall.61 Hypoalbuminemia is often accompanied by intensified inflammatory responses and increased vascular permeability in the body.62 After thrombolytic therapy for ischemic stroke, such patients are more prone to exudation of blood components, which in turn leads to HT.63 The mSII provides a new quantitative tool for predicting HT in thrombolytic patients with ischemic stroke by integrating indicators related to coagulation, immunity and nutritional status.
Elevated systemic immune-inflammation index (SII) and systemic inflammatory response index (SIRI) increased the risk of some cardiovascular diseases.64 There are some research reports on the relationship between SII, SIRI, pan-immune-inflammation value (PIV) and ischemic stroke. Xu et al found that a high SIRI is associated with an increased risk of stroke among middle-aged and elderly adults in China.65 SIRI is a risk factor for ischemic stroke in patients with rheumatoid arthritis.66 Elevated PIV and SIRI increase stroke risk in hypertensive individuals.28 Some studies suggested that high SII,67–69 and SIRI69–71 are associated with adverse clinical outcomes in ischemic stroke patients. SII,72–74 SIRI,72–74 and PIV73 are also associated with the risk of adverse outcomes in patients with acute ischemic stroke after intravenous thrombolytic therapy. This study investigated the relationship between mPIV, mSII, mSIRI and the risk of HT after intravenous thrombolysis in ischemic stroke, while no related research reports had been seen before.
Although high levels of mPIV, mSII, and mSIRI showed association with HT in this study, there are still certain limitations. Firstly, the combination and weights of each parameter in the mPIV, mSII, and mSIRI calculation formula lack clear evidence-based medical evidence support. The influence degree of each index on mPIV, mSII, and mSIRI under different disease backgrounds may vary, and its scientificity awaits further verification. Secondly, this study was a retrospective one, with sample selection bias. Moreover, the synergistic effect of mPIV, mSII, and mSIRI with other important clinical factors (such as patient age, underlying diseases, thrombolysis timing, blood pressure control, and so on) was not fully considered, which may affect the universality of the prediction results. Thirdly, at present, the optimal critical value of mPIV, mSII, and mSIRI in patients with ischemic stroke has not been unified, and there are significant differences among different research results, which limits its wide application in clinical diagnosis and treatment.
Conclusion
Overall, in patients with ischemic stroke who received intravenous thrombolysis treatment, high levels of mPIV, mSII, and mSIRI may be associated with hemorrhagic transformation. Of course, this result still requires more research to be verified. Moreover, these comprehensive indices based on hematological indicators need to be combined with other clinical indicators to improve the efficacy of risk prediction.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
All participants were informed on the study procedures and goals and the study obtained written informed consent from all the participants. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital.
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Project of Medical and Health Scientific Research of Meizhou City (Grant No.: 2024-B-98).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhao Y, Zhang X, Chen X, Wei Y. Neuronal injuries in cerebral infarction and ischemic stroke: from mechanisms to treatment (Review). Int J Mol Med. 2022;49(2):15. doi:10.3892/ijmm.2021.5070
2. Li W, Zhang Y, Yang F, Zhang L. Molecular mechanism by which TRPC6 regulates calcium signaling and neuroinflammation in the onset and development of ischemic stroke: a review. Altern Ther Health Med. 2024;30(8):170–175. PMID: 37971464.
