Back to Journals » Journal of Inflammation Research » Volume 16
Predictive Value of the Changes in Neutrophil-Lymphocyte Ratio for Outcomes After Off-Pump Coronary Surgery
Authors Bae MI ![]() , Shim JK, Song JW, Ko SH, Choi YS, Kwak YL
, Shim JK, Song JW, Ko SH, Choi YS, Kwak YL
Received 20 March 2023
Accepted for publication 26 May 2023
Published 2 June 2023 Volume 2023:16 Pages 2375—2385
DOI https://doi.org/10.2147/JIR.S411057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Myung Il Bae, Jae-Kwang Shim, Jong Wook Song, Seo Hee Ko, Young Seo Choi, Young-Lan Kwak
Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Republic of Korea
Correspondence: Young-Lan Kwak, Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, Republic of Korea, Tel +82-2-2228-8513, Fax +82-2-2227-8063, Email [email protected]
Purpose: The neutrophil-to-lymphocyte ratio (NLR) is an extensively analyzed prognostic inflammatory index in cardiac patients. The degree of change in NLR values before and after surgery (delta-NLR) can represent the inflammatory response induced by surgery and serve as a meaningful prognostic biomarker in surgical patients; however, this has not been well investigated. We aimed to investigate the predictive value of the perioperative NLR and delta-NLR for outcomes of off-pump coronary artery bypass (OPCAB) surgery by evaluating “days alive and out of hospital (DAOH)”, a novel patient-centered outcome.
Patients and Methods: In this single-center retrospective study, perioperative data, including NLR data, from 1322 patients were analyzed. The primary endpoint was DOAH at 90 days postoperatively (DAOH 90), and the secondary endpoint was long-term mortality. Linear regression analysis and Cox regression analysis were performed to identify independent risk factors for the endpoints. In addition, Kaplan–Meier survival curves were plotted to assess long-term mortality.
Results: The median NLR values significantly increased from 2.2 (1.6– 3.1) at baseline to 7.4 (5.4– 10.3) postoperatively, with median delta-NLR values of 5.0 (3.2– 7.6). Preoperative NLR and delta-NLR were independent risk factors for short DAOH 90 in the linear regression analysis. In Cox regression analysis, delta-NLR, but not preoperative NLR, was an independent risk factor for long-term mortality. When patients were divided into two groups according to delta-NLR, the high delta-NLR group had a shorter DAOH 90 than the low delta-NLR group. Kaplan–Meier curves showed higher long-term mortality in the high delta-NLR group than in the low delta-NLR group.
Conclusion: In OPCAB patients, preoperative NLR and delta-NLR were significantly associated with DAOH 90, and delta-NLR was an independent risk factor for long-term mortality, indicating their role in risk assessment, which is essential for perioperative management.
Keywords: neutrophil-to-lymphocyte ratio, off-pump coronary artery bypass, days alive and out of hospital
Introduction
Emerging evidence has shown the role of objective inflammatory indices in predicting postoperative outcomes,1–3 and the neutrophil-to-lymphocyte ratio (NLR) is one of the most extensively analyzed inflammatory indices in various subsets of surgery, including cardiac surgery.4–7 The NLR shows an interaction between neutrophilia and lymphopenia, which are complementary immune pathways. Neutrophilia reflects a nonspecific inflammatory reaction, whereas lymphopenia reflects a poor general condition.8–10 Further, NLR is less affected by physiological changes, such as exercise or dehydration, than individual cell subtypes.10,11 With the practical advantage of being able to measure neutrophil and lymphocyte counts through routine blood tests, NLR has been suggested as an easily accessible and cost-effective predictor of outcomes in cardiovascular disease and surgical patients.12
In a previous study, NLR value measured at the immediate postoperative period (within 1 hour) was associated with postoperative morbidity after coronary artery bypass graft using cardiopulmonary bypass,13 indicating the impact of the surgery-related inflammatory response on the patient’s outcome. In this regard, the degree of change in NLR values before and after surgery (delta-NLR) can represent the inflammatory response induced by surgery and serve as a meaningful prognostic biomarker in surgical patients.14 Although there are a few studies for delta-NLR in cardiac surgery with cardiopulmonary bypass,15,16 the prognostic significance of delta-NLR value has not been well investigated compared to that of the preoperative or postoperative NLR value, especially in off-pump coronary artery bypass (OPCAB) surgery. Given the different perioperative inflammatory kinetics and NLR values in OPCAB compared to on-pump cardiac surgery,17,18 it would be worth examining the predictive value of delta-NLR in OPCAB patients.
Recently, days alive and out of hospital (DAOH), an index that counts the days spent out of hospital after surgery, has been studied as a novel patient-centered outcome parameter.19–23 It integrates the hospital length of stay, readmission, and mortality, representing postoperative outcomes in a patient-centered manner. (Figure 1) In this retrospective study, we aimed to investigate the predictive value of perioperative NLR and delta-NLR for outcomes after OPCAB surgery, which was evaluated using DAOH.
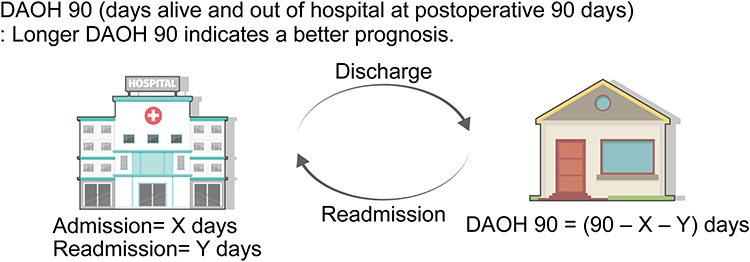 |
Figure 1 Graphical explanation of the days alive and out of hospital. |
Materials and Methods
The Institutional Review Board of the Yonsei University Health System (Seoul, Republic of Korea) approved this study on December 9, 2020 (#4-2020-1187). We retrospectively collected data from electronic medical records stored in the Yonsei University Health System database in South Korea. The need for informed consent was waived since this study retrospectively analyzed clinical data obtained from already completed treatment, and the risk to the subject does not exceed the minimum risk. To maintain the confidentiality of patient data, the collected data were stored on a computer with restricted access, and the case reports were stored on a locked device. This study adhered to the principles of Good Clinical Practice and the Declaration of Helsinki.
Study Population
Patients aged ≥18 years who underwent OPCAB at the Severance Cardiovascular Hospital (Seoul, Republic of Korea) between January 2010 and November 2019 were included. In contrast, we excluded patients who underwent minimally invasive direct coronary artery bypass.
Data Collection
We collected data on sex, age, body mass index (BMI), history of cardiac operation, and preoperative comorbidities, including hypertension, chronic renal failure (CRF), cerebrovascular accident (CVA), diabetes mellitus (DM), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and recent myocardial infarction (MI) (defined as MI within 1 month preoperatively). Moreover, perioperative laboratory results were collected, including neutrophil count; lymphocyte count; and serum levels of albumin, cholesterol, glucose, creatine kinase-MB (CK-MB), C-reactive protein (CRP), and creatinine. We also collected the following perioperative data: EuroSCORE2, preoperative left ventricular ejection fraction, emergency surgery, operation time, number of bypass grafts, intraoperative urine output, and perioperative transfusion (defined as transfusion from the start of surgery to 24 h postoperatively). The following postoperative data were collected: intensive care unit (ICU) length of stay, in-hospital length of stay, readmission, mortality, acute kidney injury (AKI), CVA, deep sternal infection, prolonged mechanical ventilation, and cardiac reoperation. AKI was defined according to the guidelines of the Kidney Disease Improving Global Outcomes,24 and the definitions of CVA, deep sternal infection followed the guidelines of the Society of Thoracic Surgeons Adult Cardiac Surgery Database.25 Furthermore, prolonged mechanical ventilation was defined as mechanical ventilation for > 24 h. In addition, we also collected information on the date of surgery, admission, discharge, death, and last follow-up.
Calculation of NLR
The NLR was calculated using the following formula, described in a previous study:26 NLR = (neutrophil count) / (lymphocyte count). The preoperative NLR (pre-NLR) was calculated from the preoperative laboratory results dated closest to the time of surgery (within 7 days before surgery), and the postoperative NLR (post-NLR) was calculated from laboratory results obtained on postoperative day 3 (POD 3). The delta-NLR was calculated by subtracting the pre-NLR from the post-NLR.
Endpoints
The primary endpoint was the DAOH at postoperative 90 days (DAOH 90), which indicates the number of days spent out of the hospital for 90 days after surgery. It was calculated from the length of hospital stay, readmission, and mortality, and a longer DAOH 90 indicates a better prognosis. (Figure 1) As in previous studies, if a patient died within 90 days postoperatively, DAOH 90 was calculated as zero.19,20 The secondary endpoint was long-term mortality.