3. Kalaria R, Englund E. Neuropathological features of cerebrovascular diseases. Pathology. 2025;57(2):207–219. doi:10.1016/j.pathol.2024.10.003
4. Zheng X, Zhang Y, Man Y, Hu Z, Zhang N, Pan S. Clinical features, risk factors, and early prognosis for Wallerian degeneration in the descending pyramidal tract after acute cerebral infarction. J Stroke Cerebrovasc Dis. 2021;30(2):105480. doi:10.1016/j.jstrokecerebrovasdis.2020.105480
5. Novotny V, Aarli SJ, Netland Khanevski A, Bjerkreim AT. Clinical manifestation of acute cerebral infarcts in multiple arterial territories. Brain Behav. 2021;11(8):e2296. doi:10.1002/brb3.2296
6. Hasan TF, Hasan H, Kelley RE. Overview of acute ischemic stroke evaluation and management. Biomedicines. 2021;9(10):1486. doi:10.3390/biomedicines9101486
7. Keselman B, Gdovinová Z, Jatuzis D, et al. Safety and outcomes of intravenous thrombolysis in posterior versus anterior circulation stroke: results from the safe implementation of treatments in stroke registry and meta-analysis. Stroke. 2020;51(3):876–882. doi:10.1161/STROKEAHA.119.027071
8. Wang Q, Wang Y, Wang Y, Bi Q, Zhang Q, Wang F. Impact of improved stroke green channel process on the delay of intravenous thrombolysis in patients with acute cerebral infarction during the COVID-19 pandemic: an observational study. Front Neurol. 2022;13:998134. doi:10.3389/fneur.2022.998134
9. Ooi YC, Miremadi BB, Mukarram F, et al. Role of intravenous tissue plasminogen activator in acute ischemic stroke with large vessel occlusion. World Neurosurg. 2021;148:e321–e325. doi:10.1016/j.wneu.2020.12.142
10. Zhong K, An X, Kong Y, Chen Z. Predictive model for the risk of hemorrhagic transformation after rt-PA intravenous thrombolysis in patients with acute ischemic stroke: a systematic review and meta-analysis. Clin Neurol Neurosurg. 2024;239:108225. doi:10.1016/j.clineuro.2024.108225
11. Ping Z, Min L, Qiuyun L, Xu C, Qingke B. Prognostic nomogram for the outcomes in acute stroke patients with intravenous thrombolysis. Front Neurosci. 2022;16:1017883. doi:10.3389/fnins.2022.1017883
12. Zhang D, Sheng J, Chen L, et al. Effects of dietary fiber on the risk of gestational diabetes mellitus in advanced maternal age women: study protocol for a randomized controlled trial. Mol Nutr Food Res. 2023;67(3):e2200437. doi:10.1002/mnfr.202200437
13. Zhao C, Xie G. Correlation study of chronic renal insufficiency and long-term prognosis of patients with acute ischemic cerebral apoplexy after intravenous rt-PA thrombolysis. Altern Ther Health Med. 2023;29(8):66–69. PMID: 37708556.
14. Jin M, Peng Q, Wang Y. Post-thrombolysis early neurological deterioration occurs with or without hemorrhagic transformation in acute cerebral infarction: risk factors, prediction model and prognosis. Heliyon. 2023;9(5):e15620. doi:10.1016/j.heliyon.2023.e15620
15. He J, Fu F, Zhang W. Prognostic significance of the clinical and radiological haemorrhagic transformation subtypes in acute ischaemic stroke: a systematic review and meta-analysis. Eur J Neurol. 2022;29(11):3449–3459. doi:10.1111/ene.15482
16. Guasch-Jiménez M, Ezcurra Díaz G. Influence of asymptomatic hemorrhagic transformation after endovascular treatment on stroke outcome: a population-based study. Neurology. 2025;104(9):e213509. doi:10.1212/WNL.0000000000213509