Statistical Analysis
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), R Statistics version 4.2.2, and IBM SPSS Statistics 25 (IBM Corp., Armonk, NY, USA). We performed the Kolmogorov–Smirnov test to evaluate the normality of continuous variables. Since none of the continuous variables in this study showed a normal distribution, all continuous variables were expressed as medians (interquartile ranges). Dichotomous variables were expressed as numbers (percentages). Additionally, Spearman’s rank correlation coefficients were calculated between pre-NLR, post-NLR, and delta-NLR.
Regarding DAOH 90, linear regression analysis was performed for each variable. Additionally, multivariable linear regression analysis was performed using a multivariable model, including the variables that showed a p-value less than 0.05 in the univariable analysis. Since the post-NLR and delta-NLR showed a strong correlation (Spearman correlation coefficient = 0.918), the pre-NLR and delta-NLR, but not the post-NLR, were included in the multivariable model to avoid multicollinearity.
Cox regression analysis for long-term mortality was performed on each variable. Further, multivariable Cox regression analysis was conducted using a multivariable model, which included the variables that had p-values less than 0.05 in the univariable analysis. Pre-NLR and delta-NLR, but not post-NLR, were included in the multivariable model to avoid multicollinearity.
Linear regression analysis was also performed between variables and delta-NLR, and a multivariable linear regression analysis was conducted using a multivariable model that included variables with a p-value less than 0.05 in the univariable analysis.
Patients were divided into high and low delta-NLR groups according to the values arranged in a row, and postoperative outcomes were compared between the two groups. As all continuous variables did not show a normal distribution, the Mann–Whitney U-test was used to compare them between the two groups. The chi-squared test or Fisher’s exact test was used to compare dichotomous variables between the two groups.
Furthermore, Kaplan–Meier survival curves were plotted to assess long-term mortality, and the Log rank test was performed to assess whether there was a difference between the survival curves. For all statistical analyses, a p-value < 0.05 was considered statistically significant.
Results
Initially, 1539 patients who underwent OPCAB at Severance Cardiovascular Hospital between January 2010 and November 2019 were screened. Fifty-four patients who underwent minimally invasive direct coronary artery bypass surgery and one patient who required emergent conversion to an on-pump procedure were excluded. In addition, 162 patients with missing data were excluded from the analysis. Therefore, data from 1322 patients were included in the final analysis (Figure 2).
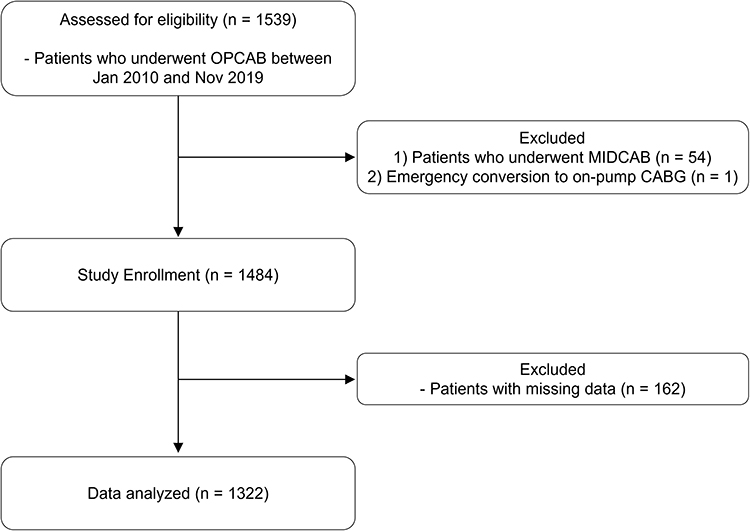 |
Figure 2 Flow diagram of the study. Abbreviations: OPCAB, off-pump coronary artery bypass; MIDCAB, minimally invasive direct coronary artery bypass; CABG, coronary artery bypass graft surgery. |
The median NLR values significantly increased from 2.2 (1.6–3.1) at baseline to 7.4 (5.4–10.3) on POD 3. When analyzing the changes in NLR values pre- and postoperatively, the NLR increased in 1299/1322 patients (98.4%), with a median delta-NLR value of 5.0 (3.2–7.6) (Table 1). Notably, there was a moderate degree of correlation between pre-NLR and post-NLR (rho = 0.433, P < 0.001), a poor degree of correlation between pre-NLR and delta-NLR (rho = 0.115, P < 0.001), and a strong correlation between delta-NLR and post-NLR (rho = 0.918, P < 0.001).
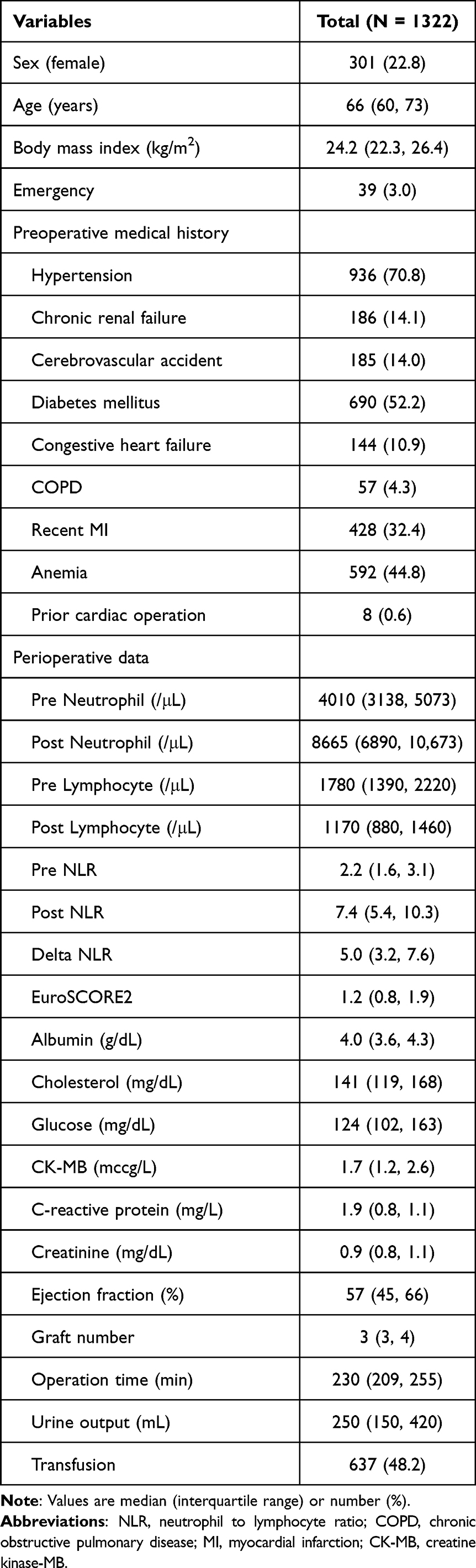 |
Table 1 Patient Demographics, Clinical Data, and Laboratory Finding |
The median DAOH 90 was 81 (76–82) days, and the overall mortality rate was 5.3% (70 patients) during the median follow-up duration of 36 (17–59) months. All deaths occurred after POD 3 (delta-NLR measurement). The patient demographics, clinical data, and laboratory findings are presented in Table 1.
Multivariable linear regression analysis between the chosen variables and DAOH 90 is summarized in Table 2. Pre-NLR, delta-NLR, age, history of CRF and CHF, and serum albumin levels were significantly correlated with DAOH 90. Univariable regression analyses regarding DAOH 90 are summarized in Supplementary Table S1.
 |
Table 2 Multivariable Linear Regression Analysis Between Chosen Variables and DAOH 90 |
Table 3 presents the multivariable Cox regression analysis for long-term mortality. Delta-NLR, age, and history of anemia showed a significant hazard ratio for long-term mortality; however, pre-NLR did not show a significant hazard ratio for long-term mortality in the multivariable analysis. Univariable Cox regression analysis of each variable for long-term mortality is shown in Supplementary Table S2.
 |
Table 3 Multivariable Cox Regression Analysis of Chosen Variables for Long-Term Mortality |
When comparing postoperative outcomes between the high and low delta-NLR groups, the high delta-NLR group showed a significantly shorter DAOH 90 and higher incidences of in-hospital morbidities compared to the low delta-NLR group (Table 4).
 |
Table 4 Postoperative Outcome According to delta-NLR Groups |
Multivariable linear regression analysis between the chosen variables and delta-NLR showed that sex, age, BMI, history of hypertension, CRF, CHF, MI within 1 month, EuroSCORE2, and serum albumin levels were significantly correlated with delta-NLR (Supplementary Table S3).