17. Yuan S, Gao D, Shi W, et al. The association of serum biomarkers with symptomatic hemorrhagic transformation in acute ischemic stroke patients: a combined retrospective and prospective study. CNS Neurosci Ther. 2025;31(3):e70321. doi:10.1111/cns.70321
18. Hong JM, Kim DS, Kim M. Hemorrhagic transformation after ischemic stroke: mechanisms and management. Front Neurol. 2021;12:703258. doi:10.3389/fneur.2021.703258
19. Yang K, Zeng L, Ge A, et al. A systematic review of the research progress of non-coding RNA in neuroinflammation and immune regulation in cerebral infarction/ischemia-reperfusion injury. Front Immunol. 2022;13:930171. doi:10.3389/fimmu.2022.930171
20. Miyamoto N, Hattori N. Development of functional recovery therapy for post-stroke sequelae: towards a future without stroke aftereffects. Juntendo Med J. 2025;71(1):26–31. doi:10.14789/ejmj.JMJ24-0026-P
21. Song HY, Chung JI, Jalin AMA, Ju C, Pahk K. The Quinazoline Otaplimastat (SP-8203) reduces the hemorrhagic transformation and mortality aggravated after delayed rtPA-induced thrombolysis in cerebral ischemia. Int J Mol Sci. 2022;23(3):1403. doi:10.3390/ijms23031403
22. Li Y, Liao J, Xiong L, et al. Stepwise targeted strategies for improving neurological function by inhibiting oxidative stress levels and inflammation following ischemic stroke. J Control Release. 2024;368:607–622. doi:10.1016/j.jconrel.2024.02.039
23. Tuz AA, Hoerenbaum N, Ulusoy Ö, et al. Hypercholesterolemia triggers innate immune imbalance and transforms brain infarcts after ischemic stroke. Front Immunol. 2024;15:1502346. doi:10.3389/fimmu.2024.1502346
24. Del Cuore A, Pacinella G. The role of immunosenescence in cerebral small vessel disease: a review. Int J Mol Sci. 2022;23(13):7136. doi:10.3390/ijms23137136
25. Meng J, Zhang J, Fang J, et al. Dynamic inflammatory changes of the neurovascular units after ischemic stroke. Brain Res Bull. 2022;190:140–151. doi:10.1016/j.brainresbull.2022.10.003
26. Shaik NF, Regan RF, Naik UP. Platelets as drivers of ischemia/reperfusion injury after stroke. Blood Adv. 2021;5(5):1576–1584. doi:10.1182/bloodadvances.2020002888
27. Genc O, Yildirim A. Modification, validation and comparison of Naples prognostic score to determine in-hospital mortality in ST-segment elevation myocardial infarction. Eur J Clin Invest. 2025;55(1):e14332. doi:10.1111/eci.14332
28. Chen J, Luo C, Tan D, Li Y. J-shaped associations of pan-immune-inflammation value and systemic inflammation response index with stroke among American adults with hypertension: evidence from NHANES 1999–2020. Front Neurol. 2024;15:1417863. doi:10.3389/fneur.2024.1417863
29. Liu J, Pang SY, Zhou SY, et al. Lipocalin-2 aggravates blood-brain barrier dysfunction after intravenous thrombolysis by promoting endothelial cell ferroptosis via regulating the HMGB1/Nrf2/HO-1 pathway. Redox Biol. 2024;76:103342. doi:10.1016/j.redox.2024.103342
30. Jiang W, Zhao Y. Histidine-rich glycoprotein modulates neutrophils and thrombolysis-associated hemorrhagic transformation. EMBO Mol Med. 2024;16(9):2146–2169. doi:10.1038/s44321-024-00117-y
31. Hasumi K, Suzuki E. Impact of SMTP Targeting Plasminogen and Soluble Epoxide Hydrolase on Thrombolysis, Inflammation, and Ischemic Stroke. Int J Mol Sci. 2021;22(2):954. doi:10.3390/ijms22020954
32. Liu L, Li Z. Chinese Stroke Association guidelines for clinical management of ischaemic cerebrovascular diseases: executive summary and 2023 update. Stroke Vasc Neurol. 2023;8(6):e3. doi:10.1136/svn-2023-002998