Figure 3 shows the Kaplan–Meier survival curves according to the delta-NLR groups. Log-rank analysis indicated that long-term mortality increased in the high delta-NLR group compared to the low delta-NLR group (P<0.001).
 |
Figure 3 Kaplan–Meier survival curves according to delta-NLR groups. The blue line represents the survival curves of the low delta NLR group, and the red line represents the survival curves of the high delta-NLR group. |
Discussion
In this single-center retrospective study, preoperative NLR and delta-NLR were proven to be good predictors of DAOH 90 after OPCAB. Additionally, delta NLR, but not preoperative NLR, was significantly associated with long-term mortality. Patients in the high delta-NLR group demonstrated poorer postoperative outcomes than those in the low delta-NLR group.
Considering the significant association between inflammatory responses and outcomes after cardiac surgery,3 objective inflammatory indices have been developed to improve risk stratification in cardiac surgery. Among these indices, the NLR has been demonstrated to be an important inflammatory biomarker that predicts outcomes after cardiac surgery.6,7 The NLR represents a complex interplay between two complementary immune pathways, represented by neutrophils and lymphocytes.8–10 An elevated neutrophil count reflects the nonspecific activation of inflammation associated with oxidative stress. In contrast, a decreased lymphocyte count reflects poor general health and a dysregulated host immune response to physiologic stress.8–10 In addition to their pivotal role in immune activities, neutrophils and lymphocytes have an essential role in the formation and stability of atherosclerotic plaque,27–29 and the NLR is closely related to the progression of atherosclerosis.30,31 Accordingly, the NLR has been reported to be a meaningful predictor of prognosis in coronary artery disease patients who underwent surgery.32 However, previous studies have focused on preoperative NLR, and there have been few studies on the dynamic changes in the NLR. The delta-NLR can represent the degree of inflammation and physical stress induced by surgical stimulation and may serve as a valuable prognostic indicator in surgical patients.14 Therefore, we evaluated the effects of delta-NLR on outcomes after OPCAB.
In the current study, delta-NLR was strongly correlated with postoperative NLR (rho = 0.918) but poorly correlated with preoperative NLR (rho = 0.115). When patients were divided into high and low delta-NLR groups, the difference in preoperative NLR value between the two groups was significant, but not by much in the present study (2.1 (1.5–2.9) in the low delta-NLR group; 2.3 (1.7–3.2) in the high delta-NLR group). These findings may indicate that the preoperative NLR alone cannot sufficiently predict the increase in inflammation caused by OPCAB surgery. Notably, pre- and delta-NLR demonstrated significant relationships with DAOH 90, whereas only delta-NLR showed a significant relationship with long-term mortality in this study. These results imply that measuring pre- and delta-NLR together would be helpful for better risk stratification and screening of high-risk patients. However, they are not definitive diagnostic tests and should be used in conjunction with other clinical assessments. The delta-NLR was significantly related to well-known risk factors for poor prognosis after cardiac surgery, which implies that delta-NLR may be affected by the patient’s underlying condition, and delta-NLR can properly represent it.
The timing of measuring postoperative NLR values varies among different studies and could affect the delta-NLR values. In the current study, laboratory results on POD 3 were used to calculate postoperative NLR and delta-NLR. Previous studies have reported that the inflammatory response after cardiac surgery peaks within 48 hours and shows a decreasing trend.33,34 Therefore, we hypothesized that the NLR measured on POD 3 might reflect the early recovery phase after cardiac surgery. The delta-NLR on POD 3 may be a valuable indicator for identifying patients who were not in the high-risk group preoperatively but had a poor recovery pattern postoperatively. In this regard, greater incidences of postoperative in-hospital morbidity were observed in the high delta-NLR group than in the low delta group in the current study. This might indicate that delta-NLR reflects the declined immediate postoperative conditions. It could contribute to the predictability of delta-NLR for long-term mortality.
The active role of neutrophils and lymphocytes in atherosclerotic plaque formation may contribute to the high preoperative NLR values in patients with coronary artery disease.29,35 Similar to the result of the present study, a preoperative NLR was an independent risk factor of postoperative outcomes in patients with stable coronary artery disease and acute coronary syndromes, as well as in patients undergoing coronary artery bypass graft surgery.36–38 Interestingly, some studies on OPCAB reported that the postoperative NLR, but not the preoperative NLR, was related to long- and mid-term mortality rates after surgery,39,40 while they did not evaluate the prognostic value of the delta-NLR.