33. Lu Y, Zhuoga C, Jin H, et al. Characteristics of acute ischemic stroke in hospitalized patients in Tibet: a retrospective comparative study. BMC Neurol. 2020;20(1):380. doi:10.1186/s12883-020-01957-0
34. Chen R, Hua W. Association between basal ganglia infarction and hemorrhagic transformation after mechanical thrombectomy in acute ischemic stroke: insights from the DIRECT-MT trial. J Neurointerv Surg. 2025;17(e2):e288–e294. doi:10.1136/jnis-2024-022323
35. Yang Y, Xie D, Zhang Y. Increased platelet-to-lymphocyte ratio is an independent predictor of hemorrhagic transformation and in-hospital mortality among acute ischemic stroke with large-artery atherosclerosis patients. Int J Gen Med. 2021;14:7545–7555. doi:10.2147/IJGM.S329398
36. Yang Y, Han Y, Sun W, Zhang Y. Increased systemic immune-inflammation index predicts hemorrhagic transformation in anterior circulation acute ischemic stroke due to large-artery atherosclerotic. Int J Neurosci. 2023;133(6):629–635. doi:10.1080/00207454.2021.1953021
37. Amin N, Chen S, Ren Q, Tan X, Botchway BOA. Hypoxia inducible factor-1α attenuates ischemic brain damage by modulating inflammatory response and glial activity. Cells. 2021;10(6):1359. doi:10.3390/cells10061359
38. Kumari S, Dhapola R, Sharma P, Nagar P, Medhi B, HariKrishnaReddy D. The impact of cytokines in neuroinflammation-mediated stroke. Cytokine Growth Factor Rev. 2024;78:105–119. doi:10.1016/j.cytogfr.2024.06.002
39. Alsbrook DL, Di Napoli M, Bhatia K, et al. Neuroinflammation in acute ischemic and hemorrhagic stroke. Curr Neurol Neurosci Rep. 2023;23(8):407–431. doi:10.1007/s11910-023-01282-2
40. Huang Y, Wang Z, Huang ZX, Liu Z. Biomarkers and the outcomes of ischemic stroke. Front Mol Neurosci. 2023;16:1171101. doi:10.3389/fnmol.2023.1171101
41. Barreca MM, Raimondo S. The combination of natural compounds Escin-Bromelain-Ginkgo Biloba-Sage Miltiorrhiza (EBGS) reduces platelet adhesion to TNFα-activated vascular endothelium through FAK signaling. Int J Mol Sci. 2024;25(17):9252. doi:10.3390/ijms25179252
42. Burkard P, Vögtle T. Platelets in thrombo-inflammation: concepts, mechanisms, and therapeutic strategies for ischemic stroke. Hamostaseologie. 2020;40(2):153–164. doi:10.1055/a-1151-9519
43. Huang L, Chen Y, Liu R, et al. P-glycoprotein aggravates blood brain barrier dysfunction in experimental ischemic stroke by inhibiting endothelial autophagy. Aging Dis. 2022;13(5):1546–1561. doi:10.14336/AD.2022.0225
44. Liang Y, Yu Y, Liu J, et al. Blood-brain barrier disruption and hemorrhagic transformation in acute stroke before endovascular reperfusion therapy. Front Neurol. 2024;15:1349369. doi:10.3389/fneur.2024.1349369
45. Gelbenegger G, Jilma B. Clinical pharmacology of antiplatelet drugs. Expert Rev Clin Pharmacol. 2022;15(10):1177–1197. doi:10.1080/17512433.2022.2121702
46. Tsujimoto H, Inoue N. Coagulation and complement crosstalk: molecular mechanisms of complement-mediated diseases. Rinsho Ketsueki. 2024;65(6):576–583. doi:10.11406/rinketsu.65.576
47. Sharma S, Tyagi T, Antoniak S. Platelet in thrombo-inflammation: unraveling new therapeutic targets. Front Immunol. 2022;13:1039843. doi:10.3389/fimmu.2022.1039843
48. Stark K, Kilani B, Stockhausen S, et al. Antibodies and complement are key drivers of thrombosis. Immunity. 2024;57(9):2140–2156.e2110. doi:10.1016/j.immuni.2024.08.007