Compared with previous studies that used mortality several years after surgery as a primary outcome, the present study focused on relatively short-term outcomes such as DAOH 90. Although mid- and long-term mortality are important endpoints in cardiac surgery, DAOH is a novel outcome that accounts for multiple outcome parameters in a patient-centered manner.19–21 In recent years, there has been an increasing emphasis on patient-centered outcomes, which represent actual patient experiences, such as improved quality of life or cost savings.21 DAOH is an easily accessible patient-centered outcome, which reflects the days spent healthy after surgery.22,23 It has been validated to be a valuable outcome for clinical investigations.19–23 To the best of our knowledge, this is the first study to investigate DAOH 90 in patients undergoing OPCAB.
An elevated NLR can occur in various whole blood cell subgroups, including those with elevated neutrophil, reduced lymphocyte, normal neutrophil, and normal lymphocyte counts. When we evaluated each component of the NLR in the present study, median preoperative neutrophil and lymphocyte counts were within the normal range; however, the NLR was higher than that in a healthy population,41 indicating the importance of a balance between the two components. Postoperatively, the neutrophil count increased by 117% (65–175%), and the lymphocyte count decreased by 35% (20–48%), resulting in a 235% (136–362%) increase in the NLR. These findings clearly show the activation of opposite immune-inflammatory pathways induced by OPCAB and confirm the importance of delta-NLR as a risk stratification marker.
This study had some limitations. First, this was a retrospective study, and the data were limited to a single center; however, this study analyzed a large sample size of 1322 patients and included many variables that could affect postoperative outcomes. Second, we excluded the data of 162 patients with missing values, which may have affected the statistical results; however, the data of the remaining 1322 patients were intact data without missing values and were large enough for analysis.
Conclusion
In conclusion, both pre- and delta-NLR were significantly associated with DAOH 90, and delta-NLR showed a significant relationship with long-term mortality after OPCAB surgery, indicating their beneficial role in risk assessment, which is essential for the perioperative management of these patients.
Abbreviations
AKI, acute kidney injury; AUROC, area under the receiver operating characteristic curve; BMI, body mass index; CHF, congestive heart failure; CK-MB, creatine kinase-MB; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; CRP, C-reactive protein; CVA, cerebrovascular accident; DAOH, days alive and out of hospital; DAOH 90, days alive and out of hospital at postoperative 90 days; DM, diabetes mellitus; ICU, intensive care unit; MI, myocardial infarction; NLR, neutrophil-to-lymphocyte ratio; OPCAB, off-pump coronary artery bypass; POD, postoperative day; ROC, receiver operating characteristic.
Data Sharing Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The Institutional Review Board of the Yonsei University Health System (Seoul, Republic of Korea) approved this study on December 9, 2020 (#4-2020-1187). The need for informed consent was waived since this study retrospectively analyzed clinical data obtained from already completed treatment, and the risk to the subject did not exceed the minimum risk.
Acknowledgments
The authors thank Medical Illustration & Design, part of the Medical Research Support Services of Yonsei University College of Medicine, for providing support with the medical illustration. The authors also thank the Biostatistics Collaboration Unit of Yonsei University College of Medicine for providing statistical consultation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Aviles RJ, Martin DO, Apperson-Hansen C, et al. Inflammation as a risk factor for atrial fibrillation. Circulation. 2003;108(24):3006–3010. doi:10.1161/01.CIR.0000103131.70301.4F
2. Collaboration ERF. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–140. doi:10.1016/S0140-6736(09)61717-7
3. Laffey JG, Boylan JF, Cheng DC, Cheng DH. The systemic inflammatory response to cardiac surgery: implications for the anesthesiologist. Anesthesiology. 2002;97(1):215–252. doi:10.1097/00000542-200207000-00030
4. Paramanathan A, Saxena A, Morris DL. A systematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumours. Surg Oncol. 2014;23(1):31–39. doi:10.1016/j.suronc.2013.12.001
5. Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil–lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol. 2013;88(1):218–230. doi:10.1016/j.critrevonc.2013.03.010
6. Perry LA, Liu Z, Loth J, et al. Perioperative neutrophil-lymphocyte ratio predicts mortality after cardiac surgery: systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2022;36(5):1296–1303. doi:10.1053/j.jvca.2021.07.001
7. Tan TP, Arekapudi A, Metha J, Prasad A, Venkatraghavan L. Neutrophil–lymphocyte ratio as predictor of mortality and morbidity in cardiovascular surgery: a systematic review. ANZ J Surg. 2015;85(6):414–419. doi:10.1111/ans.13036
8. Gibson PH, Cuthbertson BH, Croal BL, et al. Usefulness of neutrophil/lymphocyte ratio as predictor of new-onset atrial fibrillation after coronary artery bypass grafting. Am J Cardiol. 2010;105(2):186–191. doi:10.1016/j.amjcard.2009.09.007
9. Shao Q, Chen K, Rha S-W, Lim H-E, Li G, Liu T. Usefulness of neutrophil/lymphocyte ratio as a predictor of atrial fibrillation: a meta-analysis. Arch Med Res. 2015;46(3):199–206. doi:10.1016/j.arcmed.2015.03.011
10. Azab B, Zaher M, Weiserbs KF, et al. Usefulness of neutrophil to lymphocyte ratio in predicting short- and long-term mortality after non-ST-elevation myocardial infarction. Am J Cardiol. 2010;106(4):470–476. doi:10.1016/j.amjcard.2010.03.062
11. Chen C, Gu L, Chen L, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as potential predictors of prognosis in acute ischemic stroke. Front Neurol. 2020;11:525621. doi:10.3389/fneur.2020.525621
12. Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther. 2016;14(5):573–577. doi:10.1586/14779072.2016.1154788
13. Abanoz M, Engin M. The effect of the relationship between post-cardiotomy neutrophil/lymphocyte ratio and platelet counts on early major adverse events after isolated coronary artery bypass grafting. Turk Gogus Kalp Damar Cerrahisi Derg. 2021;29(1):36–44. doi:10.5606/tgkdc.dergisi.2021.20873
14. Yamamoto T, Kawada K, Obama K. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int J Mol Sci. 2021;22(15):8002. doi:10.3390/ijms22158002
15. Parla K, Tatli AB, Pala AA, Goncu MT. The ımportance of ınflammatory parameters ın predıctıng deep sternal wound ınfectıons after open heart surgery. Rev Assoc Med Bras. 2022;68:1185–1190. doi:10.1590/1806-9282.20220140
16. Parlar H, Arıkan AA, Önmez A. Dynamic changes in perioperative cellular inflammation and acute kidney injury after coronary artery bypass grafting. Braz J Cardiovasc Surg. 2021;36(3):354–364. doi:10.21470/1678-9741-2020-0163
17. Tomic V, Russwurm S, Möller E, et al. Transcriptomic and proteomic patterns of systemic inflammation in on-pump and off-pump coronary artery bypass grafting. Circulation. 2005;112(19):2912–2920. doi:10.1161/CIRCULATIONAHA.104.531152
18. Aldemir M, Baki ED, Adali F, Çarşanba G, Tecer E, Taş HU. Comparison of neutrophil: lymphocyte ratios following coronary artery bypass surgery with or without cardiopulmonary bypass. Cardiovasc J Afr. 2015;26(4):159–164. doi:10.5830/CVJA-2015-015
19. Myles PS, Shulman MA, Heritier S, et al. Validation of days at home as an outcome measure after surgery: a prospective cohort study in Australia. BMJ Open. 2017;7(8):e015828. doi:10.1136/bmjopen-2017-015828
20. Jerath A, Austin PC, Ko DT, et al. Socioeconomic status and days alive and out of hospital after major elective noncardiac surgery: a population-based cohort study. Anesthesiology. 2020;132(4):713–722. doi:10.1097/ALN.0000000000003123
21. Jerath A, Austin PC, Wijeysundera DN. Days alive and out of hospital: validation of a patient-centered outcome for perioperative medicine. Anesthesiology. 2019;131(1):84–93. doi:10.1097/ALN.0000000000002701
22. Spurling L-J, Moonesinghe SR, Oliver CM. Validation of the days alive and out of hospital outcome measure after emergency laparotomy: a retrospective cohort study. Br J Anaesth. 2022;128(3):449–456. doi:10.1016/j.bja.2021.12.006