49. Zheng Z, Mukhametova L, Boffa MB, et al. Assays to quantify fibrinolysis: strengths and limitations. Communication from the International Society on Thrombosis and Haemostasis Scientific and Standardization Committee on fibrinolysis. J Thromb Haemost. 2023;21(4):1043–1054. doi:10.1016/j.jtha.2023.01.008
50. Kryczka KE, Kruk M, Demkow M, Lubiszewska B. Fibrinogen and a triad of thrombosis, inflammation, and the renin-angiotensin system in premature coronary artery disease in women: a new insight into sex-related differences in the pathogenesis of the disease. Biomolecules. 2021;11(7):1036. doi:10.3390/biom11071036
51. Li J, Tong D, Song B, et al. Inflammatory cytokines induce neutrophil extracellular traps interaction with activated platelets and endothelial cells exacerbate coagulation in moderate and severe essential hypertension. J Hypertens. 2022;40(11):2219–2229. doi:10.1097/HJH.0000000000003250
52. Islam MM, Takeyama N. Role of neutrophil extracellular traps in health and disease pathophysiology: recent insights and advances. Int J Mol Sci. 2023;24(21):15805. doi:10.3390/ijms242115805
53. Johansson L, Berglin E, Eriksson O, Mohammad AJ, Dahlqvist J, Rantapää-Dahlqvist S. Complement activation prior to symptom onset in myeloperoxidase ANCA-associated vasculitis but not proteinase 3 ANCA associated vasculitis - A Swedish biobank study. Scand J Rheumatol. 2022;51(3):214–219. doi:10.1080/03009742.2021.1989814
54. Liu X, Hu Y, Yu X, et al. Differential contributions of the C5b-9 and C5a/C5aR pathways to microvascular and macrovascular thrombosis in complement-mediated thrombotic microangiopathy patients. Clin Immunol. 2024;259:109871. doi:10.1016/j.clim.2023.109871
55. Rosafio F, Vandelli L, Bigliardi G, et al. Usefulness of thromboelastography in the detection and management of tissue plasminogen activator-associated hyperfibrinolysis. J Stroke Cerebrovasc Dis. 2017;26(2):e29–e31. doi:10.1016/j.jstrokecerebrovasdis.2016.10.039
56. Tang G, Yuan X, Luo Y, et al. Establishing immune scoring model based on combination of the number, function, and phenotype of lymphocytes. Aging. 2020;12(10):9328–9343. doi:10.18632/aging.103208
57. Gong Z, Guo J, Liu B, et al. Mechanisms of immune response and cell death in ischemic stroke and their regulation by natural compounds. Front Immunol. 2023;14:1287857. doi:10.3389/fimmu.2023.1287857
58. Nakano T, Goto K. Diacylglycerol kinase ε in adipose tissues: a crosstalk between signal transduction and energy metabolism. Front Physiol. 2022;13:815085. doi:10.3389/fphys.2022.815085
59. Erstad BL. Serum albumin levels: who needs them? Ann Pharmacother. 2021;55(6):798–804. doi:10.1177/1060028020959348
60. Sawashita Y, Kazuma S, Tokinaga Y, et al. Albumin protects the ultrastructure of the endothelial glycocalyx of coronary arteries in myocardial ischemia-reperfusion injury in vivo. Biochem Biophys Res Commun. 2023;666:29–35. doi:10.1016/j.bbrc.2023.04.110
61. Sun L, Yin H, Liu M, et al. Impaired albumin function: a novel potential indicator for liver function damage? Ann Med. 2019;51(7–8):333–344. doi:10.1080/07853890.2019.1693056
62. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and Clinical Significance. J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
63. Liu MS, Liao Y, Li GQ. Glomerular filtration rate is associated with hemorrhagic transformation in acute ischemic stroke patients without thrombolytic therapy. Chin Med J. 2018;131(14):1639–1644. doi:10.4103/0366-6999.235873