23. Fanaroff AC, Cyr D, Neely ML, et al. Days alive and out of hospital: exploring a patient-centered, pragmatic outcome in a clinical trial of patients with acute coronary syndromes. Circ Cardiovasc Qual Outcomes. 2018;11(12):e004755. doi:10.1161/CIRCOUTCOMES.118.004755
24. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–c184. doi:10.1159/000339789
25. Bowdish ME, D’Agostino RS, Thourani VH, et al. The Society of Thoracic Surgeons adult cardiac surgery database: 2020 update on outcomes and research. Ann Thorac Surg. 2020;109(6):1646–1655. doi:10.1016/j.athoracsur.2020.03.003
26. Zahorec R. Ratio of neutrophil to lymphocyte counts-rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
27. Naruko T, Ueda M, Haze K, et al. Neutrophil infiltration of culprit lesions in acute coronary syndromes. Circulation. 2002;106(23):2894–2900. doi:10.1161/01.CIR.0000042674.89762.20
28. Major AS, Fazio S, Linton MF. B-lymphocyte deficiency increases atherosclerosis in LDL receptor-null mice. Arterioscler Thromb Vasc Biol. 2002;22(11):1892–1898. doi:10.1161/01.ATV.0000039169.47943.EE
29. Bodi V, Sanchis J, Nunez J, et al. Uncontrolled immune response in acute myocardial infarction: unraveling the thread. Am Heart J. 2008;156(6):1065–1073. doi:10.1016/j.ahj.2008.07.008
30. Balta S, Celik T, Mikhailidis DP, et al. The relation between atherosclerosis and the neutrophil–lymphocyte ratio. Clin Appl Thromb Hemost. 2016;22(5):405–411. doi:10.1177/1076029615569568
31. Açar G, Fidan S, Uslu ZA, et al. Relationship of neutrophil–lymphocyte ratio with the presence, severity, and extent of coronary atherosclerosis detected by coronary computed tomography angiography. Angiology. 2015;66(2):174–179. doi:10.1177/0003319714520954
32. Gurbuz O, Kumtepe G, Ozkan H, et al. Predictive value of neutrophil-lymphocyte ratio for long-term cardiovascular event following coronary artery bypass grafting. Braz J Cardiovasc Surg. 2020;35:274–284. doi:10.21470/1678-9741-2018-0362
33. Boyle EM, Pohlman TH, Johnson MC, Verrier ED. Endothelial cell injury in cardiovascular surgery: the systemic inflammatory response. Ann Thorac Surg. 1997;63(1):277–284. doi:10.1016/s0003-4975(96)01061-2
34. Chew MS, Brandslund I, Brix-Christensen V, et al. Tissue injury and the inflammatory response to pediatric cardiac surgery with cardiopulmonary bypass: a descriptive study. Anesthesiology. 2001;94(5):745–753. doi:10.1097/00000542-200105000-00010
35. Arbel Y, Finkelstein A, Halkin A, et al. Neutrophil/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients undergoing angiography. Atherosclerosis. 2012;225(2):456–460. doi:10.1016/j.atherosclerosis.2012.09.009
36. Wada H, Dohi T, Miyauchi K, et al. Pre-procedural neutrophil-to-lymphocyte ratio and long-term cardiac outcomes after percutaneous coronary intervention for stable coronary artery disease. Atherosclerosis. 2017;265:35–40. doi:10.1016/j.atherosclerosis.2017.08.007
37. Dong C-H, Wang Z-M, Chen S-Y. Neutrophil to lymphocyte ratio predict mortality and major adverse cardiac events in acute coronary syndrome: a systematic review and meta-analysis. Clin Biochem. 2018;52:131–136. doi:10.1016/j.clinbiochem.2017.11.008
38. Gibson PH, Croal BL, Cuthbertson BH, et al. Preoperative neutrophil-lymphocyte ratio and outcome from coronary artery bypass grafting. Am Heart J. 2007;154(5):995–1002. doi:10.1016/j.ahj.2007.06.043
39. Urbanowicz T, Michalak M, Olasińska-Wiśniewska A, et al. Neutrophil counts, neutrophil-to-lymphocyte ratio, and Systemic Inflammatory Response Index (SIRI) predict mortality after off-pump coronary artery bypass surgery. Cells. 2022;11(7):1124. doi:10.3390/cells11071124
40. Urbanowicz T, Michalak M, Gąsecka A, et al. Postoperative neutrophil to lymphocyte ratio as an overall mortality midterm prognostic factor following OPCAB procedures. Clin Pract. 2021;11(3):587–597. doi:10.3390/clinpract11030074
41. Forget P, Khalifa C, Defour J-P, Latinne D, Van Pel M-C, De Kock M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res Notes. 2017;10:1–4. doi:10.1186/s13104-016-2335-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.