64. Jin Z, Wu Q, Chen S, et al. The associations of two novel inflammation indexes, SII and SIRI with the risks for cardiovascular diseases and all-cause mortality: a ten-year follow-up study in 85,154 individuals. J Inflamm Res. 2021;14:131–140. doi:10.2147/JIR.S283835
65. Xu M, Wang W, Chen R, et al. Individual and combined associations of estimated pulse wave velocity and systemic inflammation response index with risk of stroke in middle-aged and older Chinese adults: a prospective cohort study. Front Cardiovasc Med. 2023;10:1158098. doi:10.3389/fcvm.2023.1158098
66. Jin Z, Hao D, Song Y, Zhuang L, Wang Q, Yu X. Systemic inflammatory response index as an independent risk factor for ischemic stroke in patients with rheumatoid arthritis: a retrospective study based on propensity score matching. Clin Rheumatol. 2021;40(10):3919–3927. doi:10.1007/s10067-021-05762-z
67. Huang YW, Yin XS, Li ZP. Association of the systemic immune-inflammation index (SII) and clinical outcomes in patients with stroke: a systematic review and meta-analysis. Front Immunol. 2022;13:1090305. doi:10.3389/fimmu.2022.1090305
68. Ma F, Li L, Xu L, et al. The relationship between systemic inflammation index, systemic immune-inflammatory index, and inflammatory prognostic index and 90-day outcomes in acute ischemic stroke patients treated with intravenous thrombolysis. J Neuroinflammation. 2023;20(1):220. doi:10.1186/s12974-023-02890-y
69. Huang S, Xie W, Gao Y, et al. A role for systemic inflammation in stroke-associated infection and the long-term prognosis of acute ischemic stroke: a mediation analysis. J Inflamm Res. 2024;17:6533–6545. doi:10.2147/JIR.S474344
70. Dang H, Mao W, Wang S, et al. Systemic inflammation response index as a prognostic predictor in patients with acute ischemic stroke: a propensity score matching analysis. Front Neurol. 2022;13:1049241. doi:10.3389/fneur.2022.1049241
71. Chu M, Luo Y, Wang D, et al. Systemic inflammation response index predicts 3-month outcome in patients with mild acute ischemic stroke receiving intravenous thrombolysis. Front Neurol. 2023;14:1095668. doi:10.3389/fneur.2023.1095668
72. Wang N, Wang L, Zhang M, Deng B, Wu T. Correlations of 2 novel inflammation indexes with the risk for early neurological deterioration in acute ischemic stroke patients after intravenous thrombolytic therapy. Neurologist. 2024;29(3):146–151. doi:10.1097/NRL.0000000000000557
73. Li Y, Xi L, Sun H, et al. Association of six complex inflammatory indicators with prognosis in patients with intravenous thrombolysis stroke. Int J Gen Med. 2024;17:5511–5521. doi:10.2147/IJGM.S489482
74. Zhao Y, Zhang R, Li P, et al. A new nomogram for predicting 90-day outcomes of intravenous thrombolysis in patients with acute ischaemic stroke. Front Neurol. 2025;16:1512913. doi:10.3389/fneur.2025.1512913
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio and Platelet-to-Lymphocyte Ratio as Predictors of Short- and Long-Term Outcomes in Ischemic Stroke Patients with Atrial Fibrillation
Guo J, Wang D, Jia J, Zhang J, Liu Y, Lu J, Zhao X, Yan J
Journal of Inflammation Research 2024, 17:6661-6672
Published Date: 23 September 2024
Predictive Value of Epicardial Adipose Tissue for Hemorrhagic Transformation and Functional Outcomes in Acute Ischemic Stroke Patients Undergoing Intravenous Thrombolysis Therapy
Liu L, Jia C, Xing C, Fu X, Liu Z, Ma A
Journal of Inflammation Research 2024, 17:11915-11929
Published Date: 31 December 2024